Article Text

Abstract
Objective To evaluate the association of serum vitamin D levels and dietary intake with melanoma risk and prognostic factors.
Methods Two independent investigators systematically searched PubMed, Embase and ISI Web of Knowledge (Thomson Scientific Technical Support, New York) databases for eligible studies published between January 1992 and September 2020 using the following combinations of search terms: (vitamin D, or 25-hydroxyvitamin D) AND (melanoma, malignant melanoma, cutaneous melanoma, or cutaneous malignant melanoma). Articles not written in English but with English titles and abstracts were also checked. We obtained the full text of all potentially eligible articles, and reference lists of all studies retrieved at the first stage were also checked to identify other eligible papers. Review articles not reporting original data were excluded, but their reference lists were inspected.
Results Six studies including 212 723 cases reported the association between dietary intake of 25(OH) D serum levels and melanoma risk. The total relative risk for the comparison between the highest and lowest quantiles of the distribution of vitamin D intake was 1.10 (95% CI 0.96 to 1.26) with I2=56%. Another six studies including 12 297 cases evaluated the association between serum vitamin D levels and melanoma risk. The total relative risk for the comparison of serum vitamin D levels between the highest and lowest quantiles was 1.12 (95% CI 0.53 to 2.35) with I2=91%. Four studies with 2105 cases investigated the association between serum 25(OH)D (nmol/L) and Breslow thickness, three of which found an inverse association between serum 25(OH)D (nmol/L) and melanoma thickness.
Conclusions Vitamin D intake and serum 25(OH)D levels were not closely related with melanoma risk, but an inverse association between serum 25(OH)D levels with melanoma thickness was discovered. As the positive correlation between melanoma thickness and melanoma mortality has been recognised, hence it is concluded that a moderate dietary vitamin D supplement to avoid the serum 25(OH)D deficient might be beneficial to the long-term survival of patients with melanoma.
- ONCOLOGY
- DERMATOLOGY
- Dermatological tumours
- Public health
Data availability statement
All data included in this study are available upon request by contact with the corresponding author.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This is the first systematic review that comprehensively identified, assessed and summarised the evidence regarding the association between vitamin D deficiency and the risk and prognosis of melanoma.
This systematic review was reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
In case of disagreements, a third independent researcher was consulted to reduce the risk of observer bias.
First, the exact data on the vitamin D intake and serum 25(OH)D levels of individuals were not available from all studies, which may lead to less accurate estimates of risk.
Second, the number of studies included was relatively small; therefore, some subgroup analyses were difficult to perform.
Third, the heterogeneity and deficiencies of the included studies limited the extraction of accurate and conclusive information for quantitative analysis in some cases.
Background
Cutaneous malignant melanoma is the most dangerous type of skin cancer and represents the most important cause of death from skin diseases, occurring in all age groups.1 The incidence of melanoma has been increasing, despite the efforts to improve sun protection; thus, there is a demand on additional preventive treatments or measures.
Vitamin D is a prohormone following conversion to calcitriol and exhibits a wide range of biological functions in the human body. In addition to bone and calcium metabolism disorders, many illnesses have been linked with vitamin D deficiency in recent epidemiological studies.2–4 As vitamin D is either synthesised in the skin or obtained from dietary sources, optimal sun exposure and dietary intake are related to optimal vitamin D status. However, vitamin D insufficiency remains as a global health problem, the major causes of which are insufficient exposure to sunlight, decreased dietary intake, skin pigmentation, obesity and advanced age. To overcome or avoid these causes, vitamin D supplementation has been considered to be the most convenient and effective means.
Some studies have suggested an inverse relationship between vitamin D levels and cancer risk, especially in the risks of breast, pancreatic, prostate and colon cancers.5–8 However, several studies have reported a null association or even an increase in cancer risk with higher vitamin D levels.
Vitamin D is a fat-soluble steroid hormone, which binds to the vitamin D receptor (VDR), thereby mediating its genetic effects. The relationship of serum levels with melanoma risk and mortality remains unclear. In vivo studies have found that vitamin D could inhibit the metastatic ability of lung cancer cells in animal models, and in vitro studies have showed that vitamin D could result in a decrease in cell proliferation and induce apoptosis in lung cancer cell lines. In fact, UV radiation is not among the main causes of non-sun-exposed melanomas; systemic immunosuppression and physiological features in these special sites may contribute to the development of the disease. Additionally, some studies have reported that higher serum levels of vitamin D are associated with a better prognosis in patients with melanoma.9
Vitamin D binds to the VDR, resulting in the transcription of many genes that play roles in the inhibition of MAPK signalling pathway, induction of apoptosis, and cell-cycle inhibition.10 Vitamin D also has suppressive effects on adaptive immunity and has been reported to promote innate immunity.11 Recently, several cohort studies have addressed the associations of vitamin D status with incidence and survival of patients with melanoma. However, the strength of the associations and their statistical significance varied among these studies. We therefore conducted a systematic review and meta-analysis to provide a comprehensive overview of the evidence on the potential protective role of high 25(OH)D level, the main form of vitamin D in the body, on the incidence and prognosis of melanoma.
Methods
This systematic review was reported following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines.12 13
Patient and public involvement
No patient involved.
Search
Two reviewers searched PubMed, Embase and ISI Web of Knowledge (Thomson Scientific Technical Support, New York) databases for eligible studies published between January 1992 and September 2020. The following search terms related to vitamin D and melanoma were combined for a main search: “vitamin D” OR “25-hydroxyvitamin D” AND “melanoma” OR “malignant melanoma” OR “cutaneous melanoma” OR “cutaneous malignant melanoma”. See online supplemental appendix A for the full search for all databases.
Supplemental material
Eligibility and exclusion criteria
Literature inclusion criteria: (1) cohort studies or case-control studies; (2) assessing the association between vitamin D intake and melanoma risk or serum vitamin D levels and melanoma risk, or serum vitamin D levels and melanoma tumour thickness; (3) the outcomes were melanoma incidence or tumour thickness. Exclusion criteria: (1) reviews, case-only studies, independent studies, case reports and editorials were all excluded. (2) The association between vitamin D intake and the risk of melanoma could not be calculated. (3) The results are repeatedly reported in the literature.
When several articles reported results from the same participants, only the study with the largest sample of subjects was considered. Regarding the effect of vitamin D on the prognosis of melanoma, we focused on tumour thickness only, as this is the most frequently reported and the most important prognostic factor in early-stage melanoma. Therefore, we also included studies reporting on the average vitamin D intake or blood level across categories of tumour thickness.
Procedures
All references were imported into the bibliographic management software Mendeley and duplicates were identified and removed. Two independent authors screened the remaining results by title and abstract. Two reviewers screened the full texts of the selected articles to identify those that satisfied the eligibility criteria. A third reviewer was consulted in case of any disagreements.
Data extraction and quality assessment
A standardised protocol for data collection was used for data extraction. For each study, we extracted information on the first author, publication year, country where the study was conducted, number of participants, sex distribution, study design, exact definition of dietary intake of vitamin D, serum vitamin D levels, cases of incident melanoma and risk estimates for melanoma risk. Two authors independently performed the quality of included studies and data collection, and any initial disagreements were checked by another author and resolved by consensus after a further review of the studies. Since melanoma is a relatively rare disease, we ignored the distinction between the various estimates of relative risk (ie, OR, risk ratio, rate ratio), and all measures were interpreted as relative risk.
We used the Newcastle–Ottawa Scale to evaluate the quality of the included studies. The evaluation criteria consisted of the following three parts: the selection method of the case and the control groups, the comparability of the case and the control groups, and the exposure assessment method. The semiquantitative principle of the star system was adopted to evaluate the literature quality, with a full score of 9 stars and a score of≥7 stars considered as high-quality studies; studies with a score of≤4 stars were not included.
Data synthesis and statistical analysis
All the statistical analyses were performed using the R software, V.R-3.5.1. (https://cran.r-project.org), and the library (metafor), library (meta), library (rmeta) packages were loaded for data collection and analysis. The pooled RRs and 95% CIs were calculated to assess the strength of the association between vitamin D intake (or serum vitamin D levels) and melanoma risk. Serum vitamin D concentrations are presented as in nmol/L. Concentrations reported in ng/mL were accordingly converted based on the following equivalence: 1 ng/mL=2.5 nmol/L. The summary RR with 95% CI was used to assess melanoma risk. The RR comparing high levels of vitamin D with low levels of vitamin D was used in this meta-analysis. Between-study heterogeneity was assessed using Cochrane’s Q test, and p<0.1 indicated obvious heterogeneity in the included studies. A further assessment of heterogeneity was performed using the I2 statistic method, and an I2<50% was acceptable of the variability level, I2>50% indicated that there was heterogeneity among the included studies Heterogeneity was also investigated by considering all the possible factors that could influence the estimates, including country, type of controls, adjustment for confounding factors, and study design. Random effect model was adopted to calculate the pooled RR when the heterogeneity was obvious; otherwise, a fixed effect model was used.
Sensitivity analysis was conducted by removing one study by turns to evaluate the reliability and validity of the pooled RRs. Publication bias was evaluated using the funnel plot, and asymmetry in the funnel plot indicated possible risk of publication bias. Egger’s test was also used to assess publication bias.
Results
Search results and characteristics of the included studies
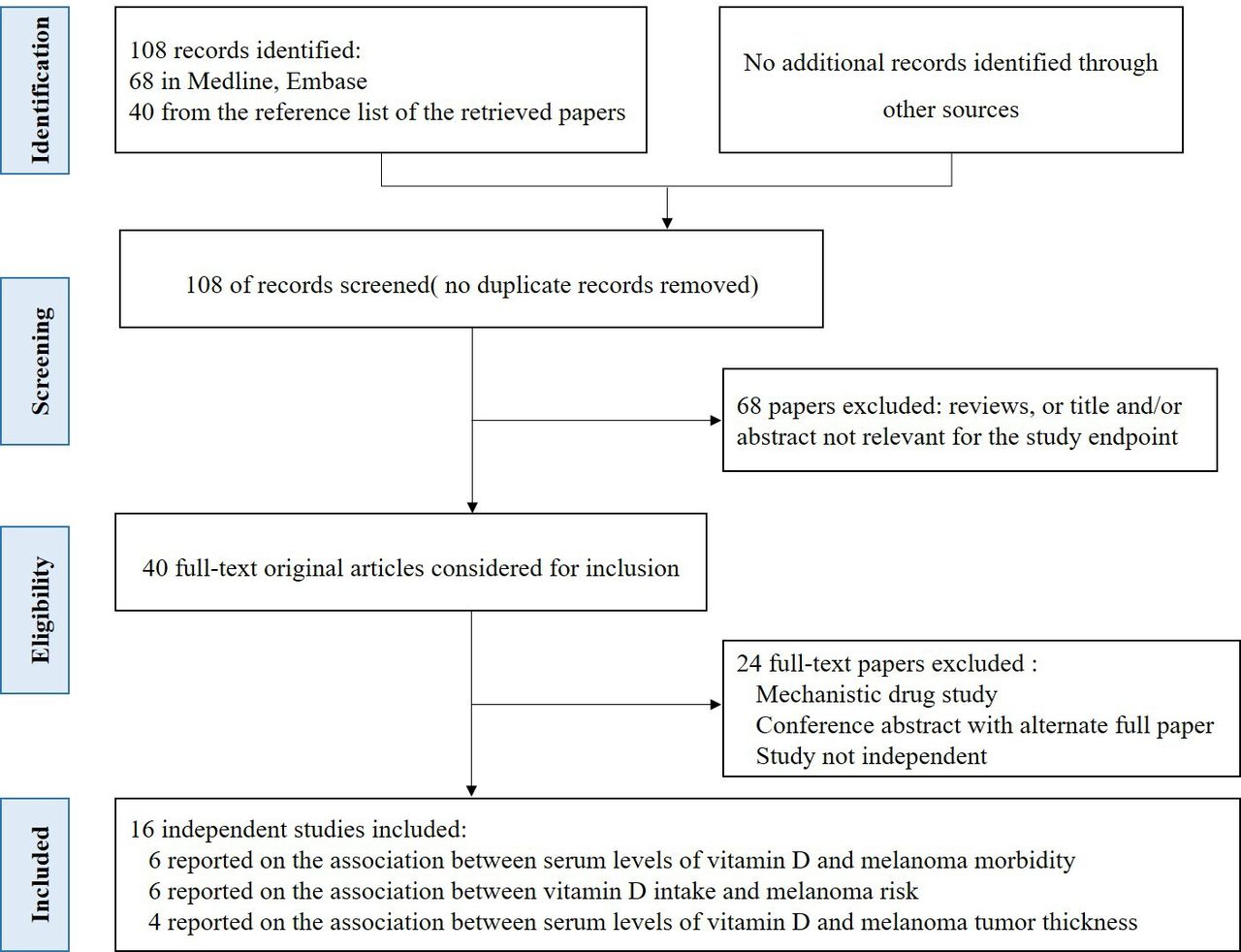
The flow diagram of the systematic literature search process and results are depicted in figure 1. A total of 108 abstracts of possible studies were identified from Medline, Embase and ISI Web of Knowledge up to September 2020. After an initial screening, 40 papers were preliminarily considered for inclusion, 24 studies were excluded based on the inclusion criteria. Among the 16 studies remaining, 3 were prospective cohort studies, 8 were case-control studies, 4 were retrospective studies and 1 was a randomised controlled trial. They were conducted in the US (n=5) and in European (n=7) and Asian (n=4) regions and published from 1992 to 2019. The main features of these studies are shown in table 1. All studies provided risk estimates of melanoma according to the levels of vitamin D. There were six studies that assessed the association between vitamin D intake and melanoma risk (table 1) and another six studies that assessed the association between serum vitamin D levels and melanoma risk (table 2).

Flow chart of the selection process of the studies included in the meta-analysis.
Main features of studies included in this meta-analysis on the association between dietary intake (from food and/or supplements) of 25(OH)D and melanoma risk
Main features of papers included in this meta-analysis on the association between serum vitamin D levels and melanoma risk
The Newcastle-Ottawa Scale mentioned above was adopted to evaluate the quality of the studies included. All studies had scores of≥7 and were thus considered to be high-quality studies. This demonstrates the rationality of the selection method and the comparability between the case and the control groups.
Meta-analysis
Table 1 shows the main features of the six included studies14–19 with 212 723 cases overall reporting on the association between dietary intake of 25(OH) D serum levels and melanoma risk. The total relative ratio for the comparison between the highest and lowest quantiles of the distribution of vitamin D intake was 1.10 (95% CI 0.96 to 1.26) with I2=56% (figure 2). As the number of studies was limited so we did not carry out subgroup analyses. Sensitivity analyses did not identify any significant factor influencing the summary results. The funnel plot showed that all the included studies were evenly distributed, with no study located out of the funnel (figure 3).

Forest plot comparing the risk of melanoma in the highest versus lowest categories of vitamin D intake (through diet and/or supplementation).
Begg’s funnel plot. The funnel plot was used to evaluate publication bias. All studies are within the limits determined by the graphic, indicating low bias.
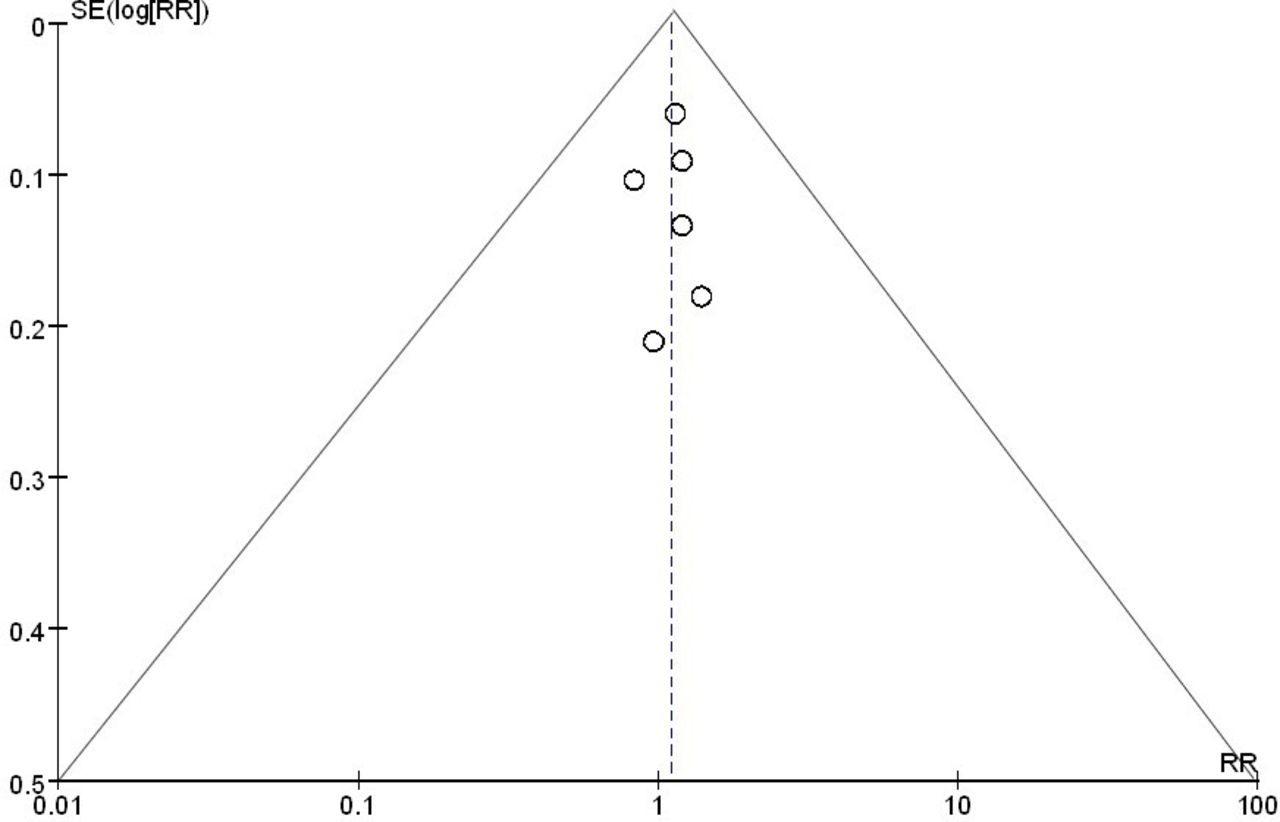
Table 2 shows the main characteristics of the other six studies20–25 with 12 297 cases overall reporting the association between serum vitamin D levels and melanoma risk. The total relative ratio for the comparison of serum vitamin D levels between the highest and lowest quantiles was 1.12 (95% CI 0.53 to 2.35) with I2=91% (figure 4). The funnel plot showed no publication bias in these studies (figure 5).
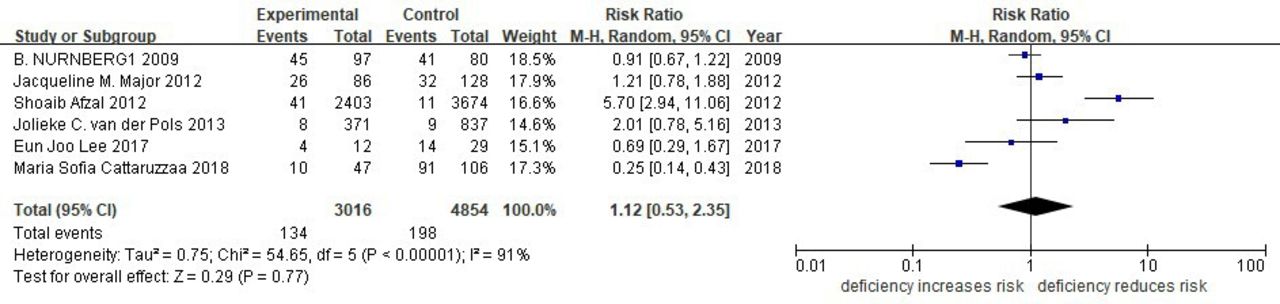
Forest plot comparing the risk of melanoma in the highest versus lowest categories of vitamin D serum levels.

The funnel plot was adopted to evaluate publication bias. All included studies are within the limits determined by the graphic, indicating no obvious bias.
Table 3 summarises descriptive statistics of four studies26–29 with 2105 cases overall reporting on the association between serum 25(OH) D (nmol/L) and Breslow thickness. All studies found an inverse association between serum 25(OH) D (nmol/L) and melanoma thickness. With the exclusion of the small study by Candy Wyatt,28 the inverse association in all the other studies was significant (figure 6).
Summary descriptive statistics of papers reporting on the association between serum 25(OH)D (nmol/L) and melanoma thickness

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Melanoma thickness is slightly negatively related with serum 25(OH)D levels.
Discussion
Serum 25(OH) D levels are positively correlated with the prognosis of patients with melanoma
This meta-analysis summarises the results of prospective and retrospective studies, including 6 studies on vitamin D intake comprising 211 230 patients and 1493 controls and 6 studies on serum 25(OH) D levels comprising 11 725 patients and 572 controls, 4 studies on serum 25(OH) D levels and melanoma thickness including 2105 patients with melanoma. Our results indicate that vitamin D intake and serum 25(OH) D levels are not strongly associated with melanoma risk; however, we found an inverse association between serum 25(OH)D levels and melanoma thickness, which was identified as a prognostic factor.
Vitamin D deficiency is an important risk factor for many types of solid cancers, such as colorectal cancer. The prevalence of vitamin D deficiency is higher in patients with colorectal cancer (approximately 90%) than in those of other types of cancer.30 Vitamin D may decrease the risk of cancer through several mechanisms, including the regulation of proliferation and differentiation, the induction of apoptosis, and the inhibition of angiogenesis.31
As melanoma is the most aggressive malignant disease among skin tumours, studies on the aetiological factors of melanoma have attracted much attention. The synthesis of vitamin D requires UV radiation, an important factor in melanoma incidence; thus, the relationship between vitamin D and melanoma seems more complex and significant. A few studies have provided information on vitamin intake and melanoma incidence; however, their conclusions remain controversial. Meta-analysis is an important tool to reveal trends that are not apparent in a single study. Pooling of similar but independent studies increases precision and therefore increases the confidence level of the findings.
Limitations of this meta-analysis directions for future research
This meta-analysis had some strengths. First, the number of total cases and controls included was substantial, thus significantly increasing the statistical power of the analysis. Second, our quantitative assessment was mainly based on prospective studies, thereby minimising selection or recall bias. Third, the publication biases were small, indicating that the entire pooled result may be unbiased.
Nevertheless, thus study had some limitations. First, the exact data of the vitamin D intake and serum 25(OH) D levels of individuals were not available from all studies, which may lead to less accurate estimates of risk. Second, the number of studies involved was relatively small; thus, some of the subgroup analyses were difficult to perform. Third, the controls were not uniformly defined. Although most participants in the control groups were healthy, some may have had benign disease. Therefore, there might be non-differential misclassification because the included control participants may have different risks of developing melanoma. Fourth, the range of values for the cut-off points for these categories for both the plasma 25(OH) D levels and the vitamin D intake in the studies was wide, thus affecting the analysis. Therefore, large randomised clinical trials should be conducted with uniform criteria for vitamin D intake and plasma 25(OH) D levels in several countries and regions. Finally, although there was no clear indication of major publication bias in the formal evaluation, potential publication bias is difficult to completely exclude because small studies with negative results may not be published.
In summary, the results of this meta-analysis demonstrated that vitamin D intake and serum 25(OH) D level were weakly associated with the risk of melanoma, but positively correlated with an improved prognosis of patients with melanoma. However, in-depth analyses of the assessed associations using longitudinal studies are required to enable more precise estimates of the role of vitamin D in melanoma; further investigations are needed to ulteriorly demonstrate the benefits and to suggest the implications of dietary vitamin D supplements, prospective studies with large samples are especially demanded to set up a clear and convictive guideline for vitamin D supplement.
Data availability statement
All data included in this study are available upon request by contact with the corresponding author.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
YS and HL contributed equally.
Correction notice This article has been corrected since it published online to update author contribution.
Contributors All authors contributed to the study design. YS and HL searched and screened the articles. All authors contributed to data analysis and interpretation of the data. YS drafted the manuscript, HL and YC revised it critically, and all authors contributed to revisions and approved the final manuscript. YS is responsible for the overall content as the guarantor.
Funding This study was funded by the National Natural Science Foundation of China (nos. 82102777) and the Joint Co-construction Project of Henan Medical Science and Technology Research Plan (nos. 2018020494 and LHGJ20210281), Funding Plan for Key Scientific Research Projects of Universities in Henan Province (nos. 22A320059) and Zhengzhou University Undergraduate Teaching Reform Project (nos. 2021ZZUJGLX197).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.