Article Text

Abstract
Objectives Since the onset of the COVID-19 pandemic in 2020, there have been plausible suggestions about the need to augment vitamin D intake by supplementation in order to prevent SARS-CoV2 infection and reduce mortality. Some groups have advocated supplementation for all adults, but governmental agencies have advocated targeted supplementation. We sought to explore the effect of the COVID-19 pandemic on both vitamin D status and on the dose of new-to-market vitamin D supplements.
Setting University hospital, Dublin, Ireland.
Participants Laboratory-based samples of circulating 25-hydroxyvitamin D (25OHD) (n=100 505).
Primary and secondary outcome measures Primary outcomes: comparing yearly average 25OHD prior to the pandemic (April 2019 to March 2020) with during the pandemic (April 2020 to March 2021) and comparing the dose of new-to-market vitamin D supplements between 2017 and 2021 (n=2689). Secondary outcome: comparing prevalence of vitamin D deficiency and vitamin D excess during the two time periods.
Results The average yearly serum 25OHD measurement increased by 2.8 nmol/L (61.4, 95% CI 61.5 to 61.7 vs 58.6, 95% CI 58.4 to 58.9, p<0.001), which was almost threefold higher than two similar trend analyses that we conducted between 1993 and 2016. There was a lower prevalence of low 25OHD and a higher prevalence of high 25OHD. The dose of new-to-market vitamin D supplements was higher in the years 2020–2021 compared with the years 2017–2019 (p<0.001).
Conclusions We showed significant increases in serum 25OHD and in the dose of new-to-market vitamin D supplements. The frequency of low vitamin D status reduced indicating benefit, but the frequency of vitamin D excess increased indicating risk of harm. Rather than a blanket recommendation about vitamin D supplementation for all adults, we recommend a targeted approach of supplementation within current governmental guidelines to at-risk groups and cautioning consumers about adverse effects of high dose supplements on the market.
- COVID-19
- NUTRITION & DIETETICS
- Calcium & bone
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This is a laboratory-based 25-hydroxyvitamin D (25OHD) trend analysis that includes a large sample size.
This trend analysis is compared with two prior trend analyses dating back to 1993.
This is not a population-based representative sample and is subject to selection bias.
There is no clinical information about reason for 25OHD testing or about vitamin D supplementation.
Introduction
Vitamin D is an essential micronutrient in all age groups for bone and muscle health.1–4 Vitamin D may have a role in extraskeletal health such as the immune response to acute respiratory illnesses,5 which is pertinent during the COVID-19 pandemic.6 Following the onset of the pandemic, some reports advocated blanket oral supplementation to entire populations with doses ranging from 20 to 50 µg daily,7–10 which are in excess of vitamin D intake requirement as specified by governmental agencies in Europe and North America.1–4 By contrast, other groups have countered this blanket recommendation, favouring a targeted approach based on modelling of total vitamin D intakes.11 12
Governmental reports, which have been issued over the past decade prior to the pandemic, are based on similar health outcomes such as musculoskeletal health, falls and total risk of mortality, but not on immune response to infection.1–4 Subsequently, governmental agencies from England and Ireland issued advice about vitamin D supplementation during the pandemic.13 14 This advice targeting at-risk populations included measures to facilitate supplementation13 14 (table 1) given the ongoing concerns about vitamin D inadequacy across Europe.15 16
Vitamin D intake recommendations from governmental agencies and from COVID-19 vitamin D advocate groups
Ensuring adequate vitamin D intake across all age groups is a challenging population health task. Vitamin D intake requirements must be modelled to cover total intake because vitamin D supply has various sources: skin production on exposure to ultraviolet light, natural foods, fortified foods and supplements. There is almost complete unanimity about total vitamin D intake population requirements across governmental agencies for North America and for Europe.1–4 In circumstances of minimal or no sunlight exposure, the total oral intake requirement varies between 10 and 20 µg daily (400 to 800 IU daily).1–4 The pre-eminent measure of vitamin D status is the measurement of the circulating vitamin D metabolite, 25-hydroxyvitamin D (25OHD).
We have been engaged in clinical research on 25OHD since the 1970s.17 We have noted substantial improvement in vitamin D status over the past five decades. In our early studies in Ireland, we noted the primacy of oral intake over sunlight exposure for both the prevention and correction of vitamin D deficiency.18–21 Following the advent of voluntary milk fortification in Ireland in the 1980s at 1 µg/100 mL (but more recently some milk products fortify at 2 µg/100 mL) and the ready availability of low-dose vitamin D supplements, vitamin D status has improved substantially.22 In more recent years, we reported instances of hypervitaminosis D raising concerns about excessive oral intake of vitamin D.23
We have published two trend analyses of laboratory-based 25OHD results: the first trend study reported 25OHD from 1993 to 2013 that incorporated a time series analysis to predict 25OHD trend from 2014 to 201624; the second trend study reported 25OHD from 2014 to 2016 that confirmed the forecast analysis from the first study.25 We reported that over 24 years in Ireland from 1993 to 2016 that the yearly average 25OHD concentration increased by about 1 nmol/L/year. As early as 2014, we recognised a dual concern about vitamin D status in Ireland: hypovitaminosis D in at-risk groups; and hypervitaminosis D due to high supplemental intake, especially from over-the-counter preparations in individuals who already have adequate vitamin D status.23 One of the consequences of raising public awareness, whether it be from governmental agencies or from professional bodies, is the increased supply of vitamin D supplements, which are available for over-the-counter purchase.
We sought to explore the effect of COVID-19 pandemic on vitamin D status from April 2020 to March 2021 given the conflicting advice: governmental agencies promoting vitamin D supplementation in at-risk groups, and groups advocating blanket recommendations for vitamin D supplementation to all adults. We examined vitamin D status before and during the first year of the pandemic when public debate and temporary emergency legislative measures (such as social distancing and mask wearing) were focused on how people could protect themselves against COVID-19. We also assessed the Food Safety Authority of Ireland (FSAI) notification database for new-to-market vitamin D supplements notified between 2017 and 2021; all food supplements placed on the Irish market must be notified to the FSAI.26
Methods
Data mining
Our laboratory data system was mined to identify all 25OHD samples over a 24-month period from April 2019 to March 2021: pre-COVID-19 era being represented by 12 months from April 2019 to March 2020, and the COVID-19 era being represented by April 2020 to March 2021. In order to identify duplicate samples, the following identifiers were extracted: date of birth and medical record number. Additional data included age, sex, referral source (either hospital consultant or general practitioner) and date of 25OHD test. The sample size for the 24 months from April 2019 to March 2021 was 137 963; after excluding those with more than one sample during the 2 years (n=37 458), the final sample was trimmed to 100 505. Regarding those cases with more than one 25OHD sample, the analysis was based on the 25OHD being the first sample, which hereafter is termed the first in sequence. A secondary analysis was performed, whereby the selected 25OHD of those cases with more than one sample was the final sample, which hereafter is termed the last in sequence.
In order to enable closer monitoring of food supplements, Ireland took up the option within the EU Directive regulating food supplements of mandating food businesses, which place food supplements on the Irish market, to notify all details on the products to the FSAI.26 We mined this FSAI notification database about new-to-market vitamin D supplements that were notified between January 2017 and December 2021 (n=2689).
Public and patient involvement
It was not appropriate or possible to involve patients or the public in the design, or conduct, or reporting, or dissemination plans of our research.
Study design
The primary analysis entailed a comparison of serum 25OHD concentration in the pre-COVID-19 era, hereafter referred to as group 1, with 25OHD in the COVID-19 era, hereafter referred to as group 2. The prevalence estimates for categories of 25OHD in the two groups were calculated according to the following thresholds: <30 nmol/L; 30–50 nmol/L; 50.1–125 nmol/L; and >125 nmol/L. In addition, a composite analysis of the entire group over the 2 years was performed in order to assess vitamin D status according to sex and different age groups.
The list of vitamin D supplements that were notified to the FSAI between 2017 and 2020 was collated with respect to the total dose of vitamin D. Vitamin D supplements were categorised as high dose according to two different standards: first, if they exceeded the tolerable upper intake level (UL) of 100 µg, which is defined as is the highest level of long-term daily intake of a nutrient from all sources that is judged to be unlikely to pose a risk of adverse health effects to humans27; and second, if they exceeded the maximum safe level (MSL) of 75 µg, which is defined as maximum amount of vitamin D that can safely be added to food supplements targeting teenagers and adults in Ireland. The MSL is calculated using a risk assessment approach: it is equal to the UL minus the estimated intake of vitamin D intake in the highest consumers (95th percentile of intake from both base diet and fortified foods).28
Analytical methods
Serum 25OHD concentrations were quantified using the Elecsys Vitamin D total II (Roche Diagnostics GmbH, Mannheim, Germany) automated competitive binding protein assay, which measures total vitamin D, including isomers in the form of the C3 epimer as well as 24,25OHD metabolites. This is not specifically corrected for; rather, an assumption is made that there is a non-statistically significant difference in the per cent concentration of vitamin D metabolites relative to the measured concentration in patient samples tested over the 3-year period. The average interassay coefficients of variation (CV) for the 25OHD assay determined over the period studied were as follows: 14.6% at a mean concentration of 37.7 nmol/L, 8.7% at a mean concentration of 74.6 nmol/L and 7.6% at a mean concentration of 112.1 nmol/L. Functional sensitivity was verified at 15 nmol/L (%CV<20%). To ensure a high standard of analysis for serum 25OHD concentrations, the laboratory participates in an external quality assurance scheme: the Vitamin D External Quality Assessment Scheme (DEQAS).29 During the 2-year period 2019–2021, our assay displayed a mean bias of 1.12% from target values provided by the Centers for Disease Control and Prevention (Atlanta, Georgia, USA) using their isotope dilution LC-MS/MS Reference Measurement Procedure.30 Assay performance also met DEQAS defined quality assurance performance criteria. For samples with undetectable 25OHD (<15 nmol/L), the result was censored at 14.9 pmol/L. For samples with high 25OHD (>175 mol/L), the result was censored at 175.1 nmol/L.
Statistical analysis
Descriptive statistics are presented as number and per cent for categorical variables and as mean (95% CIs) or median (IQR) for continuous variables. Differences in independent categorical variables were tested by χ2. Differences between two means for 25OHD (both yearly and monthly) were tested by independent samples t-test using Levene’s test for equality of variances. To account for multiple testing of monthly mean 25OHD, the Benjamini-Hochberg correction method was applied with a false discovery rate of 0.05; p values were converted to corresponding q values for the determination of true significance. A one-way analysis of variance was conducted to explore the impact of year on dose of new-to-market vitamin D supplements; post-hoc comparisons were made using Tukey honestly significant difference (HSD) test. Statistics were considered significant if p value<0.05. Analyses were performed using IBM SPSS Statistics V.25 (Armonk, New York, USA).
Results
Group 1 and group 2 were similar with respect to age, sex and source of referral (table 2). Mean 25OHD was 2.8 nmol/L higher in group 2 compared with group 1 (61.4, 95% CI 61.5, 61.7 nmol/L vs 58.6, 95% CI 58.4, 58.9 nmol/L, p<0.001) (table 2). If the 25OHD duplicate result was selected as last in the sequence, then mean 25OHD was 5.1 nmol/L higher in group 2 compared with group 1 (63.3, 95% CI 63.2, 63.6 nmol/L vs 58.2, 95% CI 58.0, 58.5 nmol/L, p<0.001). In group 2 compared with group 1, there was a lower per cent (12.0% vs 13.4%) of low vitamin D status (25OHD<30 nmol/L) but a higher per cent (2.1% vs 1.7%) of high vitamin D status (25OHD>125 nmol/L) (p<0.001) (table 2).
Descriptive statistics for year prior to COVID-19 pandemic (Group 1) and for year during COVID-19 pandemic (Group 2)
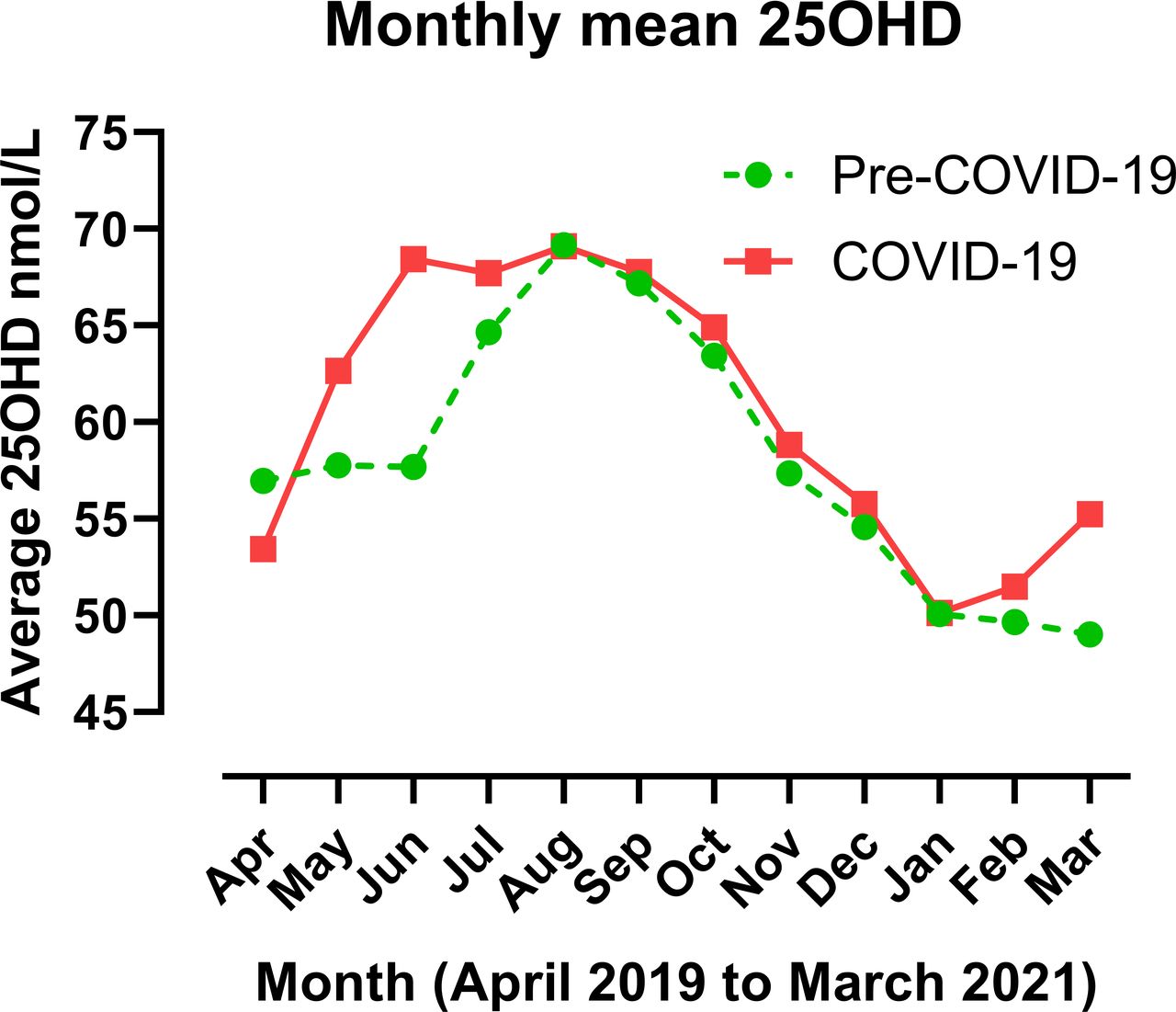
The monthly 25OHD trimmed values for both groups are plotted showing the seasonal variation (figure 1). The average seasonal change in 25OHD from nadir to peak was almost identical for both at 20.2 nmol/L in group 1 and 20.1 nmol/L in group 2. Starting the monthly sequence in April 2020, the monthly mean 25OHD in group 2 compared with group 1 following Benjamini-Hochberg correction for multiple comparisons was significantly higher in the following months: May (q<0.001), June (q<0.001), July (q<0.001), October (q=0.012), November (q=0.012), December (q=0.012), February (q=0.003) and March (q<0.001) (figure 1).

Monthly mean 25-hydroxyvitamin D (25OHD) during COVID-19 pandemic was significantly higher than prior to the pandemic for the following months: May, June, July, October, November, December, February and March (see Results).
For the composite analysis, mean 25OHD was higher in women compared with men (61.3, 95% CI 61.1 to 61.5 nmol/L vs 56.9, 95% CI 56.7 to 57.3 nmol/L, p<0.001), and in those sourced from primary care compared with hospital care (60.7, 95% CI 60.5 to 60.9 nmol/L vs 57.4, 95% CI 57.0 to 57.7 nmol/L, p<0.001). Vitamin D status according to age categories showed that infants and toddlers had the lowest prevalence of 25OHD<30 nmol/L and the highest prevalence for 25OHD>125 nmol/L (table 3). Regarding vitamin D status according to sex, adult females had better vitamin D status than males, but in infants a greater per cent of females compared with males had both the lowest and the highest prevalence of vitamin D status, but the numbers were small (table 3).
Crosstabulation of vitamin D status according to age categories and sex in the entire group from April 2019 to March 2021
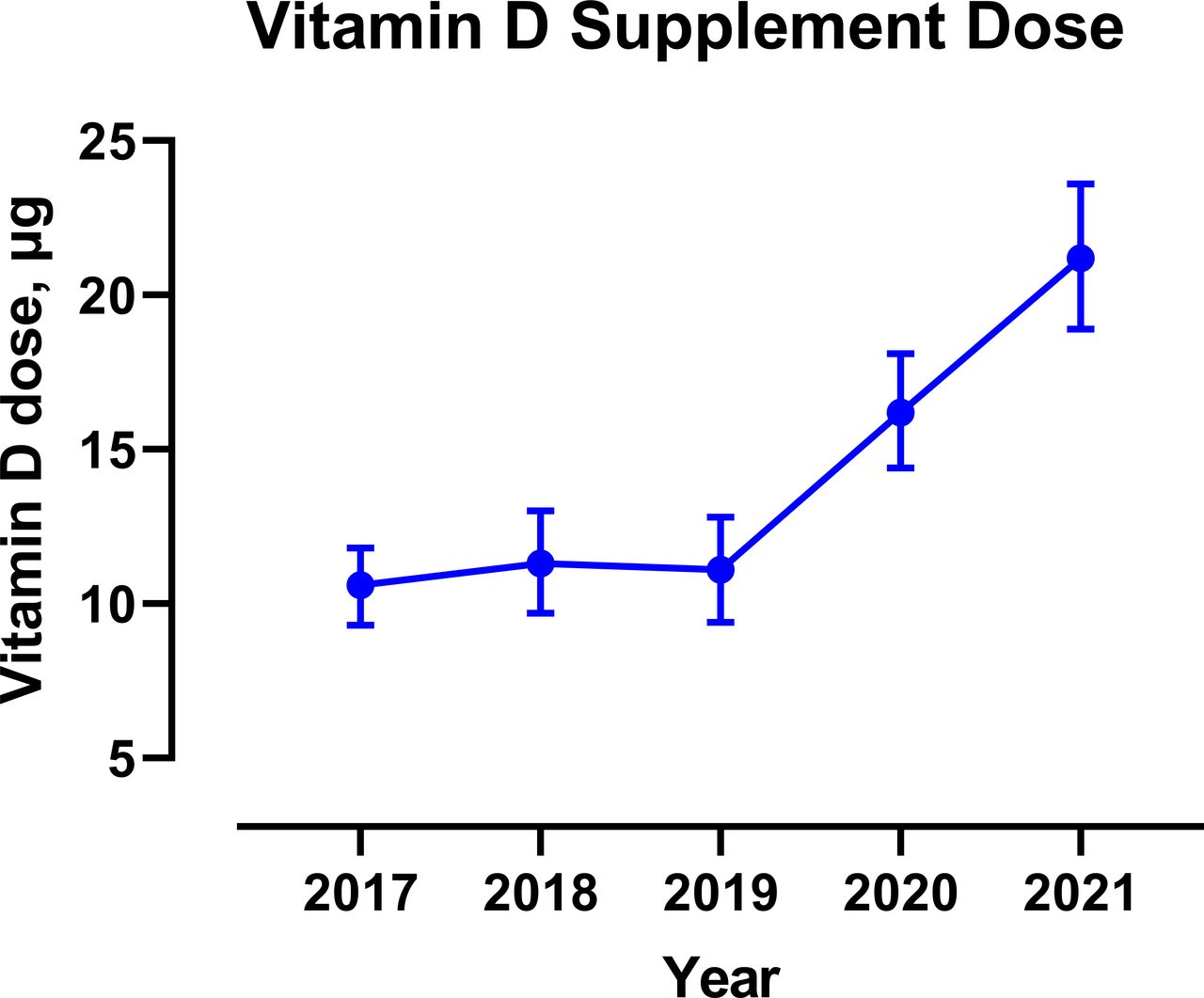
Regarding the analysis of the FSAI notification database of new-to-market vitamin D supplements notified between 2017 and 2021, there was a significant difference in mean vitamin D doses over the 5 years (p<0.001). Post-hoc comparisons showed no differences among 2017, 2018 and 2019, but higher in 2020 compared with the 2017, 2108 and 2019 (respectively, p=0.002, p=0.021, p=0.008) and higher in 2021 compared with 2020 (p=0.002) (figure 2). Regarding the proportion of food supplement products notified that provide daily amounts of vitamin D exceeding the UL of 100 µg (1%, n=9) and the MSL of 75 µg (3%, n=80), the majority were notified during the COVID-19 pandemic (n=3 in 2017–2019 vs n=6 in 2020–2021 above the UL; n=18 in 2017–2019 vs n=62 in 2020–2021 above the MSL) (table 4).

{kind=link}
{kind=link}
Yearly mean (95% CIs) new-to-market vitamin D supplement doses, which were significantly higher in 2020 and 2021 compared to 2017, 2018 and 2019 (see Results).
Descriptive statistics of new-to-market vitamin D supplement doses from 2017 to 2021
Discussion
In a trend analysis of laboratory-based 25OHD samples comparing yearly average 25OHD in the 12 months before the onset of the COVID-19 pandemic (April 2019 to March 2020) with the first 12 months of the COVID-19 pandemic in Ireland (April 2020 to March 2021), we showed the average yearly 25OHD increased by 2.8 nmol/L/year. This yearly trend was nearly threefold higher than the average yearly increase in 25OHD of 1 nmol/L/year that we recorded in two prior trend analyses of laboratory-based samples from 1993 to 2016.24 25 If the 25OHD duplicate was selected as last in sequence for the trend analysis, then average 25OHD increase during the pandemic was even higher at 5.1 nmol/L/year. We observed benefit with respect to their being lower prevalence of 25OHD<30 nmol/L, but to a lesser extent there was a higher prevalence of 25OHD>125 nmol/L. Higher average monthly 25OHD was noted in nearly all months except at the end of summer, suggesting an increase in the prevalence of vitamin D supplementation. The dose of new-to-market vitamin D supplements increased significantly during the pandemic with an increase in the frequency of supplements exceeding the UL and the MSL.
The 25OHD threshold for diagnosis of vitamin D deficiency depends on the approach: whether is it viewed as being population-based1 4 or as being case-based.31 For a population-based approach, the Institute of Medicine (IOM) for the USA and Canada in 2011 used a statistical probability method to determine the prevalence of nutrient inadequacy.32 The IOM set a 25OHD threshold of 30 nmol/L. IOM referred to 25OHD as a ‘biomarker of exposure’ but not as a ‘biomarker of effect’, which means that 25OHD is the pre-eminent measure of total vitamin D intake, but it only estimates risk of disease. Thus, 25OHD below 30 nmol/L was defined by IOM as ‘risk of deficiency’. Similarly, the Scientific Advisory Committee on Nutrition for the UK set a 25OHD threshold of 25 nmol/L.4 Governmental agencies set their specifications for vitamin D intake based on total vitamin D intake. Modelling intake from all sources estimates the shortfall in vitamin D intake that can be bridged by supplemental intake33. Whereas, a case-based approach, which is guiding clinicians about the need for supplemental vitamin D on an individual basis, sets higher 25OHD thresholds—for example, the European Calcified Tissue Society set a 25OHD threshold at 50 nmol/L.31 Case-based approaches tend to give guidance about 25OHD monitoring.
Governmental agencies have adopted a precautionary approach to vitamin D harm. The tolerable UL from all oral sources of vitamin D (natural foods, fortified foods and supplements) in those with minimal sunlight is 100 µg (4000 IU) daily.1 34 The UL is 10-fold higher than the average total vitamin D intake requirement for healthy adults.1 The UL is not intended as a target intake; rather, the risk for harm begins to increase once vitamin D intake surpasses this level.35 In Ireland, over-the-counter vitamin D products are regulated by the FSAI. The UL determines the maximum dose of a vitamin D product that can be marketed. Labelling requires that the dose not exceed the UL.
In addition to the UL, in Ireland the FSAI has also published guidance for food business operators regarding the MSL of vitamin D that can be added to food supplements in Ireland.28 Since the UL encompasses daily oral vitamin D intake from all sources (base diet, fortified foods and food supplements), then the maximum safe dose of a vitamin D supplement should be less than the UL. Following a risk assessment approach, the FSAI deemed that the MSL for vitamin D in food supplements is 75 µg per day for teenagers and adults.28 In our analysis of new-to-market vitamin D supplements, we noted that the frequency of supplements exceeding the MSL had increased from 0.8% to 6.1% between 2017 and 2021.
During the COVID-19 pandemic, some groups have advocated the need for mass vitamin D supplementation in order to enhance the immune response to SARS-CoV2 infection.7 9 10 36 37 The European Food Safety Authority permits stating that benefit from vitamin D supplementation covers the normal functioning of the immune system without specifying a vitamin D intake for this benefit.38 There is some evidence of benefit from vitamin D in randomised controlled trials that have been conducted during the pandemic but there is wide variation in vitamin D doses.39–44 A Mendelian randomisation study did not support an association between 25OHD and COVID-19 susceptibility, severity45 or hospitalisation; similar findings have been reported in a UK biobank study.46 Further studies should provide clarity about benefit and optimal vitamin D schedules. These studies might provide cogent evidence for higher vitamin D intake requirements that could form part of population-based or case-based recommendations. Meanwhile, the likely effect of advocating for mass supplementation is that individuals, who are best able to self-medicate, are the ones who are least likely to need supplementation. Frail older adults, lower socioeconomic groups and minority ethnic groups are more likely to have lower 25OHD and are less likely to afford the means for supplementation.47 48 It is better to have a targeted approach to vitamin D supplementation such as the frail older adult.13 14
Mandatory fortification of foodstuffs with vitamin D, which has been shown to be effective in Finland,49 poses many challenges,50 but has the major advantage of reaching lower socioeconomic groups excluded from the benefits of foods voluntarily fortified with vitamin D due to the significantly higher prices of such foods. Voluntary fortification, while less satisfactory than mandatory fortification, is effective at ameliorating seasonal decline in 25OHD, as has been shown in Ireland.22 Fortification with any nutrient (whether mandatory or voluntary) in addition to supplementation (whether mandatory or voluntary), can result in total nutrient intakes that are higher than requirement and may even exceed the UL, especially if nutrient intake targets the recommended daily allowance (RDA) and not the estimated average requirement.51
Our trend analysis has many limitations. First and foremost, it is not a representative sample because samples are not collected as part of a population-based survey. We do not have information on the clinical indication for the test nor do we know whether patients were on vitamin D supplements or had an underlying condition that predisposed to vitamin D deficiency. The plot of the seasonal variation of 25OHD is open to many interpretations, such as: more outdoor activity during the first lockdown accounting for the increased in 25OHD early in the pandemic from May 2020 to July 2020, coupled with higher supplemental intake during the winter months accounting for higher 25OHD from October 2020 to March 2021 (excepting January 2021). The 12-month trend analysis is too short to declare with any certainty that the COVID-19 pandemic has contributed to a shift upwards in the yearly average 25OHD increase or if it just a transient trend upwards due to the unique circumstances of living through legislatively enforced measures implemented globally to protect people from a pandemic while the search for solutions—such as the potential benefit of vitamin D—was the highest profile news story.
In conclusion, we report in Ireland a laboratory-based trend analysis of 25OHD showing that the rise in yearly average 25OHD increased by about threefold during the first year of COVID-19 pandemic compared with our prior trend analyses. This trend reflects benefit for those with low vitamin D status but risk for those with high vitamin D status, especially since there is a trend for greater availability of high dose supplements. Public health efforts should be redoubled at maximising the provision of specified daily vitamin D supplements in at-risk groups and clinically vulnerable patients and should advise about safe vitamin D supplement use. There should be a precautionary approach to population-based blanket recommendations for vitamin D supplementation to healthy adults, as well as a caution to consumers about adverse effects of high dose vitamin D supplements on the market.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
The Clinical Audit Committee, St Vincent’s Healthcare Group, approved the extraction and audit of the data from our hospital laboratory system (reference number: 3174). Audits reviewed and approved in Ireland by an institutional clinical audit committee are neither subject to Research Ethics Committee approval nor require individual consent, as per Irish Health Research Regulations 2018.
Acknowledgments
For 25OHD data mining, we thank John Hill, Department of Pathology, St Vincent’s University Hospital. For data mining of new-to-market vitamin D supplements, we thank Paul Devlin (freelance Excel consultant). We did not receive financial support from any source.
References
Footnotes
Contributors All authors read, edited and approved the submitted manuscript. Conception and design: MJM, OCL, MATF, RKC, PJT, MTK. Laboratory analysis: PJT and MTK. Food Safety Authority of Ireland supplement analysis: OCL and MATF. Statistical analysis and data interpretation: MJM. Drafting manuscript: MJM. Critical review and revising manuscript: all authors. MJM takes responsibility for the overall content as guarantor; MJM accepts full responsibility for the finished work, had access to the data, and controlled the decision to publish.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.