Article Text

Abstract
Objective To evaluate the durability of response 3 months after the third BNT162b2 vaccine in adults aged 60 years and older.
Design Prospective cohort study.
Setting Single tertiary centre.
Participants Healthcare workers/family members aged ≥60 years old who received the third BNT162b2 dose.
Interventions Blood samples were drawn immediately before (T0), 10–19 days (T1) and 74–103 days (T2) after the third dose.
Primary and secondary outcome measures Anti-spike IgG titres were determined using a commercial assay and seropositivity was defined as ≥50 arbitrary units (AU)/mL. Neutralising antibody titres were determined at T2. Adverse events, COVID-19 infections and Clinical Frailty Scale (CFS) levels were documented.
Results The analysis included 97 participants (median age, 70 years (IQR, 66–74), 58% CFS level 2). IgG titres, which increased significantly from T0 to T1 (median, 440 AU/mL (IQR, 294–923) and median, 25 429 AU/mL (IQR, 14 203–36 114), respectively; p<0.001), decreased significantly by T2, but all remained seropositive (median, 8306 AU/mL (IQR, 4595–14 701), p<0.001 vs T1). In a multivariable analysis, only time from the second vaccine was significantly associated with lower IgG levels at T2 (p=0.017). At T2, 60 patients were evaluated for neutralising antibodies; all were seropositive (median, 1294 antibody titres; IQR, 848–2072). Neutralising antibody and anti-spike IgG levels were correlated (r=0.6, p<0.001). No major adverse events or COVID-19 infections were reported.
Conclusions Anti-spike IgG and neutralising antibody levels remain adequate 3 months after the third BNT162b2 vaccine in healthy adults aged ≥60 years, although the decline in IgG is concerning. A third dose of vaccine in this population should be top priority.
- COVID-19
- EPIDEMIOLOGY
- IMMUNOLOGY
Data availability statement
Data are available upon reasonable request. This study is ongoing. Individual participant-level data that underlie the results reported in this article (text, tables and figures) will be shared after de-identification, following the publication of the final endpoint of this study (6-month follow-up), upon request from the corresponding author.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
Study strengths include assessment of both IgG and neutralising antibodies and follow-up which included a questionnaire on adverse events.
Study weaknesses include lack of cellular immunity testing and lack of neutralising antibody testing at the first two timepoints.
At the time of study initiation, the third dose of vaccine was available only to those aged 60 years and older.
Introduction
The COVID-19 pandemic, which has been affecting global health for the past 2 years, is caused by SARS-CoV-2. Age and frailty are among the strongest predictors of COVID-19 mortality.1 2 Due to immunosenescence, the primary vaccine response in those aged 65 years and older is associated with lower rates of protection compared with younger individuals.3 The BNT162b2 messenger RNA (mRNA) vaccine (Pfizer/BioNTech) induces generally lower antigen-binding IgG and virus-neutralising responses in individuals aged 65–85 years compared with those aged 18–55 years, when monitored 2 weeks post vaccination,4 and immunity wanes in all age groups.5 6 In Israel, COVID-19 was first diagnosed at the end of February 2020, and since then and up to our study period three waves of the pandemic have been clearly defined in the country. In July 2021, the Israel Ministry of Health has approved mRNA-based vaccines (Pfizer/BioNTech, mRNA-BNT162b2, which requires two doses, 21 days apart) and a national immunisation programme started vigorously on 19 December 2020. The national immunisation programme prioritised elderly adults and other populations at higher risk of severe COVID-19, followed by the general population. The first wave in Israel resulted in 4000 hospitalisations and 329 deaths, whereas the second and third waves were severe and ended with 40 000 hospitalisations and 6099 more deaths.7
We recently reported the initial findings of a prospective cohort study that evaluated the anti-spike (anti-S) IgG antibody response before and after the third dose of the BNT162b2 vaccine in adults aged 60 years and older.8 We showed that the third dose of vaccine was associated with significantly increased IgG titres, 10–19 days after that dose, with no major adverse events. The difference in median IgG titres before and after the third dose was >50-fold.8
The durability of response to the vaccine in adults aged 60 years and older is yet to be determined. Understanding the extent of waning immunity is critical to policy making, especially surrounding vaccination strategies. In this study, we evaluated the anti-S IgG antibody titres and neutralising antibodies 3 months after the third BNT162b2 dose in adults aged 60 years and older.
Methods
Patient and public involvement
Patients or the public were not involved in the design, or conduct, or reporting or dissemination plans of our research.
Study setting and participants
Rabin Medical Center (RMC) is a tertiary hospital staffed by 7500 healthcare workers, including employees, students and volunteers. Following the authorisation of a third dose in Israel on 1 August 2021, RMC offered this dose to healthcare workers and their family members. Between 4 and 12 August, study participants were recruited from those aged 60 years and older at the RMC vaccination centre. Exclusion criteria included prior SARS-CoV-2 infection (confirmed by PCR); steroidal treatment equivalent to 15 mg prednisone for the past 21 days or longer; active chemotherapy, immunotherapy or biological treatments; active solid, haematological malignancy or both; and conditions affecting immunocompetence, including liver cirrhosis, haemodialysis, solid organ transplant, bone marrow transplant, AIDS, inherent immune deficits such as congenital/acquired deficiencies of the complement system, and asplenism or functional asplenism (eg, sickle cell disease).
Sample collection
Blood samples were drawn from the study participants before they received their third dose of the BNT162b2 vaccine (T0; 4–12 August 2021). Blood samples were also drawn 10–19 days (T1; 16–24 August 2021) and 74–103 days after the third vaccination (T2; 3–15 November 2021; except for two patients who came to their follow-up appointment on the wrong date and for whom the blood sample was drawn on 17 October 2021).
At T2, a second blood sample was drawn from 60 participants who were randomly selected for neutralisation antibody analysis and was sent to the Israel Institute for Biological Research (Ness Ziona, Israel), where SARS-CoV-2 pseudovirus neutralisation assay was performed. The serum samples were stored in −80°C until the day of analysis.
Assessments
Titres of anti-S IgG antibodies in the serum from the blood samples were determined at the RMC microbiological laboratory, using a chemiluminescent microparticle immunoassay, performed on the Abbott architect i2000sr platform, in accordance with the manufacturer’s package insert for SARS-CoV-2 IgG II Quant assay (Abbott Laboratories, Abbott Park, Illinois, USA; reference 6S60-22).9 The strength of the response (in relative light units (RLU)) was determined relative to IgG II calibrator/standard and reflects the quantity of IgG antibodies present. Seropositivity was defined as 50 arbitrary units (AU)/mL and higher. The assay is 98.1% sensitive 15 days or longer after the onset of COVID-19 symptoms or positive PCR test result and 99.6% specific.10
Pseudovirus-neutralising assay was performed using pseudoviruses expressing SARS-CoV-2 spike protein. Plasmids encoding a luciferase reporter (pGreenFire1, System Biosciences), lentivirus backbone (psPAX, Addgene) and S genes (19 S-covid-pCMV3, a kind gift from Professor Yossef Shaul, Weizmann Institute of Science, Rehovot, Israel) were cotransfected into HEK293T cells (ATCC CRL-3216). Forty-eight hours later, the medium was collected and virus aliquots were stored at −80°C for future use. One day before the pseudovirus neutralisation assay, hACE2-expressing HEK293T cells were plated in a white-wall 96-well plate (2×104 cells per well). On the day of the assay, heat-inactivated sera were twofold serially diluted and mixed with pseudovirus, incubated for 1 hour at 37°C, and added to hACE2-expressing HEK293T cells. Twenty-four hours later, cells were lysed and luciferase activity (in RLU) was measured.11 12 Per cent neutralisation was normalised using uninfected cells as 100% neutralisation and cells infected with only pseudovirus as 0% neutralisation. IC50 titres were determined using a log (agonist) versus normalised-response (variable slope) non-linear function using Prism software (GraphPad). Seropositivity was defined as a titre of 20 and higher.
The frailty of all participants was assessed at recruitment and confirmed at each timepoint thereafter via an interview using the 9-point Clinical Frailty Scale (CFS).13 In addition, data were derived from the electronic medical records of all participants, including age, sex, vaccine doses and vaccination dates, and comorbidities.
Before the third vaccination and during both postvaccination follow-up appointments, the study participants completed a questionnaire on adverse reactions post vaccination and whether they had a confirmed COVID-19 infection since the third dose/last follow-up, and if so their symptoms were documented.
Statistical analysis
Participant characteristics were analysed using descriptive statistics. The difference in anti-S IgG values from T0 to T1 and from T1 to T2 was evaluated using a linear mixed effects model. Spearman correlation was used to assess the correlation between the anti-S IgG antibody values and neutralising antibodies titres. Univariate and multivariable analyses were performed by fitting a linear model on the log of anti-S IgG antibody values at T2 and included age and days from the second vaccination as continuous variables, and sex, comorbidities (dyslipidaemia, hypertension, obesity, diabetes and ischaemic heart disease) and CFS as categorical variables.
For all analyses, IgG values above 80 000 AU/mL were considered as 80 000 AU/mL. A p value of less than 0.05 was considered significant. All tests were two-sided. Statistical analysis was performed using R V.4.0.2.14
Results
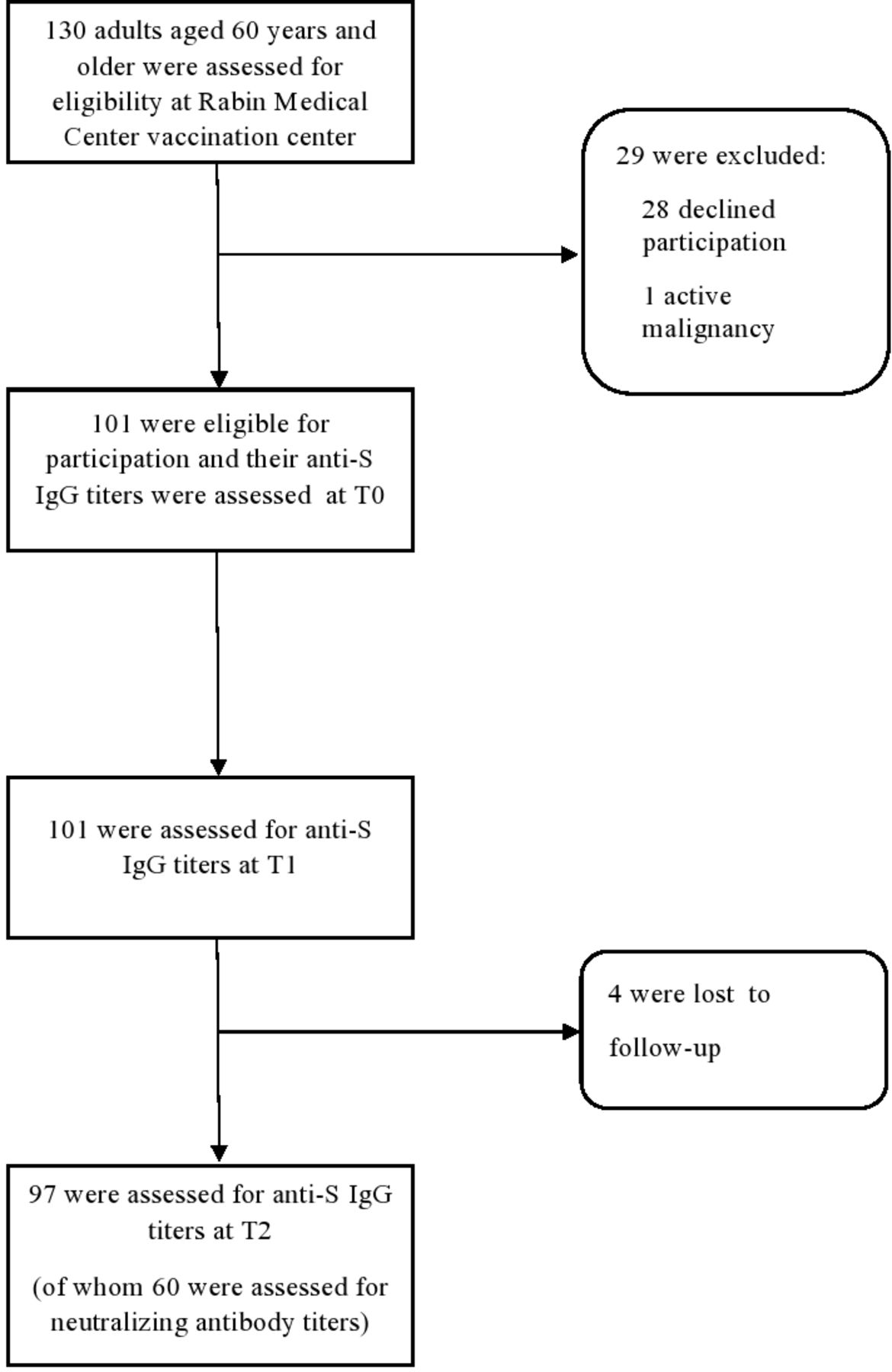
Overall, 130 consecutive individuals aged 60 years and older were approached at the RMC vaccination centre, of whom 1 did not meet the eligibility criteria due to active malignancy and 28 refused participation. IgG levels at T0 were determined for 101 participants (78%). A total of four participants (3%) were lost to follow-up. Thus, the final cohort included 97 participants (figure 1). The median age was 70 years (IQR, 66–74) and 61% were women. The most common comorbidity was dyslipidaemia (61%), followed by hypertension (49%). The frailty of majority of the participants (58%) was characterised as ‘well’ (CFS level 2) (table 1).
Baseline demographics and cohort characteristics before and up to 3 months after the third BNT162b2 dose
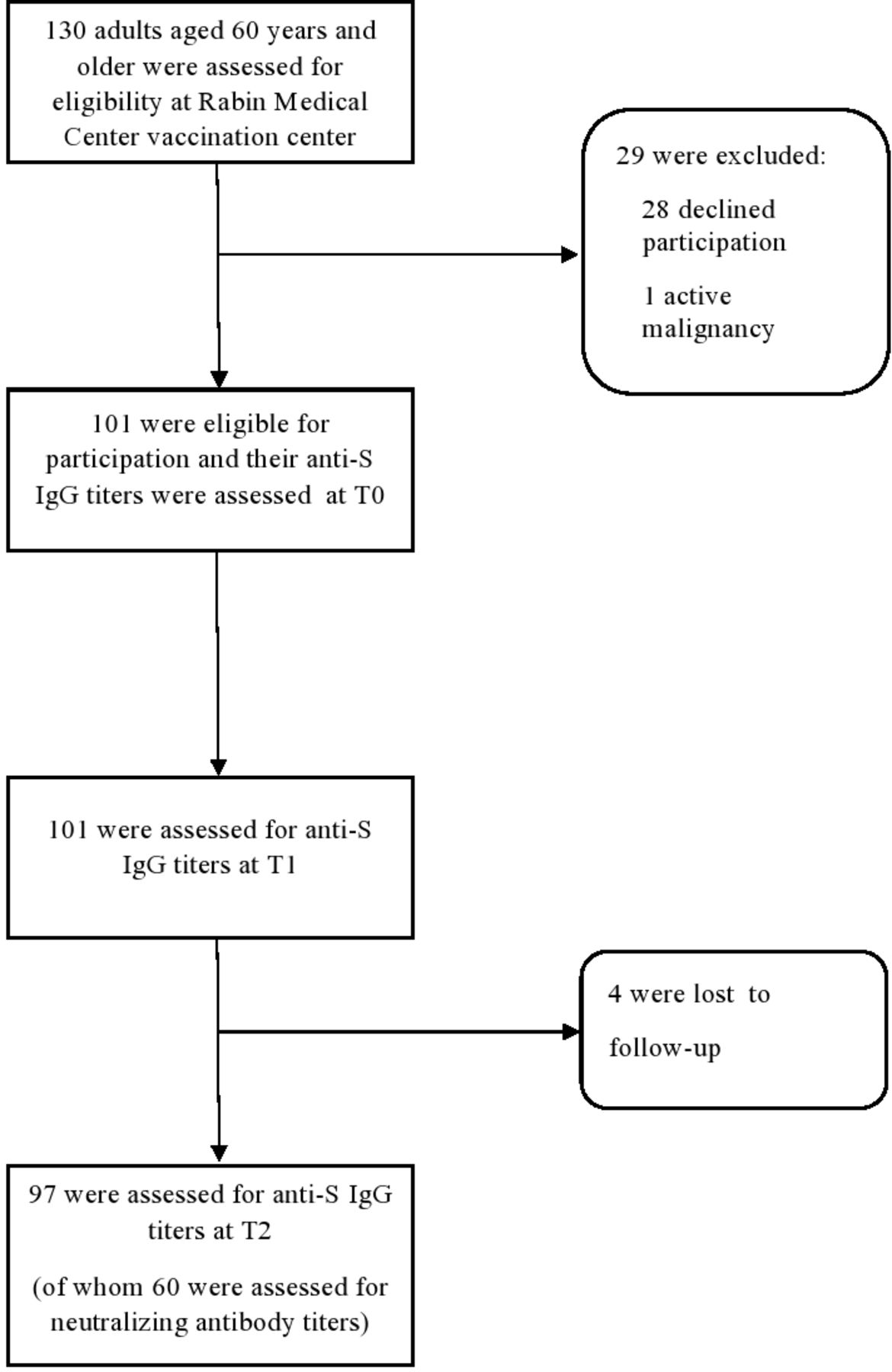
Study flow chart. Anti-S, anti-spike; T0, before the third dose; T1, 10–19 days after the third dose; T2, 74–103 after the third dose.
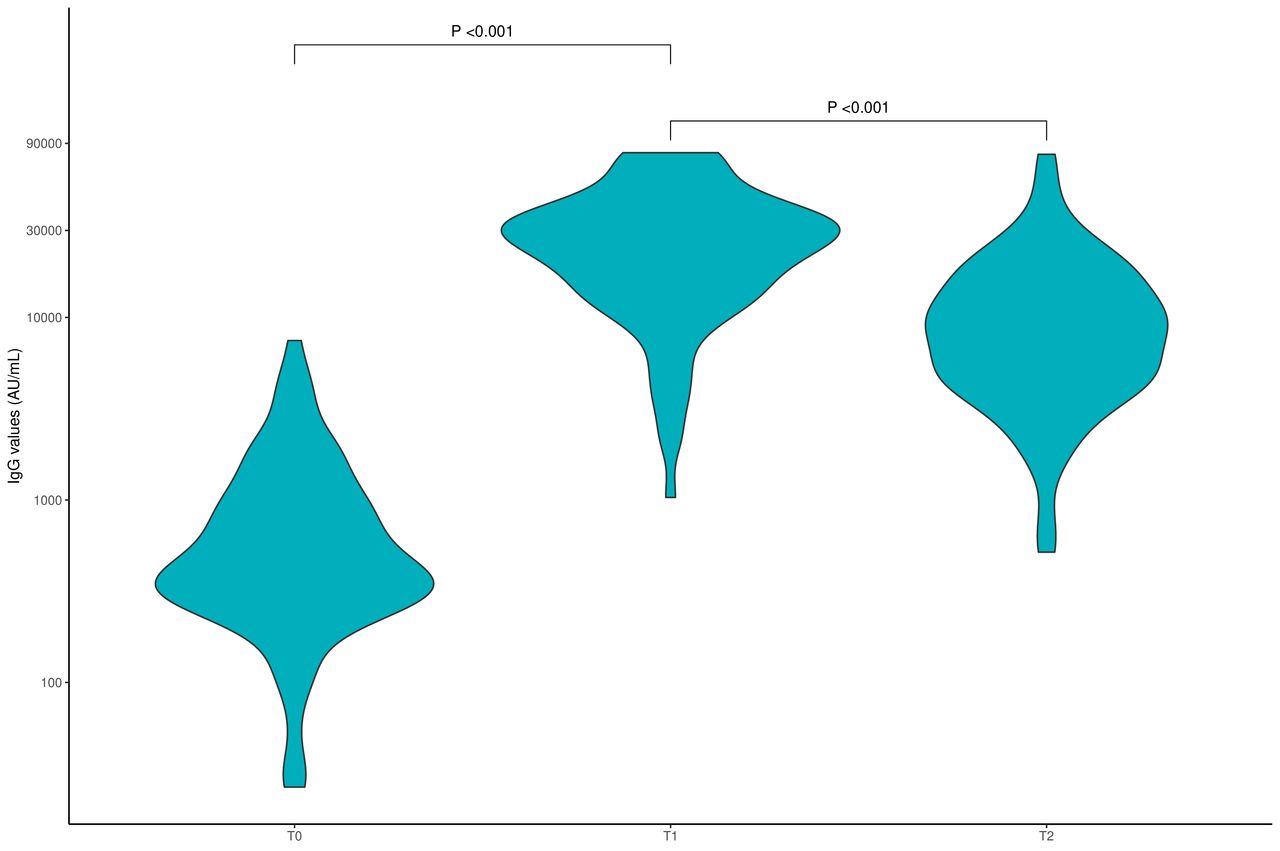
IgG titres, which increased significantly from before the third dose (T0) to a median of 14 days (IQR, 14–17) after the third dose (T1) (median of 440 AU/mL (IQR, 294–923) vs 25 429 AU/mL (IQR, 14 203–36 114); p<0.001), decreased significantly approximately 3 months after the third dose (T2; median of 94 days (IQR, 92–97) after the third dose), but all participants remained seropositive. At the T2 timepoint, the median IgG titre was 8306 AU/mL (IQR, 4595–14 701) (p<0.001 vs T1) (table 1, figure 2).

Anti-S IgG antibody titres over time. Anti-S IgG titres were measured immediately before the third BNT162b2 dose (T0), a median of 14 days (IQR, 14–17) after the dose (T1) and a median of 94 days (IQR, 92–97) after the third dose (T2). Anti-S, anti-spike; AU, arbitrary units.
In univariate and multivariable analyses, the only variable significantly associated with lower IgG levels at T2 was the number of days from the second dose of vaccine (table 2).
Univariate and multivariable analyses of log IgG values
All participants for whom neutralising antibody levels were assessed (n=60) were positive for these antibodies. The median value of neutralising antibody titre was 1294 (IQR, 848–2072). Evaluating the correlation between anti-S IgG titres and neutralising antibody titres in these participants at T2 demonstrated a positive linear correlation (r=0.6, p<0.001) (figure 3).

{kind=link}
{kind=link}
{kind=link}
Neutralising antibody titres versus anti-spike IgG titres at T2 (median of 94 days (IQR, 92–97) after the third dose of vaccine) in 60 participants for whom both assessments were performed. Area in grey represents 95% CI. AU, arbitrary units.
During the study period (median follow-up of 94 days; IQR, 92–97), no major adverse events were reported and no participant had a COVID-19 infection. No change in frailty levels was observed in any of the participants throughout the study period.
Discussion
This prospective cohort study demonstrated that anti-S IgG antibody levels increased significantly from before the third BNT162b2 dose to approximately 2 weeks after (median of 440 AU/mL vs 25 429 AU/mL). However, approximately 3 months after that dose, a significant decrease in anti-S IgG levels was observed (median of 8306 AU/mL), although all participants remained seropositive.
In patients after natural COVID-19 infection, anti-S IgG levels were shown to be sustained, or progressively but moderately declined, whereas the anti-receptor-binding domain of the spike protein (anti-RBD) IgG levels declined more commonly.15 One study showed that within 1.3 and 6.2 months of SARS-CoV-2 infection, titres of IgM and IgG antibodies against RBD decreased significantly while neutralising activity in the plasma decreased fivefold in pseudotype virus assays.16 Neutralisation antibody dynamics were similar to that of anti-RBD antibodies in other studies as well.17 18 Overall, seropositivity rates remain high (88%–90%) 6–8 months after natural infection.19
The clinical effectiveness of BNT162b2 against SARS-CoV-2 infection peaks in the first month after the second dose, declines gradually thereafter, and the decline accelerates after the fourth month.20 A recent study evaluated the long-term effectiveness of the BNT162b2 vaccine in participants of phase II–III randomised trial and found a fourfold decrease in its effectiveness between months 1–<2 and 4–7 after the second dose (from 96% to 84%).6
The durability of protection after third vaccination in healthy individuals at any age is still unknown. Understanding the extent of waning immunity is critical to public health policy making. To our knowledge, no serological follow-up beyond 1 month after the third dose has been published. The rapid waning of immunity5 prompted investigation of the durability of the immune response after the third dose in order to assist decision-making regarding additional booster vaccinations.
During the fifth wave, in January 2022, the Israeli Ministry of Health authorised a fourth BNT162b2 dose to individuals aged ≥60 years, assuming waning of immunity. Recent data on 1 252 331 persons who were 60 years of age or older and eligible for the fourth dose demonstrated the rate of severe COVID-19 in the fourth week after receipt of the fourth dose was lower than that in the three-dose group by a factor of 3.5 (95% CI 2.7 to 4.6), but this difference appeared short-lived, further questioning the decisions regarding additional boosters.21
Neutralising titres correlate with protection against infection, although the assays are complex and time-consuming.22 We found that all study participants were positive for neutralising antibodies at T2 with high titre levels and that the neutralising antibody levels were in correlation with anti-S IgG levels. Furthermore, in both univariate and multivariable analyses, the number of days from the second dose of vaccine is significantly associated with lower IgG levels at T2. Studies of other vaccines, such as for measles, mumps and rubella, demonstrated a decrease of 5%–10% in neutralising antibody levels per year.23 24 For COVID-19, the neutralisation level is highly predictive of immune protection. A recent study estimated that 50% protective neutralisation level equates to approximately 54 international units (IU)/mL (95% CI 30 to 96 IU/mL).22 Recent studies demonstrated that for those vaccinated at least 5 months earlier, a third BNT162b2 vaccine led to a rise in serum neutralisation titres by fivefold to sevenfold25 and was accompanied by 11.3-fold reduction in breakthrough infection rates.26 Comparing normalised neutralisation levels and vaccine efficacy demonstrated a strong non-linear relationship between mean neutralisation levels and the reported protection across different vaccines, including BNT162b2.22
It is well established that more than chronological age, biological age (as reflected by frailty) is significantly associated with mortality.27 In patients with COVID-19 aged 65 years and older, the CFS score was the strongest prognostic factor for mortality.2 In our cohort, the median age was 70 years (IQR, 67–74) and the participants were ambulatory adults, mostly fit, as reflected by a median CFS of 2 (‘well’) (IQR, ‘very fit’ to ‘well’). Thus, the study population was young with respect to biological age. Investigating the waning immunity in a truly frail population is warranted.
No major side effects were observed in the 3 months after the third BNT162b2 vaccine and none of the participants experienced a COVID-19 infection.
Lastly, it is impossible to discuss vaccine boosters without addressing the inherent ethical concerns. The current global environment manifests an imbalance in vaccine availability, with high-income countries delivering booster doses while low-income countries are undervaccinated with the first and second doses. Given the endemicity of this disease, waning vaccine protection and the emergence of new variants, efforts are required to expand global vaccine access rapidly.28
Study limitations include its small sample size, the lack of cellular immunity testing and the lack of neutralising antibody testing at the first two timepoints. Although accumulating evidence suggests that IgG response and neutralising antibodies are correlates of disease protection,29 cellular immunity is also suggested to play an important role in protecting against SARS-CoV-2.30 We have decided to use two models to evaluate the difference in anti-S IgG values from T0 to T1 and from T1 to T2, thus perhaps increasing the risk of type 1 error, which is an additional possible limitation.
In conclusion, in our cohort of 97 adults aged 60 years and older, 3 months after the third BNT162b2 vaccine, high levels of anti-S and neutralising antibodies were found, but with significant waning of the immune response. Although further studies are needed to advance our understanding of waning immunity, the results suggest that a third dose of vaccine for adults aged 60 years and older is effective and should be a top priority worldwide.
Data availability statement
Data are available upon reasonable request. This study is ongoing. Individual participant-level data that underlie the results reported in this article (text, tables and figures) will be shared after de-identification, following the publication of the final endpoint of this study (6-month follow-up), upon request from the corresponding author.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Rabin Medical Center (RMC) (reference number 0558-21-RMC). Participants gave informed consent to participate in the study before taking part.
References
Footnotes
NE-R and AS contributed equally.
Contributors NE-R, AS, YL-W, AN, MA, NG, NE, AB-S, AL-B, HB-Z, NM, EB-H and SMS contributed to this article. NE-R and SMS designed the trial and the study protocol. NE-R, AS, YL-W, AN, MA, NG, NE, AB-S, AL-B, HB-Z, NM, EB-H and SMS contributed to data collection. AS performed the formal analysis. NE-R, AS, YL-W, AN, MA, NG, NE, AB-S, AL-B, HB-Z, NM and EB-H had access to the data, which SMS verified. NE-R, SMS and AB-S wrote the first draft of the manuscript. NE-R, AS, YL-W, AN, MA, NG, NE, AB-S, AL-B, HB-Z, NM, EB-H and SMS reviewed the manuscript and contributed to data interpretation and revisions. NE-R, AS, YL-W, AN, MA, NG, NE, AB-S, AL-B, HB-Z, NM, EB-H and SMS had access to the data in the study, and SMS verified the data and the analysis. SMS reviewed and approved the submitted version and had final responsibility for the decision to submit the manuscript. SMS is responsible for the overall content as the guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests SMS received research grants (to the institution) from CAN-FITE, AstraZeneca, BiolineRx, BMS, Halozyme, Clovis Oncology, CTG Pharma, Exelixis, Geicam, Incyte, Lilly, Moderna, Teva Pharmaceuticals and Roche, and owns stocks and options in CTG Pharma, DocBoxMD, TyrNovo, VYPE, Cytora and CAN-FITE. AB-S is employed by BioInsight.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.