Article Text

Abstract
Objective Ischaemic stroke incidence is on the decline globally, but the trend in South Korea is unknown. In this study, the 10-year incidence trends of first-ever ischaemic stroke in South Korea were evaluated.
Design, setting and participants The National Health Insurance Services medical claim data were used to construct 10 annual cohorts of adults aged 20 years and older, who had not been diagnosed with stroke, to find out the incidence trends of first-ever ischaemic stroke from 2010 to 2019.
Outcome measures The primary outcomes were crude and age-adjusted incidence rates for 10 years. Crude incidence rates of the age groups and incidence age statistics were calculated. For comparison among the income groups, age-adjusted incidence rates were used. Incidence rates in all the groups were analysed separately by sex.
Results Age-standardised incidence rates of ischaemic stroke per 100 000 were 101.0 in men, and 67.6 in women in 2010; and 92.2 in men, and 55.0 in women in 2019. By age group, there was a decrease in women over 40 years of age, and men over 60 years of age. The relative difference in stroke incidence rates between medical aid beneficiaries and the highest income group increased from 1.5 to 1.87 over 10 years.
Conclusions Age-standardised incidence rate of ischaemic stroke has decreased from 2010 to 2019 for both man and women. The incidence rate was stable in the younger age groups and decreased in the older age groups, and the disparities between income groups have widened over the past decade. Stroke prevention strategies are needed for the younger age group and the low-income group. Further research is needed to study the risk factors contributing to the incidence of ischaemic stroke in different groups.
- stroke
- epidemiology
- public health
Data availability statement
Data are available upon reasonable request. Data may be obtained from a third party and are not publicly available. Raw data were generated at Korea National Health Insurance Service. Derived data supporting the findings of this study are available from the corresponding author on request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
The primary strength of this study is that it calculated the ischaemic stroke incidence using population-based nationwide claim data.
The trends of ischaemic stroke incidence in the subgroups were calculated by applying the same criteria for 10 years.
The limitations of this study are that it did not include mild patients who stayed home and visit outpatient clinic, died before coming to the hospital and stroke that occurred during hospitalisation.
It is believed that determining stroke incidence accurately with claim data is difficult, but we defined the stroke incidence rate by considering the possible clinical situations, such as hospitalisation via the emergency room and brain imaging, along with the diagnosis.
Introduction
Stroke is a major cause of disability and death, resulting in huge medical expenditures.1 The incidence of stroke is declining worldwide,2–4 with the decrease in high-income countries reportedly due to a decrease in the prevalence of risk.5–7 In South Korea, the prevalence of risk factors of ischaemic stroke such as hypertension, diabetes, obesity and atrial fibrillation was increasing over the past years.8–10 Moreover, ageing is the strongest risk factor of ischaemic stroke,11 and Korea is rapidly becoming an ageing society.12
Stroke incidence and prevalence differ according to the sex and socioeconomic position, and many studies have shown that these differences persist over time.13–16 In South Korea, the inverse relationship between socioeconomic position and stroke incidence was also studied.17 However, there are few studies that track the incidence trends and reveal the difference in trends by age and household income in South Korea.
The purpose of this study is to examine the first-ever ischaemic stroke incidence trends over 2010–2019 in South Korea using National Health Insurance Data (NHID). This study would have greater significance as a nationwide study.
Methods
Study data
This study used data from the NHID of National Health Information Service (NHIS) between 2010 and 2019. The NHID has information on 97% of national health insurance beneficiaries and 3% of medical aid beneficiaries,18 including data on healthcare utilisation, health screening, sociodemographic variable and income-related data for the whole population.19
Study design
This study examined the 10-year trend of first-ever ischaemic stroke incidence from 2010 to 2019. Ten cohorts were constructed retrospectively for 10 years. Each cohort consisted of adults aged 20 years and older, who had not been diagnosed with I60 (subarachnoid haemorrhage), I61 (intracerebral haemorrhage), I62 (other non-traumatic intracranial haemorrhage), I63 (cerebral infarction), or I64 (stroke, not specified as haemorrhage or infarction) for the previous 3 years.
Study population
First-ever ischaemic stroke cases were defined as: (1) patients admitted via an emergency room, with the principal or additional four diagnosis codes of I63; (2) who underwent brain imaging during their hospitalisation including ‘brain CT’, ‘brain MRI’, and ‘brain CT angiography’; and (3) cases who had been diagnosed with I60–64 code were excluded, with a wash-out period of 3 years (figure 1). Hospitalisation through an outpatient clinic was not included as an incidence of acute stroke, because hospitalisation through an outpatient clinic is likely to receive a health examination or elective intervention such as carotid angioplasty or intracranial angioplasty.

Selection process of study population.
Patient and public involvement
No patient involved.
Variables
For subgroup analysis, the stroke incidence trend was calculated by age group and household income group.
Age
For subgroup and age-standardised analysis, age was divided into 10-year units from age 20, and age 80 and older were grouped into one group (20–29, 30–39, 40–49, 50–59, 60–69, 70–79, and 80 and more).
Household income
In Korea’s NHIS, the premium varies depending on the income level.19 Medical aid beneficiaries with low household incomes do not pay insurance premiums, and they pay minimal or no copayments for medical use.18 The study population was divided into six groups; NHIS beneficiaries divided into quintiles, and one group of medical aid beneficiaries.
Statistical analyses
Sex-specific crude and age-standardised incidence rates of ischaemic stroke were analysed from 2010 to 2019. Subgroup analyses were undertaken for the age groups and income groups. Crude rates were calculated by dividing the number of patients defined as annual stroke by the number of people in the year in the retrospective cohort. For age standardisation, the 2005 mid-year population from Statistics Korea and WHO standard population were used as a reference population. To study the trend of incidence by age group, we used Jonckheere Terpstra Test which is a rank-based non-parametric test. For comparison among the income groups, age-standardised incidence rate (reference population: 2005 mid-year population from Statistics Korea) according to the household income level (medical aid beneficiaries, first, second, third, fourth, and fifth) was calculated. The incidence rate ratio was calculated between medical aid beneficiaries which is the lowest income group, and the highest income group. All analyses were performed separately for both the sexes using SAS V.9.4 (SAS Institute).
Results
In men, the number of ischaemic stroke incidence patients was highest in the age group of 60–69 or 70–79 years, and in women, the number of ischaemic stroke incidence patients was highest in the age group 70–79 in all years. For those over 80 years of age, the number of stroke incidence patients increased sharply between 2010 and 2019. For both men and women, the number of ischaemic stroke incidence patients increased in all household income groups over 2010–2019 (table 1).
Characteristics of patients who had an ischaemic stroke by sex, 2010–2019
From 2010 to 2019, the number of life-first diagnosed ischaemic strokes increased from 20 138 to 26 768 in men (33%), and 17 309 to 20 234 in women (17%), over the past decade. In men, the crude incidence rate per 100 000 was 106.7 in 2010, 103.9 in 2015 and 124.8 in 2019. In women, the crude incidence rate per 100 000 was 90.1 in 2010, 83.0 in 2016, and 93.4 in 2019. The standardised rate per 100 000 using the Korean annual population was 101.0 in 2010, decreased to 85.7 in 2015, and then increased to 92.2 in 2019 in men; and 67.6 in 2010, decreased to 50.7 in 2018 and then surged to 55.0 in 2019 in women. A statistically significant decrease was observed in the age-standardised rate for both women and men (p for trend (P) in men=0.040, P in women<0.001) (figure 2, online supplemental table 1).
Supplemental material

Trends in crude, age-standardised ischaemic stroke incidence rate per 100 000 by sex, 2010–2019.
For both men and women, the incidence rate increased with age, being highest in those aged 80 years or older. The gap in the incidence rate between the sexes was the smallest in the age group with 20–29, and contrary to the general trend, women had a higher rate than men over many years. The incidence rate trend decreased in men in their 60–69 and 70–79, and in women in their 40–49, 50–59 and 60–69. The decreasing trends were significant in 70–89 in men (P=0.002), and 40–49 (P=0.025), 50–59 (P=0.002), 60–69 (P<0.001), and 70–79 (P<0.001) in women (figure 3, online supplemental table 2).

Trends in crude incidence rate per 100 000 person year of ischaemic stroke by sex according to age group.
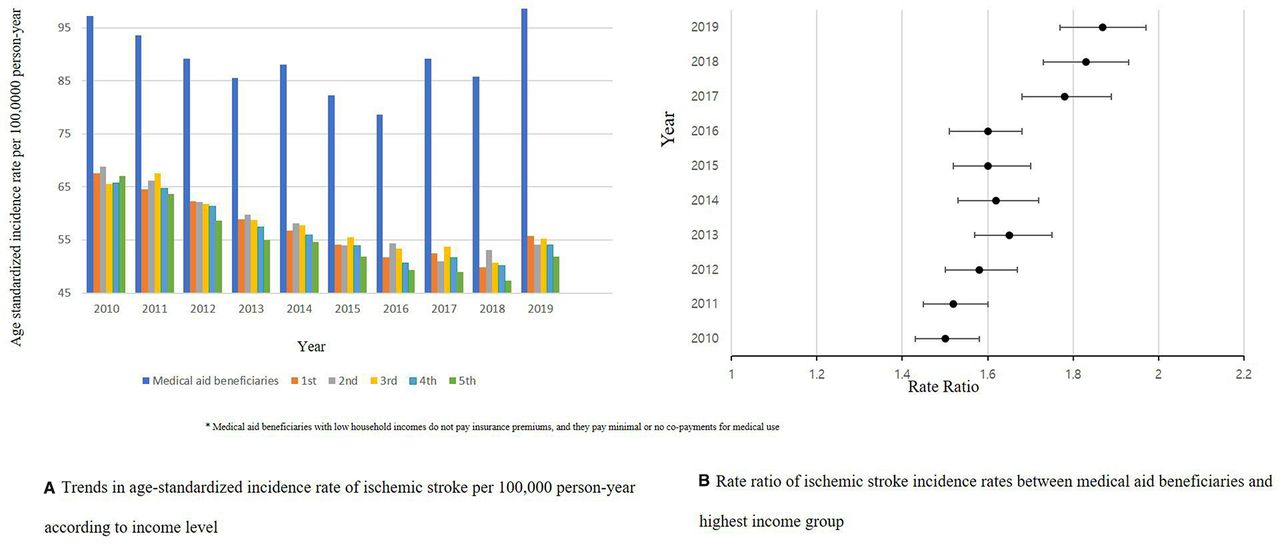
For the household income analysis, the higher income group had a lower stroke incidence over 10 years. The age standardised incidence rates of the NHIS beneficiaries decreased over the 10 years, but such a trend was not observed in medical aid beneficiaries (p=0.531) (figure 4, online supplemental table 3). The ratio of the incidence rate between medical aid beneficiaries and the highest income group was 1.5 (CI 1.43 to 1.58) in 2010, and 1.87 (CI 1.77 to 1.97) in 2019 (figure 4, online supplemental table 4).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Trends in the age-standardised incidence rate of ischaemic stroke per 100 000 person year according to income level (A) and rate ratio of ischaemic stroke incidence rates between medical aid beneficiaries and highest income group (B).
For the median age of stroke incidence, there was no significant change over time (Data not shown).
Discussion
This was a nationwide retrospective cohort study that analysed how stroke incidence changed for each sex during 10 years. For this, the crude rate and standardised rate were calculated, and subgroup analysis was performed for the incidence rates by age and household income.
The crude incidence of stroke, specifically in men, showed J-shaped association when plotting crude rate on vertical axis against year from 2010 to 2019 on the horizontal axis; it was on a downward trend, but has increased sharply since 2015. This is also true for the age standardised rate, with the overall age standardised rate declining, but it has been increasing since 2015. Previous studies report it as a detection bias, as people better detect minor stroke or change care-seeking behaviours. Since stroke severity was not included in our study, it is possible that the aforementioned causes resulted in the rise in incidence of stroke. The reason for the significant increase in 2019 may be that the expansion of the cerebrovascular MRI health insurance coverage policy has improved access to brain imaging, leading to an increase in MRI scans and, accordingly, an increase in diagnosis. In December 2019, brain-related MRI fiscal expenditures increased by 173.8% compared with the fiscal estimate. Although not all brain imaging was limited to strokes, it would have led to an increase in stroke diagnoses. As the access to brain imaging increases, an increase in stroke diagnoses is also observed in other countries.20 21
Even though the number of patients who had a stroke increased every year, the age-standardised rates decreased until 2018 but increased significantly in 2019 for all groups. This can be due to two reasons: first, the age of the population increased over the period of study,12 and second, because the risk factors for stroke were better managed.22 A decline in stroke incidence has also been observed in high-income countries,2 which is consistent with the findings of this study: age-standardised incidence rate of ischaemic stroke decreased from 1990 to 2014 in Scotland,23 decreased from 2003 to 2013 in Iran,4 decreased from 2005 to 2018 in Denmark,24 and showed a declining trend from 2003 to 2011, then increased until 2017 in Canada.25
In this study, the incidence rate by age group showed a decreasing trend in men over the age of 60, and women over the age of 40, while showing a stable trend in the younger age groups. According to the Netherlands national registries, ischaemic stroke incidences of ages 18–49 years increased from 1998 to 2010, and the increase was greater in those of 18–39 years of age.26 In the Framingham Study, there was no significant change in stroke incidence rate in those of 35–54 years of age, whereas there was a significant decrease in those aged 55 years and older.27 A Swedish study that tracked the incidence by age from 2001 to 2015 reported no change in the incidence in those under 65 years of age.3 The different trends in the incidence rate by age would be due to different contributions of the risk factors by age, and different trends in the prevalence of these risk factors. Temporal trends of stroke risk factors in the Korean population also showed different trends by age group.8–10 Further research is needed on the factors that cause stroke in different age groups, and how they affected the stroke incidence.
In the younger age groups, women are reported to have a higher incidence than men,28 29 and this phenomenon was also observed in the results of this study. Because this study was conducted using claim data, it is difficult to identify the cause of the higher incidence rates among women in their 20s than men. There is a possibility that the practice to rule out stroke in migraine with aura, which has a high prevalence in young women, contributed to the higher stroke incidence in women in this study.28
Income inequality in stroke incidence is well known.14–17 This study also showed that the stroke incidence decreased as the income level increased after adjusting for age, and the magnitude of this inequality increased over the 10 years. In particular, it was observed that the stroke incidence rate was highest in the medical aid beneficiary group. This seems to have many causes, such as a higher prevalence of risk factors of stroke30 in medical aid beneficiaries, and more cases due to excessive medical use, which should be further explored. Medical aid benefits are reported to use medical care a lot because of the low out-of-pocket expenses.31 Expanding the health insurance coverage of cerebrovascular MRI may complement the unfulfilled part of stroke diagnosis in patients with medical benefits.
A limitation of this study is that it is difficult to accurately capture the incidence because stroke incidence was calculated from claim data. However, NHIS claim data have very high sensitivity and specificity for stroke-related diagnosis.32 In addition, we tried to overcome this limitation by defining the stroke incidence rate by considering possible clinical situations, such as hospitalisation via the emergency room and brain imaging, along with the diagnosis of stroke, which further enhance the specificity and sensitivity of the study. We could not include patients who had an ischaemic stroke who stayed at home, died before imaging or had no imaging in very mild cases.
However, it is of great value to reveal the 10-year stroke incidence trend using the same criteria. Moreover, the study is valuable as a population-based nationwide incidence study. Although claim data are not as accurate as the registration data in calculating the stroke incidence, Korea does not have a registration system for the entire population. The criteria of this study include several elements of the ‘Core Criteria for a Comparable Study of Stroke Incidence’.33 Therefore, this nationwide study can be used as valuable data on the stroke incidence trend, and for international comparison. This contributes to global knowledge about stroke epidemiology and can be used as policy evidence about stroke-related medical use.
Conclusions
Stroke incidence rate has increased while the age-standardised rate has been on the decline since 2010 in South Korea. Incidence has decreased among the elderly but has not changed in the younger age groups. The income-based and sex-based inequality in stroke incidence persisted from 2010 to 2019. In the future, it will be necessary to study which factors have a causal relationship with the stroke incidence trends. In addition, strategies to reduce and prevent stroke in the younger age groups and in the low-income groups are needed.
Data availability statement
Data are available upon reasonable request. Data may be obtained from a third party and are not publicly available. Raw data were generated at Korea National Health Insurance Service. Derived data supporting the findings of this study are available from the corresponding author on request.
Ethics statements
Patient consent for publication
Ethics approval
The study protocol was approved by the Institutional Review Board of Konkuk University (IRB number: 7001355-202105-E-143). It was also approved in a review by the internal committee of NHIS (NHIS study number: NHIS-2021-1-479).
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
HK and YK contributed equally.
Contributors JL, HK and YK designed the study. JM and JS provided intellectual input into the content. HJ analysed the data. JL, JM and JS drafted the manuscript. HK and YK revised the article for intellectual content. All authors have read and approve of the final version. HK and YK are responsible for the final content as guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.