Article Text

Abstract
Objective The clustering of multiple cardiovascular disease (CVD) risk factors (CRFs) increases the risk of CVD prevalence and mortality. Little is known about CRF clustering among community-dwelling older people in Xinjiang. The objective of this study was to explore the prevalence of CRF clustering in this population.
Design Cross-sectional study.
Setting Xinjiang, China.
Participants Multilevel random sampling was used to survey individuals aged ≥60 in six regions of Xinjiang. In total, 87 000 participants volunteered, with a response rate of 96.67%; 702 participants with incomplete data were excluded and data from 86 298 participants were analysed.
Outcome measures The prevalence of smoking, hypertension, diabetes, dyslipidaemia and overweight/obesity was 9.4%, 52.1%, 16.8%, 28.6% and 62.7%, respectively. The prevalence of CRF clusters among people of different ages, regions and ethnic groups differed significantly. The 85.7% of the participants presented at least one CRFs and 55.9% of the participants presented clustering of CRFs. The proportion of CRF clusters tended to be higher in men, 60–69-year-old group, northern Xinjiang and the Kazakh population. After adjusting for age and sex, logistic regression analysis revealed that men, 60–69-year-old group, northern Xinjiang and the Kazakh population were more likely to have clustering of CRFs, compared with their counterparts.
Conclusions The prevalence of CRFs in the older Xinjiang population is high and their clustering differs by sex, age, region and ethnicity. CRF prevention and management should be active in this population, and strategies to reduce CVD risk based on sex, age, ethnic group and region are warranted.
- cardiology
- epidemiology
- geriatric medicine
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. The original contributions presented in the study are included in the article, further inquiries can be directed to the corresponding author/s.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
The study is the first epidemiological investigation of cardiovascular disease risk factor (CRF) clustering in the older population of Xinjiang.
Strengths included the use of multilevel random sampling, representative samples, a large sample size, strict presurvey staff training and standard protocols and instruments to ensure the reliability of the data.
Cross-sectional studies cannot quantify the importance, nor can they determine the causality and temporality, of the relationship between CRF clustering and the morbidity of cardiovascular disease.
The study did not conduct an oral glucose tolerance test, which may underestimate the morbidity of diabetes.
Introduction
Cardiovascular disease (CVD) remains the primary burden of global population health due to its high morbidity and mortality rate. Studies suggest that the prevalence of CVD is increasing in developing countries compared with developed countries, more than 80% of CVD deaths occur in low-income and middle-income countries.1–3 The Report on Cardiovascular Health and Diseases Burden in China: an Updated Summary of 2020 showed that due to widespread CVD risk factors (CRFs) exposure, the prevalence of CVD in China is continuously on the rise, with an estimated 330 million patients with CVD in 2020. A rapid ageing process will further increase the prevalence and mortality rate of CVD in China.4 The CVD mortality rate ranks first among urban and rural residents, and the total cost of hospitalisation due to CVD increases annually, further highlighting the urgency of CVD prevention and control.
CVDs are caused by quite a few factors. Some of them are invariable (gender, age, genetic heritage), others are variable (cigarette smoking, dyslipidaemia, diabetes, elevated blood pressure, obesity, physical inactivity, excessive alcohol consumption, low intake of fruits and vegetables, psychosocial stress).5 Variable risk factors can be influenced by changing bad habits. Framingham Heart Study has reported that CRFs are closely related to the incidence and prevalence of CVD. For example, each increment of 20 mm Hg in systolic blood pressure (SBP) or 10 mm Hg in diastolic blood pressure (DBP) doubles the risk of CVD at 40–70 years of age. Diabetes is associated with a 2- to 3-fold increase in the likelihood of developing CVD. A 10% drop in serum cholesterol reduces the risk of coronary heart disease by 50% at age 40.6 In most people, CVD is the product of several risk factors. Clustering of multiple CRFs has been found to increase the risk of CVD occurrence and death.7–10 Individuals with more than one CRF have a greater risk of CVD than those with a single CRF.9 10 Additionally, studies have found that the prevalence of clustered CRFs in different countries, populations, regions and ethnic groups is not uniform.11–13 These variations may be related to differences in national income, urbanization, industrialization, environmental exposures, socio-economic status, diets, cultural habits, and lifestyle behaviors.14 Therefore, understanding these differences may assist with CVD prevention and control through the targeting of CRFs unique to different regions and ethnic groups.
Xinjiang is located in northwestern China, Eurasia hinterland. Since ancient times, Xinjiang has been a multiethnic, multicultural and multireligious place. Xinjiang spans a large latitude and longitude and has large differences in altitude, temperature (in southern and northern Xinjiang) and residents’ genetic background, cultural customs and eating habits. Uyghur, Han, Kazakh and Hui people accounted for 97.32% of the total population at this time.15 Population of Xinjiang aged ≥65 years in 2015 accounted for 7.21% of the total population, the growth rate of which is much faster than that of Xinjiang’s total population, highlighting this ageing population.16 At present, there have been no large-scale surveys or analyses of the prevalence and clustering of CRFs in the older population of Xinjiang.
It is also well known that findings from the younger population may not be applicable to the older. Therefore, our research aims to provide the latest prevalence of CRFs and their clusters in the older population of Xinjiang. By understanding the differences in CRFs and their clusters among different sexes, ages, regions and ethnic groups, we can formulate specific intervention measures against CRFs to prevent, manage and reduce the mortality of CVD and the economic burden of medical insurance.
Materials and methods
Study population
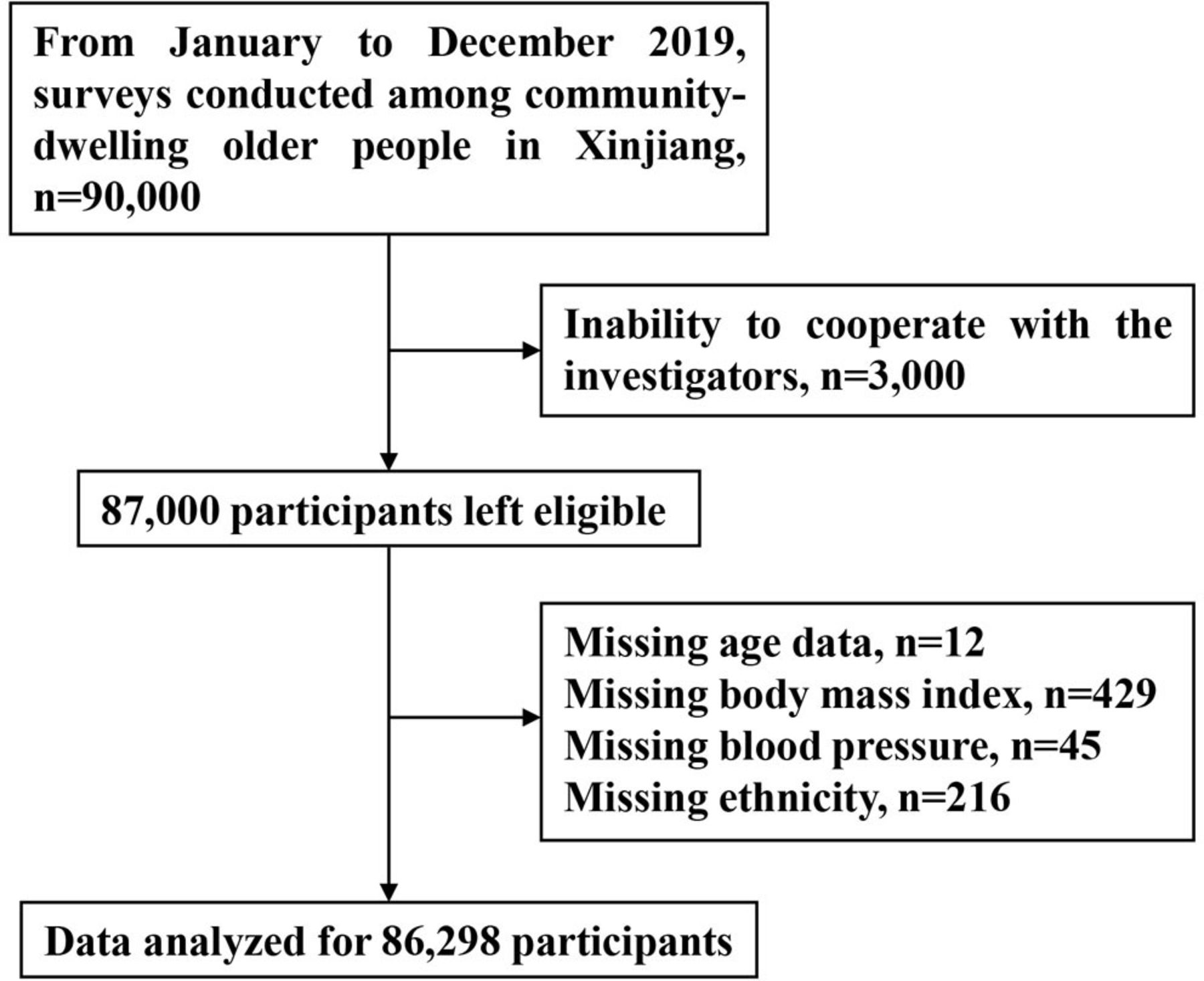
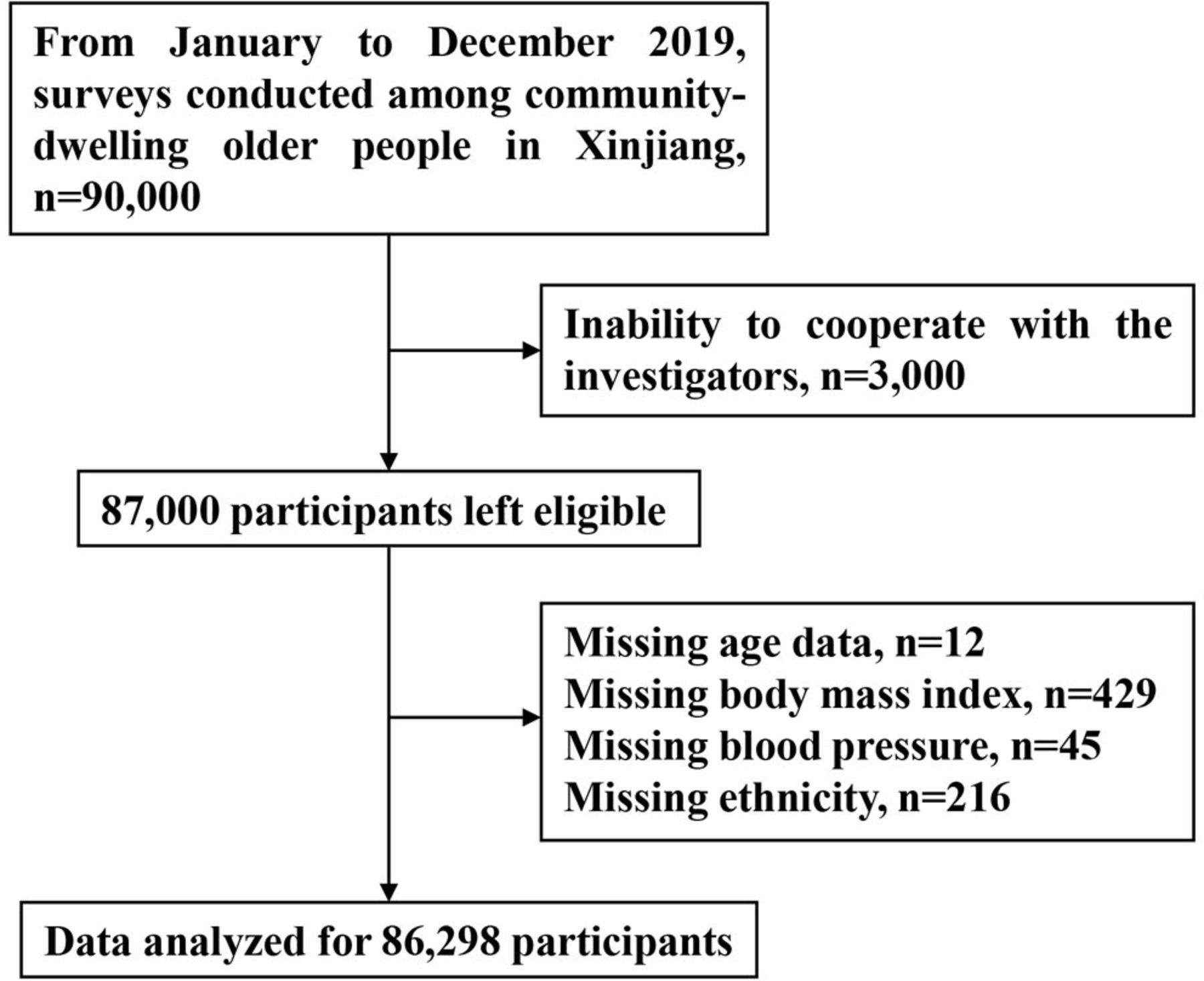
This study was a cross-sectional epidemiological survey of the older population of Xinjiang. According to natural settings and climate patterns, Xinjiang is divided into three distinct subregions (north, south and east). A multistage random sampling method was used between January and December 2019 to administer surveys in this population. In the first stage, two prefectures were randomly selected from southern, northern and eastern Xinjiang (Altai and Tacheng in northern Xinjiang, Kashgar and Hotan in southern Xinjiang and Hami and Turpan in East Xinjiang). In the second stage, one city was randomly selected from each prefecture. In the third stage, two counties were randomly selected from each city. In the fourth stage, 7500 people aged ≥60 were randomly selected from each county. From this pool, a total of 90 000 participants were randomly selected. All participants met the inclusion criteria of this survey: participants were aged ≥60 with independent consciousness, who were able to understand and cooperate with investigations and sign an informed consent form. Ultimately, 87 000 participants accepted the survey, with a response rate of 96.67%; 702 participants with incomplete data were excluded and data from 86 298 people were analysed (figure 1).
{kind=link}
Selection procedure of the study participants.
Research methods
Questionnaire
A set of standardised questionnaires was completed under physician guidance. The questionnaire collected information such as age, sex, ethnic group, education, occupation, disease history, medication history, family history, drinking history, smoking history, eating habits and other details.
Physical examination
A detailed physical examination was carried out on each subject by a physician and blood pressure, weight and height were measured by qualified professionals according to standard methods.
Blood pressure measurement: SBP and DBP were measured according to the method recommended by the American Heart Federation. All participants were prohibited from smoking and drinking alcohol, tea, coffee and other such caffeinated drinks 30 min before. Participants were seated and the blood pressure of their right upper arm was measured after a 10 min rest. A specialist doctor used a desktop mercury sphygmomanometer to measure blood pressure every 2 min for three consecutive measurements, with room temperature kept above 18°C.
Weight measurement: the participants were required to have an empty stomach, take off their shoes and wear only light clothes. A calibrated medical scale was used for weighing. The participants were relaxed and stood upright in the middle of the scale’s chassis, with the reading being accurate to 0.1 kg.
Height measurement: a measuring ruler with a minimum scale of 1 mm was fixed vertically to the ground. The participants stood upright with both heels together and their body, hips and shoulders close to the ruler. The examiner put a square ruler on the top of the participants’ head, with one side of the right angle being near to the measuring ruler and the other side to the participants’ scalp. The reading on the measuring ruler was accurate to 1 mm.
Calculation of body mass index (BMI)=weight (kg)/height (m).2
Collection of blood samples and laboratory testing
Disposable blood collection equipment was used to draw 10 mL of fasting peripheral venous blood from all participants in the morning (participants’ stomachs should have been empty for a minimum of 10 hours). Plasma (serum) was centrifugally separated from blood cells immediately and both components were stored at −80℃. Fasting blood glucose (FBG), total cholesterol (TC), triglycerides (TG), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), serum creatinine, serum urea nitrogen and other biochemical indicators were examined within 1 month, using a Hitachi 7600 automatic biochemical analyser at the clinical Laboratory Center of People’s Hospital of Xinjiang Uyghur Autonomous Region (a Third-Grade Class A hospital).
Assessment criteria
Hypertension: SBP ≥140 mm Hg and/or DBP ≥90 mm Hg or a previous diagnosis of hypertension with the use of antihypertensive medication.
Diabetes: fasting plasma glucose (FPG) concentration ≥7.0 mmol/L or a previous diagnosis of diabetes with use of hypoglycaemic agents.
Overweight/obesity: according to criteria listed in the Guidelines for Prevention and Control of Overweight and Obesity in Chinese Adults, a BMI of 18.5–24 kg/m2 was considered as normal weight, 24.0–28.0 kg/m2 as overweight and ≥28.0 kg/m2 as obese.
Dyslipidaemia: according to criteria from the Guidelines for Prevention and Control of Dyslipidemia in Chinese Adults (2016 Revised Edition), dyslipidaemia was defined as the presence of at least one of the following: TC ≥6.2 mmol/L, TG ≥2.3 mmol/L, HDL-C <1.0 mmol/L and LDL-C ≥4.1 mmol/L.
Smoking: according to WHO standards, participants were defined as smokers if they smoked continuously or smoked for a cumulative period of at least 6 months.
The clustering of CRFs: smoking, hypertension, diabetes, dyslipidaemia and overweight/obesity were the CRFs included in this study. Clustering referred to the same individual exposed to at least two of the above CRFs.
Quality control
Standard methods and unified, standardised instruments (checked and corrected by professionals) were used to collect the relevant data. In order to control observer error to the greatest extent, investigators were rigorously trained and assessed to administer the questionnaire (the questionnaire administrator was a specialist doctor) and to perform physical examination, blood sample collection, transportation, separation, preservation, marking, recording, questionnaire review, data entry, etc. Only trained and qualified individuals could administer the survey. Double blind data entry was used in which two professionals entered data in parallel and performed statistical analysis after verification.
Statistical analysis
Data analyses were performed using SPSS for Windows (V.19.0; SPSS, Chicago, Illinois). Values were expressed as the mean±SD. Count data were shown as the number of total cases (n) or percentages (%). Comparisons of clinical phenotypic measurement data between two groups were performed using a Student’s t test, and categorical data were analysed using a χ2 test. Logistic regression analysis was used to analyse the influence of differences in sex, age, region and ethnicity on the clustering of CRFs after adjusting for age and sex. p<0.05 indicated that the difference was statistically significant.
Results
Demographic and physiological characteristics of participants
As shown in table 1, a total of 86 298 participants aged ≥60 years were involved in this study, including 41 087 (47.6%) men and 45 211 (52.4%) women. Moreover, 33.5%, 6.1%, 57.3% and 3.1% of participants were of Han, Kazakh, Uyghur and Hui ethnicities, respectively. The DBP value of men was higher than that of women (p<0.05); smoking rate in men was also significantly higher than in women (p<0.001). The BMI, SBP, TC, TG, LDL-C, HDL-C and FPG values of women were all higher than those of men (p<0.001). The prevalence of smoking, hypertension, diabetes, dyslipidaemia and overweight/obesity among the older population of Xinjiang was 9.4%, 52.1%, 16.8%, 28.6% and 62.7%. Men were more likely than women to have a bad health-related behaviour of smoking. The prevalence of hypertension, diabetes, dyslipidaemia and overweight/obesity were higher in women than in men (p<0.001).
Demographic and physiological characteristics of participants in Xinjiang, China
The prevalence of CRFs among different ages, regions and ethnic groups in the older population of Xinjiang, China
Participants were divided into five groups by age (60–69 years old, 70–79 years old, 80–89 years old, 90–99 years old, ≥100 years old). Differences in the prevalence of smoking, hypertension, diabetes, dyslipidaemia and overweight/obesity across age groups were statistically significant (p<0.05). Prevalence rates of smoking, dyslipidaemia and overweight/obesity were highest in the 60–69-year-old group; diabetes prevalence was highest in the 70–79-year-old group; and hypertension was highest in the 80–89-year-old group, thereafter showing a downward trend with age (table 2).
The prevalence of cardiovascular disease risk factors (CRFs) among community-dwelling older people in Xinjiang
There were statistically significant differences in the prevalence of all five CRFs between northern, eastern and southern Xinjiang (p<0.05). The prevalence of smoking, hypertension, diabetes and overweight/obesity was highest in northern Xinjiang, followed by eastern and southern Xinjiang. The prevalence of dyslipidaemia was highest in southern Xinjiang, followed by northern and eastern Xinjiang (table 2).
Statistically significant differences in the prevalence of the five CRFs were also found between ethnic groups (p<0.05). Kazakh individuals had the highest prevalence of hypertension and overweight/obesity, followed by Hui and Han; Uyghurs had the lowest. However, nearly half or more than half of all participants suffered from hypertension and overweight/obesity. The prevalence of smoking and dyslipidaemia in Han individuals were higher than in other ethnic groups. The prevalence of diabetes was the highest in Hui individuals (table 2).
Heat maps of CRF clustering among the older population of Xinjiang, China
In Xinjiang, only 14.3% of the older population did not have any CRFs. People with 1, 2 or ≥3 CRFs accounted for 29.8%, 33.3% and 22.6% of those sampled, while those with ≥1, ≥2, ≥3 or ≥4 CRFs accounted for 85.7%, 55.9% and 22.6%, respectively (table 3).
Heat maps of CRF clustering among the older population of Xinjiang, China
Differences in the prevalence of CRFs clustering differed by sex, age, region and ethnic group (p<0.05). Men had more CRF clusters than women. Furthermore, CRF clustering decreased gradually with age. People in northern Xinjiang with ≥1, ≥2 or ≥3 clustered CRFs had the highest morbidity. Moreover, 90.1% of people were exposed in to at least one CRF. After eastern Xinjiang, people in southern Xinjiang had the lowest morbidity. By ethnic group: Kazakhs with ≥1 or ≥2 clustered CRFs had the highest morbidity; Hui with ≥3 clustered CRFs had the highest morbidity; and Uyghurs with ≥1, ≥2 or ≥3 clustered CRFs had the lowest morbidity (table 3).
Logistic regression analysis of ≥1, ≥2 and ≥3 clustered CRFs among different sexes, ages, regions and ethnic groups in the older population of Xinjiang
After adjusting for age and sex, the logistic regression analysis revealed that the risk of illness (OR (95% CI) in women with ≥1, ≥2 and ≥3 clustered CRFs was 1.087 (1.045 to 1.131), 1.002 (0.974 to 1.030)and 0.893 (0.864 to 0.923) times that of a man, respectively. Compared with people aged 60–69 years old, the ORs of CRFs clustering decreased gradually with age. Northern Xinjiang, and the Kazakh population were more likely to have clustering of CRFs (table 4).
Adjusted ORs (95% CIs) of having ≥1,≥2,≥3 versus none CRFs associated with different groups
Discussion
In this study, we investigated the epidemic characteristics of CRFs clustering among a large representative sample in the older Xinjiang population. The results show that the prevalence of CRFs was very high, and over 85% of participants had one CRF at least. Half of the older adults had two or more CRFs. After adjusting the confounding factors, the clustering of CRFs differs by sex, age, region and ethnicity.
This study found a high morbidity of clustered CRFs in Xinjiang; only 14.3% of the older population was not affected by any CRFs. The most common CRFs in our study were overweight/obesity (62.7%) and hypertension (52.1%). The prevalence of overweight/obesity, hypertension and diabetes (16.8%) was higher than the national level (28.2%, 26.1%, 5.2%, data collected in 2005 by InterAsia),11 while the morbidities of smoking (9.4%) and dyslipidaemia (28.6%) were lower (34.4%, 53.6%,); these findings are consistent with that of previous research.17 18 Additionally, the morbidity of the participants with ≥2 and ≥3 clustered CRFs (55.9%, 22.6%) was higher than the national level (45.9%, 17.2%),19 and that of northeastern China (32.7%, 10.0%),20 suburban areas of Beijing (47.2%, 17.5%),21 Qamdo (47.1%, 20.9%),22 Nanjing (35.2%, none),23 Malaysia (33.0%, 14.0%)24 and southwest Nigeria (47.0%, 23.9%).25 In contrast, the morbidity of the participants with ≥2 and ≥3 clustered CRFs was lower than that reported in the USA (73.0%, 35.9%), India (78.6%, none),26 Nepal (86.0%, 63.4%),27 rural areas of Yunnan (66.2%, 34.8%).28 Potential reasons for these differences may include differences in social economy, environmental exposures, cultural customs and diets. Moreover, the differences across different studies could be attributed to differences in participants’ age range, the sample size, definitions and diagnostic criteria used in those studies. Our study shows that the older population in Xinjiang is more likely to have clustered CRFs; thus, active public health measures should be taken to prevent and control these factors.
In this study, the prevalence of smoking was significantly higher in men (18.9%) than in women (0.4%). Conversely, the prevalence of the other four CRFs in men was lower than in women. This study also found that women had a higher risk than men of having at least one clustered CRF, while men had a higher risk than women of having ≥3 clustered CRFs. This is in line with the study results of Zhao et al29 and Wang,30 who found that CRF clustering occurs easily in men. A study showed that the morbidity of CVD in women was further increased in participants aged 51 years (the average menopausal age of Asian women) or older. Like in whites, the onset of menopause may further increase the risk of CVD.31 Compared with premenopausal women, postmenopausal women have higher levels of CRF indicators (hypertension, diabetes, dyslipidaemia) related to metabolism. Considering the decline of hormone levels in postmenopausal women, the protective effect is reduced for metabolic CRFs. Meanwhile, lifestyle and eating habits are hard to change in a short time.32 Furthermore, we conjectured that smoking may be somehow increased the tendency of CRFs clustering in men, as smoking was more common among men than women.
The study also found that the highest CRF exposure was in those aged 60–69 years old, and that both CRF clustering and age-adjusted and sex-adjusted CRF clustering gradually decreased with age. Numerous studies have shown that correlations between several traditional CRFs and cardiovascular events are reduced in the older adult.33 For individuals whose lifestyle risk factors remain the same throughout life, their lifetime risk of CVD is lower at 70 years old than at 50 years old.34 Similarly, a strong relationship has been found between hypertension and the hazard of death in the older at younger ages, while a weak relationship has been found at very older ages.35 The risk of hypertension does not continue to increase with age.36 This may be because people with a high risk of CVD are more likely to have early lifetime events, and multiple clustered CRFs and competition between diseases lead to a greater risk of death. Another possible reason may be that more older survivors with one CRF are less likely to have been adversely affected by other CRFs. People with longer lifespans may either have a genetic composition resistant to CVD or have a lower burden of CRFs, which in turn reduce their risk of CVD.37 38 Moreover, the physiological changes that occur during ageing may change the effects of some CRFs. One study found that a minimum cholesterol level is necessary to maintain neuronal function39; a very older individual with a heavy weight in the overweight range may reflect lower weakness and less loss of physiological reserve40; the optimal BMI for an older individual is considered higher than that of one who is middle aged.41 In this study, it was found that the morbidity of cardiovascular CRFs was relatively low among individuals aged 100 years old and above, which is consistent with the results of Zyczkowska et al.42 In this study, participants ≥100 years did not smoke and had a healthier lifestyle with a low morbidity (33.3%, 6.3%, 27.0%, 46%) of hypertension, diabetes, dyslipidaemia and overweight/obesity. This explains to some extent why fewer than three CRFs were clustered in this age group.
Consistent with our results, one systematic review of 16 studies published in 2007 and another of 101 Canadian studies published in 2015 certified that there are striking differences in the morbidity of clustered CRFs across ethnic groups.43 44 After adjustment for age and sex, the ORs for the prevalence of ≥1 and ≥2 clustered CRFs were higher in the Kazakh population than in the Han; ORs in the Uyghur population was lower than in the Han. The differences may be due to the striking differences between ethnic groups about the prevalence of smoking, hypertension, diabetes, dyslipidaemia and overweight/obesity. The morbidity of overweight/obesity and hypertension in Kazakhs (75.0%, 66.3%) was higher than other ethnic groups. The morbidity of smoking and dyslipidaemia in the Han population (11.5%, 30.2%) was also higher than other ethnic groups. The prevalence of diabetes in the Hui population (22.9%) was higher than in other ethnic groups. The mechanisms underlying these phenomenons may be associated with environment of inhabited area, residents’ genetic background, cultural customs and eating habits. The striking differences between ethnic groups about the prevalence of CRFs suggest that it is necessary to develop the ethnic-specific CVD prevention programmes and health services.
This study also showed that among the clustered CRFs, the morbidity of smoking, hypertension, diabetes and overweight/obesity was higher in northern Xinjiang than in eastern and southern Xinjiang. Hypertension, diabetes, obesity and dyslipidaemia are multifactor diseases affected by genetics and the environment. In northern Xinjiang, the temperature is relatively low with an average annual temperature of −4°C to 9°C. It is dominated by animal husbandry and 96.4% of the Kazakh in China live here.45 The Kazakh population mainly follows a nomadic lifestyle. Men often drink hard liquor and eat a simple diet of meat and salt to resist the cold, with fewer fruits and vegetables.46 In contrast, southern Xinjiang is a typical comprehensive zone integrating three systems: oasis, mountain and desert. Belonging to an arid and warm temperate climate, it has low rainfall. Light and heat are abundant. Most Uygurs live here. Residents mainly rely on farming for their livelihood and they eat sufficient fruits and vegetables.47 Eastern Xinjiang is a typical continental desert climate. It is arid and hot, with a large temperature difference between day and night. The annual precipitation is low and evaporation is large. Salinisation and desertification are serious.48 The natural environments, production and lifestyles mentioned above may cause differences in the morbidity and clustering of CRFs. This study suggests that the morbidity and clustering of CRFs in northern, eastern and southern Xinjiang are different, with the highest clustering of CRFs in northern Xinjiang, and a relatively low risk of CRFs clustering in southern Xinjiang and eastern Xinjiang. Therefore, it is necessary to take region-oriented CRF prevention and control measures.
The advantages of this study were distinct. First, the results were based on a community-dwelling population with a large sample size, which made our conclusions more convincible. Second, to the best of our current knowledge, this was the first epidemiological investigation of CRF clustering specifically for older people in Xinjiang. Third, the high-quality study design, high response rate, multilevel random sampling, representative samples, strict presurvey staff training and standard protocols and instruments were used to ensure the reliability of the data. Despite these strengths, our study also had several limitations. The cross-sectional studies cannot quantify the importance, nor can they determine the causality and temporality, of the relationship between CRF clustering and the prevalence of CVD. Therefore, further prospective studies should be conducted. Additionally, the study did not perform an oral glucose tolerance test or check 2-hour postprandial blood glucose, which may underestimate the morbidity of diabetes.
Conclusions
In summary, the morbidity risk of CVD in the older population of Xinjiang is high, and there are differences in CRFs based on sex, age, region and ethnic group. Some studies have found that eliminating health-threatening behaviour (such as smoking, sedentary lifestyle, unreasonable diet) through the evaluation and early screening of high-risk groups contributes to the prevention of at least 80% of CVD cases.49 Similarly, the ‘Million Hearts’ plan in the USA has achieved good results after implementation. The results of this study suggest that in the older population in Xinjiang, it is necessary to actively carry out measures for the prevention and treatment of CRFs and to formulate specific strategies based on sex, age, region and ethnic group to reduce the risk of CVD. These strategies include promoting smoking cessation among men and Han population, encouraging women to exercise and lose weight, increasing fruit and vegetable consumption for population of Northern Xinjiang and designing hypertension-prevention, diabetes-prevention and dyslipidaemia-prevention programmes for Kazakh and Hui populations. These measures might help to reduce the prevalence of CRFs and the burden of CVD.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. The original contributions presented in the study are included in the article, further inquiries can be directed to the corresponding author/s.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Ethics Committee of People’s Hospital of Xinjiang Uygur Autonomous Region (reference number:NNSFC 2016011). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We are grateful to the director of the Public Health Bureau for the continuous support of our population survey in the Altai, Tacheng, Hami, Turpan, Hotan and Kashgar. We also thank the staff of the Second Department of the Cadre Healthcare Centre of People’s Hospital of Xinjiang Uygur Autonomous Region for their support in the medical examinations and demographic data collection.
References
Footnotes
Contributors HW contributed to the study design, data collection, and provided critical manuscript revisions. WX analysed the data, interpreted the results, and wrote the article. AW, ZM, JL and SX were involved in the data collection and analysis and also provided critical manuscript revisions. All authors read and approved the submitted manuscript. HW is responsible for the overall content as the guarantor.
Funding This work was supported by the National Natural Science Foundation of China (81660242).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.