Article Text

Abstract
Objective The study was aimed at examining the magnitude, trends and determinants of grand multiparity in the Sidama regional state of Ethiopia.
Design We retrieved cross-sectional data from the Ethiopia Demographic and Health Survey from 2000 to 2016.
Setting Community-based demographic and health survey (DHS) was conducted in Ethiopia.
Participants The study population was women (aged 15–49 years) who had delivered children with the available DHS data set.
Outcomes Multilevel multivariate logistic regression analyses assessed the relationship between grand multiparity and its determinants.
Results The magnitude of grand multiparity was 70.8% (95% CI 68.5% to 72.9%). The multilevel multivariable logistic regression model showed illiteracy (adjusted OR (AOR)=2; 95% CI 1.25 to 3.75), non-use of any contraceptive (AOR=3.8; 95% CI 1.2 to 12.2), early marriage (AOR=4.5; 95% CI 2.6 to 7.9), polygamous marriage (AOR=4.2; 95% CI 2.0 to 9.3), short birth intervals (AOR=2.3; 95% CI 1.4 to 3.5) and husband’s low education status (AOR=5.8; 95% CI 2.1 to 16.1) were significantly associated with grand multiparity.
Conclusions This study revealed that 7 of 10 women were grand multipara, and the magnitude did not show significant change over the last 16 years. Early marriage and early age at first birth, low literacy level, low family planning utilisation, polygamy, short interbirth interval and unmet need for family planning were determinants of grand multiparity. We recommended the stakeholders to design new strategies to address the root cause of high fertility factors in communities.
- Community child health
- Epidemiology
- Maternal medicine
- Prenatal diagnosis
- Antenatal
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
The strength of this study included analysing the most recent nationally representative data sets aided in providing a broad comparative picture of grand multiparity in the study setting, as well as significant predictors of children ever born among ever-married women.
To avoid misleading inferences and thus valid interpretation of the results, clustering effects were considered using a mixed modelling approach.
Despite the above strengths, the study may have had recall bias because participants were asked about the events that occurred 5 years or more before the survey.
Also, we used secondary data sets; we were limited in our ability to select exposure variables for statistical analysis.
Background
Grand multiparty, a situation when a woman has at least five deliveries at gestational age greater than or equal to 20 weeks, is a major public health concern in developing countries, particularly in sub-Saharan Africa.1–3 Its obstetric performance is considered as high risk which is defined as the one in which the woman, fetus and/or newborn are at increased risk of morbidity or mortality prenatal, intrapartum or post partum.4 In this regard, there is a high disparity in the fertility rates between the developed and developing countries.5 The factors responsible for the huge disparity are usually neglected in existing family planning and reproductive health programmes, which causes the grand multiparity to be a serious public health problem worldwide, particularly in developing countries including Ethiopia.6 7
While the global fertility rate declined from 3.2 live births per woman in 1990 to 2.5 in 2019, the magnitude increased to 4.6 in 2019 in sub-Saharan Africa including Ethiopia, which indicates a high fertility rate.8–10
Various factors have been identified to be associated with the grand multiparity and these include early age at first marriage, low socioeconomic status, polygamous marriage,11 husband’s preference, culture, religion and residence in a rural area. Others are low literacy level, poor mass media exposure, low level of awareness of health and lack of access to modern contraceptives especially in most sub-Saharan Africa.1 12 13
According to studies conducted in some developing countries, grand multipara women have a higher number of children than women in developed countries. Indeed, many factors contribute to grand multiparity, but some published literature identified the factors for grand multiparity in low and lower middle-income countries.1 14–16 Still, grand multiparity has not been well addressed, as there is a dearth of evidence on a larger scale. Also, there were inadequate studies carried out on the trend, magnitude and associated factors of grand multiparity by using nationally representative demographic and health survey (DHS) data. Therefore, this study was carried out to assess the trend and associated factors of grand multiparity using DHS data for the Sidama region from 2000 to 2016. The findings will assist programme managers and policy makers in developing appropriate intervention strategies to effectively address the challenges and problems of grand multipara women in order to prevent high parity in the community in terms of reproductive health services at all levels.
Methods and materials
Study area and period
Sidama National Regional State is one of the 10 national regional states in Ethiopia. The region is divided into 36 districts (6 urban districts and 30 rural districts). Hawassa city is the capital of the region, and it is situated in the Southern part, about 273 km away from Addis Ababa, Ethiopia’s capital. The Sidama people have a total number of 8.8 million (4.01% of the national population) and are the fifth most populous ethnic group in Ethiopia. Sidama National Regional State has 123 health centres and 17 hospitals.10 17–20 For this study, we used secondary data from the 2000 to 2016 Ethiopia Demographic and Health Survey (EDHS). The DHS data had been collected from 18 January 2016 to 27 June 2016 by the Ethiopian Central Statistical Agency.10
Study design, data source and sampling techniques
Cross-sectional survey data were obtained from 2000 to 2016 (EDHS). The data were retrieved from the (DHS) programme’s official database website (http://dhsprogram.com). It is a nationally representative household survey that collects information about population, health and other important indicators. The sample of the EDHS study was designed to collect up-to-date information from each of the 10 regions and the two administrative cities. Each region was stratified into urban and rural areas; 21 sampling strata were obtained. Samples of enumeration areas (EAs) were selected independently in each stratum in two stages. In the first stage, a total of EAs were selected with a proportional sampling technique and with independent selection in each sampling stratum. The selection of households was the second stage. A fixed number of households per cluster were selected with an equal probability proportional allocation to sample size.10
This study used the birth record data set, and the study population was women (aged 15–49 years) who had delivered children with the available DHS data set. From the birth record data set, the total number of multiparous (para 2–4) and grand multiparous (para 5–9) women was extracted for Sidama National Regional State from 2016 EDHS. The total sample was extracted for women who gave birth (parity 2–9) from the birth record data set. The total number of women (parity 2–9) in the study region of Ethiopia was included in 1654 weighted samples. For trend analysis, grand multipara women in all the four DHS data from 2000 to 2016 were extracted by using the quantitative method.10 21–23
Study variables
Dependent variable
The outcome variable of this study was grand multiparity which was categorised into ‘Yes=1/No=0’ form. This includes all women who have five to nine deliveries as grand multiparity categories.1 2 24

Yi=represent the parity of the ith ever-born children.
Independent variables
The independent variables for this study were identified based on previous studies conducted on the factors affecting grand multiparity at the different places that were reviewed from the literature as associated factors of grand multiparity.11 14 25–35 The independent variables selected for analysis from the available data set were place of residence, maternal age, education status of women, wealth index, current marital status, polygamous marriage, women currently working, religion, husband’s education level, husband’s occupation status, women supported by husband, community media exposure, age of women at first birth, age at first sex, number of living children, preceding birth interval (months), the contraceptive method used, unmet need for contraceptives, the desire for more children, the child being alive, place of delivery and husband’s desire for more children. In this analysis, independent variables were categorised into individual-level and community-level variables. Individual-level variables were age of women, women’s education status, wealth index, women’s age at first birth, number of living children, current marital status, polygamous marriage, women’s age at first sex, desire for more children, contraceptive method, unmet need for contraceptives, women currently working, the child being alive, preceding birth interval (months), place of delivery, women supported by husband, husband’s education status, husband’s occupation status and husband’s desire for more children. Community-level variables were religion, place of residence (rural or urban) and community media exposure.
Data analysis
For analysis, the weighted sample data were used to ensure the survey results were representative of the regions. Based on each weighted variable, the descriptive statistics were reported with summary indices, frequency and proportion. The trend analysis of grand multiparity was assessed using the extended Mantel-Haenszel χ2 test for linear trend using the OpenEpi (V.3.01) response program.36 A p value <0.05 was used to declare a 95% significant probability of the existence of a trend. The degree of crude association for individual and community variables was checked by employing a χ2 test.
For the nested structure of the EDHS data, a multilevel multivariable logistic regression analysis was used. Also, for the mixed effect (a fixed effect for both the individual-level and community-level factors and a random effect for the between-cluster variation), a two-level mixed-effects logistic regression analysis was used. The final findings were measured using an adjusted OR (AOR). Within the multilevel multivariable logistic regression analysis, four models were fitted for the result variable. The primary model (null or empty model) was fitted without explanatory variables. The second model (individual model), third model (community model) and fourth model (final model) variables were fitted for individual-level, community-level, and each individual-level and community-level variable, respectively. The final model was used to check for the independent effect of the individual-level and community-level variables on grand multiparity. To show cluster correlation within a model, the intracluster correlation (ICC) was calculated. The proportional change in variance (PCV) was also calculated to determine the predictive power of the variables included in each model. To identify the factors associated with grand multiparity, the model with the highest PCV value was used.
The model fitness was assessed using the Akaike information criterion (AIC), the Bayesian information criterion (BIC) and the likelihood ratio test. The values for each model of AIC and BIC were compared, the lowest one assumed to be a better explanatory model.37 Multicollinearity between the individual-level and community-level variables was checked using the variance inflation factor (VIF). The mean value of VIF <10 was the cut-off point.38 In the present study, the mean VIF value was estimated to be 2.44 showing the absence of multicollinearity in the models. The data were analysed using the STATA statistical software system package V.14.0 (StataCorp, College Station, Texas, USA). It was considered statistically significant if the p values were less than 0.05 with the 95% CIs.
Patient and public involvement
No patient was involved in this study.
Results
Sociodemographic characteristics of study participants
In this study, a total weighted sample of 1654 women were included in the analysis from the latest EDHS data (2016). The mean age (±SD) of the women was 35±6.7 years, with the majority aged between 40 and 49 years. Almost all (99%) of the women lived in a rural setting, and close to two-thirds (67%) were illiterate. Slightly more than half (55%) of the women were under a low level of socioeconomic status. Almost all of them were married (93%) and follow the protestant religion (92%). More than three-fourths (77%) of the women were not supported by their husbands to do day-to-day chores. In addition, the majority of husbands had attended formal education and had different types of occupations. The summarised information on the sociodemographic background is displayed in table 1.
Sociodemographic characteristics of study participants in the Sidama National Regional State; data from 2016 Ethiopia Demographic and Health Survey.
Sexual and reproductive health characteristics of study participants
The mean age (±SD) of women at first delivery was 17.69±2.75 years and at first coital exposure was 16±2.6 years. The women’s mean number of living children was 4.9 with ±1.8 SD. About two-thirds (64.8%) of women had short birth intervals within or less than 36 months. Among participants, a considerable proportion of women (45.81%) did not use modern contraceptives. Nearly 1 out of 10 women (10.9%) had experienced child death in the survey. Slightly more than three-fourths (80%) of women gave birth at home (table 2).
Fertility, and sexual and reproductive health characteristics of study participants in Sidama regional state; data from 2016 Ethiopia Demographic and Health Survey.
The magnitude of grand multiparous women
The prevalence of grand multiparity with the weighted sample was 70.8% (95% CI 68.5% to 72.9%) in the 5 years preceding the survey in the Sidama region. Evidence is from 2016 EDHS (figure 1).

The magnitude of grand multiparity in Sidama region, data from Ethiopia Demographic and Health Survey (EDHS) 2016.
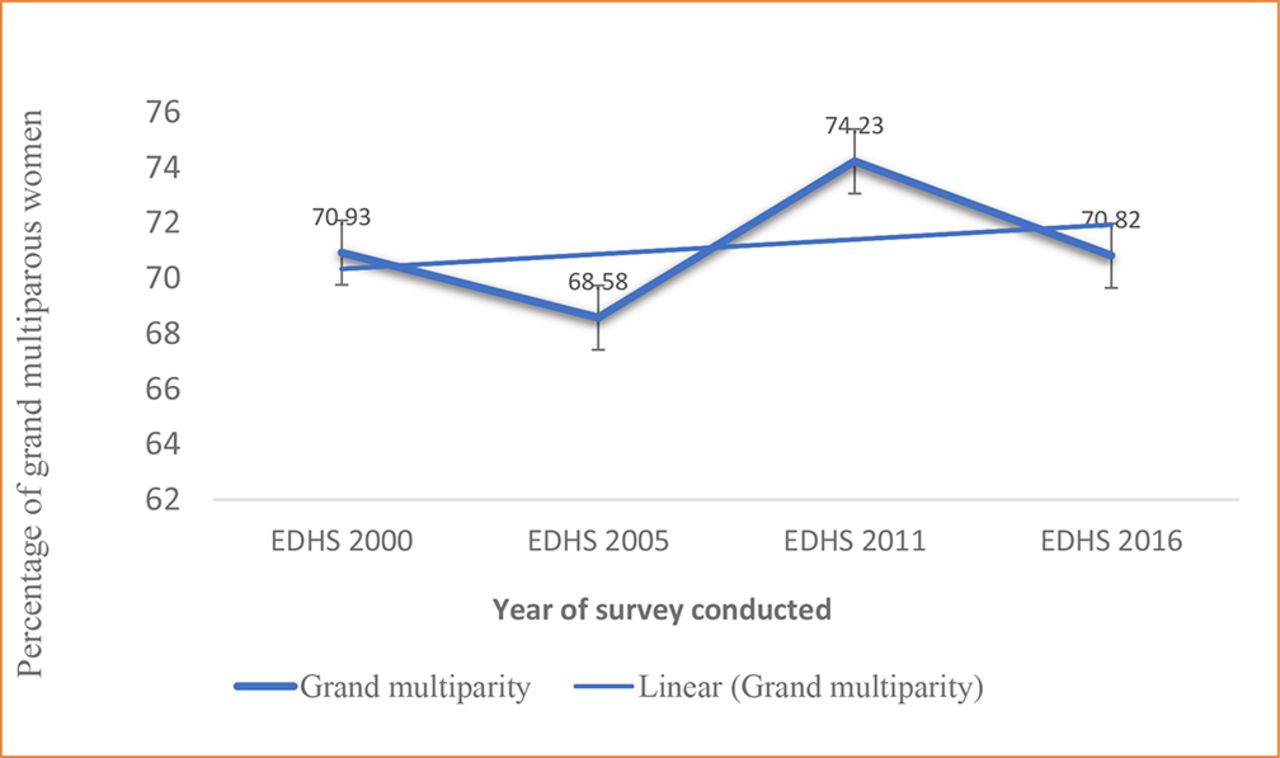
The trend of grand multiparous women
The magnitudes of the grand multiparity were 70.93% in 2000 EDHS, 68.58% in 2005 EDHS, 74.23% in 2011 EDHS and 70.82% in 2016 DHS in the Sidama National Regional State. Over 16 years, the trend of grand multiparous women from four surveys showed no significant change (extended Mantel-Haenszel χ2 test for linear trend=1.13, p=0.29). Likewise, no percentage change was observed between 2000 and 2016 EDHS in the Sidama region (figure 2).
{kind=link}
{kind=link}
Trend of grand multiparous women in Sidama National Regional State, Ethiopia; Ethiopia Demographic and Health Survey (EDHS) data from year 2000 to 2016.
Bivariate variable association with grand multipara women
Regarding education status, the lack of formal education (75.8%) was significantly higher in grand multiparous women than in multipara (48.6%) (p<0.001). An enormous number of women in both groups were of the poorest and poorer status on the wealth index. The unmet need for contraceptives and underutilisation of long-acting family planning were significantly higher in grand multipara than multipara (p<0.001). Among grand multipara, women in polygamous marriages were significantly higher compared with multipara women (p<0.001). Likewise, the age of women at first birth, short birth intervals, husband’s education level, number of living children and place of residence showed significant associations in both study groups (p<0.001).
However, no significant differences were observed between grand multipara and multiparous regarding women currently working, place of delivery, the child being alive, current marital status, husband’s occupation status and community media exposure (p>0.05) (table 3).
Bivariate variable association of individual-level and community-level variables with grand multipara and multiparous women in Sidama National Regional State, Ethiopia; data from EDHS 2016
Determinants of grand multiparity
We applied a two-level mixed-effects multivariable logistic regression using the extracted data from 2016 DHS for the Sidama National Regional State that is aimed at identifying individual-level and community-level determinants of grand multiparity or women having high parity. Those four models were developed to analyse factors accordingly. According to random effects analysis, model 1 had no individual-level and community-level variables, and it observed only the random and intercept variables. In model 1, the ICC value was 20%. This indicates that the variation on the grand multiparity occurred at the community level (between-cluster variability) and it contributed to the community-level factors. The ICC greater than zero in the null model indicates that it guided the researcher to use multilevel modelling than the standard single-level regression model. Also, results in subsequent models between cluster variabilities were found to be 14.4% in model 2 (individual-level factors), 18.6% in model 3 (community-level factors) and 14.5% in model 4 (combined individual-level and community-level factors). In another way, the PCV results indicated that the predictor variables to the null model better explained the factors associated with grand multiparity. The PCV finding for model 2 was 33.7%, for model 3 was 9.6% and model 4 was 33.7%. The final model (combined individual-level and community-level factors) indicated that 34% of the community-level variation on grand multiparity was explained by the combined factors at both the individual and community levels. The result was reported based on model 4 (combined individual-level and community-level factors were fitted simultaneously). As a result, variables such as education level, age of women at first birth, contraceptive methods used, husband’s occupation status, polygamy, age at first sex, unmet need for contraceptives, preceding birth interval and husband’s education level were significantly associated with grand multiparous women, according to model 4 findings.
The odds of grand multiparity compared with multiparity was two times (AOR=2; 95% CI 1.25 to 3.75) higher among women who were uneducated compared with women who were educated. The odds of grand multiparity compared with those multiparous women not using any contraceptive method was 3.85 times higher compared with those women using long-acting family planning (AOR=3.8; 95% CI 1.2 to 12.2).
The odds of grand multiparity was 4.5 times higher among women who had their first births before 18 years old compared with those after 18 years old (AOR=4.5; 95% CI 2.6 to 7.9). The odds of grand multiparity was 4.2 times higher for those who were in polygamous marriages compared with those in monogamous marriages (AOR=4.2; 95% CI 2.0 to 9.3). In addition, the likelihood of grand multiparity was 80% less likely to have met needs for contraceptives compared with those women who have unmet needs for contraceptives (AOR=0.2; 95% CI 0.09 to 0.83). The odds of grand multiparity was 2.3 times higher among women who had short birth intervals compared with those women with normal birth intervals (AOR=2.3; 95% CI 1.4 to 3.5). The odds of grand multiparity was 5.8 times higher among women whose husbands had primary education compared with those who attended secondary schools and above (AOR=5.8; 95% CI 2.1 to 16.1). Also, the odds of grand multiparity was 3.4 times higher among women whose husbands lacked formal education compared with those women whose husbands had a secondary level of education and above (AOR=3.4; 95% CI 1.2 to 9.9) (table 4).
Multilevel logistic regression model of individual-level and community-level factors associated with grand multiparous women in Sidama National Regional State, Ethiopia, using data from the 2016 EDHS.
Discussion
Seven out of 10 reproductive age women had experienced grand multiparity. Age at marriage, literacy status of women, age of women at first birth, modern contraceptive method utilisation, polygamy, husband’s education level, preceding birth interval and unmet need for contraceptives were significantly associated with women having high parity.
During the analysis, the ICC value was found to be 14.5% in the combined model. This indicates that 14.5% of the chances of grand multiparous women were explained through cluster differences. The ICC greater than zero in the null model indicates that it guided the researcher to use multilevel modelling than the standard single-level regression model.37 39 40 Similarly, the study indicates that the proportion change in variance of the final model was accountable for about 33.7% of the log odds of high parity in the communities. In addition to that, the results of the median OR, a measure of unexplained cluster heterogeneity, are 2.48, 3.51, 2.43 and 3.34 in models 1, 2, 3 and 4, respectively. Hence, the results of the median OR showed that there is unexplained variation between the clusters of the community.
In the present study, the magnitude of grand multiparity was 70.8%. This is similar to a community-based study conducted in Gedeo Zone (69.1%) and Tigray Region, Ethiopia (51%).25 29 This figure was quite higher than the prevalence reported by other investigators ranging from 9.4% to 27% in Gambian, Cameroon, Nigeria, Tanzania and India.2 33 34 41 42 The fact that later studies were all carried out in health facilities and urban catchment areas could explain these low prevalence rates. The educational backgrounds, and socioeconomic, sociodemographic and cultural settings of these studies are different from the current findings.31 Similarly, there are many contributing factors to high fertility, among which are early marriage, the perceived ideal number of children and mass media exposure by women.14 25 While the prevalence of grand multiparity in developed countries has significantly declined ranging from 3% to 4%,43 it has increased in the current study and this could be explained by lack of formal education (75.8%) and a high number of early marriages. As individual health implications, the women are given more subsequent births while they get more maternal and child health risks and many socioeconomic challenges in their lifetime in low-resource setting areas.24 35 44 45
The trends of grand multiparity over study periods showed no significant change. This finding was consistent with a previous study done in rural Cameroon.31 However, in Tanzania, the previous study’s findings showed a significant change in the trend of grand multiparity.26 This decline could have been explained by the availability of higher education to women and increased community awareness of the health risks of giving birth at an advanced maternal age and the benefits of family planning and empowerment of women in reproductive health decision-making.26
This study revealed that grand multiparity was higher among women who had their first births before 18 years old compared with those women who started after 18 years. We realised that in the study community where women start birth before 18 years, the period of fertility is longer, and they have many ever-born children. As a result of these, women have high parity. Similarly, the women not using modern family planning appropriately and timely for spacing and limiting the number of births have high fertility. This is similar to the previous study done in Gedeo Zone, Ethiopia,25 Nigeria,46 Nepal14 and Pakistan.28 Nevertheless, the problem of early age at first delivery is significantly more alarming in the present study area than in the previous findings.
The odds of grand multiparity compared with that of multiparity was higher among women who were illiterate compared with literate women. This finding is in line with previous studies conducted in Nigeria,46 Kenya,27 Nepal14 and the Tigray Region in Ethiopia.29 In this study, almost all the women were rural dwellers (99%). Women who are rural inhabitants are less likely to spend much time in school and would rather get married early. A possible explanation is that women residing in the urban area stay longer in school, thereby postponing the time for marital engagement.25 On the other hand, researchers found that education is an important factor for high parity, with several causal relationships from a theoretical perspective.47 To sum up, education generally results in an improvement in the status of individuals in society in the form of a better understanding of health issues and employment status.48 The low social class found among the grand multiparous women is usually associated with illiteracy and low socioeconomic status, which may be an encouraging factor to produce more children.11
The grand multiparity was higher among women with short birth intervals (less than or equal to 36 months). This finding is also consistent with a study conducted in Wonago District, Gedeo Zone, Ethiopia.25 The possible explanation might be due to women not using modern contraceptives that lead the women to get more children in a short period.
In our study, it was found that grand multiparity is significantly associated with polygamous marriage compared with monogamous marriage. This finding is similar to other studies conducted in Nigeria.1 The variation could be due to competition among wives to have many children and to build large family sizes.
The grand multiparity among women not using any contraceptive and using short-acting contraceptive methods was higher compared with those women using long-acting contraceptives. Similar findings were reported in Nigeria,46 Cambodia,49 Pakistan28 and Wonago District, Gedeo Zone.25 Most factors in this study are directly or indirectly associated with the low utilisation of contraceptives, which indicated that it is the root cause of high fertility in the study setting. In addition, in one study, the women were not using contraceptives because their husbands did not allow them to make contraceptive decisions.49
Conclusions
This study revealed that 7 of 10 women had experienced grand multiparity and the magnitude did not show significant change over the last 16 years. Early marriage and early age at first birth, low literacy level, low family planning utilisation, polygamy marital status, short birth interval and unmet need for family planning were determinants of grand multiparity. We recommended the stakeholders to design new strategies to address the root cause of high fertility factors in communities. The Ministry of Health should focus on health education and create awareness about maternal health risks related to grand multiparity in the community. Furthermore, special attention should be given to improving the utilisation of contraceptives in the community to reduce the prevalence of grand multiparity.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Acknowledgments
We would like to thank the MEASURE DHS Program and ICF International for providing us the permission to use the EDHS data. We would also like to acknowledge the African Union for supporting this study.
References
Footnotes
Contributors TTD, MAO and YD conceptualised the idea and designed the study. TTD and YD carried out the execution, data acquisition, analysis and interpretation, and wrote the draft manuscript. MAO and YD provided intellectual comments and contributed to revising the manuscript. All authors contributed to the revision of the manuscript content and approved the final version. TTD accepts responsibility for the conduct of the study, has access to the data and has control over the decision to publish and the overall content of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.