Article Text

Abstract
Objective The study aims to determine discontinuation among long-acting reversible contraceptive users at 3, 6, 9 and 12 months after initiation and its associated factors among new long-acting reversible contraceptive (LARC) users.
Design A facility-based multicentre prospective cohort study was conducted with a sample size of 1766 women.
Setting The study was conducted in five large cities of Ethiopia (Addis Ababa, Gondar, Mekelle, Jimma and Harar) between March 2017 and December 2018. Various referral hospitals and health centres that are found in those cities are included in the study.
Participants The study population was all women who were new users of LARCs and initiated LARCs in our selected public health facilities during the enrolment period.
Interventions A pretested structured questionnaire was administered at enrolment and at 6 and 12 months to determine discontinuation proportion and factors associated with discontinuation.
Result From the total of 1766 women sampled for the study only 1596 (90.4%) participants completed all the questionnaires including the 12-month follow-up study. The overall proportion of discontinuation of LARCs at 12 months was 21.8% (95% CI 19.8 to 23.9). The overall discontinuation proportions at 3, 6, 9 and 12 months were 2.94%, 8.53%, 3.94% and 6.36%, respectively. Location of method initiation (adjusted HR (aHR)=5.77; (95% CI 1.16 to 28.69)) and dissatisfaction with the method (aHR=0.09; (95% CI 0.03 to 0.21)) were found to be the predictors of discontinuation among intrauterine contraceptive device users. Being satisfied with the method (aHR=0.21; (95% CI 0.15 to 0.27)), initiation after post abortion (aHR=0.48; (95% CI: 0.26, 0.89)) and joint decision with partner for method initiation (aHR=0.67; (95% CI: 0.50, 0.90)) were inversely associated with implant discontinuation.
Conclusion The majority of LARC users discontinue the method in the first 6 months after insertion and dissatisfaction with the method increased the likelihood of removal during the first year of LARC use.
- health services administration & management
- public health
- obstetrics
- gynaecology
- health & safety
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
A relatively large sample size and diverse population.
Participants were interviewed by someone not directly involved in the clients’ care.
The measures of satisfaction are not externally validated.
Lost to follow-up is high.
Introduction
Background/rationale
Unintended pregnancy (mistimed or unwanted) is a crucial public health problem which is one cause of high-risk pregnancy. In addition, it is associated with high rates of negative consequences for the mother and the newborn.1–6 Increasing the use of highly effective contraceptive methods may provide one solution to the persistent problem of health disparities of unplanned pregnancies and improve women’s and children’s health.7
Ethiopia is among the countries with a high pregnancy-related mortality ratio, which is 412 deaths per 100 000 live births.8 Although timing and spacing of pregnancy are important for the health and survival of the newborn and the mother, unintended pregnancy and short birth intervals are still among the contributing factors for the high maternal and child mortality in developing countries like Ethiopia.9 The 2016 Ethiopia Demographic and Health Survey revealed that 25% of pregnancies in Ethiopia were reported as either mistimed or unwanted.10 Moreover, improved access to and consistent use of effective contraceptive methods is fundamental to reducing the risk of unintended pregnancy and its complications.11
Long-acting reversible contraceptives (LARCs) are a type of contraceptive that is easily reversed and do not rely on the user to maintain efficacy for at least 3 years.12 Copper intrauterine contraceptive devices (IUCDs), the levonorgestrel (LNG)-releasing intrauterine system, and LNG-releasing and etonogestrel (ENG)-releasing subdermal implants are categorised as LARC methods as they do not require ongoing effort on the client’s part for long-term and effective use.2 13 14 LARCs enable women and couples to cost-effectively avert unwanted pregnancy by allowing women to space and/or limit births.15
The ability of couples to achieve their reproductive intentions partly depends on the effectiveness of, and continuity with which they practice, contraception.16 Additionally, effective contraception better enables women to achieve a broader set of reproductive goals.17 The total fertility rate would be between 28% and 64% lower if the births following discontinuation, that were not the result of a desire to become pregnant, had not occurred.16 Many factors contribute to poor maternal health outcomes and maternal mortality.18 19 Promoting family planning in high-birth-rate countries not only has the potential to reduce maternal and childhood death, poverty and hunger, but also offers the opportunity to change the default from unintentionally drifting into parenthood to planned conception.7 20 Contraceptive discontinuation may be associated with external factors or individual and partner factors.3 21–23 LARC users who are younger than 20 years, unmarried, uneducated and who experienced side effects are more likely to discontinue the method although they do not want to become pregnant.3 24 25 Although not all contraceptive discontinuation should be of concern, discontinuation while still in need, that leaves 15%–20% of women at risk of an unwanted pregnancy 3 months after discontinuation, is a concern because it contributes to increased fertility rate, unintended pregnancy and associated complications.15 26 27 Understanding contraceptive discontinuation and its determinates may help policy makers to identify better strategies to support women and improve continuous use of contraceptives when in need.
LARC use among US women was 16% during 2017–2019.28 In developed nations 14%−21.8% of LARC users discontinue the method within 12 months of initiation.23 29 In a study conducted in Colorado, an increase in LARC use from 15% to 19% among low-income teenagers and young women was accompanied by a 29% and 34% decrease in birth and abortion rates in teenagers, respectively, and a 14% and 18% drop in birth and abortion rates among young women, respectively.30 LARCs comprise only 10% or less of all contraceptive methods used in most low-income countries, of which 9% of implant users and 15% of IUCD users discontinue the method within the first year of use.15 Among the 9% implant and 2% of IUCD users in Ethiopia, the 12-month discontinuation rate was 11% and 13% for implants and IUCDs, respectively.8 31 A 1-year discontinuation rate for Implanon in Ethiopia ranged from 15.7% to 23.4%, of which 5.12% discontinued at 4–6 months and 18.3% discontinued at 7–12 months.24 25 Ethiopia is among the most populous African countries with a total fertility rate of 4.6 children per woman and an unmet need for family planning of 22%.8 In such a country, it is important to understand how long women continue using different LARC methods and what factors are associated with discontinuation so that it can help in supporting them in improving their reproductive health. There is limited knowledge on the magnitude of discontinuation and its associated factors in Ethiopia. In order to address these limitations, this facility-based multicentre prospective cohort study aims to determine LARC discontinuation and describe factors associated with discontinuation in Ethiopia.
Objective
The study aims to determine discontinuation among LARC users at 3, 6, 9 and 12 months after initiation and its associated factors among new LARC users.
Methodology
Study design
A multisite prospective cohort study design was used.
Setting
The study was conducted in five large cities in Ethiopia (Addis Ababa, Gondar, Mekelle, Jimma and Harar) between March 2017 and December 2018. Addis Ababa is the capital city of Ethiopia with a total population of 4646 759; Gondar is located in north-west Ethiopia 733 km from the capital with a total population of 500 788; Mekelle is 762 km north of the capital with a total population of 409 512; Jimma is to the south-west of Ethiopia 352 km from the capital with a total population of 207 573, and Harar is in the eastern part of the country 530 km from the capital with a total population of 215 373. Various referral hospitals and health centres that are found in the aforementioned cities are included in the study. According to the Ethiopian health sector, a health centre is a health facility that offers primary-level care in areas where health posts (which are the lowest level of care centres) are not available, accepts referrals from health posts, and sends referrals to primary hospitals, whereas referral hospitals provide clinical care to patients referred from primary and general hospitals. In all governmental and public health institutions contraception is provided for free.
Participants
The study population were all women who were new users of LARC and initiated LARC at the time of data collection.
Variables
Dependent variable
Our study defined discontinuation of LARC as: when a participant reported not using the baseline LARC method at the follow-up survey time (at 6 months and 12 months of enrolment) or reported any temporary halt of the method for 1 month or longer during the follow-up period.
Independent variables
We collected information on sociodemographic characteristics (such as age, residence, educational status and marital status), economic status (domestic animals, vehicles, house, land and monthly income) which was analysed with principal component analysis, reproductive history (including fertility plan, history of pregnancy, abortion, live birth and unintended pregnancy), knowledge and utilisation of LARCs (including who helped them in the decision to use LARC, time of method initiation, the intention of method use) and satisfaction on service provision. We also collected information on participants’ satisfaction with the LARC method they chose. Participants who scored 80% and above on questions for assessment of satisfaction with the LARC method were considered satisfied. Reliability testing shows the variables used to assess satisfaction with LARC have a high Cronbach’s α value (0.937).
Data sources/measurement
A structured questionnaire was prepared in the English language, translated to local languages (Amharic, Afan-Oromo and Tigrigna) and then translated back to English independently for reliability. The first part of the questionnaire documented sociodemographic characteristics, economic status, reproductive history, utilisation and knowledge of LARC, and satisfaction with service. The second part assessed continuation of, and satisfaction with, the LARC method. The questionnaire was pretested before being applied. Data collectors were trained and were experienced family planning service providers who were not directly involved in the counselling and provision of the contraception for that specific client. Participants were interviewed alone in an audio-visual private setting.
The first part of the pretested structured questionnaire was administered at the facility’s exit from the family planning clinic immediately after LARC was initiated. Study participants were advised to report to the health facility provider about the discontinuation of that contraception before their 6-month appointment.
At month 6 of enrolment, continuation was assessed by administering the second part of the questionnaire in face-to-face interviews for those who came to the clinics for their appointments, or via phone-call-administered interviews for those who could not visit the clinics. Study participants who did not report discontinuation were again interviewed at the 12-month point of enrolment in a similar way. Participants who self-reported discontinuation during the 1-year period, who did not use the baseline LARC method at the survey time (at 6 months and 12 months of enrolment), or reported any temporary stop of the method for 1 month or longer during the follow-up period, were counted as method discontinuers and the second part of the questionnaire was administered immediately after their report or at the survey time. Discontinuation at 3 months and 9 months was enquired during the interview at 6 months and 12 months, respectively. In a few cases it was impossible to reach the study participants via phone. Therefore, in many cases follow-up data were collected via house visits.
Sample size
The sample size was determined using a systematic random sampling method. Study sites were selected based on the geographical distribution and sociocultural diversity of the population. For the follow-up study sample size calculation we assumed the following: 95% CI, power of 80%, discontinuer to continuer ratio of 1:2, outcome among discontinuers (discontinuation proportion) of 7% and loss to follow-up rate of 10%.3 We arrived at a total of 321, multiplied by five sites and adding 10%, for a minimum sample size of 1766. The total sample size is equally distributed among the five study sites but, among the health institutions within a site, sample size distribution was according to their average caseload.
Sampling
First, the study selected five sites by considering the geographical distribution and sociocultural diversities and we included the main cities in five of the nine regions of Ethiopia. One referral hospital and three to five health centres were randomly selected from the health institutions in each study site. On average about 20 LARC users who were women visited each family planning clinic every week and sample sizes were distributed to the health institutions according to their case load. Eligible women were those aged 15–49 years who wanted LARC service in public health facilities in our selected institutions during the enrolment period. To enrol the study participants, every other woman was included through a systematic sampling procedure.
Data quality control measures
The data collectors were trained for 5 days by the investigators on the contents of the questionnaire and interviewing techniques. The first 2 days of the training were focused on the objectives of the study, the contents of the data collection tool, and the interviewing techniques. Starting from the third day, pretesting of the tool was done by the data collectors at nearby health institutions and each data collector interviewed 5–10 eligible women. The results of the pretest were not included in this analysis. In addition, the whole team met at the conclusion of the pretest with the researcher to review the data collection process and to solve problems that were encountered. The purpose of the pretest was to assess the clarity, understandability and flow of the questions.
The investigators monitored the data collection process by visiting the facilities. The questionnaires completed each working day by all data collectors were reviewed at the end of the day by the investigators for their completeness as well as consistency, and appropriate feedback was given thereafter.
Quantitative variables
The data collected were checked manually for completeness and consistency and coded by the investigator. Subsequently double data entry was made to an Epi Info V.7 database and 10% of the questionnaires were re-entered in order to compare and assess the quality of the data entry. Data entry was performed simultaneously with the data clerks. Then the data were exported to the Stata V.14 software package for data cleaning and analysis.
Statistical methods
Percentages and proportions tables were used for the overall description of the data. Mean, median and SD were computed for continuous variables. The incidence (discontinuation) estimation was made with a 95% CI. Kaplan-Meier survival analysis was used for estimating the 3-month, 6-month, 9-month and 12-month LARC discontinuation proportion. The proportion of satisfaction among LARC users’ methods (IUCDs and implants) were described. Stratification analysis was done for discontinuation and associated factors of discontinuation of IUCDs and implants as an outcome. For time to event (discontinuation) analyses, first episodes were used and subsequent follow-up data were censored. The failure event was the removal of the contraception. We examined time to discontinuation (removal of contraception) following the episode (insertion of contraception) for 12 consecutive months. Those individuals who didn’t develop the event of interest/outcome (discontinuation) until 12 months were right-censored (were not followed). A Cox proportional hazards model was used to investigate factors associated with the discontinuation of IUCDs and implants in a separate model. Independent variables (age of women, residence, education status of both husband and wife, marital status, history of stillbirth, history of live birth, history of unintended pregnancy, number of children, history of methods used and its purpose, source of decision for LARC use, time of insertion (interval) and income) with a value of p≤0.20 during the bivariate test were included in the multivariable model with an adjusted HR (aHR). The results were considered statistically significant at p≤0.05. There were 15 questionnaires that had missing variables including sociodemographic factors (age, marital status and educational status) at baseline. In addition to this end-line information on the contraceptive status of those cases was not collected, which is very relevant for the outcome of interest. For this reason, we excluded (dropped) those questions from the final analysis. Furthermore, we counted them as a non-response rate because we were not able to find the study participant to complete the missing data.
Patient and public involvement
No patient was involved.
Ethical consideration
The study participants were informed about the purpose of the research. Written consent was obtained from each study participant. For study participants under the age of 18 years, both agreement from the participants and written consent from the parents/guardian were obtained. The participants’ identities were kept private and were not disclosed beyond the necessary members of the study team.
Result
Participants
Sociodemographic characteristics: of the total 1766 LARC users enrolled in the study, 1596 (90.4%) completed the 12 months of follow-up in the five cities; the data from these participants are included in the final analysis. The mean age (±SD) of the study participants is 25.4 years (±13.5). Most of the study participants reside in urban areas and were married (91.2% and 77.2%, respectively). The sociodemographic characteristics of the study participants are presented in table 1, and table 2 shows sociodemographic characteristics and reproductive history by LARC type (IUCD and implant).
The sociodemographic characteristics of the study participants, Ethiopia, 2017/2018
Sociodemographic characteristics and reproductive history by LARC type (IUCD and implant)
Descriptive data
Reproductive history: most of the participants, 1313 (82.2%) have been pregnant previously. Among women who had a history of pregnancy 289 (23.03%) had a history of abortion and 271 (21.3%) had a history of unintended pregnancy (table 3).
Reproductive history of the study participants, Ethiopia, 2017/2018
Most (86.4%) of the study participants used implant contraception and of this number 1219 (88.4%) used ENG-releasing subdermal implants (Implanon). Around 8.3% of women using implants used LNG-releasing subdermal implants (Jadelle and Sino-implant (II)). IUCD was used by 13.6% of study participants of which only 5.3% of mothers used copper IUCD. Among them, only one LNG-containing IUCD was used for uterine bleeding treatment in addition to contraceptive use. There was only one LNG-containing IUCD used as contraception among the study participants. Nearly a third (511 or 32.5%) of the study participants used LARC previously.
A majority of participants (1172 or 73.4%) initiated the LARC method during family planning visits, without pregnancy-related events within 6 weeks before method initiation; while 221 (13.9%), 161 (10.1%) and 42 (2.6%) initiated it postabortion, postpartum and postplacental, respectively. Delaying pregnancy was the intention of initiating the method in 1343 (87.8%) participants while others initiated it for limiting fertility (completed family size).
The overall satisfaction proportion of LARC users in the study was 75% and specifically 73.7% for IUCDs and 75.2% for implants. Only 10% of very satisfied users discontinued the method. However, 53.5% of highly dissatisfied women discontinued the method by 12 months after initiation.
Outcome data
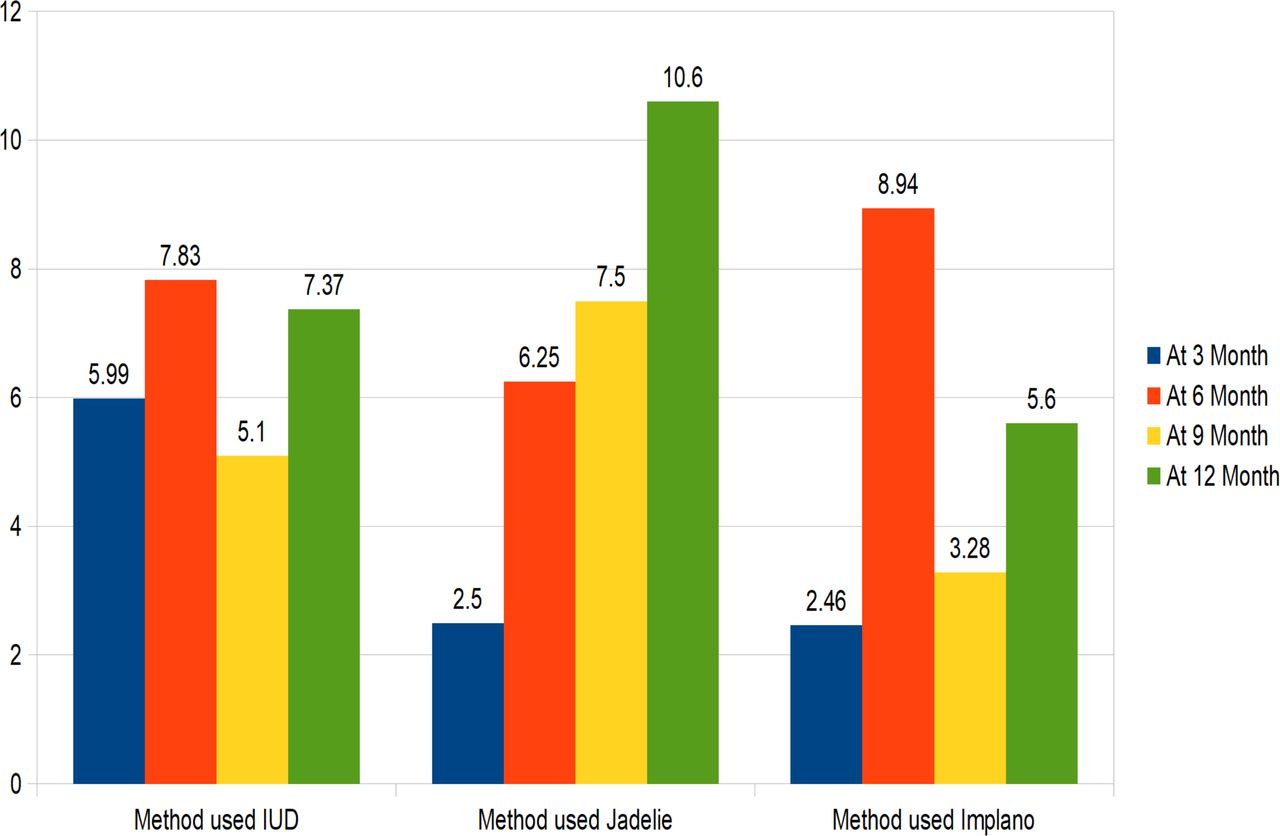
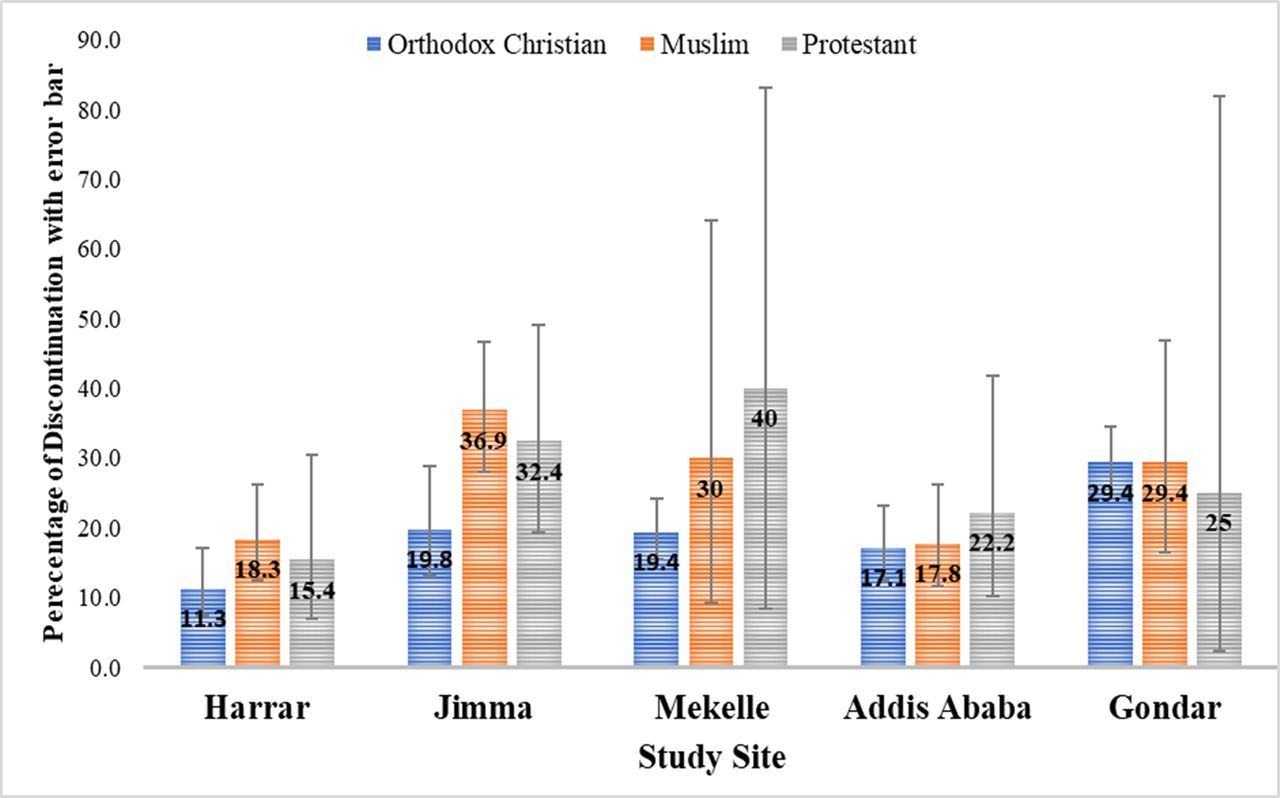
The overall discontinuation of LARC methods was 21.8% at 12 months (95% CI 19.8 to 23.9). The 12-month discontinuation proportion was 26.3% (95% CI 20.8 to 32.5) and 21.1% (95% CI 19.02 to 23.3) for IUCDs and implants, respectively. The LARC discontinuation at 3, 6, 9 and 12 months was 2.9%, 8.5%, 3.9% and 6.4%, respectively (figure 1). The maximum proportion of discontinuation was reported at 6 months after initiation of LARCs (8.53%). Regarding the type of method, more IUCD users discontinued in the first 6 months than implant users (13.8% vs 11.1%) (figure 2). Proportion of method discontinuation did not vary statistically by religion. Discontinuation among Muslims, Protestants and Orthodox Christians was 24.6% (95% CI 20.5 to 29.2), 24.1% (95% CI 17.1 to 32.9) and 20.8% (95% CI 18.5 to 23.3), respectively (figures 3 and 4).
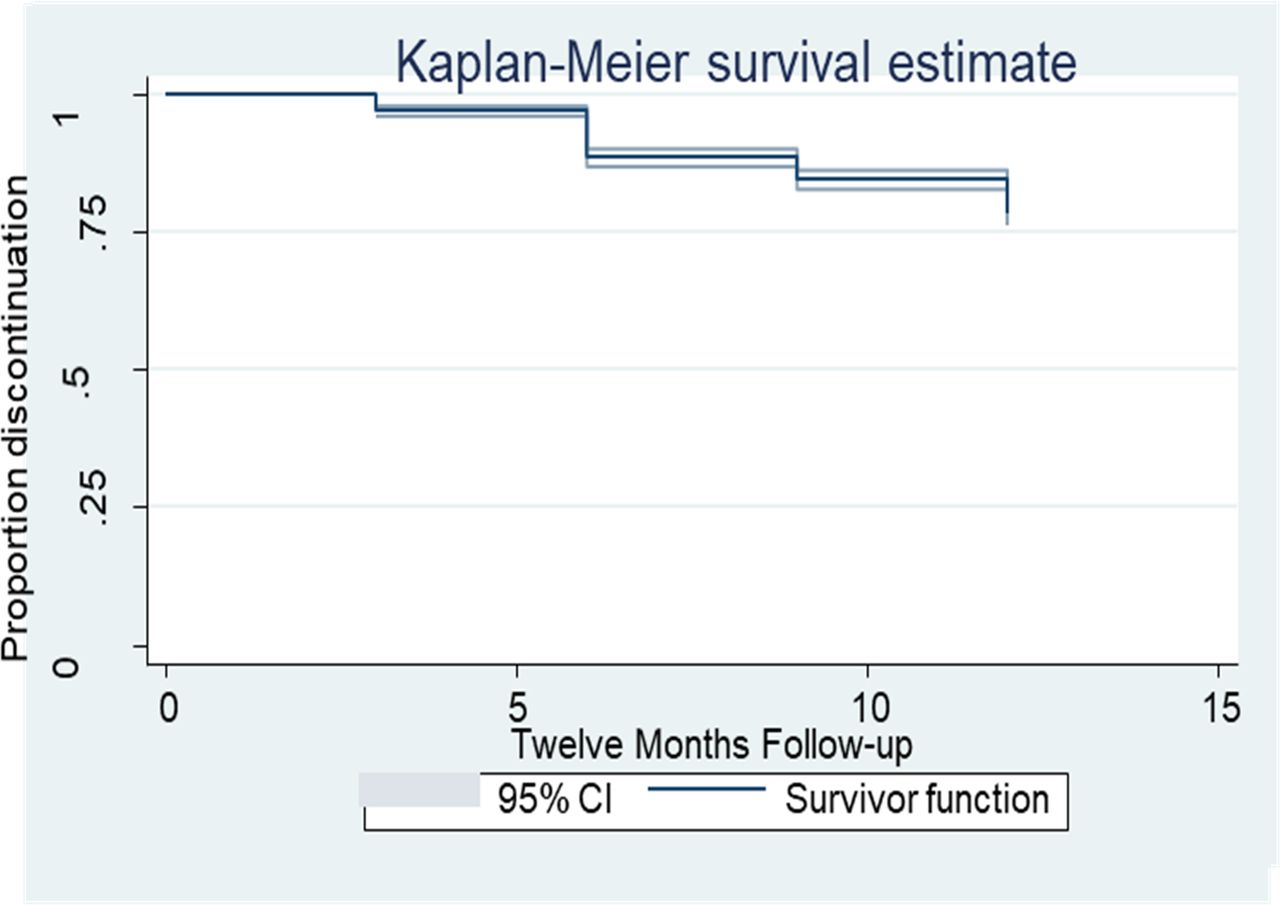
Discontinuation (%) of long-acting reversible contraceptives (LARCs) during follow-up period, Ethiopia, 2017/2018.

Discontinuation (%) among intrauterine contraceptive devices (IUCD) and implant user by months, Ethiopia, 2017/2018.

Discontinuation (%) by religion and study site, Ethiopia, 2017/2018.

Discontinuation rate by type of long-acting reversible contraceptive (LARC) method during the follow-up period, Ethiopia, 2017/2018.
Main results
Factors associated with IUCD discontinuation
The location of contraceptive initiation and dissatisfaction with the method was found to be significantly associated with discontinuation of IUCD use.
Being dissatisfied with the method was significantly associated with the discontinuation of IUCD use. Satisfied women were 91% less likely to discontinue IUCD than dissatisfied users (aHR=0.09; 95% CI 0.03 to 0.21).
Location of method initiation was another predictor of contraceptive discontinuation. IUCD users who initiated the method in Gondar were more than five times more likely to discontinue the method than users who initiated it in Harar (aHR=5.77; 95% CI 1.16 to 28.69) (table 4).
Factors associated with IUCD and implant discontinuation, Ethiopia, 2017/2018
Factors associated with implant discontinuation
Dissatisfaction with the method, time of implant insertion and method initiation without partner involvement in the decision were significantly associated with the removal of the implant.
It was found that joint decisions by the husband and wife on method initiation affected the discontinuation of implant use. Those who decided jointly were 33% less likely to discontinue implants than women who decided without involving their partner (aHR=0.67; (95% CI 0.50 to 0.90)).
Women who initiated implants postabortion were 52% less likely to discontinue than women who initiated them postpartum or during an interval period (aHR=0.48; 95% CI 0.26 to 0.89).
Being dissatisfied with the method was significantly associated with discontinuation of the implant. Satisfied women were 79% less likely to discontinue implant contraception than dissatisfied implant users (aHR=0.21; 95% CI 0.15 to 0.27) (table 4).
Discussion
Key results
In this multisite prospective cohort study, we aimed to determine the discontinuation over a 1-year time frame and its predictors among LARC users. The overall proportion of discontinuation of LARC methods was 21.8% at 12 months. Method satisfaction was the most important predictor of discontinuation during the 12-month period. In the first 6 months, more IUCD users than implant users discontinued use, although this difference was not statistically significant. During the 1-year follow-up, discontinuation increased over time following insertion, Jadelle users were more likely to discontinue the method compared with the other methods (figure 5). Male partner involvement in decisions for contraceptive use increased LARC continuation.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Discontinuation rate by type of method, Ethiopia, 2017/18.
The 6-month discontinuation proportion of all LARC, IUCDs and implants, which was 11.5%, 13.8% and 11.1% in the current study, respectively, was higher than previous reports which were in the range of 7%–8.2%, 8%–11% and 6.9%–7.5%, for all LARC, IUCDs and implants, respectively.3 23 32 Previous studies also reported lower discontinuation rates at 12 months—14% for all LARC, 16%–22.3% for IUCDs and 17% for implants—than the current study, which found a discontinuation proportion of 21.8% for all LARCs, 26.3% for IUCDs, and 21.1% for implants.23 29 In previous studies, the free provision of LARCs for research purposes only, which is not true otherwise in those settings, may have contributed to the lower discontinuation of these methods in those studies. All those studies were done in different study settings with different population characteristics. Most (61%) of the study participants in the research done by Grunloh et al used the LNG intrauterine system which can improve the continuation of its additional non-contraceptive benefits.3 The high satisfaction (84%) with the contraceptive methods is associated with the continuation of the contraceptives.29
At 12 months the proportion of discontinuation of all LARCs in the current study was similar to the finding by Cohen et al (discontinuation of all LARC=21.8% in both studies, implants=21.1% vs 21.3%, respectively).23 A similar trend of more IUCD discontinuation than implant discontinuation is found in the current study. Despite the difference in the study setting and study participants, adolescents and young women were the study population. The similar results may be attributed to the similarity in study design.
The 12-month proportion for discontinuation of implants in the current study is slightly lower than the 23.4% reported by Nageso and Gebretsadik.24 This cross-sectional study was done in a similar setting. But this study was done with a larger sample size and in a wider geographical area including more variable types of study participants. According to the EDHS 2016, the discontinuation rate for IUCDs and implants is 13% and 11%, respectively.8 Although that result may be more generalisable due to the more representative sample size, the retrospective nature of data collection and lack of follow-up makes it prone to bias as compared with the method used in this study.
Satisfaction with LARC at 12 months with 75% satisfaction in the current study was lower than the finding by Peipert et al which was 84% for all LARC users, over 80% for IUCD users and 79% for implant users.29 Satisfaction in the current study was nearly similar to a 72.7% satisfaction that was reported according to a study that evaluated satisfaction with LARC, frequency, and reasons behind early removal with a sample size of only 132, but where the proportion of IUCD users and implant users was 58.3% and 41.7%, respectively.11 In the former study a higher proportion of LNG intrauterine system users may have contributed to the higher satisfaction rate. The low satisfaction rate in our study may also result from inadequate information and or understanding during counselling at the method initiation. Women satisfied with the method are least likely to discontinue LARC in the current study. Similarly, women reporting satisfaction with LARC were less likely to have LARC removed early according to Dickerson et al and Peipert et al.11 29 However, age, number of children, history of previous abortion, educational level and marital status were not determinants for discontinuation in our finding, in contrast to previous reports.23 25 33–35
Decision to use LARC in consultation with partner or significant other (in regards to choice of method) decreases discontinuation of implants as women may discontinue it for fear of marital disharmony with a partner who disagreed. This result is consistent with a previous report that women who believe that their male partners support contraception are twice as likely to use contraception effectively.36 Male partner support improves the use and compliance of women for modern contraceptives.37 38 Discontinuation of implants is low when the method is initiated postabortion, which may be either due to fear of a similar experience or to healthcare providers’ influence, especially in the case of induced abortion. The difference in proportion of discontinuation of IUCD at different cities may be explained by sociocultural differences as well as different rumours and myths among the people.
Orthodox Christians are more likely to discontinue LARCs than Protestants and Muslims, according to the study’s findings. In one study in Ethiopia, Muslims were 65% less likely to use modern contraceptives as compared with Orthodox Christians.39 Also, Protestant women are less likely to use LARCs compared with Catholics.40 Though religious acceptability of family planning methods is important, religious tradition may have a wide range of interpretations regarding family planning.41 Evidence shows that the meaning and relevance of Muslim scriptures to fertility have been variably interpreted.41
Most of the participants (82.2%) in the current study had been pregnant at some point in time but the proportion of prior unintended pregnancy (19%) and abortion (21.9%) was low as compared with a prospective cohort study in St. Louis, USA, which involved 4167 participants and found 66% of unintended pregnancies.29 Similarly, an unintended pregnancy rate of 67% was reported in a prospective cohort study which measured characteristics associated with 6-month discontinuation of LARC among 5928 participants.3 The abortion history in the current study is comparable to a 22.5% rate reported from a facility-based cross-sectional study of 449 participants in Debre Tabor, Ethiopia.35 A low abortion rate of 4.7% was also reported in a community-based cross-sectional study of 683 participants in Dale district, Ethiopia.24 The lower rates in all these Ethiopian studies may be because, once pregnancy happens, most women may accept that and may not consider it as unintentional. Their previous pregnancy experience was asked and they may not remember and sometimes may not be happy to share their failed pregnancy experience.
Among the strengths of the study the prospective follow-up method in which participants were enrolled and checked after they initiated the method of choice was a strong point. The frequency of follow-ups were reasonably short to avoid recall bias and at the same time reasonably long to decrease influence on continuity of the contraception. The relatively larger sample size and diversified participants will enhance the generalisability of the results. Study participants were interviewed by someone not directly involved in the clients’ care, which may give this study’s participants relative freedom to respond.
Limitations
One of the limitations of the study is the proportion of participants lost to follow-up, which is high as compared with other follow-up studies (9.6% vs 3.7% and 3%3 29); this will lead to bias. Repeated trials were made to access participants with two telephone numbers which were recorded at enrolment, but either the telephone was not functional or was not located in network-accessible areas. Some participants changed their residence and data collectors could not access them during scheduled home visits. Sensitivity analysis, which could have checked whether the dropouts have similar characteristics to the discontinuers, was not done for the LARC users who dropped out. We assume the dropouts are random and do not represent a refusal to continue participation and as a result, the study did not expect a significant impact on the outcomes of interest. The measures of satisfaction were not externally validated. Other limitations include that self-reported discontinuation may lead to bias and the smaller proportion of IUCD users may lower the generalisability of the results. Our data collection with the interview, instead of a self-administered questionnaire, may have resulted in inaccurate responses from the study participants on sensitive issues.
Conclusion
The majority of LARC users discontinued the method in the first 6 months after insertion and dissatisfaction with the method increased the likelihood of removal during the first year of LARC use. Method dissatisfaction may be related to a lack of knowledge about LARCs (benefits, use, potential side effects, etc); policy makers and other stakeholders should support the use of shared decision making in contraceptive counselling and widespread community education about LARC methods. Community education to increase husbands’ knowledge of LARC and encourage involvement in contraceptive decision making could be valuable in supporting a women’s reproductive goals. We encourage stakeholders to make all contraceptive options, including LARC, available at abortion care provision institutions to those who want to initiate contraception. This will improve maternal health and subsequently the community health at large. Other studies with larger numbers of IUCD users and studies which assess the risk of unintended pregnancy after LARC discontinuation are also recommended.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the Ethical Committee of the University of Gondar Institutional Review Board, Ethiopia (Reference Id: O/V/P/RCS/05/90/2016).
Acknowledgments
The authors thank CIHRT at the University of Michigan for fully funding this research and for the continuous support from the beginning to the end of this research. The authors also thank Pre-Publication Support Service (PREPSS) for supporting the development of this manuscript by providing prepublication peer review and copy editing. The authors also thank Dr Mulat Adefris (MD, OBGYN, MPH), the study participants and data collectors.
References
Footnotes
Twitter @ateklu72
Contributors GSM, SMA designed the study and performed the analysis and interpretation of data; GSM, SMA, YA, LG, TG, BAA, DA, DT, GAF, FAA, AY, ADG, AMT, MHD, BG drafted and finalised the write-up of the paper. All authors prepared the draft manuscript, and read and approved the final manuscript.
Funding CIHRT and the University of Gondar funded data collection. There are no funders for publication. The funder(s) had no role in the design, data collection, analysis and writing of this manuscript.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.