Article Text

Abstract
Objectives To analyse the association between individual and contextual socioeconomic position (SEP) with health status and to investigate the role of SEP and baseline health status on survival.
Design Cross-sectional and cohort study.
Setting Rome, Italy.
Participants, primary and secondary outcomes We selected the 25–99 year-olds included in the Rome 2011 census cohort. As a measure of health status on the census reference date (09 October 2011), we used the presence of chronic or rare conditions from the Disease-Related Co-payment Exemption Registry, a database implemented to provide free care to people with chronic or rare diseases. We used logistic regression to analyse the association between both individual (educational attainment) and contextual SEP (neighbourhood real estate price quintiles) with baseline health status. We analysed the role of SEP and the presence of chronic or rare conditions on 5-year survival (until 31 December 2016) using accelerated failure time models with Weibull distribution, reporting time ratios (TRs; 95% CI).
Results In middle-aged, subjects with low SEP (either individual or contextual) had a prevalence of chronic conditions comparable with the prevalence in high SEP individuals 10 years older. Adjusted logistic models confirmed the direct association between SEP and baseline health status in both women and men. The lowest educated were up to 67% more likely to have a chronic condition than the highest educated, while the difference was up to 86% for lowest versus highest contextual SEP. Low SEP and the presence of chronic conditions were associated with shorter survival times in both sexes, lowest versus highest educated TR was TR=0.79 for women (95% CI: 0.77 to 0.81) and TR=0.71 for men (95% CI: 0.70 to 0.73). The contextual SEP shrunk survival times by about 10%.
Conclusion Inequalities were present in both baseline health and survival. The association between SEP and survival was independent of baseline health status.
- EPIDEMIOLOGY
- SOCIAL MEDICINE
- PUBLIC HEALTH
Data availability statement
No data are available. The data sets analysed during the current study are not publicly available due to privacy policies.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This work links the information of baseline health status with individual socioeconomic position (SEP), contextual SEP and survival.
We used the administrative cohort of the entire Italian adult population of Rome (1.8 million individuals).
The individual and contextual SEP measures have good reliability and help to account for different facets of individual wealth, resources and human capital.
Presence of chronic conditions from the Disease-Related Co-payment Exemption Registry could underestimate mild forms of illness.
Changes in contextual SEP and presence of chronic or rare conditions during the follow-up were not considered in survival analyses.
Introduction
Multiple factors such as sex, socioeconomic position, citizenship and ethnicity are associated with differences in health. Some inequalities are unavoidable, others represent disparities in opportunities, knowledge and resources that could be reduced or avoided by ad-hoc policies.1 2 Among the characteristic of a population, socioeconomic position (SEP) is often used to tackle avoidable disparities in health. Overall and cause-specific mortality appear to be inversely correlated with SEP,3–6 as well as the prevalence of different diseases,7–9 multimorbidity10 11 and access to healthcare.12 13 There are several, valid, indicators of SEP,14 15 each representing different facets of individual wealth, resources and human capital. While personal SEP represents actual material or immaterial resources directly owned by the individual, contextual SEP expresses the reality and opportunities of the context in which the person lives. Both individual and contextual measures are found associated with health outcomes either used alone,3 10 11 or used together.6 16 17
In Italy, there is a universal healthcare system, where healthcare is publicly funded and there is general access and comprehensive coverage under the National Health Service. All subjects have free access to hospital care, general practitioner visits, screening programmes and maternity care. However, all individuals contribute to payments for drugs (especially to brand-name drugs when a generic drug exists), to emergency room visits in absence of an emergency and to outpatient care, both for specialist visits and diagnostic tests and procedures.18 As in several other countries, there are cost-sharing exemptions for people economically disadvantaged.19 Moreover, in 1999, the National Health Service set up a co-payment exemption for people with chronic or rare diseases to cover outpatient specialist services aimed at monitoring the disease and at preventing further aggravations.18 20 The recognition of the co-payment exemption right is obtained after a request to the local health unit of residence with a certificate, issued by a medical doctor from a public hospital, attesting the presence of the disease.20
This study had two main goals. The first was to analyse the association between individual and contextual SEP with health status, as the presence of a chronic or rare condition from the Disease-Related Co-payment Exemptions Registry. The second goal was to investigate the role of (individual and contextual) SEP on survival, considering the baseline health status in a cohort of 1.8 million adults followed for 5 years.
Methods
Design
We used a cross-sectional design to investigate the association between SEP and health status at baseline, and a cohort design to analyse the role of SEP on survival taking into account the baseline health status.
Setting and participants
Rome is the largest Italian city, with a surface of 1290 km2 and a population of 2.5 million residents at the 2011 census. The Rome longitudinal study included the residents in Rome who filled in the 2011 census questionnaire.6 The census included several individual information, such as sex, age, achieved education and residential census area. Through an anonymous identifier, the subjects enrolled were linked to the Municipal Registry database and the Regional Health Information System, which includes the Mortality Registry and the Disease-Related Co-payment Exemption Registry. The record-linkage procedures were performed under strict control to protect individual privacy. The Rome longitudinal study is part of the National Statistical Program 2019 and was approved by the Italian Data Protection Authority. The study excluded subjects without an identifier, the homeless and those living in institutions (such as prisons, nursing homes, monasteries, or convents), overall, the 1.43% of the census population.
Since the interest in this study was to have both individual and contextual measures of SEP, only residents in census areas located in residential neighbourhoods, and with the same address in both census and Municipal Registry database, were included (excluding 2.35% of the census population). Finally, only Italian citizens aged 25–99 years at the census reference date (09 October 2011) were selected.
Variables of interest
Two different measures of socioeconomic position were considered: the educational attainment achieved at the census date (individual SEP) and the quintiles of the distribution of neighbourhood real estate prices (contextual SEP).
The individual SEP was categorised considering the differences between birth cohorts. The variable was defined as ‘Low’ for compulsory education, that is, primary education for individuals born before 01 January 1952 and lower secondary education for individuals born after. It was defined as ‘Medium’ for degrees higher than compulsory education but lower than tertiary degrees. Finally, individual SEP was defined as ‘High’ for tertiary education, that is, bachelor’s, master’s or PhD degrees independently of the cohort.
The contextual SEP was obtained by assigning to all residents the average 2010 housing price (€/m2) of the neighbourhood21 and then calculating the quintiles of the distribution weighted on the population, to have 20% of individuals under study in each quintile.
The number of chronic or rare conditions was derived from the Disease-Related Co-payment Exemptions Registry from 01 January 2008 to 09 October 2011. To characterise the baseline health status of the population, a binary variable indicating the presence of a chronic or rare condition was used.
Age in complete years at the census date, categorised in 10-years age groups and sex have also been included in the analyses.
Statistical analysis
Frequencies and graphical displays have been used for descriptive analyses.
Binary logistic regressions to estimate the association between the presence of chronic or rare diseases (1=present, 0=absent) with the measures of SEP were implemented. ORs and their 95% CIs adjusted for age and stratified for sex have been estimated and reported along with those stratified by sex and adjusted for every other variable in the analysis.
Subjects were followed from the census reference day (09 October 2011) to the first event of censoring, that was, the date of emigration outside Rome, the 100th birthday, the date of death or 31 December 2016, whichever came first. Accelerated failure time (AFT) models assuming Weibull distribution for the log-time have been used and shown, the results were reported in terms of time ratios (TRs) along with 95% CI. Estimations of expansion (shrinkage) of times reported in the manuscript were adjusted for age and presence of chronicity, and stratified for sex, along with estimates stratified by sex and adjusted for every other variable in the study.
In all models, we analysed significant trends across categories of both SEP using Wald tests. Also, all models were checked for multicollinearity through the estimation of variance inflation factors (VIF). All analyses were performed using R V.4.0 or higher.
Sensitivity analyses
As sensitivity analyses, we ran ordinal and non-proportional odds models using a three-category chronicity (0-1-2+) instead of the dichotomic variable as the response. We also implemented sensitivity analyses on survival models using the three-category chronicity variable in place of the dichotomic variable.
Patient and public involvement
No participants were involved in our work as we used administrative data and was not possible to have access to individual contact information or involve participants in the study due to privacy policy restrictions. We aim to disseminate results to the population as part of our Institutions’ mission.
Results
Descriptive analysis
A total of 1 780 243 individuals, resulting from the above-mentioned selection, have been analysed.
Table 1 shows the socio-demographic characteristics of the study population and the prevalence of chronic diseases. The population was mostly composed of women (54.2%), people aged between 45 and 54 years (19.5% of the female population and 21.2% of the male population) and individuals with medium educational level (45.8% of women and 47.9% of men). The percentage of people with at least one chronic condition increased with age, it was higher in women than in men and was inversely related to educational attainment and quintile of real estate prices.
Description of the study population by demographic characteristics, socioeconomic positions and presence of chronic or rare disease (CRD). Rome, 09 October 2011, 25–99 year-olds
The most common chronic conditions recognised for the co-payment exemption were hypertension, diabetes and cancer. Although these conditions were in the top three for all educational levels, some differences in the prevalence were seen. In the low educated, hypertension was the most common cause of chronicity (9.9% of the low educated population) followed by diabetes (8.5%) and cancer (5.2%). In the highly educated, the main cause of disease was cancer (3.6% of the highly educated), followed by hypertension (2.9%) and diabetes (2.2%). The same pattern was found using the contextual SEP variable.
In figure 1 the percentage of individuals with chronic or rare diseases by age group, sex and educational attainment is shown. Although there was a clear increasing pattern over age as well as the differences between SEP categories in both sexes, the gap across levels of education was more marked for women than for men. It is possible to compare the proportion of subjects with at least one chronic condition by age and educational level. For example, the 22% of highly educated women in the age group 55–64 had at least one disease, while in the group of low educated, roughly the same proportion was reached in those aged 45–54 (21%). Similar patterns can be observed for the other sex: low educated men with 55–64 years had the same proportion of chronic conditions as highly educated individuals in the age group 65–74 (30%).

Percentage of individuals with chronic or rare disease (CRD) by age, sex and educational attainment.
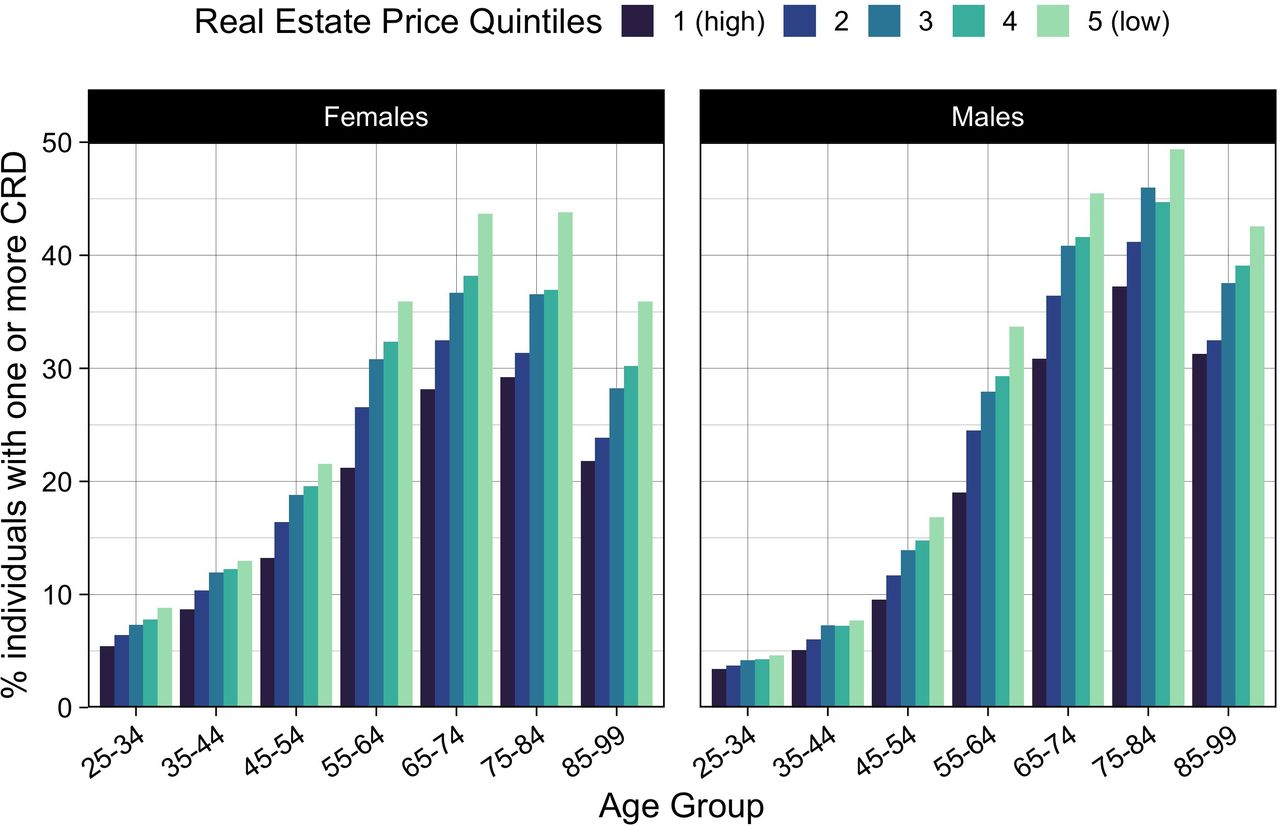
Figure 2 shows the percentage of individuals with chronic or rare diseases by age group, sex and real estate price quintiles. The differences between the lowest and the highest contextual SEP increased steadily with increasing age group. In figure 2, it is also possible, given a proportion of individuals affected by chronicity, to compare the differences in age group by SEP. As in figure 1, the lowest SEP group aged 45–54 had a proportion of chronic conditions like those of the highest SEP in the age group 55–64 for both women (22% lowest, 21% highest) and men (17% lowest, 19% highest).

{kind=link}
{kind=link}
Percentage of individuals with chronic or rare disease (CRD) by age, sex and real estate price quintiles.
Cross-sectional analysis
Table 2 shows the results from logistic regression implemented to identify the association between the two measures of SEP and the presence of chronic or rare diseases on the census reference day. Age-adjusted and sex-stratified OR are reported with 95% CI. Educational attainment had a clear negative gradient, both medium and low educated people, either female or male, are shown as more likely to have at least one chronicity than the reference category of highly educated (low educated women: OR 1.61, 95% CI: 1.59 to 1.64; low educated men: OR 1.67, 95% CI: 1.64 to 1.70). It should be noted that OR for men with medium education was closer to OR for lower educated than women were. The contextual SEP showed a strong negative association with the response variable. Those living in the least expensive neighbourhoods (fifth quintile) were almost twice as likely to have chronic conditions than people in the most affluent quintile (women OR 1.86, 95% CI: 1.83 to 1.89; men OR 1.83, 95% CI: 1.80 to 1.87). The strength of the association for both individual and contextual SEP decreased when the complete model was considered, but all associations remained significant as well as the overall trends as shown in online supplemental table S1. The check for multicollinearity showed VIF always lower than 2.5 in every logistic model, indicating the absence of strong correlations among variables.
Supplemental material
Association between indicators of socioeconomic position and presence of chronic or rare diseases. Italian residents aged 25–99 years. Rome, 09 October 2011
Results obtained from sensitivity analyses with ordinal models and non-proportional odds models were very similar and never differed in meaning and trend from those obtained with logistic models (not shown).
Survival analysis
During the study period (09 October 2011 to 31 December 2016) 64 978 women and 58 680 men died (for a total of 123 656 deaths), 55 702 were lost due to emigration outside the municipality of Rome (27 537 women and 28 165 men), 1578 women and 378 men reached the 100th birthday and were censored, and 1 598 929 were still alive at the end of the follow-up (870 193 women and 728 736 men).
Table 3 shows the results from AFT models, TR adjusted for age and presence of chronicity and stratified by sex are reported with 95% CI. Individual SEP was found directly associated with survival: people with both medium and low education had shorter survival than the reference category either women or men. Educational attainment had a stronger effect on men than on women (low educated females TR 0.79, 95% CI: 0.77 to 0.81; low educated males TR 0.71, 95% CI: 0.70 to 0.73). Contextual SEP showed an impact on survival across each category, compared with the highest, the lowest quintile had a survival time of 93% in women (TR 0.93, 95% CI: 0.91 to 0.95) and 88% in men (TR 0.88, 95% CI: 0.86 to 0.91). The variable with the strongest association with survival was the presence of chronic conditions at baseline: women having chronicity shortened the mean survival time approximately by a fourth compared with women without chronic conditions (TR 0.73, 95% CI: 0.72 to 0.74). A similar effect was found in men (TR 0.69, 95% CI: 0.67 to 0.70) for which having certified chronicity was comparable to having low educational attainment.
Association between indicators of socioeconomic position and survival. Italian residents aged 25–99 years. Rome, 2011–2016
All the associations lost some strength in the fully adjusted model shown in online supplemental table S2, but they remained statistically significant and there was only a slight change in the effect size. The only exception was the effect of the real estate price quintiles that became non-significant. All AFT models showed lower VIF than the chosen threshold of 2.5.
As sensitivity analyses, we ran AFT models replacing the dichotomic chronicity variable with a three-level variable. The strength of the association between indicators of SEP and survival was comparable to results presented in table 3 and online supplemental table S2. Having two or more chronicity had a higher impact on survival than having one. In the sex-stratified and age-adjusted models, women with one chronic condition had survival times shortened by a fifth (TR 0.79, 95% CI: 0.77 to 0.80) and those with two or more about a third (TR 0.66, 95% CI: 0.65 to 0.67). Similarly, men with one chronicity had TR=0.75 (95% CI: 0.74 to 0.77) and TR=0.62 (95% CI: 0.61 to 0.64).
Discussion
Principal findings
Our analysis of the 2011 Rome cohort found an inverse association between both individual and contextual SEP indicators with having a chronic or rare disease, an inverse association of chronicity with survival, and a direct association between individual and contextual SEP with survival. These associations enlighten the presence of multiple levels of inequalities in the Rome cohort of 2011 always disadvantaging the lower strata of SEP. The first level of inequality is at the individual level: highly educated individuals have an advantage in health as less likely to suffer from a chronic condition, and an advantage in survival taking account of baseline health status, as more likely to live longer than low educated. This advantage could be due to immaterial resources (knowledge and awareness attained from education itself), but also to material resources (wealth obtained from better-paid jobs, resulting in the possibility to afford healthier life conditions). The second level of inequality is at the neighbourhood level: people living in wealthier neighbourhoods are more likely to be in better health and to live longer than individuals who are living in more disadvantaged areas. A worse and shorter life characterises the more disadvantaged groups of the population in Rome.
This work shows a difference in baseline health of about 10 years in middle-aged between low and high SEP (either individual or contextual), for both sexes. The percentage of individuals with a chronic or rare disease reaches a plateau and then a reduction at old ages. The authors attribute this phenomenon to two possible explanations. The first is the action of a selection effect, by which only healthier individuals reach older ages. The second explanation is that a competing action of the most common type of income-related co-payment exemption, acquirable after 65 years of age and not considered in this study, could have occurred. However, a strong competing action between the two types of exemptions is considered unlikely. In fact, income-related co-payment exemption does not cover drug expenditures. Moreover, 37.7% of 65+ year olds that had an income exemption had also an exemption in the Disease-Related Co-payment Exemption Registry, and the exemption right based on the income is given by the Tax Agency independently on the health condition of the user. On the assumption that Income-exemptions compete with Disease-Related Co-payment Exemptions, underestimation of inequalities in baseline health and overestimation of the effect of SEP on survival might exist.
Every analysis reported in this work shows that individual and contextual SEP are inversely associated with having at least one chronic condition. The association between SEP and having a Disease-Related Co-payment Exemption was stronger for contextual than individual SEP, this result is unexpected because individual indicators are generally more strongly associated with health than the contextual ones.16 17 22 Our results on inequalities in the presence of chronic conditions, although not fully comparable, show similar patterns to a study based on 2007 Scottish data, which found a higher prevalence of multimorbidity in lower area-deprivation deciles.11
Results of survival analysis are consistent with previous works on the Rome population and general studies on inequalities. A study found an inverse association between education and overall or cause-specific mortality in the Rome census cohort of 2001.23 Association between real estate price quintiles and mortality, when the educational level is considered, has been found in recent research.6 In our complete model, the contextual SEP had no association with survival times, when the other measure of SEP was considered. In both logistical and survival analyses, we found stronger inequalities for men than for women as already reported in the literature for similar cohorts.3
Strength and weakness of this study
This work has its limitations. Mainly, chronicity data should only be considered as a proxy of morbidity but not as a substitutive measure due to a possible underestimation of mild forms of chronic conditions. The measure was obtained from the Disease-Related Co-payment Exemption Registry, an administrative data set implemented to help people with chronic or rare diseases to receive appropriate and free-of-charge assistance. The data set was not intended for medical or statistical purposes, leading to rough definitions of chronicity and the possibility to observe only the more severe conditions. Nevertheless, good reliability over severe forms of illnesses is expected because a medical certificate is needed and the economic advantage deriving from the co-payment exemption should incentivise all the people with chronic or rare diseases to apply for it. However, people with multiple chronicity may not be interested in multiple certificates as the expenses for specialist visits or diagnostic tests could be already covered, totally or partially, by the first certificate. This might result in marked differences between who owns a chronicity certificate and who does not, and in smaller differences between who has one certification and who owns more. From this last point comes our choice to dichotomise the variable in our study. Finally, a small proportion of the well-off population could rely on private insurance companies and not use the National Health Service. However, the proportion of the wealthy population leaning on private insurances is expected to be small as in 2011 the voluntary health insurances covered around 1% of the whole health expenditure.18 Under the assumption that higher SEP were less likely to request co-payment exemptions for conditions with non-expensive treatments, an overestimation of inequalities in baseline health might exist. On the opposite, the same assumption would result in an underestimation of the association between SEP and mortality. In this work, we explicitly or implicitly stated that SEP (individual and contextual) acts on health, but a reverse pathway is plausible. Individuals in bad health conditions during their youth may have more difficulties attending school, thus, limiting their instruction to lower levels. Those individuals could also have fewer opportunities to find well-paid jobs that would allow them to afford houses in wealthy neighbourhoods. Moreover, we considered as lost to follow-up all subjects who moved from Rome during the study period. In logistic regressions, implemented to analyse differences in baseline characteristics between those lost to follow-up and the rest of the population, we found that younger people, individuals with lower education, residents in higher quintiles neighbourhoods and people in good health were more likely to emigrate. However, in a previous work, the results obtained using an inverse probability approach to weight for the characteristics of the population were very similar to those from the unweighted analysis.23 Finally, changes in neighbourhood during the follow-up were not considered, but bias would happen only if individuals would have changed neighbourhood quintiles.
The main strengths of this work are the huge statistical power, the good reliability of the two measures of SEP and the robustness of the results to sensitivity analyses. Thanks to the access to administrative Roman databases, we could use almost all the Italian adult population residing in Rome, basing our estimates on more than 1.7 million individuals. Data on educational attainment came from the census, one of the most reliable data sources. Unobserved changes over time of the measure are possible but unlikely since we only analysed individuals aged 25 or more. Moreover, the real estate price is one of the main factors in selecting a population within a city.24 The average real estate price has the strength to be openly and easily available and has the potential to synthesise in one measure the quality of life in the neighbourhood with its services and infrastructures, but also in terms of perception and social prestige. Finally, sensitivity analyses using a different categorisation for the chronicity data and/or based on the implementation of different models showed minimal differences in the results and none in the meaning or the trend.
Our results highlight the need for ad-hoc policies aimed to help the most disadvantaged strata of the Rome population, to reduce socioeconomic inequalities in health that exist even in a universal healthcare coverage setting. Further studies using comorbid conditions estimated using different data sets could improve the quality of the analysis, reducing the bias and making results comparable in terms of diseases and multiple diseases with international literature.
Conclusions
Inequalities are present in both health and survival, with lower SEP having always worse outcomes than higher SEP. Lower SEP undergo a double inequality in health: the higher likelihood of being affected by at least one chronic condition, which is associated with shorter survival per se, and a shorter survival independently of the presence of chronicity.
Data availability statement
No data are available. The data sets analysed during the current study are not publicly available due to privacy policies.
Ethics statements
Patient consent for publication
Acknowledgments
We are grateful to Laura Cacciani who helped us with her insightful comments, and the three reviewers who gave great inputs to improve our work.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors LDB and GC conceived the idea and designed the study in collaboration with NA and AMB. EC and GC were responsible for the acquisition of the data. LDB was responsible for undertaking the data analysis and producing the tables and graphs, together with EC and GC. VE, EC, GC, NA and AMB provided input into the data analysis. NA, AMB and MD contributed to the interpretation of the results. The manuscript was drafted by LDB and GC, and then shared with all authors for critical revision. LDB is the guarantor of the study. All authors have read and approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.