Article Text

Abstract
Objective Although several studies have assessed treatment outcomes of drug-susceptible tuberculosis (TB) in Ghana, very little has been done in the area of multidrug-resistant TB (MDR-TB). The aim of this study was to determine treatment outcomes and associated factors among patients treated for MDR-TB in the Ashanti Region, Ghana.
Design A retrospective, cross-sectional analysis.
Setting The study was conducted in the Ashanti Region, the second most populous region in Ghana. The regional MDR-TB register, which contains information on all patients with MDR-TB being treated at the various TB centres in the region, was analysed between February and May 2021.
Participants The participants consisted of all registered patients with MDR-TB who were placed on treatment between 1 January 2015 and 31 December 2020. Patients were included in the analysis if their treatment outcome had been assigned. Patients with no record of treatment outcome were excluded from the study.
Outcome measures The main outcome variable for the study was MDR-TB treatment outcome, standardised as ‘cured’, ‘treatment completed’, ‘treatment failure’, ‘died’ and ‘lost to follow-up’. A logistic regression model was fitted for factors associated with the outcome measure.
Results Out of 159 patients included in the analysis, 86 (54.1%) were declared cured, 28 (17.6%) completed their treatment successfully, 6 (3.8%) were declared treatment failure, 12 (7.5%) were lost to follow-up and 27 (17.0%) died. The overall treatment success rate was 71.7%. Patients who were female (adjusted OR (AOR)=1.27, 95% CI: 1.18 to 1.39, p=0.023), younger (AOR=0.53, 95% CI: 0.19 to 2.11, p=0.012), had a higher level of education (AOR=1.12, 95% CI: 0.65 to 1.90, p=0.034), had a baseline body mass index of 18.5 kg/m2 or above (AOR=1.57, 95% CI: 1.23 to 2.47, p=0.011) and those who did not have a history of TB (AOR=0.47, 95% CI: 0.10 to 0.75, p=0.028) were more likely to have successful MDR-TB treatment outcomes.
Conclusions Favourable treatment outcomes for patients with MDR-TB can be achieved in a resource-limited country. Although the recommended WHO target of ≥75% was not met, the current result (71.7% treatment success rate) is still commendable considering all the challenges associated with TB treatment in Ghana.
- Tuberculosis
- Public health
- Health & safety
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This study is among few to provide an important assessment of multidrug-resistant tuberculosis (MDR-TB) treatment outcome and its associated factors in Ghana.
The findings provide important baseline information for further broader studies in the country.
There may be underestimation and/or overestimation of some of the findings as the secondary data used were not recorded systematically for research purposes.
The nature of the secondary data analysed limited the inclusion of other potential factors that could be associated with successful MDR-TB treatment outcome.
Due to the small sample drawn from a specific geographical location in Ghana, the findings might have limited generalisability.
Introduction
Tuberculosis (TB) is 1 of the top 10 causes of morbidity and mortality worldwide, and the leading cause from a single infectious agent.1 The 2020 WHO Global Tuberculosis Report indicates that in 2019, 10 million people were infected with TB globally, out of which 1.4 million resulted in deaths. Geographically, most cases occurred in the WHO regions of South-East Asia (44%), Africa (24%) and the Western Pacific (18%), with smaller shares in the Eastern Mediterranean (8%), the Americas (3%) and Europe (3%).2
Although the global incidence of TB is falling at about 2% per year,1 the emergence of multidrug-resistant TB (MDR-TB) over the past few decades poses a public health crisis and a health security threat.2 3 Globally, 206 030 MDR-TB cases were recorded in 2019, an increase of 10% from 186 883 in 2018.2 MDR-TB is diagnosed when a patient’s sputum examination reveals resistance to at least isoniazid (INH) and rifampicin (RIF).4 Estimates from WHO indicate that over half a million new cases of RIF-resistant and MDR-TB are recorded annually.1 Four main factors are known to account for drug resistance: inappropriate use of anti-TB medications, incorrect prescription of drugs by care providers, poor quality drugs and patient stopping treatment prematurely.4
MDR-TB is curable and treatment requires the administration of second-line anti-TB drugs for a minimum of 9 months and a maximum of 20 months.3 However, compared with drug-susceptible TB cases, treatment outcomes of MDR-TB cases are poorer. Globally, only 57% of patients with MDR-TB were successfully treated in 2019.2 The management of MDR-TB is complex as it puts a greater strain on countries and national health systems.2 5 6 For example, culture-based methods can take weeks to months. They are also expensive and require sophisticated and well-established laboratory infrastructure, qualified and competent staff and strict quality and infection control systems.6
The global health aim of eliminating TB by 2035 will only be possible if drug-resistant strains of Mycobacterium tuberculosis (MTB) are effectively managed by countries.6 Ghana is not ranked among the world’s high-burden TB countries. Incidence of TB has fallen gradually from 214 cases per 100 000 people in 2001 to 143 cases per 100 000 people in 2020.7 Nonetheless, studies have reported the emergence of MDR-TB in the country.7–12 For instance, Davies-Teye et al reported a cumulative incidence of MDR-TB in the Greater Accra Region of 1.4/100 000 population, with a case fatality rate of 14%.8 In a recent nationwide drug resistance survey to investigate the level and pattern of resistance to first-line TB drugs among newly and previously treated sputum smear-positive TB cases, Sylverken et al found that resistance to INH and RIF, the two most effective anti-TB drugs, was 3.2%.7
High-quality disease management is one of the key strategies in improving treatment outcomes of TB.13 In Ghana, both susceptible TB and MDR-TB are managed under directly observed treatment short course (DOTS) programme, which has demonstrated feasible and effective treatment in other resource-limited countries.14 Gaining insight into treatment outcome of MDR-TB and its associated factors could assist national TB control programmes in improving the treatment success rate of patients with MDR-TB. Nonetheless, literature on factors influencing treatment outcomes of MDR-TB in Ghana is limited. Moreover, studies conducted in other countries have revealed a wide variation in predictors of MDR-TB treatment outcomes. Some of the factors that have been found to be associated with successful or unsuccessful MDR-TB treatment outcome include patient age,15 gender,16 pretreatment body mass index (BMI)17 and body weight, drug adherence,18 positive smear at the start of treatment, history of TB,19 smoking,16 alcohol consumption,20 and comorbidities or underlining health conditions such as HIV21 and diabetes.22 However, other studies15 21 23 have reported findings contrary to the above-mentioned factors. For instance, Elliott et al found no association between MDR-TB treatment outcome and positive smear at the start of treatment and HIV coinfection.18 Also, Khan et al reported that MDR-TB treatment outcome was not significantly associated with gender, smoking and comorbidity status.15
Therefore, this study was conducted to determine treatment outcomes and associated factors among patients with TB treated for MDR-TB in the Ashanti Region, Ghana. Understanding the factors that could determine successful treatment outcome would be useful in developing strategies and making informed decisions about MDR-TB management in the region. This would help promote efficient and effective MDR-TB treatment in the country.
Methods
Study setting
The Ashanti Region is the second most populous region in Ghana, with a population of 5 432 485.24 It has a population density of 192.4 per km2. The region has 43 districts and 132 subdistricts. There are 527 health facilities in the region. The Ghana Health Service operates about 33% of all health facilities in the region. Kumasi, the regional capital, has the highest number of health facilities (29%) with Ejura-Sekyedumase having the least (2%).24
Study design, population and sample
A retrospective, cross-sectional analysis of the Ashanti regional MDR-TB register was conducted between February and May 2021. The regional MDR-TB register is a standard register containing information on all patients with MDR-TB being treated at the various DOT centres in the region. The study population consisted of all registered patients with MDR-TB who were placed on treatment between 1 January 2015 (when MDR-TB treatment started in the region) and 31 December 2020. Patients were included in the analysis if their treatment outcome had been assigned. Patients with no record of treatment outcome were excluded from the study.
Drug susceptibility testing and treatment protocol
Drug-resistant TB suspects are initially evaluated for both MTB and RIF resistance by direct sputum smear microscopy using Ziehl-Neelsen strain and Xpert MTB/RIF (Cepheid, California, USA). Sputum samples of patients with positive results are sent to the national TB reference laboratory located at the Kumasi Center for Collaborative Research in Tropical Medicine for sputum culture and phenotypic drug susceptibility test for RIF, INH, streptomycin, ethambutol and pyrazinamide (PZA).
All patients with positive diagnosis of MDR-TB are placed on a clinic-based model of treatment and care25 at the various DOT centres in the Ashanti Region. This is a form of ambulatory care, where patients travel to the treatment centres daily for directly observed therapy. Although the current treatment of patients with MDR-TB in the region is based on both the shorter and the longer treatment regimens, patients considered in this study were treated with the standardised, longer treatment regimen consisting of an 8-month initial or intensive phase with a combination of capreomycin/kanamycin, levofloxacin, prothionamide, PZA, cycloserine and vitamin B denk/pyridoxine; and a-12 month continuation phase with a combination of levofloxacin, PZA, prothionamide and vitamin B denk.
Study variables
The main outcome variable for the study was MDR-TB treatment outcome. This was standardised, as recommended by WHO, as ‘cured’, ‘treatment completed’, ‘treatment failure’, ‘died’ and ‘lost to follow-up’.25 According to the WHO guidelines for the management of drug-resistance TB, a treatment outcome is classified cured when the treatment is completed with no evidence of failure and three or more consecutive sputum cultures taken at least 30 days apart are negative after the intensive phase. A patient is declared treatment completed when he/she completes his/her treatment with no evidence of failure, but there is no record indicating that three or more consecutive cultures taken at least 30 days apart are negative after the intensive phase. Treatment failure is when treatment is terminated due to poor clinical or radiological response or adverse drug reaction. Treatment outcome ‘died’ is when a patient dies for any reason during the course of treatment. Finally, a patient whose treatment is interrupted for 2 consecutive months is declared lost to follow-up.25 26
The explanatory variables included were: age, gender, educational level, marital status, treatment regimen (new vs retreatment), baseline BMI, baseline weight, HIV status, cavitation on baseline chest X-ray and having comorbidities other than HIV. These variables were selected based on previous studies (as indicated in the introductory section of the paper) and the availability of data.
Data collection
A designed data extraction tool, reflecting the various variables under study, was used to gather data from the Ashanti regional MDR-TB register. Data extraction was done by two members of the research team and assisted by four trained data collectors, comprising two public health nurses and two health information officers. Missing information in the register was completed with data from the patients’ clinical records. All of the extracted information was audited and verified to check for completeness and quality.
Statistical analysis
Data collected were coded, entered and analysed using SPSS software V.20 (IBM Corporation). Categorical data were presented as frequencies and percentages, while continuous data were presented in the form of mean and SD. The main outcome variable, MDR-TB treatment outcome, was categorised into successful (cured and completed) and unsuccessful (treatment failure, died and lost to follow-up) treatment outcomes, and scored as follows: successful treatment=1, unsuccessful treatment=0. The continuous variables were also dichotomised as follows: age into <50 and ≥50 years, BMI into <18.5 and ≥18.5 kg/m2, and body weight into <50 and ≥50 kg.
Bivariate analysis was performed for all of the independent variables with the outcome variable. Using variables with p value of <0.2, based on the bivariate analysis, a multiple logistic regression analysis was carried out to determine the independent predictors of successful MDR-TB treatment outcome. Variables with significant associations with successful MDR-TB treatment outcome were identified based on the OR with a 95% CI and p values of ≤0.05. We evaluated the predictive accuracy of the model using receiver operating characteristic (ROC) curve analysis. The area under the ROC curve was 0.93, indicating the model classified much of the data correctly.27 Also, by computing the deviance R2, we observed that the model explained 89.17% of the total deviance in the outcome variable. This indicates further that the model provides a good fit to the data.
Patient and public involvement
There was no patient or public involvement in the study.
Results
In total, records of 159 patients with MDR-TB were reviewed. Table 1 summarises the demographic characteristics of the study participants. The mean age of the patients was 43.69±14.86 years. The majority were male (111, 69.8%), between the age group of 40 and 49 years (46, 28.9%), having educational qualification below high school (121, 76.1%) and not married (8, 53.4%). There has been a steady increase in the number of patients placed on treatment in the region since 2015 (figure 1).
Sociodemographic characteristics of the patients with MDR-TB (N=129)

Trend in patients with MDR-TB placed on treatment from 2015 to 2020 in Ashanti Region, Ghana. MDR-TB, multidrug-resistant tuberculosis.
Clinical characteristics
Table 2 summarises the clinical characteristics of the patients with MDR-TB included in the study. The majority (69%) of the patients had a baseline body weight ≥50 kg. Also, more than half (59.1%) had a baseline BMI ≥18.5 kg/m2. About 16% had a history of comorbidities such as diabetes and hypertension, and 90% had no history of HIV coinfection. Regarding treatment regimen, 33.6% were new patients, whereas 66.4% had a history of TB treatment.
Clinical characteristics of the patients with MDR-TB (N=159)
Treatment outcomes
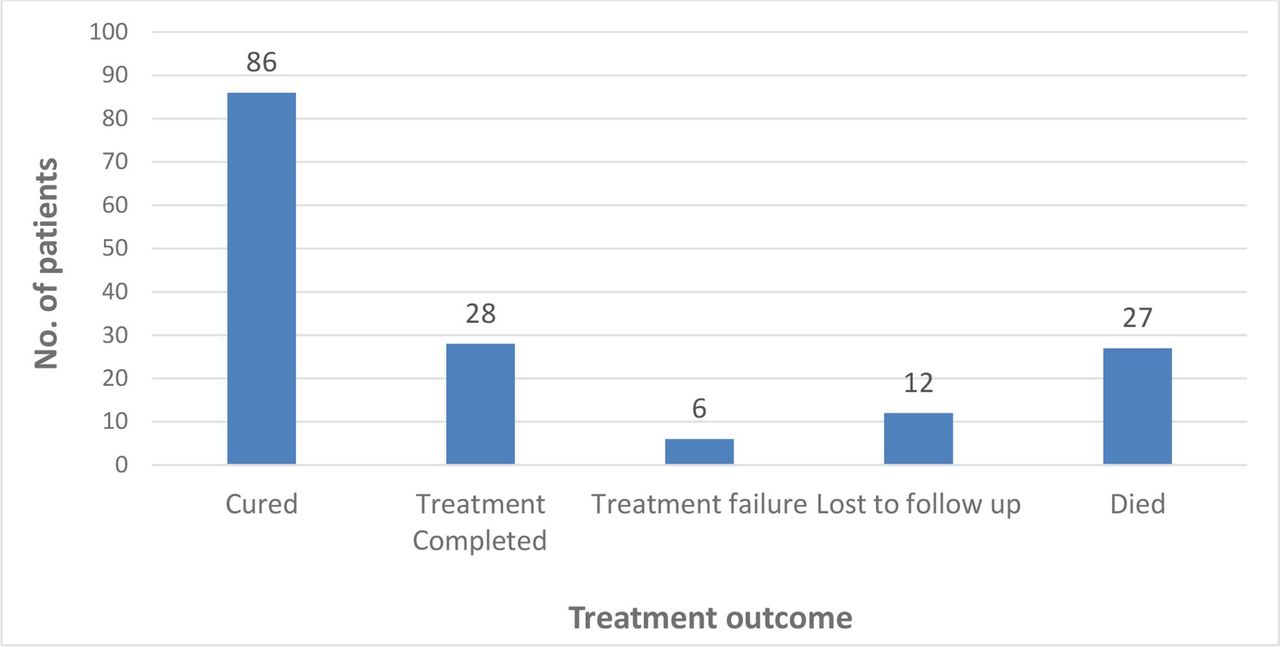
Of the 159 patients included in the analysis, 86 (54.1%) were declared cured, 28 (17.6%) completed their treatment successfully, 6 (3.8%) were declared treatment failure, 12 (7.5%) were lost to follow-up, while 27 (17.0%) died (figure 2). The overall treatment success rate for the period under study (2015–2020) was 71.7%.
{kind=link}
{kind=link}
Treatment outcomes of the patients with MDR-TB (N=159). MDR-TB, multidrug-resistant tuberculosis.
Factors associated with MDR-TB treatment outcome
In the bivariate analysis, the covariates with p values less than 0.2 level of significance for successful MDR-TB treatment outcome were gender, age, educational level, baseline BMI, baseline weight, comorbidity status, HIV status and treatment regimen (table 3).
Bivariate analysis of factors associated with successful treatment outcome among patients treated for MDR-TB in Ashanti Region, 2015–2020
Results of the binary logistic regression analysis showed that the odds of having a successful MDR-TB treatment outcome were independently associated with gender, age, level of education, baseline BMI and treatment regimen (table 4). Adjusting for the relationships of the other independent variables, we observed that the likelihood of having a successful MDR-TB treatment outcome among female patients was 1.3 times (adjusted OR (AOR)=1.27, 95% CI: 1.18 to 1.39) higher compared with male patients. Also, patients who were 50 years and above were less likely (AOR=0.53, 95% CI: 0.19 to 2.11), compared with those below 50 years, to have a successful MDR-TB treatment outcome. Furthermore, patients whose educational level was high school or above were 1.1 times (AOR=1.12, 95% CI: 0.65 to 1.90) more likely, compared with those below high school, to have a successful MDR-TB treatment outcome. Moreover, patients with baseline BMI ≥18.5 kg/m2 had higher odds (AOR=1.57, 95% CI: 0.13 to 2.17) of having a successful MDR-TB treatment outcome, compared with those having BMI <18.5 kg/m2. Finally, compared with new patients, patients with a history of TB were less likely (AOR=0.47, 95% CI: 0.10 to 0.75) to have a successful MDR-TB treatment outcome.
Independent predictors of successful treatment outcome among patients treated for MDR-TB in Ashanti Region, 2015–2020 (N=159)
Discussion
Summary of findings
Our study showed that more than two-thirds (N=114, 71.7%) of the patients had successful MDR-TB treatment outcome, while 28.3% had unfavourable treatment outcome. Cure rate was 54.1%, whereas mortality rate was 17.0%. A logistic regression model was fitted for eight variables, out of which five were independently associated with successful MDR-TB treatment outcome. Patients who were female, younger (less than 50 years), having higher level of education, having a baseline BMI of 18.5 kg/m2 and above, and not having a history of TB were more likely to have successful MDR-TB treatment outcome. Marital status, baseline weight, HIV status and having comorbidity other than HIV had no significant association with MDR-TB treatment outcome.
Strengths and limitations
To the best of our knowledge, the present study, if not the first, is among the few to provide an important assessment of MDR-TB treatment outcome and its associated factors in Ghana. The findings provide baseline information for further broader studies in the country. Nonetheless, the study is not without limitations. First, being a retrospective analysis, findings were based on secondary data obtained from patients’ medical records and registers. Since these records are not intended for research, they are not recorded systematically. This may have led to underestimation and/or overestimation of some of our findings. Second, the nature of the secondary data we used permitted us to review only records available in the regional MDR-TB register and the patients’ medical records. This did not allow us to include in the analysis other potential factors, such as smoking history, alcohol use, drug resistance status, time to culture conversion, income level and place of residence that could be associated with successful MDR-TB treatment outcome. Third, and most importantly, due to the small sample size drawn from a specific geographical location in Ghana, the study findings might have limited generalisability. That notwithstanding, the sample size used satisfies the general rule of thumb for the number of participants required to examine associations.28 The rule has been that for regression equations using six or more predictors, a minimum of 10 participants per predictor is required.28 Going by this, and with 10 predictors used in the study, a minimum of 100 participants would have been sufficient to examine the associations. Also, compared with normal TB cases, patient population with MDR-TB in the country is not very large. For instance, Svlverken et al’s recent nationwide survey found only 19 (3.2%) out of 927 patients with TB to be multidrug resistant.7 Thus, a sample of 159 is adequate to make a generalisation about the population with MDR-TB, particularly in the study area. Furthermore, except for patients whose treatment outcomes had not been confirmed at the time of the study, all of the registered patients with MDR-TB in the region for the study period (2015–2020) were included in the analysis. This approach implied the sample was more likely to be representative of the population.
Comparison with existing literature
The overall treatment success rate achieved in this study is lower than the 75%–90% target recommended by WHO4 and values reported from Northwest Ethiopia (80%)29 and Taiwan (82.8%),30 but higher compared with similar other studies, including 59% reported in a meta-analysis31 and 53.4% (44.55 cured and 8.9% treatment complete) found in a multicentric observational cohort analysis.32 Also, the 54.1% cure rate found in this study is lower compared with 62.7% reported in Tanzania,33 and 69.4%,34 76.9%35 and 83.7%36 all reported in Pakistan. These observed differences could, however, be a result of differences in sample size, study setting and study period.
Consistent with the global epidemiology of male predominance in TB cases,37 the majority of the patients in the current study were male (69.8%). However, compared with their male counterparts, more women had a higher treatment success rate (81.1%). The plausible reason for this observation could be attributed to women being more likely than men to adhere to treatment regimens, thus resulting in better health outcomes.38
We observed that as the age of the patients increased, the likelihood of having successful MDR-TB treatment outcome decreased (AOR=0.53, 95% CI: 0.19 to 2.11). This observation concurs with the literature that older age is a risk factor for unsuccessful MDR-TB treatment outcome.39 40 Generally, owing to factors such as physical deterioration, comorbidities with complicated medication schedules, malnutrition and compromised immunity, older age patients respond poorly to anti-TB treatment.41
Individuals’ level of education constitutes a unique dimension of social status and a key determining factor of health-seeking behaviour.42 Higher educational levels are noted to be associated with desirable treatment outcomes of TB.43 This assertion has been confirmed in the present study where we observed that the likelihood of having a successful MDR-TB treatment outcome was higher (AOR=1.12, 95% CI: 0.65 to 1.90) among patients with higher levels of education. Higher educational attainment creates desirable health outcomes because it reduces ignorance and increases knowledge, regarding medication management and consequences.43
Earlier studies have revealed that MDR-TB treatment failure and death are associated with low BMI.19 33 44 Our study generally supports this finding as we found that patients who started MDR-TB treatment at a BMI below 18.5 kg/m2 had decreased chances of a favourable outcome. Although baseline body weight was not significantly associated with MDR-TB treatment outcome in this study, it was close to significance (p=0.068). Underweight has been shown to be an independent predictor of poor outcome for patients treated for MDR-TB.45
Comorbidity and HIV status were not significantly associated with MDR-TB treatment outcome in this study. Nonetheless, it is acknowledged that conditions such as diabetes, hypertension and HIV positive status place patients at greater risk of poor treatment outcome.46 For instance, Ndwandwe et al reported that patients coinfected with HIV were twice as likely to interrupt TB treatment and, thus, had poor outcomes.46
The current study demonstrated that most of the newly diagnosed patients had higher successful treatment rates (86%) and that patients with a history of TB were less likely (AOR=0.47, 95% CI: 0.10 to 0.75) to have successful MDR-TB treatment outcome. This finding is consistent with the literature that re-treated patients are at higher risks of poor outcomes than newly diagnosed patients.23 47
Implications for policy and practice
The successful treatment outcome reported in this study demonstrates the success and promising performance of MDR-TB control which has been achieved through increasing awareness of TB over time and stability of service provision by treatment facilities. In addition, the result is an indication of the effectiveness of the various strategies that have been adopted to promote MDR-TB treatment in the region. These include: regular visits of patients by health professionals, assigning treatment supports from patients’ family to assist with directly observed therapy and supporting patients with food and money. There is therefore the need to sustain and improve these strategies to promote more efficient and effective MDR-TB treatment in the region and the country as a whole to catapult the global target of ending the TB epidemic by 2030 through high-quality disease management.
The rate of successful treatment outcome of MDR-TB in the region could be improved further by paying attention to the risk factors of poor outcomes identified in this study. While some of the factors are not modifiable, especially in the short term, policymakers and clinicians could influence the potentially modifiable ones to improve the management of MDR-TB cases in the region. For instance, nutritional counselling to increase energy intake and provision of nutritional supplements should be considered in patients having a baseline BMI below 18.5 kg/m2 and those with low body weight. Also, to prevent situations of treated people being diagnosed again with TB, there is the need to intensify health education, as well as addressing issues of relapse, treatment failure and loss to follow-ups during first-line treatment. The use of mobile health to remind patients with TB about their treatment and to ensure follow-up could also help in reducing the number of patients stopping treatment prematurely. In the long term, formal education should be encouraged to improve the educational levels of the citizenry so they could read well to appreciate the risk factors associated with MDR-TB.
Conclusions
MDR-TB continues to pose a great threat to the elimination of TB due to the increasing incidence and mortality rate recorded each year worldwide. The main objective of this study was to determine treatment outcomes of MDR-TB and associated factors among patients with TB in the Ashanti Region, Ghana. The findings have demonstrated that favourable treatment outcomes for patients with MDR-TB could be achieved in a resource-limited country. Although the recommended WHO target was not met, the current result (71.7% treatment success rate) is still commendable considering all the challenges associated with TB treatment in Ghana. The study has provided useful information that could inform policy decisions on strategies to improve MDR-TB management in the Ashanti Region and the country as a whole. Although several studies have assessed treatment outcomes of drug-susceptible TB in Ghana, very little has been done in the aspect of MDR-TB. We, therefore, recommend further studies in this area to bridge the dearth of information on MDR-TB treatment outcome and its associated factors in the country.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
The study was approved by the Ethics Review Committee of the Ghana Health Service Research and Development Division, Accra (Protocol No. GHS-ERC-052/04/21). In addition, approval was obtained from the Ashanti Regional Health Directorate (ARHD) to use data from the regional MDR-TB treatment register for the study. Data retrieved were not linked to individual patients.
Acknowledgments
We are grateful to the Ashanti Regional Health Directorate for granting us permission to use data from the regional MDR-TB treatment register for this study.
References
Footnotes
Contributors All authors contributed to conceptualising the study. Literature search for background information was done by VP and EK. VP, EK, POA and MAB wrote the first draft of the paper. CK, AF, SEA, PA-B and SKA provided critical review of the manuscript. All the authors read and approved the final version of the paper. EK is the guarantor for this work.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.