Article Text

Abstract
Objectives Learning health systems (LHS) integrate knowledge and practice through cycles of continuous quality improvement and learning to increase healthcare quality. LHS have been conceptualised through multiple frameworks and models. Our aim is to identify and describe the requisite individual competencies (knowledge, skills and attitudes) and system competencies (capacities, characteristics and capabilities) described in existing literature in relation to operationalising LHS.
Methods A scoping review was conducted with descriptive and thematic analysis to identify and map competencies of LHS for individuals/patients, health system workers and systems. Articles until April 2020 were included based on a systematic literature search and selection process. Themes were developed using a consensus process until agreement was reached among team members.
Results Eighty-nine articles were included with most studies conducted in the USA (68 articles). The largest number of publications represented competencies at the system level, followed by health system worker competencies. Themes identified at the individual/patient level were knowledge and skills to understand and share information with an established system and the ability to interact with the technology used to collect data. Themes at the health system worker level were skills in evidence-based practice, leadership and teamwork skills, analytical and technological skills required to use a ‘digital ecosystem’, data-science knowledge and skill and self-reflective capacity. Researchers embedded within LHS require a specific set of competencies. Themes identified at the system level were data, infrastructure and standardisation; integration of data and workflow; and culture and climate supporting ongoing learning.
Conclusion The identified individual stakeholder competencies within LHS and the system capabilities of LHS provide a solid base for the further development and evaluation of LHS. International collaboration for stimulating LHS will assist in further establishing the knowledge base for LHS.
- Health informatics
- HEALTH SERVICES ADMINISTRATION & MANAGEMENT
- Quality in health care
Data availability statement
No data are available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
Review of 13 years worth of publications relating to learning health system competencies.
Identification of requisite competencies across multiple levels of analysis.
Review includes only articles published in English and published between January 2007 and April 2020.
The following publications were excluded from this review: book chapters, commentaries, editorials or conference proceedings.
Introduction
Since first proposed by Etheredge in 2007 as a system to ‘quickly develop new evidence for daily medical practice and policy’, thereby ‘increasing the value of health care’ (p107), the learning health systems (LHS) concept has been conceptualised through multiple frameworks and models.1 The LHS concept has spread globally, with publications focusing on process models, micro to meso to macro system levels of analysis, infrastructure requirements to achieve such systems, the values underlying the cultural shift required to achieve such systems and case studies exploring the application of the concept within healthcare.2 3 However, there is a paucity of evidence indicating the effectiveness of LHS across levels of analysis. Moreover, there is a need for increased understanding of the requisite competencies and capabilities across levels of a system that promote learning and continuous quality improvement.
Conceptualisations of LHS have increased in their specificity over time. Initially, the Institute of Medicine envisioned LHS as ‘systems where science, informatics, incentives, and culture are aligned for continuous improvement and innovation with best practices seamlessly embedded in the delivery process and new knowledge captured as an integral by-product of the delivery experience’ (pix).4 Friedman and colleagues further specified the conceptualisation by defining each component word. ‘Learning’ refers to the ‘capability for continuous improvement through the collection and analysis of data, creating new knowledge, and the application of the new knowledge to influence practice’ (p1).5 ‘Health’ is defined as both an ‘end-goal’ or ‘universally recognized benefit to humanity’ as also a ‘domain of human endeavor’.5 Finally, according to Friedman et al ‘a system consists of component parts acting in unison to achieve goals not attainable by any subset of the components’ (p1).5 Correspondingly, self-monitoring and improving performance through continuous cycles of learning-supported by people, policy and processes-transforms health systems into LHS.5 6
Menear and colleagues recently provided a framework for LHS which suggests that in order to encourage learning and improvement within a system, four main components are required—core values, pillars and accelerators, processes, and outcomes.3 The conceptual framework explicates the need for change to occur within each level of the system (micro, meso, macro) and within the geographical areas for which the system acts (regional, national and international) and provides details on the components of the pillars and processes needed to lead to outcomes defined previously as the quadruple aim to optimise healthcare. However, the framework does not delineate the competencies and skills necessary for the individuals within a system, capabilities of the system itself or capabilities of networked systems (either on a national or international scale) that would result in an effective and efficient LHS.
Recent literature has begun to investigate the requisite competencies and skills needed to build LHS. Forrest presented a core set of 33 competencies for researchers embedded in LHS categorised into seven domains that included (1) systems science, (2) research questions and standards of scientific evidence, (3) research methods, (4) informatics, (5) ethics of research and implementation in health systems, (6) improvement and implementation science and (7) engagement.7 However, further identification of the personal competencies (knowledge, skills and attitudes) required of other stakeholders within LHS remain in question. Although we have conceptual frameworks to rely on that identify general areas of knowledge, skill and abilities mostly at a system and theoretical level, there is little research identifying the specific competencies required by the individuals within the LHS and how they develop and guide the processes needed to develop and assess appropriate outcomes.
Finally, there has been a significant increase in the available literature that should be integrated into our current understanding of LHS competencies. Prior literature indicates that stakeholders within LHS require specific knowledge and abilities to engage in continuous cycles of learning and that systems require specific capabilities, capacities and characteristics to support said cycles. Correspondingly, this scoping review aims to identify and describe the requisite individual competencies (knowledge, skills and attitudes) and system competencies (capacities, characteristics and capabilities) described in existing literature in relation to operationalising LHS.
Methods
Given our interest in identifying and mapping the characteristics of LHS for individuals and systems, we elected a scoping review to answer our research question. In conducting the review, we used Arksey and O’Malley’s five-stage process of performing a scoping review: identifying the research question; identifying relevant studies; selecting studies; charting data; and collating, summarising and reporting findings.8 The Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews checklist guided the writing of the study report.9 This checklist can be found in . The following research question guided this scoping review: ‘How has existing literature described requisite individual competencies and system competencies for operationalizing LHS?’.
Identifying relevant studies
We conducted a scoping review using both MESH and free-text terms “learning health system*” OR “learning healthcare system*” OR “learning health care system*”) AND (“competence*” OR “standard” OR “proficienc*” OR “capacities” OR “characteristics” OR “capabilities” OR “knowledge” OR “skills” OR “attitudes.” Searches were limited to English language studies and the period between January 2007 and April 2020. Databases searched included PubMed, CINAHL and Scopus. Publications were excluded if they were book chapters, commentaries, editorials or conference proceedings. Further, if an article did not describe LHS competencies, it was also excluded.
Titles and abstracts were screened by a team of four reviewers, split into two teams of two (PLM and KH; JM and PJvdW). The teams reviewed the articles using the agreed on inclusion and exclusion criteria. Disagreements between reviewers were resolved by consensus and the reasons for exclusion were noted.
Data extraction was conducted in the same two-person teams as article selection. The articles were divided between the two teams; each team read the full text of articles assigned prior to data extraction. Online supplemental appendix 2 presents the data extraction template the team created to guide data extraction including article identifiers, such as author, year of publication, originating discipline and article type. Data were extracted by the members of the two-person teams individually and verified through team discussions. In addition to the identifying data extracted for each article, the researchers focused on extracting the individual and system level competencies identified within each article. They further subdivided the level of individual competencies into two broad groups of stakeholders: individuals or patients as recipients of healthcare and individuals working within the healthcare system.
Supplemental material
We began with a descriptive analysis summarising the number (count) of articles published per year, level of analysis (individual/patient, health system worker, system) and number of articles by study location. To address the aim of the review, the two-person teams summarised the major findings of each study. Summary statements were then organised into individual/patient, health system worker and system level. Finally, a thematic analysis was conducted, by developing themes within each level using a consensus process and several rounds of discussion until agreement was reached among team members.10
Patient and public involvement
There were no patients involved in this research.
Results
Study selection
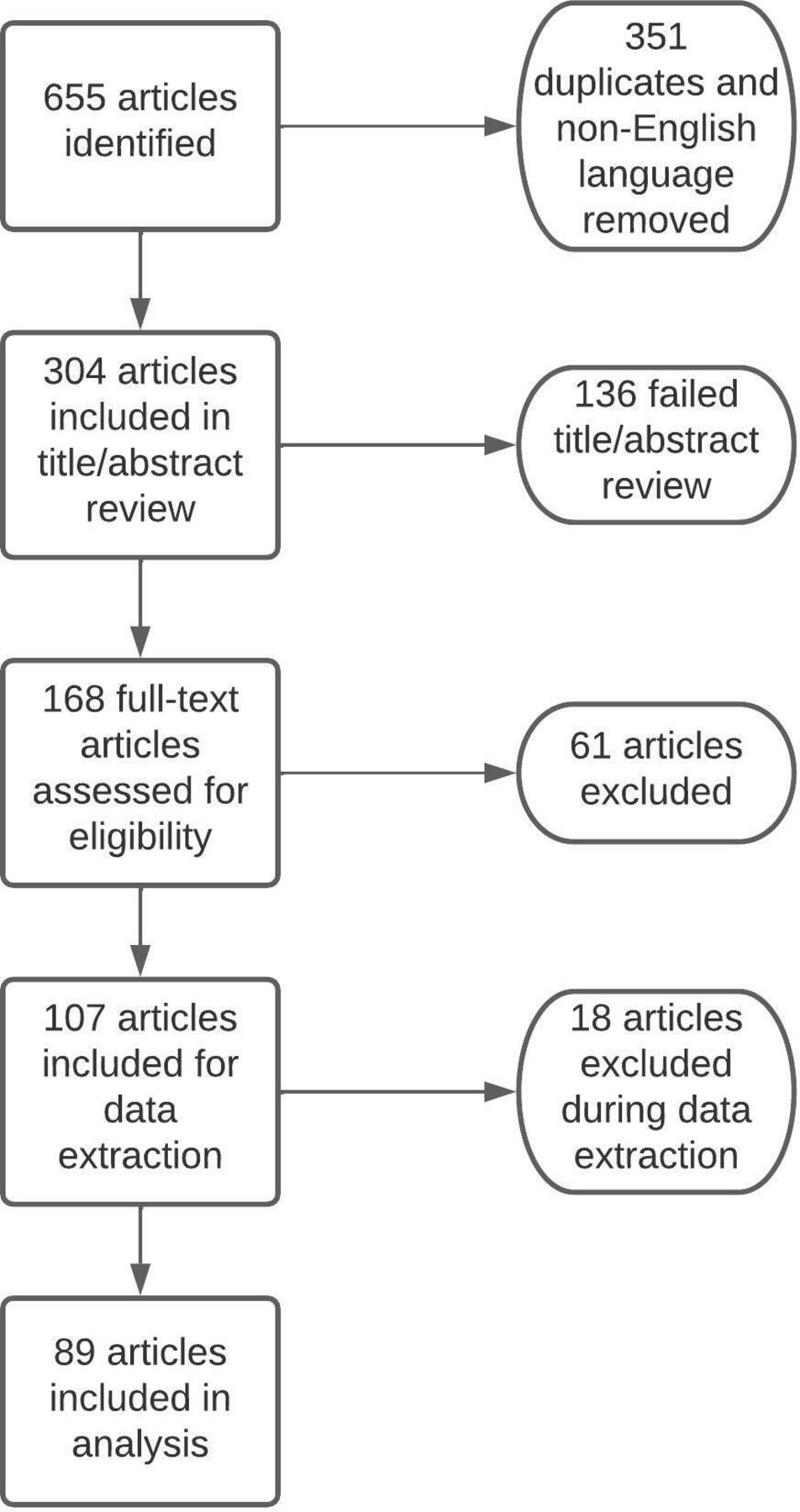
The initial search yielded 655 articles. After the removal of duplicates and non-English language articles, a total of 304 articles underwent title and abstract review. Removal of editorials, commentaries, book chapters and conference proceedings, left 168 articles that were uploaded into Covidence to undergo full-text review. Sixty-one articles were excluded based on predefined exclusion criteria. One hundred and seven articles were included for the data extraction portion of this review. Given our goal to identify published individual and system level competencies, articles were organised into ‘patient’, ‘health system worker’ and ‘system’ level competencies. System level competencies included both organisational and inter-organisational (networks of organisations or national and international systems) levels. An additional 18 articles were excluded at this final stage, as they did not discuss specific competencies related to LHS. This resulted in the final inclusion of 89 articles in this scoping review (see online supplemental appendix 3). Figure 1 depicts the search decision flowchart during the scoping review.
Supplemental material

Search results.
Descriptive analysis
Most of the studies were performed in the USA and the UK with different European countries contributing a few relevant articles. In addition, there was a growing level of interest in LHS from 2013 onward, as shown in figure 2.

Number of articles published per year.
During our assessment of the originating country of the articles, we noted the increased interest in LHS from North America and Western Europe, with a lack of publications coming from the Asia-Pacific region, as shown in figure 3.

Number of articles published by country.
This scoping review considered requisite competencies by level of analysis; correspondingly, figure 4 presents the number of publications by level of analysis. In our analysis, we isolated those articles that focused solely on one level of analysis and those that represented combined levels of analysis or addressed competencies at more than one level. As indicated by the figure, the largest number of publications represented competencies at the systems level alone. The next highest level of articles related to those indicating both system and health system worker competencies.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Number of publications by level of analysis.
Thematic analysis
Individual/patient level
Three articles were identified in the scoping review that addressed individual/patient level competencies for engaging in LHS. Two articles addressed the knowledge and skills of individuals/patients required to access and understand health-related information and to understand and share information with an established system, including the need for explicit directions and instructions for sharing.11 12 Fore and colleagues emphasised the importance of a patient’s ability to interact with the technology used to collect data. One article addressed the ability of patients to partner with physicians on research.13
Health system worker level
Of 89 articles reviewed, 21 addressed competencies required of healthcare system workers working in an LHS. Themes identified within this literature related to skills required of health system workers were skills in evidence-based practice, leadership and teamwork skills, analytical and technological skills required to use a ‘digital ecosystem’, data-science knowledge and skill and self-reflective capacity. Ten articles addressed practitioner-related competencies, with early work done in the field of nursing.14–23
Early work emphasised skills in evidence-based practice.14 21 These skills included the ability to use guidelines and quality improvement programmes for evidence-based practice, the ability to use electronic health record (EHR) data to assess quality and provide quality care and the ability to use practice guidelines and clinical decision support (CDS) for evidence-based practice.14 21 Newhouse further discussed the ability to model these skills in practice.21 Subsequent publications focused on the analytical and technological skills (computer and information technology) required to use a ‘digital ecosystem’ and the data science knowledge and skills required to access and make-sense of the data from EHR systems.16 20 22 23 Early work in the field of nursing highlighted the requirement for leadership skills to move data into clinical practice by fostering an appreciation of data and information.14 Several subsequent articles focused on other leadership skills required of practitioners in LHS, such as skills in collaboration and teamwork, motivation and engagement and self-reflective capacity.18–20 22 24
Three articles focused on competencies required of researchers embedded in LHS.7 25 26 Reid’s work proposed researchers partner with stakeholders across the health system (leaders, managers, analysts and clinicians) on all phases of a learning cycle,25 requiring skills in analysing health services delivery systems for problems and synthesising evidence related to solutions; applying solutions appropriate to the content and assisting with key system modifications or redesigns; assigning with executing, spreading and evaluating implemented changes; identifying required adjustments; and disseminating findings beyond the organisation. With regard to producing and conducting evidence reviews, specify that researchers must be able to develop a review scope and identify key questions important to multiple stakeholders and subsequently engage a variety of stakeholders in the review process.26 As noted in our introduction, Forrest et al identified seven domains comprising 33 competencies for researchers embedded in LHS.7 These domains address general competencies required of researchers embedded within any health system (application of appropriate research methods and standards of scientific evidence and ethical conduct of research); however, these domains have been interpreted from the lens of applying the competencies to investigate LHS.7 For example, the definition of the domain of ‘Research Questions and Standards of Scientific Evidence’ is defined as ‘to ask meaningful questions relevant to health systems stakeholders and evaluate usefulness of scientific evidence and insights’ (p2623).7 The domains also extend to unique requirements of researchers embedded in LHS not always associated with other embedded researchers (knowledge and application of systems science, informatics, improvement science, and implementation science).7
System level
Most articles in this review (64 of 89) addressed requisite system level competencies for LHS. Articles within this review noted that a mature LHS would have the capability to use diverse and integrated data for multiple purposes, namely developing CDSs for patients and clinicians to make good evidence-based decisions27–32; supporting quality improvement and continuous learning within and among systems27–29 31 33–41; supporting ethically sound research that is integrated into practice and enhances knowledge27 29 37 39 40 42 43; and developing sound and evidence-based healthcare and social policy.32 34 44–48
The thematic analysis resulted in three themes reflecting major areas of competence that would allow the system to address the multiple purposes required in a mature LHS. The themes include: (1) data, infrastructure and standardisation; (2) integration of data and workflow; and (3) culture and climate supporting ongoing learning.
Data, infrastructure and standardisation
Several articles emphasised that systems need the capability to provide access to real-time, secure data with integrated data infrastructures and EHR interoperability that captures patient care experiences digitally and is accessible from multiple locations and harmonised at the system level.35 47–52 Other authors suggest that systems need the capability to access big data from multiple sources including national clinical trials databases, population-based data and national and international databases.28 29 32 35 53 54 Data sharing across access points within the system was a commonly recognised required capacity.18–20 23 25 29 32 36 37 44–53 55 56 Usable and flexible data sharing among local stakeholders (clinicians, researchers and patients) was emphasised with special emphasis on the ability to share data across silos and networks without regulatory and institutional barriers.43 46 47 49 56 Several authors recommended national level systems for monitoring data access and transfer across different settings.26 54
Numerous articles suggested specific technological capabilities required for data access and management in a mature LHS.16 22 28–30 35 36 43 45–47 54–60 A sound technological infrastructure (at the organisational and inter-organisational levels) is required to support health data collection, access, interoperability and exchange.35 46 47 58 59 The infrastructure should ensure that data are easily available for many uses and purposes and supplied ‘to the right person at the right time’.23 29 30 36 43–47 61–63 Technological systems must have the capacity to manage information from clinical entities to facilitate research within practice settings and be flexible to allow for local tailoring.29 43 46 Computational tools should allow quick, real-time analysis, providing stakeholders the ability to visualise data to support important clinical decisions.16 One study recommended the need for real time natural language processing capabilities, so that data from patient narratives could be easily used as a data source.59 Another indicated that the system must develop and support ‘citizen-centered smart and mobile devices’ in order to monitor progress and care.28 Finally, the system should be able to assist in promoting public health by providing surveillance of health concerns that could inform public policy.46
Fifteen articles discussed capabilities for data standardisation and governance in LHS.18 19 24 28 33 35 36 43–46 55 64–66 Trustworthy and high-quality data that is evidence-based, ethically sound and interchangeable were essential factors.24 35 36 43 65 Standards must be transparent and apply good governance practices to ensure trustworthiness.24 64 One study suggested that the adoption of internationally recognised standards (ie, Fast Healthcare Interoperability Resources) would ensure standardisation of all systems supporting efficient clinical decision making.46 Data should be available for use by individual stakeholders (clinicians, researchers, patients) in a manner that maintains privacy and confidentiality and incorporates appropriate levels of consent in order to assist in making clinical decisions.23 44–47 61
Integration of data and workflow
To support the multiple and varied uses of data within a ‘digital ecosystem’ data must be integrated into workflow.16 19 22 25 28 29 42 43 Such integration would facilitate collaborative design on programme evaluation among researchers and stakeholders and increase the potential for timely evaluation and feedback.29 42 It would increase the capacity to manage information-intense workflows.43 Ultimately, such a digital ecosystem would increase capacity for clinical decision-making,27–32 particularly when data are aggregated at the appropriate learning unit level or point of care and decision-supports are based on real-time data mining.25 28 30
Culture and climate of supportive learning
An important competency suggested by some authors is the need to create a culture and climate supportive of learning.16 21 25–27 29 30 33 37 41 44 51 55 57 67–71 A learning culture is supported through system competencies and allows for reflection and a practicing mindful organisation.30 72 It necessarily requires a culture of transparency and effective communication supporting a ‘learning climate’.29 67 Several articles noted that enabling a learning culture requires the capability to build trust, respect and affective commitment within the organisation.70–72 Establishing trust by engaging patients and the public is important,70 with one article suggesting organisational ‘ambassadors’ for this purpose.71 Moreover, leadership capacity is required to promote a learning culture and climate.51 Organisational leadership must provide performance metrics and rewards aligned to the ‘value’ placed on learning and continuous improvement.21 27 51 Leadership capability is also required to motivate the workforce to engage in evidence-based practice and to take ownership of local processes for implementation.27
Interactions among individuals and engagement of individuals with the LHS are required for ongoing learning and quality improvement. Capability for engagement and collaboration was emphasised in 13 articles within the review;,25–27 30 33 37 41 44 55 57 67–69 an LHS must support engagement from all key stakeholders with a particular focus on engagement of patients and family members with the system.30 37 55 57 It should also enable and promote collaboration across stakeholders.26 27 33 41 57 67 68 Two articles noted collaboration as a necessary outcome of establishing shared goals within the system.33 41 Others focused on the capacity for interprofessional collaboration within an LHS specifically noting collaboration among organisational leaders and researchers to establish the scope of problems and research methods,26 27 67 collaboration within multidisciplinary teams for high-quality patient care30 and collaboration with policy experts embedded within the system.69 One article emphasised the capacity for inter-organisational collaboration for rapid synthesis and conversion of data to portable formats (eg, tools and guidelines).68
Finally, an LHS should have the capacity to train and educate the workforce to maximise participation and potential for ongoing learning and quality improvement.16 27 72 An organisation must be able to train frontline workers to deliver evidence-based practice and a data-science workforce to engage with a digital ecosystem.27 73
Discussion
This scoping review described requisite competencies at patient, health system worker and system level in relation to operationalising LHS. Themes identified at the individual/patient level were knowledge and skills to understand and share information with an established system, and the ability to interact with the technology used to collect data. Themes at the health system worker level were skills in evidence-based practice, leadership, self-reflection, and teamwork and analytical and technological skills required to use a ‘digital ecosystem’. Researchers within LHS require a specific set of competencies. Themes identified at the system level were data, infrastructure and standardisation; integration of data and workflow; and culture and climate supporting ongoing learning.
The scoping review identified that the current literature on LHS competencies has been steadily growing since 2013. As the concept of LHS is relatively new and closely associated to healthcare policy initiatives (quadruple aim), it is not surprising that there is growing interest. We also identified that a large majority of the work is being performed in the USA, the UK and Canada while a few studies have been identified from other parts of the world. Although this finding may be due to the search terms we used and the differences in global research, this finding may prove important for the future growth of LHS. An underlying premise of developing mature LHS is the need for national and international collaboration with data exchange, process sharing and outcome standardisation. For mature LHS to evolve, competent individuals and systems that effectively communicate globally is required. Further study of the global needs individual and system competencies is needed.
In this scoping review, we identified individual competencies of patients/individuals, healthcare workers and system capabilities published in the literature and considered requisite to operationalising LHS. Regarding individual level competencies, very few articles described competencies at the patient level. Those published related to the patient’s capacity to access the system, to understand and share health-related information, to interact with the technology used to collect data and to partner with healthcare workers. The lack of literature is surprising especially in consideration of the effort for patient-centred care that focuses on care that is responsive to individual patient preferences, needs and values while relying on the patient to provide important aspects of self-care and health monitoring.74 75 In many cases, basic understanding and capability to use and understand technology is requisite to appropriately and safely sharing personal health information, obtaining reliable health information and actively engaging in one’s own healthcare. Although further research is needed to determine the extent of the competencies required of patients to interact with and contribute to LHS, our work suggests that some level of technological comprehension is required of individual patients to interact effectively within LHS. At the LHS worker level, the need for skills in evidence-based practice and the ability to model these skills in practice was identified, as well as the use of data and information to evaluate the quality of practice and to inform quality improvement initiatives. Competencies of researchers embedded in LHS have been described in detail reflecting seven domains; two of those domains were reinforced by other articles reviewed. The seven competency domains for researchers in LHS described by Forrest et al provide a comprehensive framework for the further development of individual knowledge, skills and attitude of researchers.7 Greenberg-Worisek et al subsequently identified the domains from this work as competencies required of healthcare providers working in LHS.15 However, this author did not consider the alignment between the competencies identified by Forrest et al and the skills and knowledge required by practitioners beyond identification of the domains.7 Further research should explore which of the specific competencies as identified by Forrest et al should be developed for practitioners working in LHS and should also focus on the competencies of patients in the LHS.7
Leadership plays a pivotal role in supporting the development of a learning culture and climate in LHS, and leaders at clinical, operational and strategic level are deemed important for creating and supporting requisite individual and system capabilities including stimulating a culture and climate of supportive learning. Yet, questions remain regarding how to build individual level competencies within stakeholders in the system to support a culture and climate supportive of learning. The use of champions and leadership support are well-established strategies in the field of quality improvement and implementation science. However, additional research is required to distinguish the unique leadership capabilities required in relation to the complexity of the ‘system’ (ie, group within an organisation, organisation, inter-organisational network, national system, international network).
Understanding individual competency level requirements to act within an LHS is vital to the successful development and implementation of LHS. Further research should investigate individual competencies for acting within an LHS to inform important stakeholders like educational systems and industry-based training entities and policymakers to reach the quadruple aim of healthcare.
The preponderance of the included articles described system level capabilities for which we identified three main themes: (1) data, infrastructure and standardisation; (2) the integration of data and workflow and (3) the culture and climate supporting ongoing learning. However, within the literature related to systems competencies, the meaning of ‘system’ varied from being related to referring to units within organisations, to organisations, to intra-organisational groups, inter-organisational networks, national networks and international networks. While this review did not seek to analyse system level competencies according to degree of size or complexity associated with respective levels of ‘systems’, analysis did suggest that as the organisation of the respective ‘systems’ became more complex, so did the establishment of requisite competencies within those systems (ie, data standardisation, data sharing, data governance).
Our scoping review expands on previous efforts to establish frameworks that model how an LHS best functions. This scoping review demonstrates the importance of alignment of competencies and capabilities across different levels-comprehensive of the system and all the system stakeholders. Our analysis indicates that system competencies for an LHS are fairly well identified. Yet, further development is necessary to effectively integrate those competencies with those required of individual stakeholders within the system.
Multiple aspects of health systems can be evaluated in continuous learning cycles. The framework of the WHO is often used in evaluating health system performance, which includes six ‘building blocks’: service delivery; health workforce; health information systems; access to essential medicines; financing and leadership/governance.76 Braithwaite and colleagues compared health system frameworks in a comparative international analysis, showing that commonly used domains in evaluating health system performance were safety, effectiveness and access.77 In addition, the WHO has conceptualised the ‘learning’ process in LHS, by describing the learning process at multiple interconnected levels: individual, team/group, organisational and cross-organisational level. Learning across levels can be established through feedback and feedforward loops.78 Such (international) frameworks and approaches can be used by LHS in their further development.
The need for the further development of LHS has been recognised through several international initiatives. Core values have been described, a research agenda was established79 and the current knowledge on LHS was synthesised in a recent scoping review.80 Despite the high potential of LHS, their development and implementation are a challenge, and many organisations are seeking support in becoming an LHS. Exemplars of outcomes from establishment of LHS are required. In addition, guidance and tools for developing and implementing an LHS are needed to support the enactment of LHS within and across organisations.
Our scoping review has several limitations. Many studies included in this review are based on preliminary analyses of LHS which limits the ability for robust data synthesis. In addition, quantitative evaluations of LHS are scarce and causal inferences about necessary competencies and capabilities cannot be reliably constructed. However, the scoping review approach is congruent with the current developmental phase of LHS and allows for the identification of knowledge gaps and future directions for research, policy and practice.
In conclusion, the identified individual competencies of stakeholders within LHS as well as the system capabilities of LHS provide a solid base for the further development and evaluation of LHS. International collaboration for stimulating LHS will assist in further establishing the knowledge base for LHS.
Supplemental material
Data availability statement
No data are available.
Ethics statements
Patient consent for publication
Ethics approval
Review by an ethics committee or internal review board was not required for this study as it did not involve human subjects research.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors The authors confirm contribution to the paper as follows: study conception and design: PLM; data collection: PLM, JP, KH, JM, PJvdW; analysis and interpretation of results: PLM, KH, JM, PJvdW; draft manuscript preparation: PLM, JP, KH, JM, PJvdW. PLM; guarantor. All authors reviewed the results and approved the final version of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.