Article Text

Abstract
Objectives of study stage 1 were to: explore people’s experiences of illness due to COVID-19 while feeling socially isolated or socially isolating; identify perceptions of what would support recovery; and synthesise insights into recommendations for supporting people after COVID-19. Study stage 2 objectives were to engage stakeholders in evaluating these recommendations and analyse likely influences on access to the support identified.
Design A two-stage, multimethod cross-sectional study was conducted from a postpositivist perspective. Stage 1 included an international online survey of people’s experiences of illness, particularly COVID-19, in isolation (n=675 full responses). Stage 2 involved a further online survey (n=43), two tweetchats treated as large online focus groups (n=60 and n=27 people tweeting), two smaller focus groups (both n=4) and one interview (both using MS teams).
Setting Stage 1 had an international emphasis, although 87% of respondents were living in the UK. Stage 2 focused on the UK.
Participants Anyone aged 18+ and able to complete a survey in English could participate. Stage 2 included health professionals, advocates and people with lived experience.
Main outcome measures Descriptive data and response categories derived from open responses to the survey and the qualitative data.
Results Of those responding fully to stage 1 (mean age 44 years); 130 (19%) had experienced COVID-19 in isolation; 45 had recovered, taking a mean of 5.3 (range 1–54) weeks. 85 did not feel they had recovered; fatigue and varied ‘other’ symptoms were most prevalent and also had most substantial negative impacts. Our draft recommendations were highly supported by respondents to stage 2 and refined to produce final recommendations.
Conclusions Recommendations support access to progressive intensity and specialism of support, addressing access barriers that might inadvertently increase health inequalities. Multidisciplinary collaboration and learning are crucial, including the person with COVID-19 and/or Long Covid in the planning and decision making throughout.
- COVID-19
- REHABILITATION MEDICINE
- HEALTH SERVICES ADMINISTRATION & MANAGEMENT
- Health policy
- SOCIAL MEDICINE
Data availability statement
Data are available on reasonable request. The data produced during this study include: 1. Anonymous responses to the first online international survey—available on reasonable request 2. Anonymous responses to the stakeholder survey—available on reasonable request 3. Transcript of the two tweetchats—both are available online at: http://www.wecommunities.org/tweet-chats/chat-details/5589 https://physiotalk.co.uk/2020/09/19/support-after-covid-physiotalk-mon-5th-october/ 4. Transcript of the two focus groups with people living with Long Covid and with a person who represents people living on low incomes—due to the risks of identifiability through combined data, these are available on request supported by appropriate ethics review.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- COVID-19
- REHABILITATION MEDICINE
- HEALTH SERVICES ADMINISTRATION & MANAGEMENT
- Health policy
- SOCIAL MEDICINE
Strengths and limitations of this study
This study developed recommendations for support needed by people after COVID-19 based on experiences of a cross-sectional sample of 675 survey respondents.
Recommendations were evaluated through consultation with a variety of different stakeholders and mixed methods enabled deep insights into likely influences on people’s ability to access support.
The iterative study stages and expedited ethical review enabled specific exploration of the experiences of people with enduring impacts of COVID-19, later called by ‘Long Covid’ by many.
There was a lack of diversity among participants in the initial survey, with under-representation of people from seldom-heard groups.
No participants had received critical care due to COVID-19, possibly because people were cautioned to consider whether they would find survey completion too distressing; however, this affects generalisability.
Introduction
COVID-19 is caused by SARS-CoV-2 virus; highly transmissible and virulent, a global pandemic has resulted from its identification in late December 2019. Diagnosis is usually prompted by key symptoms, including cough, fever and fatigue and common tests are real-time reverse transcripterase PCR and lateral flow assay.1 The pandemic has had fundamental impacts on society worldwide, including the need to socially distance and isolate from other people for varied periods of time. The pandemic context has affected people’s experiences of illness in various ways, which must be explored, along with their perceptions of support needs.
COVID-19 has increased ill health in several ways. First, enormous numbers of people worldwide have contracted COVID-19 and experienced more and less severe symptoms. People with the most severe symptoms were often treated in hospital wards and critical/intensive care units (ICUs).2 Evidence indicates that people have multiple support needs after experiencing a period of critical care, due to ‘post-ICU syndrome’.3 Many people had highly distressing experiences of COVID-19 while at home or other accommodation. Other people were ‘shielding’—socially isolating due to higher risk of experiencing life-threatening symptoms of the virus. Frequently this was due to an existing or new long-term health condition which may have worsened due to negative impacts of the pandemic on provision of routine health interventions, lifestyle behaviours and mental health.4 Longer-term impacts of COVID-19 have now been identified. The Office for National Statistics (ONS) estimated that in March 2021 around 10% of people in the UK who had experienced COVID-19 were experiencing ‘Long Covid’.5 This is a term now commonly used to describe ongoing COVID-19 symptoms and impacts. The ONS found that around 18% of people self-reporting Long Covid felt that it significantly limited their day-to-day activities, posing a further public health challenge due to risk of developing further non-communicable health conditions.5 The National Institute for Health Research has progressed successive dynamic reviews focusing on Long Covid in 2020 and 2021.6 7 They found multiple body systems to be affected and suggested that Long Covid may be involve several different syndromes, possibly present at the same time.
A review of evidence relating to epidemics and health emergencies over recent years highlighted the risk of a ‘postpandemic double burden of disease’ due to these ongoing impacts.8 At a time when people’s support needs have been changing so much and so fast, this study aimed to:
Study stage 1
Explore people’s experiences of illness due to COVID-19 while feeling socially isolated or socially isolating.
Identify perceptions of what people felt would support their recovery.
Synthesise the insights into recommendations for supporting people after COVID-19.
Study stage 2
Engage stakeholders in evaluating these recommendations and analysing likely influences on access to the support identified.
Patient and public involvement
At an early stage of the project we contacted a person who had recently experienced COVID-19 and invited her to be a member of the research team (KS—coauthor). She provided valuable insights into the generation of all project materials, survey length and clarity, interpretation of analysis and development of the report. During study stage 1, we were contacted by members of a developing peer support group called ‘Long Covid Support’ (https://www.longcovid.org/). We involved them as we moved forward, developing a constructive collaboration with them and a peer support and campaigning group that developed in affiliation with them—‘Long Covid Scotland’ (https://www.longcovid.org/). This group supported study stage 2 through recruitment and review of project outputs; we have acknowledged their support.
Methods
The study took a rapid, pragmatic and postpositivist approach in order to rapidly generate recommendations for use in policy and planning relating to service provision.
Study stage 1 addressed the first two study aims relating to people’s experiences and support needs, while study stage 2 sought stakeholder feedback on our draft recommendations and their views on access to support. Figure 1 summarises the different stages.

Diagrammatic summary of the project with participant numbers.
Study stage 1: international online survey to explore people’s experiences and support needs
Study stage 1 involved an international online survey to explore people’s experiences during the period 14 July 2020 to 31 August 2020 (7 weeks). The survey was created using Qualtrics Online Survey Software (2020 Qualtrics—licence for use held by the Higher Education Institution). It was designed to focus on the specific study aims and included two validated questionnaires (described later). The survey was piloted within the research team and then with ten potential participants to ensure its usability. Some improvements were made to its format to enable easier completion on a mobile phone. Once final, the survey was circulated through research team networks and promoted extensively using social media (eg, using our Twitter handle @SupportAfterCovidStudy). The survey was designed for all people aged 18 or over internationally, who could respond in English, irrespective of whether or not they experienced illness or social isolation. The study aimed to recruit as large a number of people as possible, ideally over 500 in order to ensure that people who had experienced COVID-19 in isolation were represented. No sample calculation was conducted; instead, the aim was to promote the survey widely to ensure wide participation within the short timescale. People saw an email, tweet, or post online with a brief invitation to view the study webpage (https://www.cpcpr.org/COVID-19) which held further information about the study. Advice was provided that if recalling experiences of illness while feeling isolated would cause unmanageable discomfort or distress, it would be best not to take part in the survey. The information explained that people could close the survey at any time and their data would not be analysed, but once they clicked on ‘submit’, data could not be extracted due to anonymous completion. They were informed that the survey would take 15–20 min to complete. If people felt that they met the criteria and were willing to participate, they clicked on the web link to the survey in Qualtrics, which implied consent. The survey questions are available online at: https://26205d15-9a75-4aa4-b2d2-185aee599a78.usrfiles.com/ugd/26205d_377147626804489d92c2aec43e3a6bd4.pdf
First, participants were asked about specific demographic characteristics and any existing physical and mental health conditions. The next questions asked if they had felt isolated and if they had, they were asked if they had experienced illness during this time. When designing the survey we focused on perception of illness, as this should be differentiated from disease.9 Those who responded ‘yes’ were asked if they thought this was due to COVID-19. Where someone did, they were asked for more detail about their experiences, including timing, support received and recovery. People who did not feel they had recovered were asked about the nature and impacts of their ongoing symptoms. Participants completed the validated 20-item Post-Traumatic Stress Disorder Checklist for DSM-510 and the 6-item version of the de Jong Gierveld Loneliness Scale .11 12 Data from these questionnaires will be reported in depth elsewhere with treatment of missing data. Finally, all survey respondents were asked if they felt that they needed any help to support their health and well-being, with a space provided for open responses. This was the final question and all responses from this section were included in descriptive categorisation of responses as people had completed and submitted the survey. People were thanked and given further guidance on how to access support if completing the survey had led to unexpected distress. We asked people if they would be willing to be followed up in 6 months, reported elsewhere.
Data from study stage 1 were imported into R-studio (V.1.3.1093) running R (V.4.0.3) for further organisation and advanced statistical analyses. Primarily descriptive analysis was used to develop draft recommendations about what services and/or interventions people may need to support them after having COVID-19.
Study stage 2: stakeholder consultation (UK focused) on draft recommendations and access to support
A stakeholder consultation focused on finding out if the draft recommendations were appropriate, clear and sufficient, as well as gaining insights into access to support. It was important to find different ways of engaging remotely with people with diverse experiences and expertise relating to COVID-19, for example, people who had experienced COVID-19, who had family or friends who experienced COVID-19, who were involved in providing, designing or funding services for people affected by the pandemic, or in relevant policy. All participants were expected to be aged 18 or over and able to respond in English. The aim was to achieve as much participation as possible within the tight timescales of the study (approximately 3 weeks for stage 2 data collection). Three strategies were used:
Stakeholder survey: a second online survey using Qualtrics asked for the person’s role and degree of agreement with each recommendation in turn (5-point Likert scale: strongly disagree—strongly agree). For each recommendation, an open question asked for the person’s thoughts on access to the service/strategy/intervention. Participants were asked if anything was missing in the draft recommendations. Participants could also email the Principal Investigator directly if preferred. As for the first survey, the survey was promoted through research networks and social media. Survey questions can be viewed at: https://26205d15-9a75-4aa4-b2d2-185aee599a78.usrfiles.com/ugd/26205d_a9882a2c2cd0455994c302becd90a682.pdf . Descriptive analysis of the results focused on frequencies of agreement with each recommendation and categorisation of open responses to questions about access to support.
Tweetchats with professional online communities: Numerous professions have online communities which meet on a regular basis for scheduled 1-hour discussions on specific topics. Two tweetchats were held as large online focus groups:
In collaboration with WeCommunities.org (28 September 2020, including member communities such as nurses, mental health nurses, allied health professionals and healthcare managers).
With physiotalk.co.uk (5 October 2020: physiotherapy-focused online community).
Both tweetchats were carried out as large online focus groups, with information on the study, the draft recommendations and the key discussion questions uploaded to the appropriate websites 2 weeks before the chat. Tweets were sent out in this period and during the tweetchat to remind people that this chat would be analysed for the Support After COVID-19 Study. Participants were informed that if they wanted their tweet(s) to be removed from analysis they could contact the researchers in the 2 weeks following the chat to request this. Full chat information and transcripts can be found at: http://wecommunities.org/tweet-chats/chat-details/5589, and https://physiotalk.co.uk/2020/09/19/support-after-covid-physiotalk-mon-5th-october/.
The questions and polls are provided in online supplemental file 1. Both tweetchats took place 20:00–21:00 and the Symplur transcript of the chat was downloaded for 75 min to capture the end of the discussion. A pragmatic categorisation of the tweets was undertaken.
Supplemental material
Online focus group discussions and individual interviews: In order to address a lack of diversity in responses to the first survey and emergence of Long Covid we carried out further qualitative data collection. The Scottish campaigning arm of LongCovid.org (https://www.longcovid.org/) forwarded our email inviting their members to participate in focus groups, resulting in two separate online focus groups with four people (all women) in each. Study information was sent to the distribution list of the Third Sector Research Forum in Scotland (https://evaluationsupportscotland.org.uk/tsrf/). This has member organisations that work with people who may be under-represented when it comes to research and who may experience quite specific influences on their access to support. One person agreed to participate, representing people living on low incomes. Focus groups and the interview were carried out using Blackboard Collaborate and recorded with flexible use of a topic guide. The topics focused on people’s experiences relating to COVID-19, views on the draft recommendations (clarifications and additions), access to support, experiences that the participants would have liked to be different and key messages for people making decisions about supporting people during this time. Thematic categorisation of responses was undertaken from a postpositivist perspective.
Results
Figure 1 summarises participant numbers in study stages 1 and 2. Results include participant characteristics, results of study stage 1 and development of the draft recommendations relating to people who have experienced COVID-19 in isolation, then results of study stage 2 and modification of the recommendations.
Study stage 1: international online survey results
In total 835 people responded to this survey, 675 of whom provided answers to all survey questions. Most were living in the UK (86.52%) while others were based in India (3.7%), Ireland (2%), the USA (1.3%), Canada (1%), Germany (0.7%) and other countries (4.6%). The mean age of the participants was 44 years (18–87 years). Detailed participant characteristics are provided in online supplemental file 2). Figure 2 summarises the numbers of participants in relation to their experiences of isolation and illness, including COVID-19. A total of 202 people provided their email addresses, permitting us to contact them for follow-up in 6 months’ time.
Supplemental material

Study stage 1: summary of isolation and illness showing how many people were or felt they were socially isolated, how many felt ill and how many thought this was due to COVID-19.
In study stage 1, 29% of survey respondents experienced illness while socially isolating and/or feeling isolated and 19% of respondents thought they had COVID-19 due to positive COVID-19 tests and/or exhibiting one or more of the signs identified by the government.
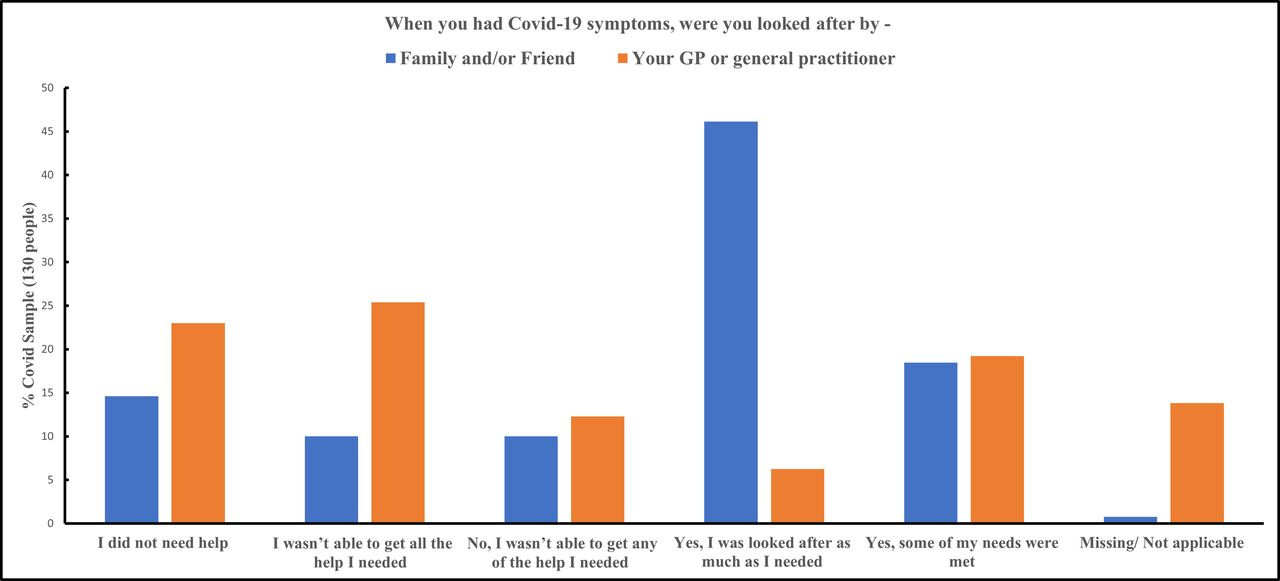
Perceptions of support from general practitioners (GPs) and from family and friends are illustrated in figure 3. Summing the % frequencies that indicate a person did not get any, or all, of the help they needed, this was around 20% in relation to support from family and/or friends, and over 35% when seeking help from a GP.
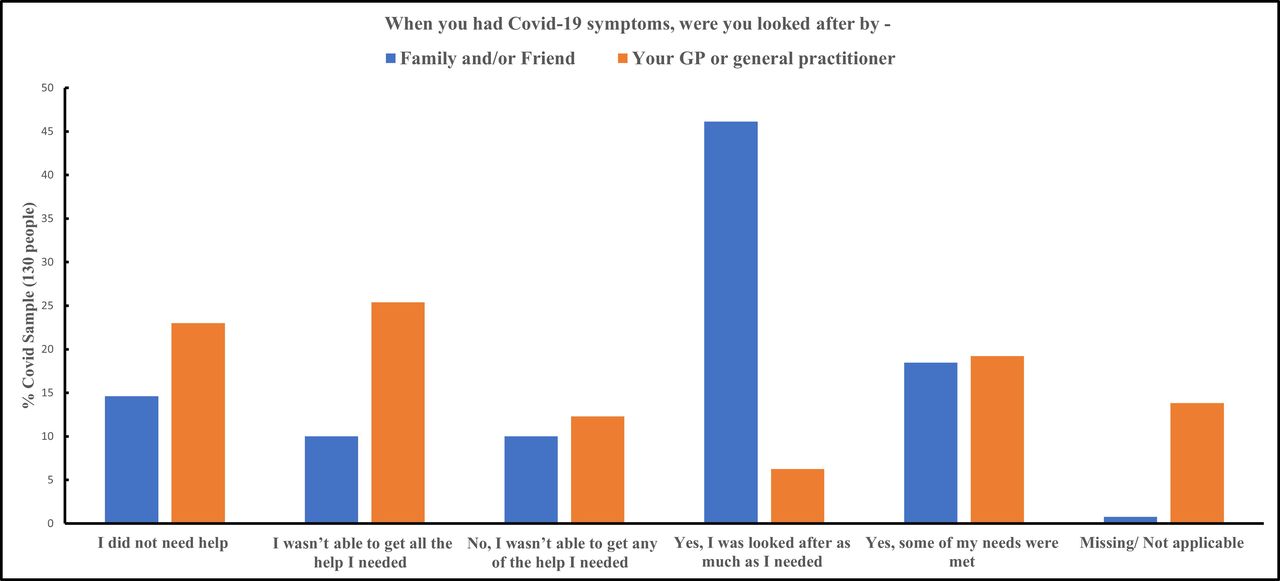
Perceptions of support from GP and from family/friends while ill with COVID-19. GP, general practitioner.
Of the 130 people who reported COVID-19, 16 had been hospitalised. Seven people were admitted to a general ward and were there for 3.4 days on average. Nine people were admitted to a COVID-19 ward and were admitted for 3 days on average. No participant was admitted to the ICU.
Four people reported that their symptoms started in December 2019 (3.29%), 4 reported February 2020 (3.29%), 89 reported March 2020 (65.93%), 26 reported April 2020 (21.97%) and 6 reported May 2020 (4.39%). Forty-five people out of 130 felt recovered and reported that this took an average of 5.26 weeks (range 1–54 weeks).
The remaining 85 participants did not feel that they had recovered at the point of completing the survey. People who had not recovered were asked about which difficulties they had, and how much each bothered them (options: not at all, a little bit, moderately, quite a bit, extremely; 45 people provided this score). The most prevalent ongoing challenge was fatigue, with 93% of people with ongoing symptoms or challenges selecting this. The next was breathlessness (65%), followed by ‘getting around’ (56%), home care (51%) and ‘other’ (44%). No one selected 0 (no bother) for any ongoing symptom or challenge, indicating that all caused some degree of difficulty for people. For most items people selected Likert scores from 1 (a little bother) to 4 (extreme bother) except for ‘self-care’ and ‘other’, where the minimum score was 2 (moderate bother). When looking at the mean Likert score for each symptom or challenge, on average the most concern was caused by ‘other’ symptoms, listed in figure 4. This was followed by similar scores for fatigue, getting around, self-care and home care. The mean Likert scores did not vary widely, however, ranging from 2 to 3.4. The more symptoms or challenges a person had, the greater the degree of difficulty they reported for each of these symptoms or challenges.
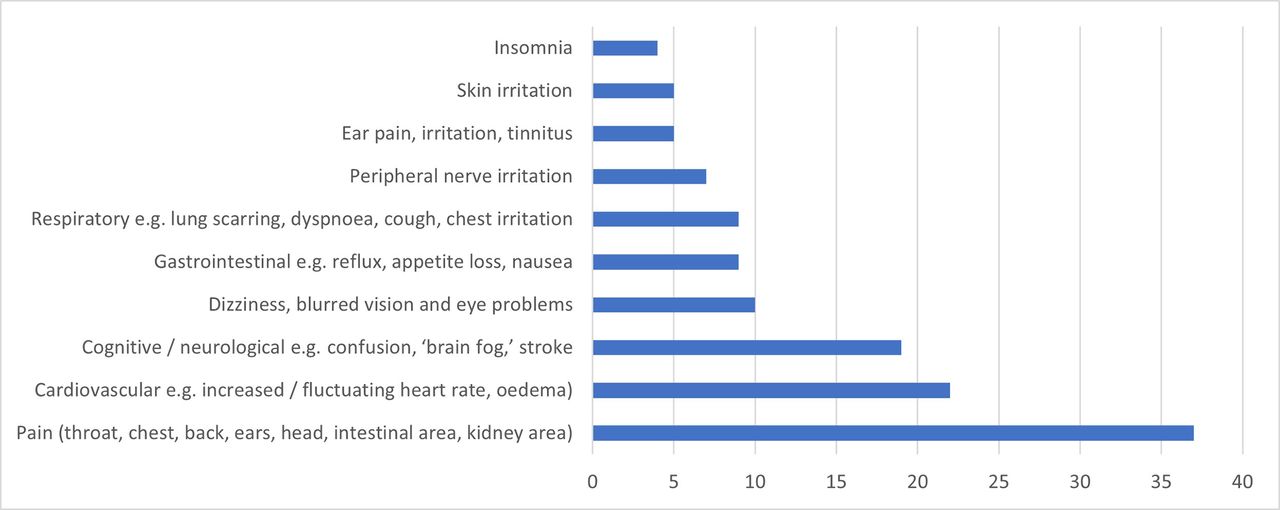
Frequencies of ongoing symptoms/challenges listed by respondents under ‘other’
Of those who had had COVID-19, 72 (55% of 130) provided further information in an open response question relating to whether, at that point in time, they felt that they needed help to support their health and well-being. Responses were categorised and frequencies of response analysed (online supplemental file 3). Overarching categories were derived from these:
Supplemental material
Recognition, understanding, clarity and reassurance.
Social/community support and participation.
Support with medical needs.
Support for mental health.
Support for physical function and activity.
Support for cognitive function and neurological symptoms.
Support for life roles and activities.
Preferred model of service provision post-COVID-19.
Types of support from which people might benefit were derived from these needs and triangulated against the difficulties that people were having when recovering from COVID-19 to ensure that these were addressed. Both enabled development of draft recommendations (online supplemental file 4). The way in which the data contributed to these recommendations is provided in online supplemental file 5 for auditability. Draft recommendations were revised based on reviews of all research team members and four people who have had COVID-19.
Supplemental material
Supplemental material
Study stage 2: stakeholder consultation on the draft recommendations (UK focused)
Stakeholder survey (survey 2) participants
Forty-three people responded and their different interests or roles are summarised in figure 5. Most lived in the UK (93%), with 22 in England, 16 Scotland, 2 in Wales and 0 in Northern Ireland. Three people were from outwith the UK (Ireland, Italy). A wide spread of geographical areas across each country were represented.

Numbers of stakeholder survey respondents within each ‘stakeholder category’.
Participants in tweetchats with professional online communities
At least 180 people participated in the WeCommunities tweetchat and completed the first poll. Of these participants, 60 people contributed a total of 368 tweets. This tweetchat included representatives of several different member communities and included a higher number of nurses, as well as some allied health professionals. At least 34 people participated in the physiotalk tweetchat and completed the first poll, with 27 people contributing 241 tweets. Participants were primarily physiotherapists, some of whom were also discussing the topic from the perspective of a person living with Long Covid.
Figure 6 shows results of the first poll in both tweetchats, broadly indicating the types of service represented. Similar proportions of tweetchat participants in both WeCommunities and Physiotalk represented the acute sector. Far more people in the WeCommunities tweetchat worked in the community, with more Physiotalk participants working in rehabilitation. It was clear that perspectives were gained from a wide variety of health providers across the UK and from diverse health contexts. It is possible that some participants represented social services as well, but this is less clear.

Summary of services represented in each tweetchat.
Participants in online focus group discussions and individual interviews
Two separate online focus groups were conducted with four people (all women) in each. All had Long Covid and were members of ‘Long Covid Scotland.’ One interview was carried out with a person who worked for an organisation that represents people living on a low income.
Findings: stakeholders’ views on the draft recommendations for support
Focusing first on results of the stakeholder survey: Frequency (n) of Likert scoresrelating to stakeholder views on the appropriateness of recommendations for support were calculated, followed by percentage frequency of responses to the survey (% of 43) (figure 7)

Stakeholder survey: summary of overall agreement with each draft recommendation.
Second, considering the qualitative stakeholder data—pragmatic categorisation of the comments (see mind maps in online supplemental files 7–10) enabled refinement of the recommendations for support, based on:
Supplemental material
Supplemental material
Supplemental material
Supplemental material
Open responses within the Stakeholder survey.
Online tweetchats with professional online communities: WeCommunities and Physiotalk.
Focus groups with people from the LongCovid.org Scottish campaigning group, and one individual interview (representing people living on low incomes).
Categories that supported and/or suggested modification to each recommendation are summarised in table 1. There was support for all recommendations, and suggestions for refining recommendations were made in relation to all except recommendation 9. There were also suggestions for additional recommendations that relate to people who have not necessarily had COVID-19 but who have been affected negatively by the pandemic, reported elsewhere.
Summary of responses relating to each recommendation from stakeholder engagement activities
Findings: analysis of factors that may affect access to support for people who have had COVID-19
Pragmatic categorisation of qualitative data (see mind maps in online supplemental files 7–10) also enabled summary and interpretation of factors that may affect access to the support suggested in the first draft recommendations. It was interesting that, for the most part, similar concerns came up in discussion with different stakeholders. These are summarised in box 1 and provide valuable insights into the many possible barriers to access that should be considered in the design of policies, strategies, services and interventions.
Summary of factors thought to affect access to support for people who have had COVID-19
Concerns regarding access to support with consensus in all stakeholder groups.
Restriction of services due to availability of funding, staff and other resources which have been impacted by the pandemic.
Impacts on access from further periods of high infection, lockdown or shielding.
Increased waiting lists due to the pandemic, with implications for people who have had COVID-19 accessing specialist services.
Better understanding is needed of longer-term effects of COVID-19 to expedite early diagnosis and timely, effective treatment.
Population-level data on long-term symptoms, their prevalence, duration and response to interventions should be recorded by general practitioners (GPs) and other health and social care professionals to inform optimal services and interventions.
Involvement of people with lived experience is crucial to evaluate services and enable improvement.
Employment policies should support phased work return/restricted or adapted roles to enable people to recover and remain within the workforce, with financial support for this journey.
Online information on COVID-19 and signposting to support services should be freely available on a range of online platforms, by telephone and in-person, using community languages, to ensure accessibility and allow people to access this by their preferred means.
There should be other forms of support that are accessed through local third sector and community organisations and libraries to support people who do not have access to the internet or the ability to navigate online resources sufficiently to gain full benefit.
Access to support services should be based uponon need, irrespective of positive COVID-19 testing, diagnosis, or other personal characteristics such as age, living situation, gender or ethnicity.
Nurses and allied health professionals discussed frequent funding of services for specific health conditions or age groups, for example, some rehabilitation services are not available to people of younger ages who are now experiencing need for support due to longer term impacts of COVID-19.
People need their GPs and health professionals to be aware of available services to provide signposting.
The right skill mix is needed to support people with highly varied long-term impacts of COVID-19, involving multiple body systems and support needs.
The value of a ‘one stop shop’ or ‘COVID-19 Clinic’ was emphasised by people with lived experience to reduce the strain of navigating services and facilitate development of expertise.
Access to support should not be based on severity of acute COVID-19 as this was not seen by professionals to correlate with severity of ongoing cognitive impacts.
There should be attention given to patient pathways and transitions between services, especially post-discharge.
The challenges of accessing health services can impact negatively on mental health and compound existing challenges.
People living on lower incomes and with unstable employment may be less able to access testing and support for COVID-19 and have greater difficulties advocating for themselves, especially where these issues intersect with others such as rurality, digital deprivation and exclusion as well as being from a Black, Asian and minority ethnic (BAME) community.
There is evidence emerging relating to lack of trust in circulating information and a growing antiexpert agenda which requires further attention to facilitate access to support.
Any national guidelines would require some form of oversight, to ensure they remain evidence based and to explore ways of ensuring that they are implemented.
Revised recommendations
For auditability, (online supplemental file 11) tracks the draft recommendations (full and abbreviated), the modification suggested with data source, and the revised recommendations (full and abbreviated). The abbreviated revised recommendations are included below in figure 8.
Supplemental material

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Revised recommendations for supporting people after COVID-19.
Discussion
Nearly one-fifth of the survey respondents reported having had COVID-19. Over 35% did not feel they had received all the support they needed from their GP, which may partly relate to the fact that the majority reported their symptoms as having started in March or April 2020, early in the pandemic. Although 35% of those with COVID-19 felt they had recovered, this had taken an average of over 5 weeks. A much higher proportion than expected were still experiencing symptoms, with fatigue as the most common, which is in line with further research.5–7 This was followed by a variety of different symptoms provided by participants under the category ‘other’. These two challenges were also perceived to be having the greatest negative impact on people, followed by breathlessness, reduced mobility and difficulty taking care of the self and the home. People who experienced COVID-19 and may have been experiencing Long Covid described substantial support needs. Data suggested huge variation in the amount, specialism and timing of help needed. The stakeholder consultation demonstrated strong support for the recommendations and enabled these to be refined and clarified. Numerous possible barriers to accessing services were identified by stakeholders and provide insights that can be used by policy makers and service providers.
This is a developing area of research which has gathered pace over recent months, demonstrated through the Office for National Statistics data and through the National Institute for Health Research Dynamic Reviews.5–7 Both have substantial strengths in the sample size and rigour of the former, and the ongoing critical synthesis of emerging literature for the latter. This study has found greater prevalence of Long Covid among those who have had COVID-19 than the Office for National Statistics: approximately 20%, compared with 10%.5 This may relate to a response bias in the current study, with people more likely to respond where they have specific interest in the topic. The first study stage was a cross-sectional survey promoted by social media. Potentially related to different preferences for use of social media, participants lacked diversity, with greater participation of women and with under-representation of seldom-heard groups. It is also important to note that a large proportion of respondents were from the UK, despite international distribution of the survey. We chose to honour the respondents by including all usable data, and we were interested in perceived support needs as more universally experienced—what people felt that they needed rather than what they had received. It is possible, however, that people may not have expressed a ‘support need’ if it was being met; this may have led to differences in response from people experiencing different health systems and public health measures as regional differences exist.13 Recommendations for support were based most heavily on people’s responses to open questions, with closed questions providing further descriptive information about what people had experienced. The open questions required people to type their thoughts into the online survey tool, which could feel cumbersome or time consuming to some. Despite this, numerous very detailed responses were provided. This study was carried out at a time of rapid change and learning in relation to experiences of COVID-19. The iterative study stages and expedited ethical review enabled response to some of the changes and learning from the first stage. As a result, perspectives from people with Long Covid were explored through focus groups. The recruitment strategy for this sub-study did not focus on women, however, only women responded to the invitation. A further study could be carried out that focused on recruiting men, however, it may be necessary to use a different recruitment strategy. Additional strategies in the study also enabled some learning about seldom-heard groups, although this did not include people from Black, Asian and minority ethnic communities. It was unexpected that none of the study stage 1 participants had been admitted to the ICU. This may be because the introductory survey information emphasised that the person should only participate if they felt that it would not be unduly distressing. It does, however, affect generalisability.
This study findings align with those of the second National Institute for Health Research dynamic review6 and Office for National Statistics data4 in relation to the debilitating impacts of Long Covid on people’s family and working lives. with similar findings in relation to one of the most prevalent ongoing symptoms being fatigue and a variety of other reported symptoms demonstrating involvement of different body systems. Findings are also aligned in finding Long COVID-19 to be prevalent in people of working age and who were not hospitalised due to COVID-19. It is important to note that the Office for National Statistics and National Institute for Health Research dynamic reviews highlight disproportionate impacts on people living on lower incomes and from minority groups.4–6 The current study adds rich insights from varied stakeholders into both support needs and aspects of policy and service design that are important to address in order to ensure people can access such support.
It is evident that long-term effects of COVID-19 are highly prevalent and people have substantial support needs. The prevalence of people living with Long Covid will keep increasing and will have substantial economic impacts due to the severity of impact in many cases and the ages of many people affected. The highly varied presentation and lack of knowledge in relation to Long Covid pose barriers to recovery. These issues intersect with lack of availability and further barriers to accessing individual services, making it exhausting for people who are ill to navigate service pathways. There was some consensus among different stakeholders that for such a new health condition, with such complexity and need for knowledge development, a ‘one-stop shop’ would be most beneficial, providing support from multiple health professions, social services and vocational rehabilitation. Such support would also help people navigate other systems with potential to impact on their abilities to focus on and benefit from rehabilitation, such as seeking financial support. It was clear that need for support varies greatly, and it makes sense that the insights learnt through a focused service are then disseminated to people who need less intense help, for example, through websites and telephone helplines. This would enable specialist resources to be more focused on people who need them. Stakeholders commented on the erosion of trust in relation to health-related messages, with people experiencing feelings of abandonment that impact negatively on their mental health. It is crucial to seek ways to regain credibility and clarity. People are having very different experiences of seeking help and access to support depending on their income, type of employment, culture, experience of existing health conditions and journeys relating to COVID-19. Services must carefully consider barriers to access in their design to ensure that they do not inadvertently exacerbate health inequalities. Policy development should ensure communication between sectors such as health and social care, the third sector, workplace and employment, with careful consideration of how policies intersect.
Over 200 participants from stage 1 consented to being contacted after 6 months in order to explore their experiences longitudinally through a follow-up survey and qualitative interviews. This will be reported elsewhere. There is much to learn from existing literature and practice experience that relate to the management of chronic fatigue and Chronic Fatigue Syndrome / Myalgic Encephalomyelitis (ME), and to supporting people after critical illness. Evaluation of telehealth strategies in supporting people is crucial, hopefully enabling more intense and/or in-person intervention to be made more accessible to those with greatest need. Parallel research and development are needed, however, in relation to solutions for people who are not able to use online or digital solutions for various reasons. Specific areas that emerged as requiring research and development include: impacts of COVID-19 on mental health, cognition and cardiorespiratory symptoms; its illness trajectory, relapse triggers, interventions and return to work strategies. All should meaningfully involve people with lived experience. Specifically designed research is needed that engages meaningfully with people who are seldom heard, including people from different Black, Asian and minority ethnic communities. As the field develops, it may be appropriate to conduct an expert consensus study that includes people with lived experience, focusing on optimal support strategies. The area has also progressed through the development of vaccines and there is a need for further research into vaccine hesitancy—the extent of which differs regionally.13
Conclusion
This two-stage, multimethod study used online quantitative and qualitative tools to describe explore people’s experiences of illness due to COVID-19 while feeling socially isolated or socially isolating and to develop recommendations for supporting people after COVID-19. This study found around one in five people who have had COVID-19 to be experiencing enduring symptoms and challenges. Fatigue and varied ‘other’ symptoms were most prevalent and also had most substantial negative impacts. Recommendations were made that support access to progressive intensity and specialism of support, addressing access barriers that might inadvertently increase health inequalities. Multidisciplinary collaboration and learning are crucial, including the person with COVID-19 and/or Long Covid in planning and decision-making throughout. This field is at an early stage, with much further research needed. One area that might easily be neglected is how to support people who are vulnerable and seldom-heard, particularly people who are living on low incomes and who are from minority groups.
Supplemental material
Data availability statement
Data are available on reasonable request. The data produced during this study include: 1. Anonymous responses to the first online international survey—available on reasonable request 2. Anonymous responses to the stakeholder survey—available on reasonable request 3. Transcript of the two tweetchats—both are available online at: http://www.wecommunities.org/tweet-chats/chat-details/5589 https://physiotalk.co.uk/2020/09/19/support-after-covid-physiotalk-mon-5th-october/ 4. Transcript of the two focus groups with people living with Long Covid and with a person who represents people living on low incomes—due to the risks of identifiability through combined data, these are available on request supported by appropriate ethics review.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Queen Margaret University Ethics Committee-stage 1 approved 22 June 2020; stages 2–3 approved 17 September 2020. No reference number available because this is not a normal practice for the ethics committee in question. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We wish to acknowledge the valuable input of Long Covid Scotland and Long Covid Support in supporting the second stage of the project in particular, including valuable support to talk to people living with Long Covid and in discussion of the study findings. We also gratefully acknowledge all participants in both stages of the project.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @CathyBulley1, @Profbrendan, @jandewing
Contributors The initial study design and funding application was carried out by CB, VT, KN, LS, BM, RM, OS and JD. The full study proposal and ethics application was developed with the input of all coauthors, who also participated in interpretation and discussion of study results and final conclusions. Data collection, ongoing analysis and reporting was conducted by CB, EC and VT, as was development of the initial manuscript. CB is responsible for the overall content as the guarantor.
Funding This work was supported by a grant from the Chief Scientist Office, Scotland (Rapid Research in Covid -19 programme: COV/QMU/20/04).
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.