Article Text

Abstract
Introduction Cryptococcal meningitis is a common fungal opportunistic infection and a leading cause of death among people with advanced HIV disease in sub-Saharan Africa. The WHO recommends cryptococcal antigen (CrAg) screening followed by pre-emptive therapy to prevent cryptococcal meningitis and death in this population. In 2016, South Africa was the first country to implement reflexive laboratory CrAg screening nationally. The Cryptococcal Antigen Screen-and-Treat National Evaluation Team (CAST-NET) aims to evaluate the effectiveness of this national screening programme to optimise health outcomes.
Methods and analysis The CAST-NET study consists of two integrated parts: a retrospective cohort study and a cluster-randomised trial (CRT). The retrospective cohort study will determine 6-month cryptococcal meningitis-free survival among CrAg-positive patients. Secondary outcomes include the proportion of CrAg-positive results noted for action in the CrAg-positive patient chart, the proportion of CrAg-positive patients offered and accept/decline a lumbar puncture, the proportion of CrAg-positive patients prescribed antifungal therapy and the proportion of CrAg-positive patients who have antiretroviral therapy initiated or reinitiated at an appropriate time according to South African national guidelines. Cohort data will be analysed by the type of facility (ie, hospital vs primary health clinic) at which the patient was diagnosed with antigenaemia. The CRT will determine if the appointment and mentoring of a healthcare worker, or ‘crypto champion’, at intervention facilities is associated with a higher proportion of CrAg-positive persons initiating pre-emptive fluconazole therapy. Secondary outcomes will include 6-month cryptococcal meningitis-free survival and the proportion prescribed fluconazole maintenance treatment.
Ethics and dissemination Ethics approvals were received from the University of the Witwatersrand Human Research Ethics Committee (Medical), the University of KwaZulu-Natal Biomedical Research Ethics Committee and the University of Pretoria Faculty of Health Sciences Research Ethics Committee. Study results will be disseminated to the South African Department of Health and participating facilities through peer-reviewed publications and reports.
- protocols & guidelines
- public health
- HIV & AIDS
- diagnostic microbiology
- epidemiology
- health policy
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
The study will evaluate South Africa’s national cryptococcal antigen (CrAg) screening programme in two interlocking parts: (1) a retrospective cohort study which will identify programmatic gaps in the clinical management of CrAg-positive patients, and (2) a cluster-randomised trial (CRT) which will evaluate the effect of a facility-level intervention to address identified programmatic gaps on initiation of antifungal treatment among CrAg-positive patients.
The overall design of this evaluation study is efficient because we will use the same methods to determine the outcomes in both the retrospective cohort and CRT.
Data quality and completeness is quality checked prior to abstraction by trained medical staff; identified gaps and missing data can be queried through targeted investigations during repeat rounds of data collection.
Patient outcome data from charts will be supplemented with routine data from alternative sources (eg, national death registers).
Retrospective chart review has the potential for selection and information biases as not all patient charts will be found, found charts may be incomplete and abstraction of patient charts by medical professionals is subject to information bias due to heterogeneity in interpretation.
Introduction
Cryptococcal meningitis (CM) is a common fungal opportunistic infection and is, after tuberculosis (TB), a leading cause of death among people living with advanced HIV disease in sub-Saharan Africa. Cryptococcus neoformans is the most common cause of meningitis among adults in South Africa, more common than bacterial meningitis.1 2 The annual global burden of CM was estimated to be 223 100 cases in 2014, with an estimated 181 100 (81%) deaths (95% CI 119 400 to 234 300), of which approximately 75% occurred in sub-Saharan Africa.3
Despite now-universal access to antiretroviral therapy (ART) in South Africa, with approximately 4.65 million people living with HIV on ART in 2019, the incidence of cryptococcal disease has only minimally decreased based on national surveillance.4 From 2018 to 2019, the incidence of laboratory-confirmed cryptococcal disease remained stable at 88 cases per 100 000 HIV-infected persons. In the Eastern Cape, Northern Cape and North West provinces, the incidence risk of cryptococcal disease increased from 2018 to 2019.5 Thus, cryptococcal disease is still a public health problem in South Africa.
CM substantially contributes to mortality among patients starting ART with advanced HIV disease. Between 8% and 26% of patients starting ART with advanced HIV disease die during the first year of treatment, with most deaths occurring during the first few months of ART.6–8 ART initiation can also be dangerous for ART-naïve patients with advanced HIV disease and CM. A randomised clinical trial demonstrated a twofold higher risk of mortality when ART was initiated before the completion of CM induction therapy versus deferring ART initiation until 4–6 weeks after CM diagnosis.9
In 2011, the WHO recommended screening asymptomatic HIV-seropositive persons with a CD4 count of <100 cells x 106/L for cryptococcal antigenaemia and then pre-emptively treating those with a positive cryptococcal antigen (CrAg) test with fluconazole. In 2018, the WHO conditionally recommended CrAg screening and pre-emptive treatment for all patients with a CD4 count of <200 cells x 106/L .10 A randomised clinical trial primarily informed this WHO recommendation.11 In the trial, CrAg screening and 4 weeks of ART adherence support resulted in a 28% relative reduction in 12-month mortality among persons with a CD4 count of <200 cells x 106/L.11 Within South Africa, reflexive laboratory CrAg screening is preferred to provider-initiated CrAg screening due to its expedited result delivery to combat loss to follow-up and proven cost-effectiveness.12
In 2016, with the support of the South African National Department of Health (NDOH), the National Health Laboratory Service (NHLS) implemented national reflexive laboratory CrAg screening of all persons with a CD4 count of <100 cells x 106/L. To ensure the success of the CrAg screening and treatment programme, the following steps in the cascade of care should be optimised. CrAg screening among eligible people with advanced HIV disease must be maximised. All CrAg results must be returned to medical charts and acted on by clinicians. A lumbar puncture (LP) must be performed to exclude CM. CrAg-positive persons must be prescribed and complete fluconazole therapy and initiate or reinitiate ART if interrupted.
Methods and analysis
Study design
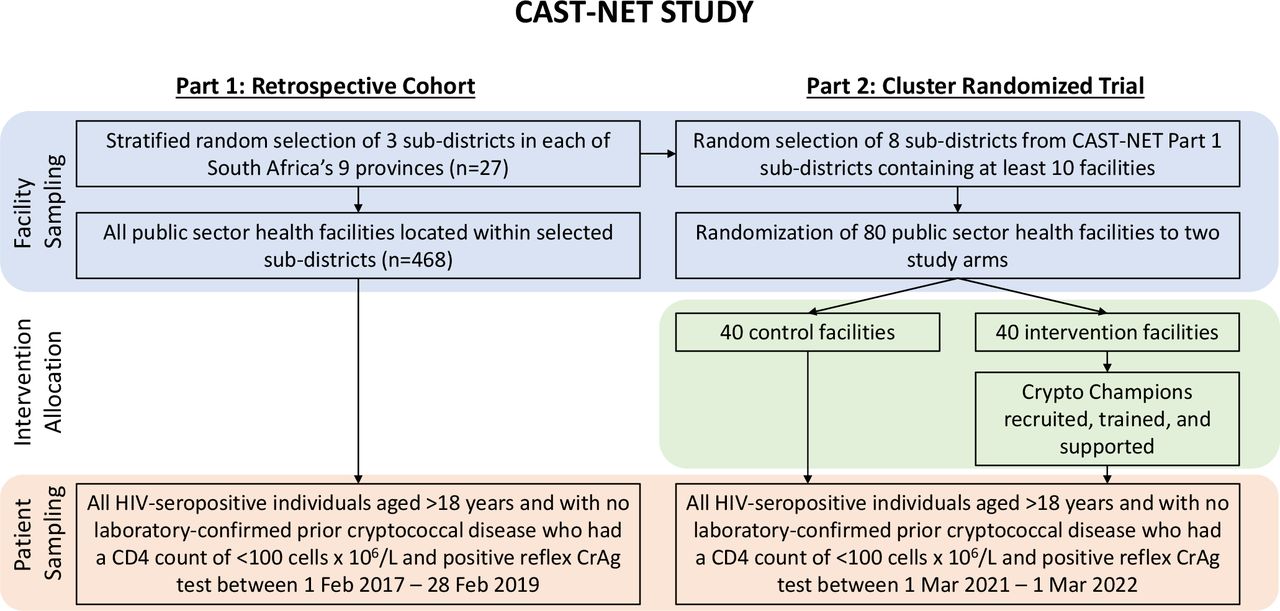
The Cryptococcal Antigen Screen-and-Treat National Evaluation Team (CAST-NET) study consists of two integrated parts: a retrospective cohort study and a cluster-randomised trial (CRT). Data will be collected by retrospective chart imaging/abstraction and other routine data sources to measure and analyse outcomes of interest among CrAg-positive patients meeting study inclusion criteria. These analyses will be used to identify programmatic gaps and develop an intervention for the CRT. The CRT draws from the same random sample of subdistricts, and all healthcare facilities within these subdistricts, as the retrospective cohort study (figure 1). Staff training and processes established during data collection for the retrospective cohort study will be reused within the CRT expediting data collection. Through these integrated parts, the CAST-NET study will aim to evaluate the effectiveness of this national screening programme. Inclusion criteria will be the same for both the retrospective cohort study and the CRT. Study participants must be HIV seropositive with a CD4 count of <100 cells x 106/L, aged >18 years, have no history of cryptococcal disease, have a positive cryptococcal blood antigen test and seeking care at a public healthcare facility within one of the randomly selected subdistricts included in the study. The retrospective cohort will include all CrAg-positive reflex results between 1 February 2017 and 28 February 2019. The CRT has a 12-month study enrolment period starting from 1 March 2021 through 1 March 2022.

Integration of the retrospective cohort study and cluster-randomised trial within the Cryptococcal Antigen Screen-and-Treat National Evaluation Team (CAST-NET) study. CrAg, cryptococcal antigen.
Part 1: retrospective cohort study
Sample
The theoretical sampling population will consist of all patients accessing healthcare through the South African public health service. Subdistricts will be the primary sampling unit as they are the lowest level of governmental public health management and represent a small geographical grouping of healthcare facilities and attending patients. Subdistricts will be ranked by socioeconomic tertiles derived from the South African census poverty head count.13 A random sample of 27 of South Africa’s 246 subdistricts, 9 subdistricts from each of the 3 socioeconomic tertiles, and 468 enclosed facilities, excluding correctional, mental health, mobile, armed service and elderly care, will be chosen for the effectiveness evaluation (figure 2).13 All attending patients with blood samples submitted to an NHLS CD4 laboratory and who meet the inclusion criteria will be enrolled in the study.

Subdistricts and facilities by type included in the Cryptococcal Antigen Screen-and-Treat National Evaluation Team (CAST-NET) retrospective cohort study.
Sample size calculation
The sample size will be dependent on the number of persons who are screened for CrAg nationally during the study period. There is no intervention assigned within the retrospective cohort study. The goal is to establish baseline figures for the South African national screening programme. We know that in four districts in Gauteng and Free State provinces, 50 000 persons had a CD4 count of <100 cells x 106/L of whom 3% tested positive for cryptococcal antigenaemia between September 2012 and September 2015.14 Expert opinion estimates there will be between 14 000 and 17 000 asymptomatic CrAg-positive cases and between 6000 and 8000 symptomatic cases of CM nationally each year.
Outcomes measured
The primary outcome measured is 6-month CM-free survival among enrolled CrAg-positive patients. Secondary outcomes include the proportion of CrAg-positive patient results that are noted for action in the patient chart, the proportion of CrAg-positive patients offered and accept/decline an LP, the proportion of CrAg-positive patients prescribed antifungal therapy and the proportion of CrAg-positive patients initiating or reinitiating ART at an appropriate time as per South African national guidelines.4
Data analysis plan
The analysis plan for data will consist of a descriptive cohort analysis comparing primary and secondary outcomes at provincial and national levels as well as by important exposures such as facility type (hospital vs primary health clinic). Baseline patient demographics will also be summarised. Patient demographics will include age, gender, CD4 count at time of reflex CrAg testing and ART status (naïve vs experienced).
Part 2: cluster-randomised trial
Sample
For the CRT, we will take a simple random sample of eight subdistricts, containing at least 10 facilities, included in the retrospective cohort study (figure 3). Of these eight subdistricts, all facilities with at least one CrAg-positive patient expected over a 6-month time interval will be randomly assigned a number. Using a random number generator, facilities will be assigned to either the control or intervention arm and placed in consecutive order. Five facilities will be randomised to the control arm. Facilities will be assigned to the intervention arm and invited to participate in the study until the five facilities per subdistrict quota is met. All study staff except for the biostatistician, project manager, principal investigator and administrators contacting the facilities will be blinded to the randomisation until the final intervention facilities are confirmed.

Subdistricts and facilities included in the Cryptococcal Antigen Screen-and-Treat National Evaluation Team (CAST-NET) cluster-randomised trial.
Sample size calculation
For the CRT, the power and sample size depend on the average number of patients per cluster, in this case, the facility, and the assumed intracorrelation coefficient (ICC). Early interim screening data showed that 56% of patients were appropriately prescribed fluconazole and that an average of 8.1 (95% CI 7.0 to 9.24) patients with a CD4 count of <100 cells x 106/L and a positive CrAg test presented per facility over the enrolment period, 1 February 2017 to 28 February 2019. The ICC is estimated at 0.03 based on expert opinion.15 An estimated average of six patients with a CD4 count of <100 cells x 106/L and a positive CrAg test will present per facility over the 1-year study enrolment period. Each study arm will have 40 facilities, leading to a total of 80 facilities and 480 patients. This sample size provides 85% power to detect a 14% improvement in the proportion prescribed fluconazole in the intervention arm with a two-sided alpha of 0.05.
Intervention measured
The CRT will aim to determine if a facility-level intervention is associated with a higher proportion of CrAg-positive persons initiated on pre-emptive fluconazole therapy. The control will be the standard of care as stated by the national guidelines.4 16 The intervention will be the informal appointment and mentoring of a healthcare worker dubbed a ‘crypto champion’ to take ownership of the CrAg screen and treat programme within their facility. We hypothesise that the crypto champions will increase the proportion of CrAg-positive persons initiated on pre-emptive fluconazole therapy through the identification, investigation and resolution of gaps within the cascade of care.
The crypto champion will be a permanent employee based at the facility willing to take on this informal voluntary role in addition to their usual duties with no formal remuneration. They will have a fairly senior rank in the clinic (eg, professional nurse/pharmacist), have the support of managers to take on this role, be a present and reliable clinic employee (eg, history of good work and attendance) and be able to prescribe fluconazole. The primary function of the crypto champion will be to take ownership of CrAg screening and pre-emptive treatment in the clinic improving fluconazole initiation among CrAg-positive persons. Their responsibility will be to ensure CD4 testing of HIV-infected persons re/entering care, placement of positive CrAg laboratory results in patient charts, communication of follow-up dates for CrAg-positive patients, hospital referral for an LP and prescription of fluconazole.
To ensure fidelity across intervention facilities, the crypto champions will be given in-service training on treatment of persons with advanced HIV disease and cryptococcal disease, real-time access to a clinician with experience treating patients with cryptococcal disease and linkage to community and patient HIV care advocate groups. Crypto champions will use a checklist to track patient movement through the crypto cascade ensuring full adherence to national/provincial guidelines while decreasing loss to follow-up (figure 4). Crypto champions will report key indicators set by the study team on a weekly basis. Assistance will be provided to crypto champions not meeting indicator targets. Non-monetary incentives will be provided, such as sponsored attendance of a conference or additional training courses.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Crypto champion checklist for new cryptococcal antigen (CrAg)-positive test results. ART, antiretroviral therapy; LP, lumbar puncture.
Outcomes measured
The primary outcome measured is the proportion of CrAg-positive patients initiated on pre-emptive fluconazole therapy across both study arms. Secondary outcomes include the proportion of patients with 6-month CM-free survival and the proportion of patients prescribed fluconazole maintenance treatment across both study arms.
Data analysis plan
Analysis of data from the CRT will summarise the number and characteristics of each clinic by treatment group. Baseline clinic characteristics will include subdistrict, location (urban or rural) and clinic type. Baseline demographics will also be summarised for patients within each treatment group. Individual-level logistic regression appropriate for CRTs (hierarchical models) will be used to compare the two randomised groups for the primary and secondary outcomes. Odds ratios (intervention compared with standard of care) and 95% CIs will be cited. The intraclinic correlation coefficient will be reported for the primary outcome.
Data sources
The retrospective cohort study and the CRT draw from the same data sources. All reflex CrAg-positive test results performed on remnant bloods from CD4 laboratories will be accessed from the National Institute for Communicable Diseases (NICD) surveillance data warehouse (SDW) and deduplicated to patient level creating a primary patient list. Patients meeting inclusion criteria will be included in the study. Prior crypto will be assessed in two ways; first, we will pull all laboratory test results based on SDW’s unique patient ID for the prospective participant and ensure no prior CM or antigenaemia-positive results. We will then look up the patient in GERMS-SA, an active NICD surveillance system, with reporting from approximately 200 clinical microbiology laboratories across public and private sectors, that captures patients with CM, cryptococcaemia (positive cryptococcal blood cultures) and culture-positive disease at other sites, but excludes cases of cryptococcal antigenaemia.5 17 Additional data sets will be accessed to support chart finding at facilities such as Tier.Net, a non-networked electronic register capturing patient-level HIV data at facility level. Since 2010, Tier.Net has been the primary monitoring platform for South Africa’s national ART programme. TIER.Net has incrementally expanded capturing patient-level HIV, ART, pre-ART and TB data. Its integration with the District Health Information System enables reporting from subdistrict to national levels.17 TIER.Net will be used to track treatment, facility attendance, and to bolster patient chart finding. We will also merge in data from a Department of Home Affairs death register, consisting of patient deceased status and deceased date, to ascertain and validate the outcome of 6-month survival post-CrAg specimen taken date.
Data management
For both the retrospective cohort and CRT, the collection and abstraction of primary source data will be managed through an electronic data capture system, REDCap. REDCap will host instruments capturing the progression of data collection across multiple rounds and data abstraction. A standard clinical case report form (CRF) designed by study staff will be created in REDCap to capture key information on patient outcomes. Automated reports will be run from REDCap enabling the tracking of data collection progress, chart finding proportions by facility, management and reimaging of blurred images and rationale for charts not found/qualification of missing data. To ensure patient confidentiality, a participant ID will be assigned to each patient. All patient identifiers within their medical records will be redacted, or covered, by data collection staff prior to chart imaging. Imaged patient charts displaying patient-identifying information will be flagged within REDCap and digitally redacted by the data manager. Quality control procedures validating data set merges, clarity of chart imaging and measurement of key indicators such as number of tests and patients included in the study will be carefully assessed by the NICD as the study progresses. All data will be hosted on a secure cloud-based storage system with data ownership solely retained by NICD and the University of Minnesota. Manual backups onto a secure password-protected external hard drive will be performed regularly throughout data collection. Imaged patient charts will be renamed to simply convey a patient identification number, where the chart was located, and when data were collected. The CRF will be completed for each patient within REDCap leading to the creation of a data set that will be cleaned, quality checked and exported for analysis. Imaged patient charts and all other data produced by the study will be retained for a period of 5 years before deletion in line with ethics and best practice guidelines.
Data collection
The method of data collection for both the retrospective cohort and CRT is chart imaging and abstraction. Patient charts will be accessed and imaged by trained data collection teams and abstraction will be carried out by clinicians. The benefit of this data collection methodology is that data can be collected at numerous facilities simultaneously, key outcomes of treatment initiation and 6-month survival can be captured simultaneously and missing data can be queried through repeated rounds of facility visits. Data collection for the retrospective cohort will be more resource intensive than the CRT as 468 facilities from 27 subdistricts will be enrolled compared with 80 facilities from eight subdistricts in the CRT. Facility and healthcare worker surveys will be administered at each facility during the retrospective cohort study to identify facility-level gaps in CrAg screening, to highlight differences between facilities nationwide and to qualify missing data.
Data collection for retrospective chart review is expected to be complex and laborious because of the paper-based medical record system used in South Africa’s public sector. Retrospective chart review requires locating charts, the redaction of personal information and imaging. Each facility has different organisational protocols and resource limitations leading to difficulty locating charts. The aim of the data collection team’s primary facility visit will be to introduce the study and gain support from the management, identify and establish rapport with key facility staff and image easy-to-locate patient charts. To mitigate selection bias, additional rounds of data collection will be required for facilities with chart-finding percentages below 80%.
During repeat data collection visits, a facility-specific report on CrAg screening and CAST-NET chart finding will be provided to facility managers. Further engagement and support from facility managers into locations of unfound patient charts will be required to increase chart finding. If necessary, patient lists will be revised to match the facility-specific organisational systems. Patient death and ART treatment registers will be used in the retrieval of records for patients who are deceased or have defaulted on ART. Alternative locations highlighted by facility staff and management, such as wards and clinics within hospitals, will be examined. Throughout the study, data collection teams will be repeatedly trained on best practice methodologies to increase patient chart finding.
Patient charts will be imaged by data collection teams at the facility in which they are found. All patient identifiers will be covered prior to imaging, except a study-specific patient identifier. A batch imaging programme will be used to combine all imaged pages within a patient record into one electronic document. Hard copy patient charts will be returned to facility staff and refiled once imaging is complete. Hard copy patient charts will never leave the facility. The electronic copy of the patient chart will be uploaded to a secure cloud-based storage system. Quality checks will be performed to reorient pages, redact missed patient identifiers and save batched images as PDF files. Quality-checked patient charts will be copied to a final images folder to be accessed for abstraction. Data collection progress will be captured electronically in real time using REDCap data collection instruments.
Patient and public involvement
There is no patient involvement.
Ethics and dissemination
The study protocol is approved by the University of the Witwatersrand Human Research Ethics Committee (Medical), the University of KwaZulu-Natal Biomedical Research Ethics Committee and the University of Pretoria Faculty of Health Sciences Research Ethics Committee. There is no interface with patients and data are collected retrospectively; therefore, individual informed consent is not required. All patient-identifying information such as patient name, national ID, date of birth, contact information and all information pertaining to contacts will be redacted prior to abstraction of patient information. Targeted reports will be generated for Department of Health as well as for each facility included in the CAST-NET study. Results will be disseminated through peer-reviewed papers as well as conferences.
Ethics statements
Patient consent for publication
References
Footnotes
Contributors DJD wrote the initial draft of the manuscript. EVS wrote the introduction section. NPG and DRB will be responsible for guidance and direction of the CAST-NET study and take overall responsibility for the manuscript as senior authors and coprincipal investigators. RR, CPS, RM and JP provided clinical insight into the development of clinical case report forms and abstraction processes. ASB and KHH provided insight into sample size, power and analyses. GG and DJD provided insight into data collection, data management and data sources. All authors contributed to the conceptualisation and design of the study. All authors read and approved the final manuscript.
Funding This work was supported by NIH (grant number: R01AI118511).
Map disclaimer The inclusion of any map (including the depiction of any boundaries therein), or of any geographic or locational reference, does not imply the expression of any opinion whatsoever on the part of BMJ concerning the legal status of any country, territory, jurisdiction or area or of its authorities. Any such expression remains solely that of the relevant source and is not endorsed by BMJ. Maps are provided without any warranty of any kind, either express or implied.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.