Article Text

Abstract
Objectives To investigate the impact of COVID-19 on the well-being of surgeons and allied health professionals as well as the support provided by their institutions.
Design This cross-sectional study involved distributing an online survey through medical organisations, social media platforms and collaborators.
Setting It included all staff based in an operating theatre environment around the world.
Participants 1590 complete responses were received from 54 countries between 15 July and 15 December 2020. The average age of participants was 30–40 years old, 64.9% were men and 32.5% of a white ethnic background. 79.5% were surgeons with the remainder being nurses, assistants, anaesthetists, operating department practitioners or classified other.
Main outcome measures Participants that had experienced any physical illness, changes in mental health, salary or time with family since the start of the pandemic as well as support available based on published recommendations.
Results 32.0% reported becoming physically ill. This was more likely in those with reduced access to personal protective equipment (OR 4.62; CI 2.82 to 7.56; p<0.001) and regular breaks (OR 1.56; CI 1.18 to 2.06; p=0.002). Those with a decrease in salary (29.0%) were more likely to have an increase in anxiety (OR 1.50; CI 1.19 to 1.89; p=0.001) and depression (OR 1.84; CI 1.40 to 2.43; p<0.001) and those who spent less time with family (35.2%) were more likely to have an increase in depression (OR 1.74; CI 1.34 to 2.26; p<0.001). Only 36.0% had easy access to occupational health, 44.0% to mental health services, 16.5% to 24/7 rest facilities and 14.2% to 24/7 food and drink facilities. Fewer measures were available in countries with a low Human Development Index.
Conclusions This work has highlighted a need and strategies to improve conditions for the healthcare workforce, ultimately benefiting patient care.
- COVID-19
- surgery
- occupational & industrial medicine
- mental health
Data availability statement
Data are available upon reasonable request. All data collected for this study, excluding participant names and contact details, will be made available with the study protocol on https://orthoglobe.org/Projects with the publication.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
An online anonymous survey was distributed worldwide through medical organisations, social media platforms and collaborators.
The survey included questions about participant demographics, physical, mental, financial and family well-being, as well as support from their institutions.
Questions on mental health were based on validated scoring systems and those on support were based on published recommendations.
The main limitations of the study were that responses were only collected from healthcare professionals in an operating theatre environment and that many collaborators themselves were surgeons.
Introduction
The COVID-19 outbreak can be traced back to Wuhan, China, where patients initially presented with pneumonia of unknown aetiology that led to a local-scale epidemiological alert on 31 December 2019.1 Thereafter, the WHO declared the outbreak ‘a public health emergency of international concern’ on 30 January 2020, due to an exponential rise in the number of cases as a result of human-to-human transmission.1 On 11 March 2020, the WHO then classified it as a pandemic.2 To date, COVID-19 has infected over 167 million people worldwide and been linked to over 3.47 million deaths.3
While advances have been made in the management and prevention of COVID-19, most notably via the advent and administration of vaccines,4 the impact of the COVID-19 pandemic on healthcare systems has been profound.5 In particular, there has been a significant effect on surgical practice that is likely to have long-term consequences for patients and healthcare professionals, specifically due to the increasing backlog of elective surgery,6 the negative impact on surgical training7 and the detrimental effect on overall mental health in both groups.8 9 The need for psychological support for surgical staff has been noted;9 however, there is a paucity of the literature on the impact of the COVID-19 pandemic on surgical team members’ overall welfare, especially with regard to domains other than mental health, such as physical, financial and family well-being.
Some previous studies on this topic have been limited to a single institution,9 a single country10–12 or a single surgical specialty with a sole focus on surgeons’ mental health.12 13 At present, the largest international study on the impact of workplace factors on the mental health of healthcare workers during the COVID-19 pandemic consists of 54.1% and 34.6% of responses from nurses and doctors, respectively, without a subgroup analysis of surgeons or surgical team members.14 The British Medical Association (BMA) also found that 45% of doctors were suffering from ‘depression, anxiety, stress, burnout or other mental health conditions’ pertaining to, or exacerbated by, COVID-19 and has therefore published recommendations to develop a long-term strategy to protect the well-being of healthcare staff.15 This includes the need for adequate personal protective equipment (PPE) along with training on its use as well as support services and facilities.
This study is the largest, international cross-sectional survey that explores the impact of the COVID-19 pandemic on the physical, mental, financial and family well-being of surgeons and allied health professionals, including anaesthetists, nurses, assistants and operating department practitioners. It has also investigated the support available to healthcare professionals as per BMA recommendations to help identify areas for improvement.
Methods
Study design and participants
This international, cross-sectional study has been reported according to Strengthening the Reporting of Observational Studies in Epidemiology guidelines. An online anonymous and voluntary survey was created on SurveyGizmo (now known as Alchemer) and distributed worldwide through medical organisations including the royal colleges of surgeons and other allied health professionals in various countries, social media platforms and collaborators. Collaborator status was given to any participant who was also able to gain 50 additional responses using a personalised link to the survey through which the number of responses gained could be tracked. Collaborators and the steering committee of this project form the OrthoGlobe Collaborative. One collaborator in Brazil was able to translate the form into Portuguese to increase the response rate from this region. Responses were collected over a 5-month period, from 15 July to 15 December 2020, from healthcare professionals currently in practice and based in an operating theatre environment, namely surgeons and anaesthetists at consultant, trust grade or trainee level, assistants, nurses and operating department practitioners.
Variables and outcomes
The survey consisted of three main sections: demographics, well-being and support. The first, demographics, included questions on age, gender, ethnicity (with options presented in line with the UK’s Office for National Statistics),16 marital status, role, grade and country. The options for grade were headed with UK-centric terms but each covers its counterparts from other countries. Consultants are synonymous with attendings, trainees with residents and interns and trust grade doctors with all other doctors that fall outside of the previously mentioned titles. The second section included questions about physical, mental, financial and family well-being since the start of the pandemic. Participants were asked if they had experienced any physical illness with or without COVID-19-related symptoms and all the questions on the Generalised Anxiety Disorder Assessment (GAD-7) and Patient Health Questionnaire (PHQ-9) to generate scores for anxiety and depression, respectively.17 18 For this group of questions on anxiety and depression, participants were asked to answer for a time 2 weeks before the start of the pandemic and after. They were also asked if they had experienced a decrease in salary and time spent with family between the time just before the start of the pandemic and now, the time at which this questionnaire was being filled out. The final section on support included questions based on recommendations by the BMA on improving the mental health and well-being of the medical workforce,15 19 specifically the availability and accessibility of PPE training on its use, a well-being guardian, occupational and mental/pastoral health services, support from managers and colleagues, sick leave regular breaks and 24 hours/7 days a week (24/7) rest and food facilities.
Study size and statistical methods
Assuming that an average of 29.6% of healthcare workers had anxiety and 29.7% had depression,20 the study would require a minimum sample size of 321 to estimate the expected proportion with 5% absolute precision and 95% confidence. The IBM Statistical Package for the Social Sciences V.26 for windows (IBM Corp) was used to perform Pearson χ² tests to compare the majority of variables, which were categorical.21 The only continuous variables were scores for anxiety and depression. The difference between scores for a time period before and after the start of the pandemic were used to categorise the responses into ‘increased’ or ‘decreased/no change’. Ethnicities were further grouped into ‘white’ and ‘other’ and countries were categorised into four according to their Human Development Index (HDI): very high, high, middle and low as described by the United Nations.22 Multivariable regression models were used to explore the relationships between variables while accounting for potential confounders. Model coefficients are presented as ORs with 95% CIs. Overall, 724 of 2314 responses had failed to provide key or outcome data so were not included in the final analysis (figure 1). A small number of participants selected ‘prefer not to answer’ where this was available. This has been included as a separate category in the analyses.

Flow chart illustrating response recruitment.
Public and patient involvement
There was no public or patient involvement in this study.
Results
Participants
Overall, 1590 complete responses came from 54 countries from 15 July to 15 December 2020. The average age of participants was between 30 and 40 years. Overall, 1032 (64.9%) were men and 516 (32.5%) of a white ethnic background. Overall, 1141 (71.8%) were married or in a relationship. Overall, 1265 (79.5%) were surgeons at consultant, trainee or trust grade level, 98 (6.2%) nurses, 86 (5.4%) assistants, 66 (4.2%) anaesthetists at consultant, trainee or trust grade level, 27 (1.7%) operating department practitioners and 48 (3.0%) classified as other. The latter included perfusionists, radiographers, managerial and administrative staff. Of the surgeons and anaesthetists combined, 680 (51.1%) were consultants, 588 (44.2%) trainees and 63 (4.7%) trust grade doctors. Overall, 720 (45.3%) participants came from a very high HDI country, 405 (25.5%) a high HDI country, 337 (21.2%) a middle HDI country and 128 (8.1%) a low HDI country.
Main results
Demographics and well-being
Figure 2 shows the proportion of participants who had become physically ill with or without COVID-19-related symptoms, an increase in anxiety and depression scores, a decrease in salary and a decrease in time spent with family. At the time the questionnaire was being answered, 746 (46.9%) had a score greater than 5 indicating mild-to-severe anxiety, based on the GAD-7. Overall, 716 (45.0%) had a score greater than 5 indicating mild-to-severe depression, based on the PHQ-9. Between a time 2 weeks before the start of the pandemic and after, there was a significant increase in mean scores for anxiety (2.24 (CI=2.01 to 2.46)) (p<0.0001) and depression (4.22 (CI=3.98 to 4.46)).
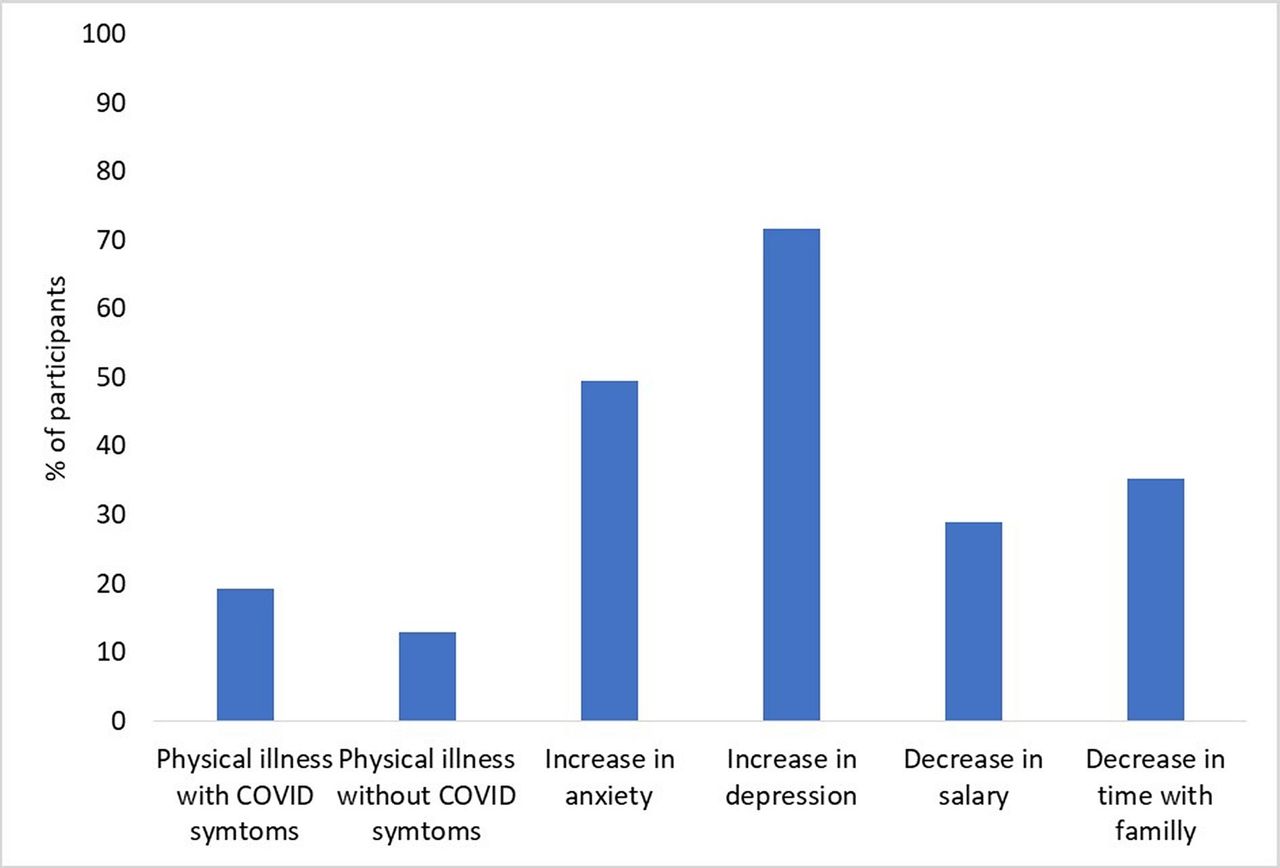
The proportion of participants (%) that had become physically ill with or without COVID-19-related symptoms, an increase in anxiety and depression scores, a decrease in salary and time spent with family.
Pearson χ² tests (shown in online supplemental appendix table 1) indicate a significant difference in physical illness across age groups (p=0.013), ethnicities (p<0.001) and occupations (p=0.010). Anxiety scores differ across ethnicities (p<0.001) and depression scores across age groups, (p=0.007), gender (p<0.001), ethnicities (p<0.001), marital status (p<0.001) and occupations (p=0.003). The difference in the number of participants with a decrease in salary is significant across age, gender, ethnicity, marital status and occupational groups (all p<0.001) as is a decrease in time spent with family across age, marital status and occupational groups (all p<0.001).
Supplemental material
Multivariable analyses to determine risk factors for physical illness, mental illness and decrease in salary and time with family
Support measures and well-being
Figure 3 shows the proportion of participants that had access to different support measures including always having access to PPE, access to training on its use, a well-being guardian, easy access to occupational health, access to mental health/pastoral services, support from managers, support from colleagues, sick leave when needed, regular breaks, 24/7 rest facilities and 24/7 food and drink facilities.
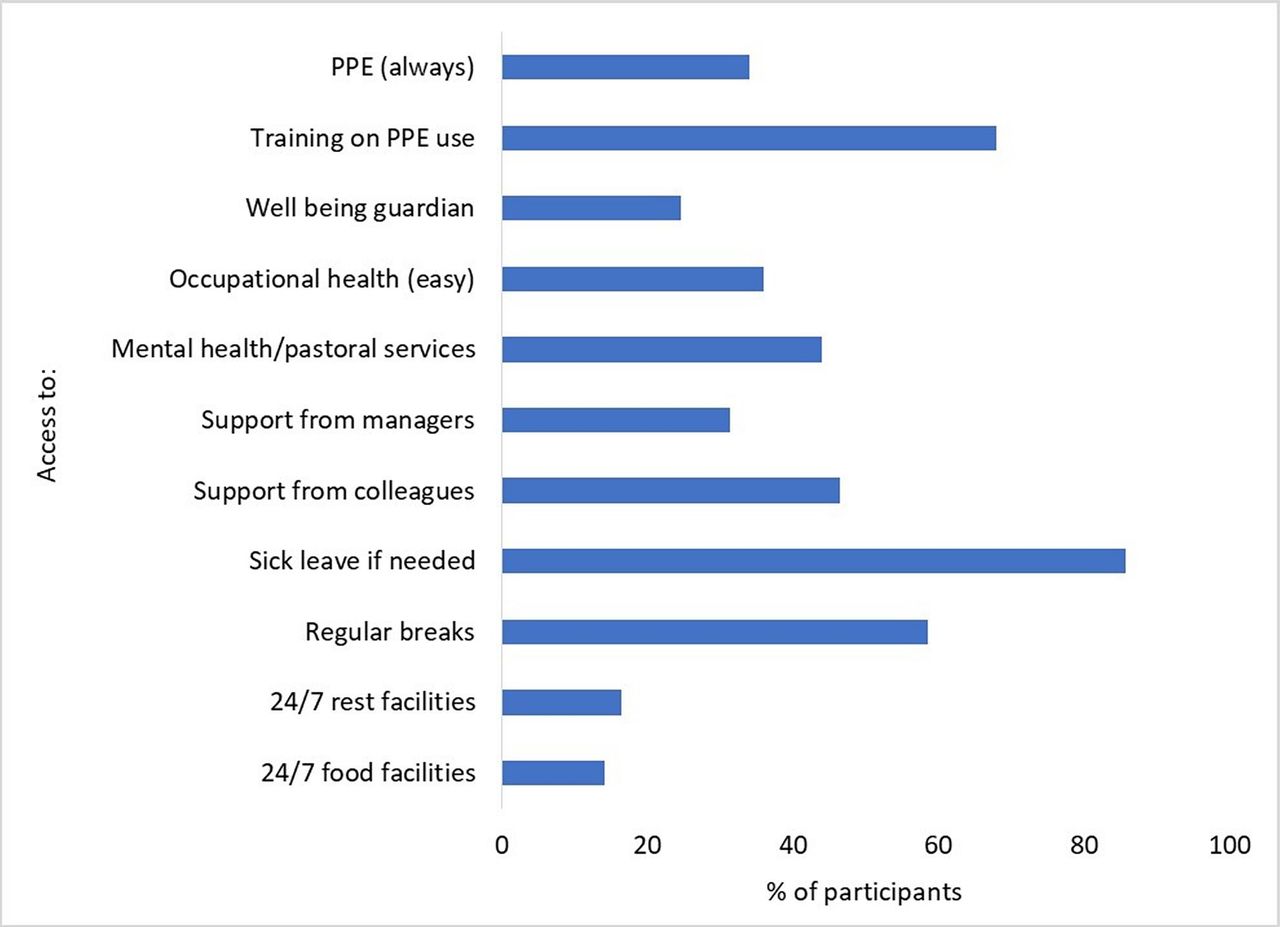
The proportion of participants that had access to different support measures including always having access to personal protective equipment (PPE), access to training on its use, a well-being guardian, easy access to occupational health, access to mental health/pastoral services, support from managers, support from colleagues, sick leave when needed, regular breaks, 24/7 rest facilities and 24/7 food and drink facilities.
Pearson χ² tests (shown in online supplemental appendix table 2) indicate a significant difference in physical illness and access to PPE, training in its use, occupational health and mental health services, support from managers and colleagues, sick leave when needed, regular breaks (all p<0.001) and 24/7 food facilities (p=0.049). The presence of an increase in anxiety differs significantly with access to PPE (p=0.002), a well-being guardian (p<0.001), occupational health (p<0.001), mental health services (p=0.018), support from managers (p<0.001), support from colleagues (p=0.02) and regular breaks (p=0.021). The presence of an increase in depression differs significantly with access to PPE (p<0.001), a well-being guardian (p=0.021), occupational health (p=0.004), support from managers and colleagues (p=0.021), sick leave if needed (p=0.011) and regular breaks (p<0.001). There was a significant difference in the availability of all support measures across country HDI groups, all with p values of less than 0.050.
Multivariable analyses
The results of multivariable analyses to determine risk factors for physical illness, mental illness and decrease in salary and time with family are shown in table 1. Multivariable analyses looking into the effect of country HDI on access to supportive measures are shown in figure 4 (and online supplemental appendix table 3).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Multivariable analyses looking into the effect of country Human Development Index (HDI) on access to supportive measures. Marker represents OR and bars the 95% CI, *p<0.05 (statistically significant). PPE, personal protective equipment.
Physical illness
Physical illness with COVID-19-related symptoms was significantly more likely, according to the OR, in those with reduced access to PPE, regular breaks and time with family. Physical illness without COVID-19-related symptoms was more likely in trust grade doctors compared with consultants and those with reduced access to PPE.
Mental illness
An increase in anxiety score was less likely in the other ethnicity group and more likely with a decrease in salary. An increase in depression score was less likely if married or in a relationship and more likely if a trust grade doctor rather than a consultant, experiencing a decrease in salary, or less time with family.
Salary and time with family
The 30–40 age group was less likely to experience a decrease in salary as was any role or occupation other than a consultant. The other ethnicity group and those married or in a relationship were less likely to have a decrease in time spent with family. Trainees and nurses were more likely than consultants to experience a decrease in time with family.
Country HDI and support measures
Participants from a country with a low HDI were significantly less likely to have access to PPE (OR 18.30; CI 7.46 to 44.87; p<0.001), occupational health (OR 4.997; CI 2.55 to 9.81; p<0.001), mental health services (OR 3.36; CI 1.82 to 6.20; p<0.001) and 24/7 food facilities but more likely to have support from managers (OR 0.29; CI 0.13 to 0.63; p=0.002) and access to sick leave when needed (OR 0.38; CI 0.17 to 0.88; p=0.023) compared with a very high HDI country.
Discussion
Overall, 1590 complete responses from surgical team members across 54 countries were obtained and the following domains were analysed: physical health, including illness related and unrelated to COVID-19; mental health as per validated anxiety (GAD-7) and depression (PHQ-9) scores; financial and family well-being; and access to PPE along with training in its use, support in the form of access to a well-being guardian, occupational health, mental health/pastoral services, support from managers and colleagues, sick leave, regular breaks, as well as facilities for rest and food.
Almost a third of respondents had become physically ill since the start of the pandemic, of which over half were due to COVID-19 symptoms. Physical illness was more likely in those with reduced access to PPE and regular breaks, which is in keeping with the well-documented risk factors for developing a coronavirus infection.23 There are a range of consequences when healthcare workers become physically ill, especially if they require sick leave as this can have a knock-on effect on the remaining staff, who will have to work short-staffed or have to work unplanned shifts.24 In the context of surgical teams, this can also have a subsequent impact on planned operations and service provision.
Validated scoring systems were used to show that 45% were suffering from mild-to-severe depression and 47% with mild-to-severe anxiety. The scores were significantly higher than a self-reported time 2 weeks before the start of the pandemic. The prevalence of mild–severe depression and anxiety in this study are similar to the upper limits of 8.9%–50.4% and 14.5%–44.6%, respectively, reported in a recently published review on the impact of COVID-19 on the mental health of healthcare workers, formed of 24 studies of which the majority were also based on validated scoring systems.20
An increase in anxiety score was less likely in the other ethnicity group, an unexpected result in the light of a known higher death rate from COVID-19 among other ethnic groups but one that may be influenced by the fact that this group was less likely to have experienced a decrease in time spent with family.25 An increase in depression score was less likely if married or in a relationship and more likely in those who spent less time with family, consistent with the literature as widely recognised protective factors.11 An increase in depression score was more likely if the participant was a trust grade doctor rather than a consultant. This could be due to the fact that more junior doctors were likely to experience redeployment and a change of clinical duties, which has now been linked to an increased risk of depression,14 as well as a decrease in time spent with family.
Understandably, those with a decrease in salary were more likely to have an increase in anxiety and depression scores, likely due to the added financial burden and impact on their personal lives. The 30–40 age group was less likely to experience a decrease in salary as was any role or occupation other than a consultant as consultants, generally of an older age group, were likely to work less due to the suspension of non-urgent elective surgeries and private practice.6 Other aspects of physical and mental health, such as fatigue, stress and drug consumption, and other potential risk factors, including whether participant’s were involved in the care of patients with COVID-19, could have been investigated; however, this would have made the questionnaire considerably longer and a possible hindrance to complete responses.
An analysis of supportive measures has highlighted an association between HDI and the availability of resources. However, where support from managers and access to sick leave when needed was more likely in lower HDI countries, this may be accounted for by contextual factors, such as understaffing and guilt from taking time off work, that were not considered in this study.26 Recommendations from the BMA were used as a standard on a global scale because there were no other widely accessible guidelines on health workforce support measures for institutions at the time the questionnaire was constructed.
Another limitation is the fact that the great majority of participants were surgeons. The idea to distribute the survey to staff in an operating theatre environment to balance covering a range of cadres with feasibility and ease may have contributed to this. Most of the collaborators collecting responses were also surgeons who may have been inclined to distribute surveys to their own colleagues. The response rate could have also been improved by translating the questionnaire into more languages from English than just Portuguese and considering a lack of internet access in certain areas; however, this would have increased the time taken to conduct the study significantly. Despite this, the study forms a large, international, multispeciality, multidisciplinary, cross-sectional assessment of the overall well-being of surgical team members and the support available to them.
Improving staff well-being is invaluable. Adverse events, including medical errors, are a leading cause of death and disability worldwide, costing 64 million disability adjusted life years annually, with a major contributor being human factors.27 Hence, it would be in the interest of public health to implement measures that improve well-being for healthcare professionals, who can then provide better patient care.
Conclusion
In conclusion, this international cross-sectional study has established the negative impact of COVID-19 on the holistic well-being of surgical team members. It is the first to assess the availability of and access to supportive measures at institutions on a global scale. This can form the basis of quality improvement projects at the local level to raise the overall standards of working conditions for healthcare professionals, which will inevitably have a positive effect on the care of patients.
Data availability statement
Data are available upon reasonable request. All data collected for this study, excluding participant names and contact details, will be made available with the study protocol on https://orthoglobe.org/Projects with the publication.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants but ethics approval was not required according to the Integrated Research Application System for the Health Research Authority. It had been approved and endorsed by the Royal College of Surgeons England COVID-19 Research Group.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @zorthodiaries, @TheSiddRaj, @orthoepi, @NegidaMD, @sobtianshul, @rawadhmd, @BrennanSurgeon, @ali_narvani, @surgasst441, @MoAImam
Collaborators The OrthoGlobe Collaborative: Ghayur Abbas, Ademola Adetoyese Adeyeye, Ahmad Nayef Althaher, Firas Arnaout, Alexis P Arnaud, Muhammed Elhadi, Ana Vega Carreiro de Freitas, Krishna Kumar Govindarajan, Sachin Y Kale, Harish Neelamraju Lakshmi, Luis Carlos Uta Nakano, Abdulrasheed A Nasir, Francesco Pata, Chandramohan Ravichandran, April Camilla Roslani, Edmund Leung-Kai Yau, Luiz Fernando Santetti Zanin.
Contributors ZJ, ANe, CFAY, ASo and MAI designed and planned the study. ZJ, SR, ASa, SL, ANe, CFAY, ASo, NB, REF, HA, RH, NQ, BS, PAB, AH, ANa, AJ, MAI and all OrthoGlobe Collaborators acquired data by distributing the survey and collecting responses, ZJ, SR, ASa, SL, ANe, NB, REF and MAI analysed and interpreted the data. ZJ, SR and NB wrote up the study. ZJ, SR, ASa, SL, ANe, CFAY, ASo, NB, REF, HA, RH, NQ, BS, PAB, AH, ANa, AJ and MAI reviewed and approved the final manuscript. MAI is responsible for the overall content as guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.