Article Text

Abstract
Objectives To investigate the prevalence of the comprehensive frailty and its associated factors among community dwelling older adults.
Design A cross-sectional study.
Setting Six community healthcare centres in Xi’an City, Northwest China.
Participants A total of 2647 community dwelling older adults completed the study between March and August 2021.
Primary and secondary outcome measures The primary outcome was the prevalence of frailty, measured with the Comprehensive Frailty Assessment Instrument. The secondary outcomes were potential factors associated with frailty, measured with a social-demographic and health-related information sheet, the Short-Form Mini-Nutritional Assessment and the Pittsburgh Sleep Quality Index.
Results The participants averaged 27.77±10.13 in the total score of the Comprehensive Frailty Assessment Instrument. According to the cut-off points defining the classification of frailty, the majority of the participants were with mild (n=1478, 55.8%) or high (n=390, 14.8%) frailty. Multivariate stepwise linear regression analysis demonstrated that older age, lower educational level, empty nesters, higher level of self-perceived medical burden, abnormal body weight, physical inactivity, medication taking, increased number of clinic visit, undernutrition and poor sleep quality are associated with higher total score in the Comprehensive Frailty Assessment Instrument, indicating higher level of frailty. Multivariate multinomial logistic regression analysis exhibited similar findings but further captured female gender as a risk factor for the presence of mild and high frailty compared with no-low frailty.
Conclusion The prevalence of the comprehensive frailty and frailty in the physiological, psychological, social and environmental domains is high. A variety of social-demographic, health-related and behavioural factors were associated with the comprehensive frailty. Further investigations on frailty prevalence and its associated factors based on comprehensive assessments are desirable.
- primary care
- geriatric medicine
- epidemiology
Data availability statement
Data are available upon reasonable request. Data are available upon reasonable requests by contacting the corresponding author through the following email address: zhangyulian0307@126.com.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
A total of 2647 participants were randomly recruited from multiple community healthcare centres, which enhanced the sample representativeness and the accuracy of point estimates.
The concurrent use of multivariate stepwise linear regression and multivariate multinomial logistic regression analyses, and their consistent results enhanced the reliability of the identified factors associated with frailty.
Due to the nature of a cross-sectional study, causal relationship could not be established.
The majority of the variables were collected with subjective measures, which might introduce reporting bias to the study.
Introduction
Frailty is physically characterised by declines in function and reserves across multiple physiological systems, accompanied by an increased vulnerability to stressors.1 2 With the rapid increase of older population, frailty has become an emerging health concern worldwide. Research evidence has consistently suggested that frailty is associated with a broad spectrum of adverse outcomes, such as increased risk of fall, comorbidity, disability, mortality, emotional disorders, hospitalisation, admission to long-term care and compromised quality of life.2–5
The reported prevalence of frailty among community dwelling older adults varied significantly across studies, from 4% to 59.1%.6–8 One of the important factors contributed to the heterogeneous prevalence is the use of different frailty screening instruments. As frailty is possibly modifiable or reversible with appropriate interventions, especially at its early stages,2 9 10 identifying individuals with the condition using an appropriate instrument for a certain setting is paramount.
An expansive body of instruments for the assessment of frailty have been developed based on different conceptual frameworks, among which the concept of physical phenotype, proposed by Fried and colleagues and the concept of accumulation of age-related deficits, proposed by Rockwood and colleagues, are currently dominating the field.2 11 12 Instruments developed based on the two conceptual frameworks, such as the Frailty Phenotype, the FRAIL (Fatigue, Resistance, Ambulation, Illnesses and Loss of weight) scale and the Frailty Index, define frailty with exclusive physical/physiological criteria and thereby could lead to fragmentation of care. With the evolving concept of frailty, psychological and social indicators were included for the comprehensive assessment of frailty. Gobbens and colleagues proposed an integral conceptual model of frailty and developed the Tilburg Frailty Indicators (TFI), an instrument measuring frailty among community dwelling older adults in three domains—physical, psychological and social.13–15
Like many chronic diseases or conditions, a large proportion of the individuals with frailty live in the community. In this sense, older adults depend highly on the sustainability of their housing conditions and environment.16 17 In other words, environmental factors could play important role in the development and progression of frailty. Under this background, the Comprehensive Frailty Assessment Instrument (CFAI), a 23-item instrument was developed based on the integral conceptual model.17 Compared with the well-known exclusively physical-originated instruments, for example, Frailty Phenotype, and the multidimensional TFI, the CFAI is featured with its incorporation of environmental indicators in addition to physiological, psychological, social perspectives. Another characteristic of the CFAI is that it presents the findings as no-low, mild and high frailty, while most existed tools regard an individual as robust, pre-frail and frail. A comprehensive assessment of frailty regards an individual as a social integrity and allows for the development and implementation of targeted and individualised management strategies. However, even though a flourishing body of studies on the prevalence of frailty have been conducted worldwide, the condition was frequently measured from a physical perspective.7 18 Research evidence regarding the prevalence of frailty based on a comprehensive assessment, especially an assessment that included the environmental domain is still lacking, and thus, further investigations are guaranteed.
Identifying the factors associated with frailty is substantial for informing the development of interventions to manage frailty and minimise its consequences. Some evidence regarding the factors associated with frailty in the community setting are available in the literature body.7 19–22 However, conclusion could not be drawn for several reasons. Foremost, in a large proportion of the existed studies, frailty was measured with physical-originated instruments. As a result, the identified factors might not be generalisable to the practice where comprehensive assessments of frailty were employed. In addition, the results regarding some factors are not conclusive across studies. Besides, the effects of some important modifiable factors of frailty were frequently neglected in the existed studies, such as nutritional status and sleep quality.
Thus, this study was conducted with the objectives to investigate the prevalence of frailty with the multidimensional CFAI, and to explore the factors associated with the comprehensive frailty among community dwelling older adults.
Methods
The reporting of this study adhered to the Strengthening the Reporting of Observational Studies in Epidemiology statement.23
Study design, setting and participants
This was a cross-sectional study conducted in six community healthcare centres in Xi’an City, Northwest China from March to August 2021. According to the governmental policy, community healthcare centres provide primary health services to all the citizens within their regions. The duties include building health records, providing primary medical treatments and health education, organising regular health check-ups and home visits and so on.
The target population was community dwelling older adults. The inclusion criteria for eligible participants were: (1) aged ≥60 years; (2) had a health record in the community healthcare centres; (3) had sufficient communication ability; (4) consent to participation. Individuals were excluded if they were with a clinical diagnosis of mental disorders, in terminal condition or taking part in other studies.
The research participants were recruited from the six community healthcare centres using simple random sampling. After an initial screening, 35 612 potentially eligible participants were identified and were coded sequentially based on their health record number in the community healthcare centres. A set of random numbers were then generated using the Research Randomizer V.4.0 to capture the research participants.

The sample size calculation formula for cross-sectional studies of qualitative variable (prevalence studies) was used to determine the sample size.
Take α=0.05, then  =1.96. According to a systematic review with meta-analysis, the prevalence of frailty among Chinese community dwelling older adults is P=14.4%24; take the absolute precision d=0.1P. Thus the minimum sample size required in this study was 2284. The precision of statistical estimates improves with the increase of sample size in a study.
=1.96. According to a systematic review with meta-analysis, the prevalence of frailty among Chinese community dwelling older adults is P=14.4%24; take the absolute precision d=0.1P. Thus the minimum sample size required in this study was 2284. The precision of statistical estimates improves with the increase of sample size in a study.
Measures
Social-demographic and health-related information
A self-designed social-demographic and health-related information sheet was used to collect data from the research participants. The social-demographic information included age, gender, marital status, educational level, working type before retirement, living status, medical insurance type and self-perceived medical burden. Health-related information included body mass index (BMI), frequency of physical exercise in the past month, types of medication taking, comorbid chronic diseases (with a clinical diagnosis) and number of clinic visits, hospital admissions and medical cost during the past year.
Frailty
The multidimensional CFAI was employed to measure frailty.17 The 23-item CFAI measures the physiological, psychological, social and environmental domains of frailty. Based on a standard scoring algorithm, equal weight was given to each domain, with the maximum domain scores of 25 and total score of 100. A higher score indicates a higher level of frailty. For the total score, the instrument developers proposed the cut-off point of 21.9 between no-low and mild frailty, and 38.8 between mild and high frailty; for the physiological, psychological, social and environmental domains, such cut-off points were 6.3 and 18.8, 5.0 and 11.5, 9.4 and 16.0, 1.25 and 7.5, respectively.25 The original version of the CFAI showed good internal consistency reliability (Cronbach’s α=0.812) and construct validity.17 The CFAI was translated and evaluated for reliability and validity among Chinese community dwelling older adults following international guidelines. The Chinese version instrument exhibited acceptable psychometric properties (Cronbach’s α=0.837, test–retest reliability coefficient: 0.6).26
Nutritional status
The Short-Form Mini-Nutritional Assessment (MNA-SF) was employed to measure nutritional status.27 The MNA-SF is a six-item instrument developed to screen for undernutrition in geriatric practice, with a total score ranging from 0 to 14. An MNA-SF score of <12 is considered as at risk for undernutrition. Both the original and the Chinese version of the MNA-SF showed adequate reliability and validity among older adults.27 28
Sleep quality
The Pittsburgh Sleep Quality Index (PSQI) was employed to measure sleep quality.29 The PSQI assesses the informants’ sleep quality and disturbances during the past month. The 19 items generate seven component scores and a global score. A PSQI total score of >7 is regarded as poor sleep quality for Chinese population. Both the original and the Chinese version of the PSQI are of sufficient reliability and validity.29 30
Procedures and ethical considerations
On the completion of sampling, the research assistants from the community healthcare centres made phone calls to the potential participants, introduced the study objectives and procedures and invited them to participate. Home visits were arranged with interested participants, during which they were provided with an information sheet outlining the study and asked to provide written informed consent. Subsequently, objective variables were measured by independent physical examiners from the research sites while subjective data collected by trained investigators via individual face-to-face interviews. The investigators entered the participants’ response to each item into an online electronic questionnaire. Input of responses to key questions/items was set as compulsory and limited to rational ranges, so that valid questionnaires were guaranteed. Training sessions and competency assessments were arranged before the commencement of the study to minimise outcome assessor-introduced bias and maximise inter-rater agreement.
The study obtained ethical approval from the Ethical Committee of Shaanxi Provincial People’s Hospital (reference identifier: 2021-R001) and permissions from the community healthcare centres. The study participants consented to participation. An information sheet outlining the study was provided to and written informed consent was obtained from the participants before data collection. The participants’ rights and safety were protected by adhering to local laws, the Declaration of Helsinki, institutional policies and the International Conference on Harmonization of Technical Requirements for Registration of Pharmaceuticals for Human Use-Good Clinical Practice (ICH-GCP).
Statistical analysis plan
The IBM SPSS V.24.0 was used for data analysis. Continuous data were described as mean±standard deviation (SD) when normally distributed, while categorical data as n (%). Independent t-test and χ2 test were employed, where appropriate, to compare the scores in the CFAI and the prevalence of frailty between men and women. A two-step procedure was employed to examine the associated factors of frailty based on the total score of the CFAI: univariate linear regression analysis was used to screen for potential associated factors, and the factors of statistical significance (defined as p<0.1) were subsequently included in the multivariate stepwise linear regression analysis. Similarly, univariate and multivariate multinomial logistic regression analyses were sequentially employed, as sensitivity analyses, to explore the associated factors for higher levels of frailty based on the classification criteria.25 The statistical significance level for multivariate regression analysis was set to α=0.05, two-sided.
Patient and public involvement
Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Results
Participants recruitment
A total of 3923 potentially eligible individuals were approached to recruit the scheduled 3000 participants, representing a response rate of 76.5%. The main reasons for refusing to participate were no interest, schedule conflict and lack of time. After screening, 2647 (88.2%) valid questionnaires remained and were included in the statistical analysis.
Social-demographic and health-related characteristics
The average age of the participants was 68.59±6.13 years. Woman accounted for around three-fifths of the total samples. Over 50% of the participants were underweight, overweight or obese. The majority (89.6%) of the participants had comorbid chronic diseases, among which hypertension was the most frequently reported condition, with a concurrent rate of 45.7%. Other social-demographic and health-related characteristics are presented in table 1.
Social-demographic and health-related characteristics of the participants (N=2647)
Frailty among community dwelling older adults
The participants averaged 27.77 (SD: 10.13) in the total score of the CFAI. According to the cut-off points defining the classification of frailty,25 the majority of the participants were with mild (n=1478, 55.8%) or high (n=390, 14.8%) frailty. The mean scores in the physiological, psychological, social and environmental domains of the CFAI were 8.27±5.66, 5.36±3.91, 9.94±3.68 and 4.21±4.97, respectively. For all domains, more than half of the participants were in mild or high frailty. Details on the assessment of frailty are presented in table 2.
Total and gender specific scores in and classification of frailty according to the CFAI (N=2647)
Women were significantly more vulnerable to higher level of frailty with regard to the physiological, psychological and the comprehensive constructs. However, they were less likely to have social frailty compared with men. No gender difference was detected in the environmental domain of the CFAI (table 2).
Factors associated with frailty among community dwelling older adults
Multivariate stepwise linear regression analysis demonstrated that older age, lower educational level, empty nesters, higher level of self-perceived medical burden, abnormal body weight, physical inactivity, medication taking, increased number of clinic visit, undernutrition and poor sleep quality are associated with higher total score in the CFAI, which indicates higher level of frailty. The results of linear regression analyses are presented in table 3.
Univariate and multivariate stepwise linear regression analyses of associated factors of frailty among community dwelling older adults (N=2647)
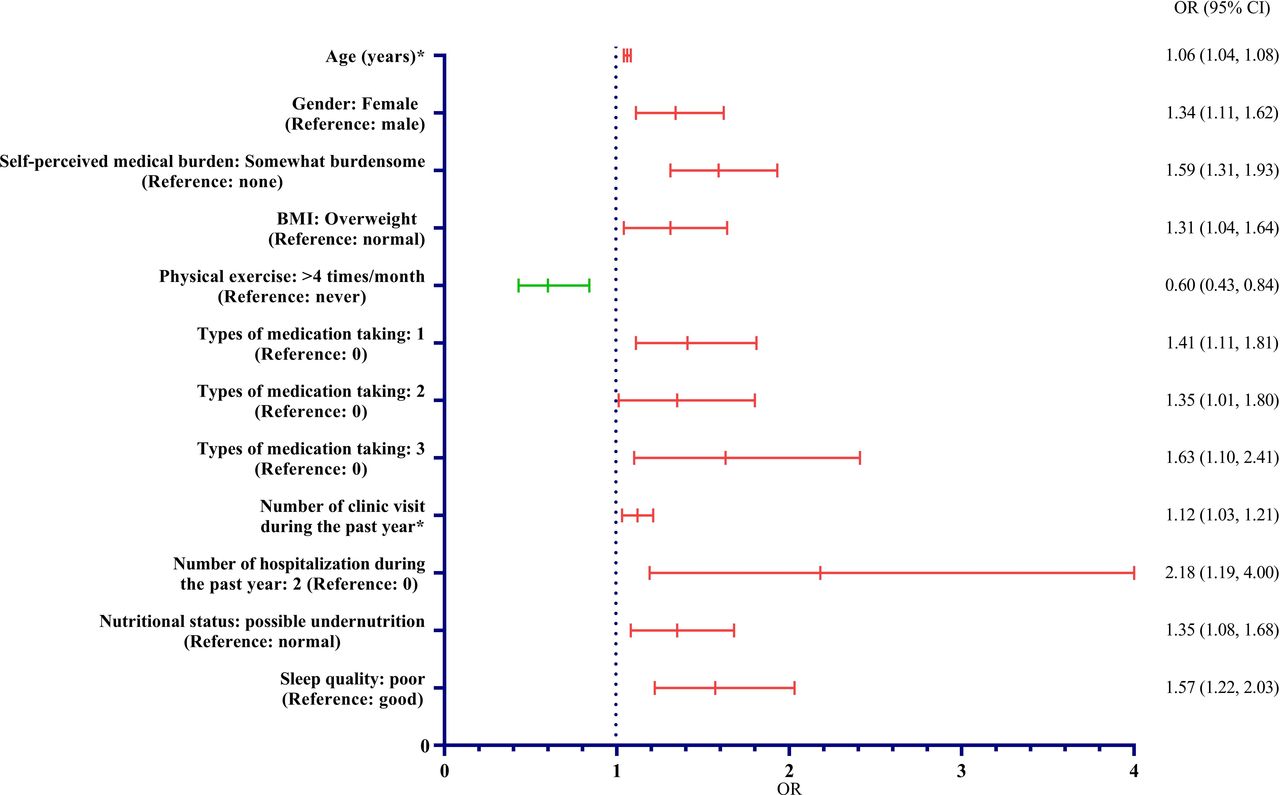
Multivariate multinomial logistic regression analysis exhibited similar findings but further captured female gender as a risk factor for the presence of mild and high frailty compared with no-low frailty. The results of logistic regression analysis are presented in figure 1, figure 2 and the online supplemental table 1.
Supplemental material

Factors associated with the present of mild frailty compared with no-low frailty. *Continuous variables. BMI, body mass index.

{kind=link}
{kind=link}
Factors associated with the present of high frailty compared with no-low frailty. *Continuous variables. BMI, body mass index.
Discussion
A comprehensive assessment of frailty and the investigation of factors associated with the condition are meaningful as the findings could inform the development and implementation of targeted and individualised frailty management strategies. In the current study, the multidimensional CFAI was employed to assess the prevalence of frailty and its associated factors among 2647 Chinese community dwelling older adults. The results of this study demonstrated high prevalence of frailty, in both the multidimensional overall frailty and the physiological, psychological, social and environmental frailty domains. Furthermore, multiple social-demographic, health-related and behavioural factors were identified to be associated with frailty.
Frailty among community dwelling older adults
This study found that 70.6% of the community dwelling older adults were in mild or high frailty based on the comprehensive assessment. As the standard scoring algorithm and cut-off points for the CFAI to define frailty classification were introduced in 2018, only one study was identified to meet the attempt of a direct comparison of the multidimensional frailty prevalence, which reported a lower prevalence compared with the current study (56.6%).25 Because the total score of the CFAI is computed from the four domain scores, the lower prevalence of the multidimensional frailty in the earlier study could be considered as a reflect of the significantly lower prevalence in the physiological and psychological domains (34.9% vs 51.2% and 37.3% vs 51.6% as compared with the current study, respectively). Thus, the difference in the prevalence of the multidimensional frailty between the two studies could be attributed to the increasing prevalence of physical-originated frailty and psychological disorders over years due to the ongoing process of population ageing,24 31 as the analysis of De Witte et al was based on a cohort established in 2004.17 25 Socioeconomic difference could be another contributor of the different frailty prevalence because evidence has suggested that people in lower socioeconomic societies tend to have higher frailty prevalence.2 Besides, the higher female-to-male ratio in the current study could be another cause of its higher frailty prevalence because female gender has been frequently identified as a risk factor of frailty.2 32 As for the quantitative assessment, the community dwelling older adults averaged 27.77 (SD: 10.13) in the CFAI total score, which is comparable to the existed studies.33 34 Besides, there is another study employed the recommended cut-off points.35 However, it did not follow the standard scoring algorithm,25 which hampered a direct comparison, neither qualitatively nor quantitatively. We also attempted to extend the comparison of the multidimensional frailty prevalence with studies that employed a different instrument covering similar domains. One instrument was eligible but no research data were available for the comparison.36
Physiological indicators are the most apparent evidence of frailty and dominating the field of frailty assessment. The results of this study showed that 51.2% of the community dwelling older adults were in mild or high physiological frailty, which is significantly higher than the prevalence reported in studies that used exclusively physical-originated instruments.6 7 37 The indicators included in the instruments could explain the significantly different prevalence: exclusively physical-originated instruments generally assess frailty with both physical constraints and functional declines while the physiological domain of the CFAI assesses physical frailty with exclusive functional declines. This hypothesis is supported by a recent study that measured frailty with the TFI: the prevalence of physiological frailty was 54.3% among 2289 older adults from five European countries.32 Meanwhile, the prevalence of physical frailty in the current study is among the highest range as reported by existed studies used comprehensive assessment instruments.24 32 38 The use of different instruments, the ongoing process of population ageing and the different socioeconomic level could be the possible reasons for the higher prevalence in the current study.2 24 31 39
Frailty is considered as a health-based, rather than organ/disease-based, integrative condition. More importantly, psychosocial indicators are associated with multiple adverse outcomes among older adults.13 So the assessment of frailty should include not only physiological but also psychosocial indicators.13 40 In the current study, the prevalence of mild or high psychological and social frailty among community dwelling older adults were 51.6% and 50.9%, respectively. The prevalence of mild or high psychological frailty in the current study is much higher than that in the study of De Witte et al (37.3%),25 possibly due to the ongoing increasing prevalence of psychological disorders among all age groups over years and the difference in female-to-male ratio.31 In contrast, the prevalence of mild or high social frailty in the current study is sign\ificantly lower than the cited study (68.1%),25 which might be explained by the fact that Chinese people tend to have more interactions with their relatives, friends, neighbours and other social support resources, and the fact that the rapidly developing digital technologies are making social interactions easier. As most of other frequently used multidimensional frailty assessment instruments do not have a well-acknowledged cut-off points for the frailty domains, the attempts to extend the comparison failed. Further evidence regarding the prevalence of psychological and social frailty is valuable.
Environmental factors could play important role in the development and progression of frailty.16 17 39 41 Environmental indicators are regarded as a necessary element for the assessment of frailty among older adults, especially in the community setting. In this study, 53.5% of the community dwelling older adults were in mild or high environmental frailty, which is slightly higher than the reported prevalence in the study conducted by De Witte et al (45.4%).25 An individual’s housing condition and the environment therein are associated with local socioeconomic level. Hence, socioeconomic difference could be the main reason for the different prevalence as the current study was originated from a middle-income country while the earlier study from a high-income country.42 The assessment of frailty in the environmental domain is in its infancy and further investigations are desirable.
Factors associated with frailty among community dwelling older adults
Identifying the factors associated with frailty is equivalently important as the assessment of the condition as it informs the development and implementation of proper frailty management strategies. This study confirmed several social-demographic (older age, female gender, lower educational level and empty nesters), health-related (underweight, undernutrition and medication taking) and behavioural (physical inactivity and poor sleep quality) risk factors associated with frailty. Remarkably, it in the first time, to our knowledge, identified higher level of self-perceived medical burden, increased number of clinical visit and overweight as the risk factors of frailty. However, comorbidity was not a significant risk factor of frailty as demonstrated in this study, contradicting the findings of many existed studies.
Social-demographic factors
Older age
Older age has been consistently found to be highly associated with frailty, in both exclusively physical-originated and comprehensive assessments.32 43 44 This study confirmed the previous findings. With the advance of age, declines in various organs accumulated, leading to physical limitations and psychological distress,2 which could further interfere an individual’s social interactions and ability to adapt to the changing environment.
Female gender
Even though female gender was identified as a risk factor of frailty in the multinomial logistic regression analysis, it did not enter the multivariate stepwise linear regression model, contradicting the existed evidence.2 32 Previous studies suggested that older men are more likely to die suddenly, while women more often exhibit a steady decline.45 Therefore, physical frailty could present more often among women. Women are also more vulnerable to psychological problems, increasing the likelihood of psychological frailty. However, men tend to be more prone to social frailty, as is shown in the current study, and equivalent in environmental frailty compared with women,32 thus lead to the missed association between gender and the multidimensional frailty. Further evidence is necessary before the association between gender and the multidimensional frailty is conclusive.
Lower educational level
This study showed that older adults who completed college or above level of education had lower level of frailty, which is consistent with previous findings.2 46 An individual’s education level is associated with his/her health literacy, coping skills and adherence to healthy lifestyles. As a result, individuals with higher education level could have better overall well-being.
Empty nesters
It was found that empty nesters, referring to older adults living alone, tended to be frailer. Evidence suggests that empty nesters may not always be frail in the physiological aspect,32 but they could have more psychological distress, more loneliness and less social supports and be more vulnerable to environmental challenges, contributing to the increased level of overall frailty.
Health-related factors
Undernutrition
Undernutrition entered the regression models of factors associated with frailty in this study. Malnutrition has been frequently identified as a risk factor of frailty.32 47 Poor nutritional status may accelerate the loss of muscle mass and the decrease of muscle strength, which could gradually lead to functional limitations, psychological problems, social isolation and vulnerability to environmental risks.48 Such syndromes comprise the comprehensive frailty.
Abnormal body weight
Notably, this study found that underweight and overweight are associated with frailty while obesity is not associated with the condition. Existed evidence, however, suggests a U-sharped curve between BMI and frailty.49 50 The missed association between obesity and frailty in this study might be due to its low power in detecting such association as only 238 (8.9%) of the samples were obese. As for the different results regarding overweight as a risk factor of frailty between the current study and previous studies, ethnic difference is the possible reason as those studies were originated from Western countries. Further investigations on the association between body composition and frailty with more accurate indicators, such as body fat and waist circumference,51 among diverse population are guaranteed.
Medication taking
Medication taking is identified as an independent risk factor of frailty, which is in accordance with existed evidence.2 Number of medication taking is a reflect of older adults’ basic health condition and an indicator of higher risk of medication toxicity, and thereby associated with frailty.
Increased number of clinic visit and higher level of self-perceived medical burden
Increased number of clinic visit and higher level of self-perceived medical burden, another two reflects of older adults’ basic health condition but rarely explored factors, were also found to be associated with frailty. Frequent clinic visit and self-perceived medical burden might cause psychological distress. Self-perceived medical burden might also influence older adults’ adherence to treatment regime. Eventually, these two health-related factors could contribute substantially to the development and progression of the comprehensive frailty.
Contradicting the majority of existed studies, this study found that comorbidity is not associated with frailty.2 32 52 The presence of chronic diseases could introduce multiple physical, psychological and social detriments to older adults,32 and hence be linked to frailty. The absence of the expected association between comorbidity and frailty might be explained by the situation that a large proportion (83.0%) of the participants in the current study were with one or two concurrent chronic diseases. As a result, the study was not powerful enough to detect the association between the number of comorbid chronic diseases and frailty. In view of the multidimensional adverse effects of concurrent chronic diseases on the well-being of older adults, healthcare providers should make comorbidity count when assessing and managing frailty.
Behavioural factors
Physical inactivity
The results of this study indicated that older adults who engaged more physical activities were less likely to be frail, which is consistent with the findings of previous studies.32 53 Physical activity improves skeletal muscle quality (both muscle mass and muscle strength) and physical performance, reduces disordered emotions, increases connections with others and thus limits the development and progression of frailty.
Poor sleep quality
In line with existed research evidence, this study linked poor sleep quality with frailty.54 55 All systems of human body are restoring during sleep. So, poor sleep quality accelerates declines in function and reserves. Sleep disturbances have been frequently found to be associated with a wide spectrum of psychological problems and compromised quality of life.56 Due to various contributors, for example, medication taking, older adults are highly vulnerable to disturbed sleep, increased the risk of the overall frailty and its domains.55
Strengths and limitations of this study
This study has several remarkable strengths. For one thing, it is among the few studies that have investigated the prevalence and associated factors of frailty from a comprehensive perspective. The validated multidimensional CFAI was used to assess frailty from the physiological, psychological, social and environmental domains. For another, a total of 2647 participants were randomly recruited from multiple community healthcare centres, which improved the accuracy of point estimates and generalisability of the findings. In addition, several understudied factors, such as nutritional status and sleep quality, were examined for the association with frailty.
Despite its strengths, the results of this study should be interpreted with the careful consideration of its limitations. First, a cross-sectional study design was employed, making causal inference and investigations on the reversibility of frailty infeasible. Second, although the sample size is large, this study only included older adults living in one metropolis in Northwest China. Thus, the generalisability of the findings could be downgraded. Third, due to the lack of studies with comprehensive frailty assessments, the comparison of findings between the current study and existed studies was limited. Moreover, the majority of the variables were collected with subjective measures, which might introduce reporting bias to the study.
Implications
Frailty is a progressive chronic condition leading to various negative consequences. However, the majority of the individuals with the condition are left unscreened. Healthcare providers, especially those in the primary healthcare institutions, should improve the awareness of frailty screening and management and select setting-sensitive instruments for the screening. Malnutrition and physical inactivity are frequently found to be associated with frailty, and meanwhile, common among older adults. They are also the main targets of frailty management strategies. Healthcare providers should consider the individualised characteristics of older adults when making preventive or management plans. At the same time, modifiable behavioural features, for example, sleep quality, should also be addressed.
To date, epidemiological evidence regarding frailty is mainly based on exclusively physical-originated assessments. Further investigations should address the gap of lacking data on other aspects of frailty, including psychological, social, environmental and even cognitive domains. Besides, longitudinal studies are necessary before the causality between frailty and various factors is well-established. It is common that scales were not always used in the standard or recommended manner, which compromised the comparisons across studies. Hence, investigators are encouraged to refer to the well-acknowledged guidance when using an instrument in further studies.
Conclusions
The prevalence of the overall frailty and frailty in the physiological, psychological, social and environmental domains is high. Factors associated with frailty including older age, female gender, lower educational level, empty nesters, higher level of self-perceived medical burden, abnormal body weight, physical inactivity, medication taking, increased number of clinic visit, undernutrition and poor sleep. Further investigations on frailty prevalence and its associated factors based on comprehensive assessments are desirable.
Data availability statement
Data are available upon reasonable request. Data are available upon reasonable requests by contacting the corresponding author through the following email address: zhangyulian0307@126.com.
Ethics statements
Patient consent for publication
Ethics approval
The study obtained ethical approval from the Ethical Committee of the Shaanxi Provincial People’s Hospital (reference identifier: 2021-R001).
Acknowledgments
We appreciate Ms. Wang Nana for the professional consultation on statistical analysis. Special acknowledges are given to the community healthcare centres and older adults participated in the study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
XY and ZS contributed equally.
Contributors XY and YZ conceptualised and supervised the study. XY prepared the manuscript. ZS, DW, YN and YM led the field survey. ZS, CX, HL, HG and ML critically revised the manuscript. All authors approved the final manuscript. XY is responsible for the overall content as the guarantor.
Funding This study was granted by the Department of Science and Technology of Shaanxi Province, P. R. China (reference identifier: 2020ZDLSF01-08, 2022ZDLSF03-15) and the Chinese Nursing Association (reference identifier: ZHKY202022). The grant bodies played no role in the development and implementation of the study and the interpretation of the findings.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.