Article Text

Abstract
Introduction Due to functional defects and structural destruction after total laryngectomy, patients experienced the poor quality of life, especially for elderly. The barriers to accessing self-care in elderly patients were considered to result from complex and multifaceted interactions of biologic and social factors. Therefore, specific efforts to improve elderly patients’ quality of life are needed. The purpose of our study is to verify nurse-led coaching of elderly patient self-care approaches, which can reduce logistic burden of patients and obtain the successful functional rehabilitation ultimately.
Methods and analysis Elderly patients (n=60) scheduled for total laryngectomy will be randomly divided into the intervention group and the control group. Patients in the control group received routinely nursing during hospitalisation and thereby at home after discharge received conventional family care without regular supervision of nurses. Patients in the intervention group will receive a series of self-care intervention based on the transtheoretical model during hospitalisation. During home after discharge, nurses will additionally evaluate and supervise the self-care effect of patients. The two groups of patients’ self-care agency, self-efficacy, quality of life and nutritional status will be recorded separately at different time points. Primary outcome is the improvement of patients’ self-care agency, and secondary outcome is the improvements of patients’ self-efficacy, quality of life, nutritional states and 3-month unplanned readmission rate.
Ethics and dissemination The Ethics Committee of Hubei Cancer Hospital has approved this protocol (KYLLBA2020006). The findings of the trial will be disseminated through peer-reviewed journals, national or international conferences.
Trial registration number ChiCTR2100043731.
- quality in health care
- adult oncology
- clinical trials
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
The protocol mobilises the self-efficacy of patients before operation, focusing on patients’ autonomous mastery of self-care skills.
The close relationship between medical team and elderly patients ensures the safety and effective implementation of home self-care scheme.
The forms of promoting patients’ self-care agency are not limited to theories and atlas and also the home care diary.
Close follow-up and supervise by nurses in the intervention group may take a lot of working time when patients are at home.
Another limitation is that the trial is a single-centre small sample test, and its popularisation may be limited.
Introduction
This protocol followed published guidelines for clinical trials protocols, along with the Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT 2013 Checklist). This protocol is, V.03, written on 20 May. 2021.
Background and significance
Head and neck squamous cell carcinoma is the sixth most commonly diagnosed cancer, and its incidence continues to rise.1 2 Laryngeal squamous cell carcinoma is the second location after oral cavity squamous cell carcinoma, with the age-adjustment standardised incidence rate was 3.6/100 000 for men and 0.5/100 000 for women, the age-adjustment mortality rate is 1.9/100 000 for men and 0.3/100 000 for women.3 Total laryngectomy (TL) offers a curative approach for patients with advanced laryngeal cancer or hypopharynx with the invasion of thyroid or cricoid cartilage and extra laryngeal soft tissues, failed response to radiotherapy or chemoradiotherapy and extensive tumours of histologic entities not suitable for conservative treatment.4 5 It is well known that patients often experience specific symptoms, such as swallowing and speech impairments, given the complex nature of everyday functions and the anatomical complexity within the larynx area, despite in who long-term survival was achieved. Indeed, with the increase in incidence and improved survival rates, more patients are confronted with numerous, profound physical and emotional disabilities owing to insufficient residual tissues and regional structural destruction,6 following TL treatment, which can also affect patients’ families and are often present long term.
The health problems of patients with TL are reflected in all aspects of social life.7 Physiological changes of tracheotomy8: permanent tracheostomy changes their respiratory tract, causing function loss of swallowing and language, dry mouth, cough, shortness of breath and a reduced sense of smell. Social pressure caused by the change of body image9: the stigmatisation of tracheostomy and the change of body image leads to patients’ self-closed, decreased self-esteem and stigmatising, resulting in the limitation of work scope. It is obvious that the physical and mental changes and social embarrassment brought by TL seriously affected patients’ quality of life (QoL).10 11 At present, some scholars have conducted research on early rehabilitation exercise based on network or self-help for patients with TL and achieved positive results.10 12 It is suitable for patients with high educational level and could master electronic equipment freely. Elderly patients, who typically have more functional impairments or comorbid conditions and various obstacles in communication (such as deafness, and lack of medical general knowledges), the opportunity to participate in high-quality self-care (SC) is often limited. The barriers to accessing SC in elderly patients were considered to result from complex and multifaceted interactions of biologic and social factors, often involving medical provider, patient and family caregivers, especially the lack of communication between patients and care providers after discharge. It goes without saying that their QoL and survival rate have not improved significantly.13 In view of this, this study attempts to develop a pictorial exercise manual and exercise diary to improve the understanding of elderly patients with laryngeal cancer and the compliance of home SC, reduce the disease burden of patients and family caregivers and promote the successful functional rehabilitation of elderly patients with TL.
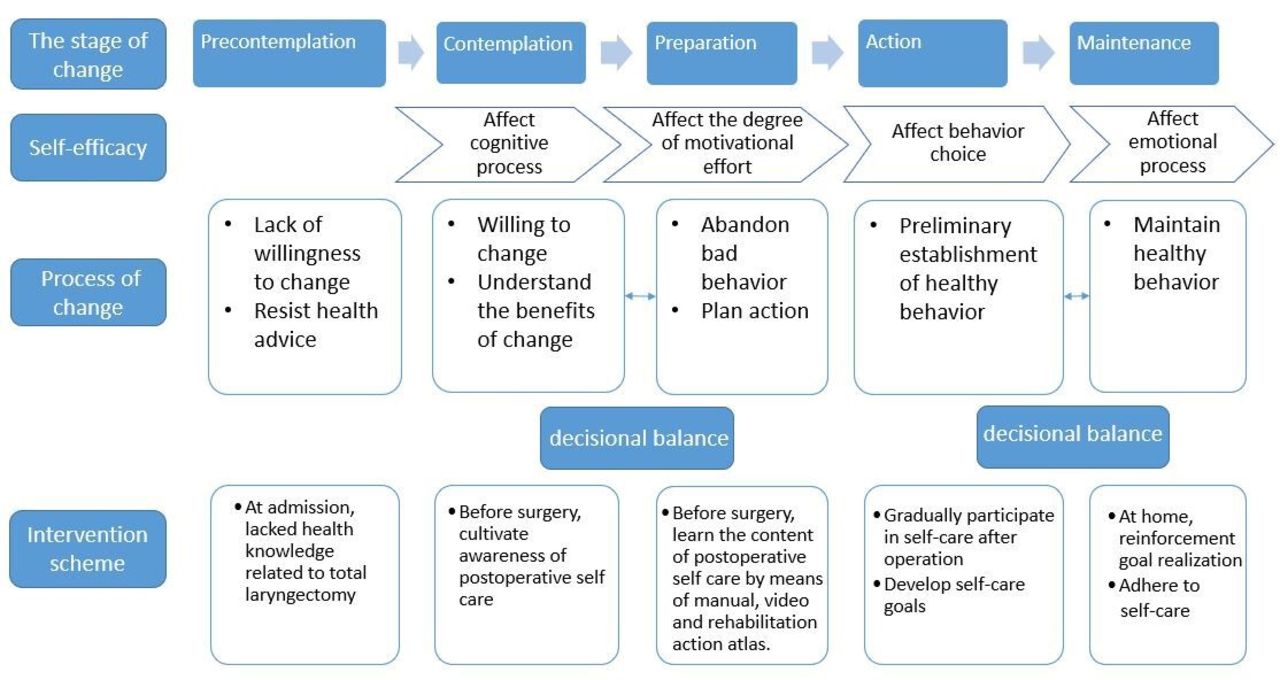
The specific SC education and exercise programme targeted to elderly patients with TL had been developed according to the transtheoretical model (TTM), which is first proposed by Prochaska14 (figure 1). This theory is based on social psychology and focuses on the process of individual needs and behaviour changes, by psychological, personal, family, social and other aspects of guidance and intervention on unhealthy behaviour, aims to promote health management behaviour and the formation of healthy lifestyles of patients. SC ability refers to a kind of health management behaviour derived from oneself, which core is to mobilise the subjective initiative of patients through effective external intervention, reduce their sense of uselessness and inferiority, to improve their body function and health status by promoting their own physical condition assessment, care and monitoring. Undoubtedly, effective SC is a dynamic process in which patients gradually change from passive behaviour to active participation in rehabilitation promotion,15 16 and it will have benefits for the rational use of nursing resources and the alleviation of logistic burdens, especially the elderly patients with weak economic income.

Study theoretical framework diagram.
Objective
In this study, through preoperative elderly patients’ SC awareness cultivation, SC knowledge training, postoperative one-on-one rehabilitation guidance by nurse-led based on the theoretical framework of TTM,14 to explore whether this systematic SC intervention programme developed by our research group can improve the postoperative SC ability of TL elderly patients, promote the persistence of SC healthy behaviour, improve QoL and functional outcomes.
Methods and analysis
Study design
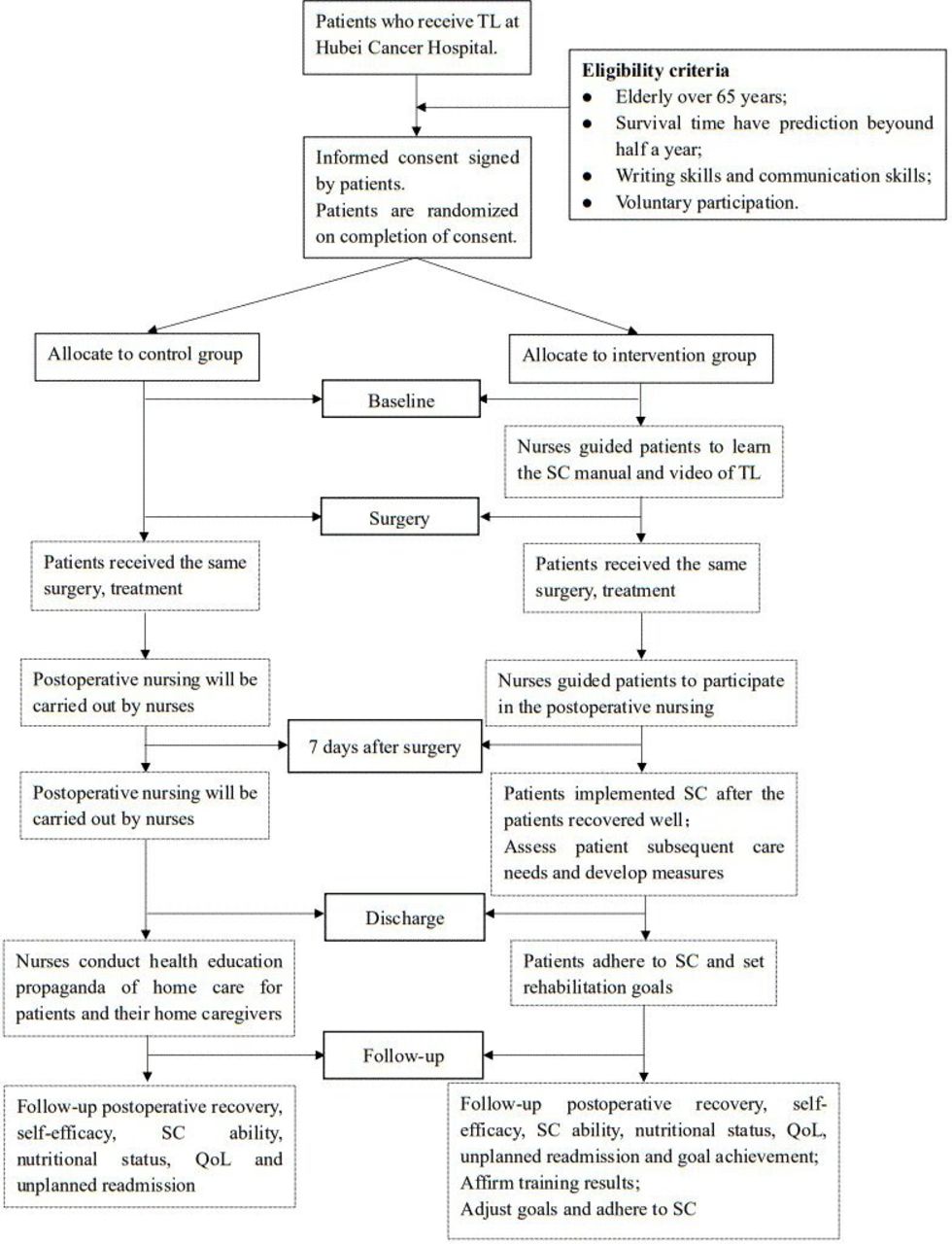
It is a single-centre randomised controlled study, with 60 patients will be randomly divided into two groups (the intervention group and the control group) after admission to Department of Head and Neck Surgery, Hubei Cancer Hospital (Wuhan, China) in 1 March 2021, ending in 30 September 2022. The first admission doctor is responsible for recruiting the participants after obtaining the informed consent of the patients in the study. The trial flowchart is shown in figure 2.

{kind=link}
{kind=link}
Flowchart. QoL, quality of life; SC, self-care; TL, total laryngectomy.
Patient and public involvement
Neither patients nor the public were involved in the design, conduct, reporting or dissemination plans of this research.
Randomisation procedure
Participants meeting the eligibility criteria will be randomly assigned to control group or intervention group with a 1:1 ratio using random number table according to the time patients admitted to hospital. The randomisation numbers were sealed in the opaque envelopes numbered in sequence, which were put in the head nurse’s office. The head nurse is directly responsible for assigning patients to nurses in the intervention or control group.
Participants
Sample size
To verify that the effect of SC intervention on the QoL of patients after TL, we designed a random control test with α=0.05, β=0.20 (a power of 80%). According to the calculation formula of sample size , considering a 20% loss of follow-up rate, no less than 60 participants.
, considering a 20% loss of follow-up rate, no less than 60 participants.
Eligibility criteria
Patients eligible for study participation met the following inclusion criteria: (1) were admitted to hospital with laryngeal malignancy diagnosis and TL was planned, (2) the survival time is expected to be more than half a year, (3) elderly over 65 years without obvious disability, (4) have certain reading and writing skills and communication skills. After receiving informed consent, patients were asked to fill out some questionnaires.
We will exclude patients with obvious defects in SC ability, such as (1) concurrent cancer; (2) severe heart, liver, kidney and other organic diseases, coagulation dysfunction; (3) suffering from other psychological or mental diseases in the treatment stage.
Implementation intervention
All eligible patients will be randomly assigned in a 1:1 allocation ratio to the control or intervention group. Participants in both groups will undergo similar treatment and nursing, but the intervention group patients will receive additional SC skill intervention from nurses to try SC during hospitalisation and continue to implement SC during home after discharge, under the continuing guidance of nurse-led health providers.
Preparation before intervention
Establish SC intervention team. The intervention team consisted of qualified members in professional fields, including a project leader (head nurse of head and neck surgery), two head and neck surgeons, one radiation therapist and eight nurses involved in rehabilitation, psychology and nutrition. The project leader is responsible for carrying out project training and project emergency plan to ensure that all team members implement it according to the project process. Doctors are responsible for disease diagnosis, patient admission control, formulate prescription and handling complications and adverse events (AEs); nurses are responsible for the implementation of the plan, supervising and recording patient feedback.
Determine the intervention scheme and form the home SC manual (see online supplemental materials for details) for patients with TL. After two rounds of expert consultation, the intervention scheme was determined, and the home SC manual (including some videos of SC) for patients with TL was established. The intervention scheme is detailed in the intervention process. The home SC manual mainly includes SC knowledge and SC diary. The SC knowledge includes trachestomy annular tube care, respiratory, swallowing and neck function training and nutrition management after TL; the SC diary includes the records of trachestomy annular tube care, respiratory, swallowing and neck function training and nutrition management.
Intervention content training on team members. The training audiences of four face-to-face meetings were doctors, nurses in the intervention group, nurses in the control group and data collector, which lasted for 2 weeks. The qualifications, training contents and job responsibilities of team members are shown in table 1.
Supplemental material
Team numbers training
Intervention process
Once the patient informed consent is signed, the whole process of nursing was carried out by a nurse from admission, perioperative nursing, discharge, first month follow-up, third month follow-up to the end of sixth month follow-up. The detailed scheme of the two groups is shown in table 2.
Two groups of implementation scheme
Control group scheme
Doctors are mainly responsible for the assessment of the disease, the answer of disease-related knowledge, the evaluation of rehabilitation effect and other medical related questions. Nurses implement routinely nursing for patients with TL, including admission education, preoperative preparations, postoperative tracheal tube nursing (online video), feeding diet guidance, medication nursing, psychological nursing, discharge health education (including rehabilitation training exercise) and regular follow-up, etc and thereby at home after discharge patients received conventional family care without regular supervision and guidance of nurses.
Intervention group scheme
Doctors are mainly responsible for the assessment of the disease, the explicate of disease-related knowledge, the evaluation of rehabilitation effect and other health-related questions. Nurses explain the concept of SC 1–3 days before operation, so that patients can understand the importance of SC, establish SC awareness, understand the content of postoperative SC; 3–7 days after operation, while nurses implement postoperative nursing, they guide patients to gradually master SC methods and skills one-on-one; 2–3 days before discharge, nurses evaluate the patients’ subsequent care needs, guide patients to SC management at home, adhere to rehabilitation exercise and assist patients to set home rehabilitation goals; within 6 months after discharge, nurses follow-up the patients’ SC management at home: evaluate patients’ postoperative recovery, nutrition, goal achievement of the previous stage and individualised guide to the goal setting of the next stage.
Blinding
In the whole intervention stage, the blinded doctors take the same medical service to the two groups of patients. The data collector is also unaware of the grouping of patients.
Measurement
As outcome variables, we assessed TL elderly patient SC agency level, self-efficacy, nutritional status and QoL at baseline, 7 days, 1 month, 3 months and 6 months after TL. These measurements are freely available in the public domain in China. In addition, we will count the unplanned readmission rate. All outcomes were assessed by a data collector who was unaware of the patients’ group allocation.
Patient SC agency level will be assessed with exercise of SC agency scale17, which consists of four dimensions: SC skills, SC responsibility, self-concept and health knowledge level. The half reliability of the scale was 0.77 and the test–retest reliability was 0.80~0.81. There are 43 items in total. The sum of the scores of each dimension is the total score. The higher the score, the higher the SC ability.
Patient self-efficacy will be assessed using general self-efficacy scale (GSES),18 which was sinicized by Schwarzer, was used to measure the self-efficacy. The scale was derived from the German psychologist Ralf Schwarzer,19 and its Cronbach’s α was 0.87, and the test–retest reliability was 0.83, the half reliability is 0.82, and the Chinese version GESE of Cronbach’s α is 0.75~0.91. There are 10 items in the scale, which were scored by Likert grade 4, all of which were positive scores. The higher the score, the stronger the general self-efficacy.
NRS-2002 (Nutritional Risk Screening 2002)20 was recommended as a nutritional risk screening tool with good predictive validity and content validity by European Society for Parenteral and Enteral Nutrition. PG-SGA (Patient-Generated Subjective Global Assessment)21 was first proposed by Ottery in 1994, which is a nutritional status assessment method specially designed for patients with cancer, the reliability and validity were higher than 0.7 in Chinese cancer population.
Patient QoL level will be assessed by QoL instruments for cancer patients-head and neck cancer22, which is a scale suitable for Chinese cultural background and clinical practice of cancer treatment, the Cronbach’s α of all dimensions was above 0.7. It is suitable to evaluate the QoL of patients with head and neck cancer in clinical work. The scale includes five dimensions: physical function, psychological function, social function, common symptoms and side effects and specific symptoms, which are composed of 7, 12, 6, 7 and 14 items respectively, with a total of 46 items. The higher the score, the better the QoL.
Data collection, management and analysis
Data collection
Once the patient informed consent is signed, a fixed data collection nurse is responsible for data collection, who does not know the grouping of patients, during the whole process to avoid the bias resulted from heterogeneity evaluation. The contact information and address of patients will be confirmed before hospital discharge. The fixed nurse collects data throughout the whole process independently, such as baseline data, clinical observation data and three follow-ups at 1, 3 and 6 months after operation questionnaire data (QoL/ Self-efficacy/ Self-care agency/ NRS-2002/PG SGA). All study data will be saved in an Excel 2015 (V.16.0.3601.1023) by the data collection nurse.
Statistical analysis
The data transmitted by the data collection nurse are saved and analysed by the data analyst. All the analyses were performed using SPSS statistical software (IBM V.22.0). We used descriptive statistics and constituent ratio to analyse the demographic data, self-efficacy, SC agency, nutritional status, health outcomes and unplanned readmission of participants. Normally or non-normally distributed continuous data will be compared by independent samples t test or the Mann-Whitney U test, and the Χ2 test will be used to compare categorical variables of the intervention and control groups. Generalised repeated measures analysis of variance will be used to demonstrate the effect of intervention and the time×intervention interaction. A value of p<0.05 will be considered significant (two tailed). An intention-to-treat analysis was performed, and missing data were analysed by the last observation-carried forward method.
Data statement
The data will be publicly approved by Resman in 6 months after the end of the trial.
Ethics and dissemination
Ethics approval
The study procedures and informed consent form have been approved by the Ethics Committee of Hubei Cancer Hospital in Hubei province, China (reference number KYLLBA2020006). The Ethics Committee is obliged to periodically evaluate the progress of this trial and track information on any AEs until the patient reaches a stable state. The doctors communicate with patients to ensure that participants’ information is anonymous and inform patients to sign the informed consent. Results will be disseminated in peer-reviewed journals and conferences, and sent to participating practices.
Discussion
With the diversification of treatment, the survival rate of laryngeal malignancy patients is increasing. Although the medical staff try their best to carry out diagnosis, treatment and nursing in the hospital, the home rehabilitation of patients after discharge is not enough due to the limited medical human resources. After TL, patients complete lung ventilation through the tracheal stoma, which is located in front of neck, this special position determines the importance of postoperative SC. In order to achieve active rehabilitation and high QoL, it is still necessary to take measures to promote patients’ self-rehabilitation management ability.
TTM theory was initially applied to the intervention of quitting smoking behaviour in a wide range of people and gradually developed to clinical management and group intervention, especially the management of patients with chronic diseases in recent 20 years.23 24 Relevant studies25 26 show that intervention based on TTM theory can effectively improve patients’ self-efficacy. In view of this, we propose a research hypothesis: SC intervention based on TTM will have a positive impact on self-efficacy and SC ability of patients undergoing TL. This study will evaluate patients’ self-efficacy, SC ability, QoL and nutritional status at 7 days, 1 month, 3 months and 6 months after operation. These time points are important time nodes for changes in patients’ SC ability, QoL and nutritional status. They are also consistent with the routine follow-up time of patients, ensuring a high follow-up rate.
For self-efficacy and QoL, Perry et al27 evaluated the self-efficacy score and QoL of TL survivors. The result showed that the self-efficacy score of TL survivors is higher than the normal level, although the survivals have lower QoL due to stigmatisation of airway fistula, significant changes in voice, destruction of self-image. However, this study has a limitation, that is, all the data are from long-term survivors, who have participated in the rehabilitation association, which may be an important factor affecting the level of self-efficacy. Moreover, this is data from a cross-sectional study. On the contrary, our study is a prospective assessment of QoL at important time points, and we hope this study can provide further evidence for the results.
Cnossen et al’s10 team developed a set of SC application to investigate the feasibility and satisfaction of online SC education for early postoperative rehabilitation of 55 patients with TL. The results showed that this application is basically feasible, and the use experience satisfaction of follow-up patients is high, although it is accompanied by high loss of follow-up. However, there are many other outcome variables worth exploring. Different from the above study, our study proposes to start early SC ability intervention before operation by the systematic SC manual based on the TTM, which is more convenient for the elderly to read. We expect that our results will exceed the effect of previous studies, because their research does not fully mobilise the enthusiasm of patients. Based on the improvement of patients’ self-efficacy and SC ability, we expect that their QoL and nutritional status will also be greatly improved half a year after surgery.
We hope that all patients with TL will have the opportunity to benefit from the SC programme. For this purpose, we designed SC intervention scheme. Our aim was to evaluate the impact of SC intervention on SC agency and QoL of patients with TL, especially self-management of tracheostomy and nutritional problem management. If the research proves that SC intervention can effectively improve the self-efficacy and SC agency of patients with TL, it may provide reference for health providers to develop rehabilitation nursing programme for patients with TL. Results from the protocol may provide the evidence of high-quality continuous nursing of oncology nurses, to optimally rearrange the continuous nursing responsibilities of oncology nurses and consequently improve the health outcomes of patients with TL.
Research ethics approval
This study is approved by the Ethics Committee of Hubei Cancer Hospital (KYLLBA2020006).
Ethics statements
Patient consent for publication
Acknowledgments
Thanks to Hubei Province health and family planning, Hubei Cancer Hospital, head and neck surgery colleagues for their support.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors CX proposed and designed the research and participated in the guidance of this research. HW, JC, ZM, LW, YQ and XL tested the feasibility of the study; ZL, LZ participated in the literature search; SL, DP, XL, YL, SY and YL are the main nurses who will perform nursing measures in the intervention group; LZ formulated the intervention program design, the intervention files, SC diary for elderly patients after total laryngectomy and wrote the manuscript. All authors approved the final version of the manuscript.
Funding This research was financed by the funds of Hubei Province health and family planning scientific research project [WJ2021M191].
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.