Article Text

Abstract
Objective To explore patient perceptions regarding doctors’ information seeking during consultations.
Design and setting Qualitative interviews with participants from six general practice waiting rooms in South East Queensland, Australia. Participants were asked about their experiences and opinions, and to comment on short videos of simulated consultations in which a doctor sought information. The interviews were analysed through a process of iterative thematic analysis using the framework of Braun and Clarke.
Participants The 16 participants were purposively sampled including 5 men and 11 women from a diverse range of educational and age groups.
Results How a doctor’s need to look up information impacted patient impressions of competence and trust was an overarching theme. The four dominant themes include: the trust a patient has in the doctor before the consultation, whether the doctor is expected to know the answer to a question without searching, has the doctor added value to the consultation by searching and the consultation skills used in the process.
Conclusions Patient trust is fundamental to positive perceptions of general practitioners’ information seeking at the point-of-care. Communication is key to building this trust. Understanding the patient’s agenda, listening, assessing thoroughly and being honest and transparent about the need to seek information all contribute to a positive experience.
- information management
- primary care
- world Wide Web technology
Data availability statement
No data are available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This is the first qualitative study to explore patient perceptions of doctors’ information seeking at the point-of-care.
Thematic saturation was achieved within the broad sample of age groups, educational levels and socioeconomic locations.
The use of simulated consultation videos as vignettes to provoke opinions.
The possibility of unequal power dynamics influencing the data. The participants may have felt that they could not express negative views during an interview with a practicing doctor.
Differences may exist between gender group however as this was an exploratory study we did not seek to differentiate between men and women.
Introduction
As the pace of new medical knowledge increases rapidly, doctors need to access information to remain up-to-date and provide best medical care. A doctor practicing in 1950 would have seen a doubling of medical knowledge every 50 years. In 2020 this rate has increased to 73 days.1 On average a general practitioner (GP) will encounter 0.57 clinical questions they need to look up per patient visit.2 In Australian primary care this equates to 58 clinical questions per week.3
Primary care doctors need to access information during the consultation due to time constraints and the fact that most care is provided with the patient, doctor and information source in the same space. Previous studies have found that use of online clinical evidence resources improves the accuracy of answers to clinical questions, doctors’ confidence in decision-making and possibly outcomes.4–10
Despite the benefits of answering clinical questions at the point-of-care, concerns remain about this practice. Anecdotally, patients have reported dissatisfaction with their doctor using online search engines to assist in medical decision-making. Furthermore, previous studies have shown that doctors feel that accessing clinical resources at the point-of-care may negatively impact on patient confidence and the perceived quality of care they are providing.10–12
Few studies have explored patient perspectives of their doctor accessing clinical resources during consultations. Kahane et al compared the perceptions of family physicians (FP) with those of their patients and found that the FPs overestimated the decrease in patients’ confidence caused by seeing them look up information. While most patients responded positively, a substantial proportion of younger patients reported decreased confidence.11
Another study asked patients about their perceptions of their GP using digital technologies to access information during consultations and found that computerised platforms can have a deleterious effect on the patient’s perception of the doctor’s competence and their interpersonal skills.13
Our study aims to provide an insight into what patients think of their doctor when it comes to accessing information and highlight areas that may strengthen or jeopardise the therapeutic relationship.
Methods
The participants of this qualitative study were patients recruited from general practice clinical waiting rooms across South Eastern Queensland, Australia. Individual emails were sent to the 128 practices affiliated with the University of Queensland Practice-Based Research Network, as well as four additional practices affiliated with the university. Interested clinics were asked to respond to the email advertising the project.
Patients were recruited through three principal methods. The first was displaying a poster advertising the project in the waiting room of clinics with a request for interested parties to contact the researcher via email, text message or phone call to arrange an interview. The second method involved the patient’s treating physician referring the patient to the researcher after their appointment to discuss participation. The final method involved the researcher or research assistant approaching patients before or after their appointment with a short explanation of the project and request for participation. Sampling was purposive to ensure maximum variation of age, education level, cultural diversity, socioeconomic status and geographical location. Sampling continued until thematic saturation was achieved. Each participant was offered a $A50 gift card for their time.
The data were collected between August and September 2021 via a short paper-based questionnaire followed by a semi-structured interview conducted either face-to-face (at the clinic or public library) or via online video conference. The interviews were audio recorded and subsequently transcribed verbatim.
The initial question schedule was broad and aimed to explore participants’ general opinions of and experiences with doctors accessing point-of-care information. The participants were also asked to comment on short (2 min) videos of simulated consultations in which a doctor accessed digital information. These video vignettes were filmed using a practicing a GP and an actor and edited by the first author. Data analysis was conducted concurrently with data collection allowing constant comparison of the interview transcripts. The interview schedule was iteratively revised to explore emerging themes. The questionnaire collected demographic data (age, gender, education), interaction with treating physician (usual doctor, frequency of visit) and technology usage (use of search engines, access of health-related information online).
All interviews were conducted by the first author who is a practicing GP. Although all participants were unknown to the interviewer, they were aware that the interviewer was a doctor. The possibility of unequal power dynamics during the interviews were explicitly acknowledged and considered throughout data collection and analysis.
The theoretical approach to data analysis was pragmatic thematic analysis as described by Braun and Clarke.14 Initial coding was conducted using NVivo V.12 software with later analysis managed using Microsoft Word. The initial coding was performed by the three investigators (IT, MLvD and BM) independently followed by in-depth group discussion. Prominent themes were generated through consensus.
Patient and public involvement
Patients or the public were not involved in the design, implementation or reporting of our research. We plan to disseminate the results of this research to the practices that participated.
Results
A total of 16 interviews were conducted. See table 1 for demographic, medical service and technology use information.
Demographics, medical service and technology usage
Participants were recruited from six practices; these included three clinics in middle-to-higher-income areas, two university health centres and one free of charge clinic in a lower socioeconomic and culturally diverse area. All six of these practices were associated with University of Queensland Practice-Based Research Network.
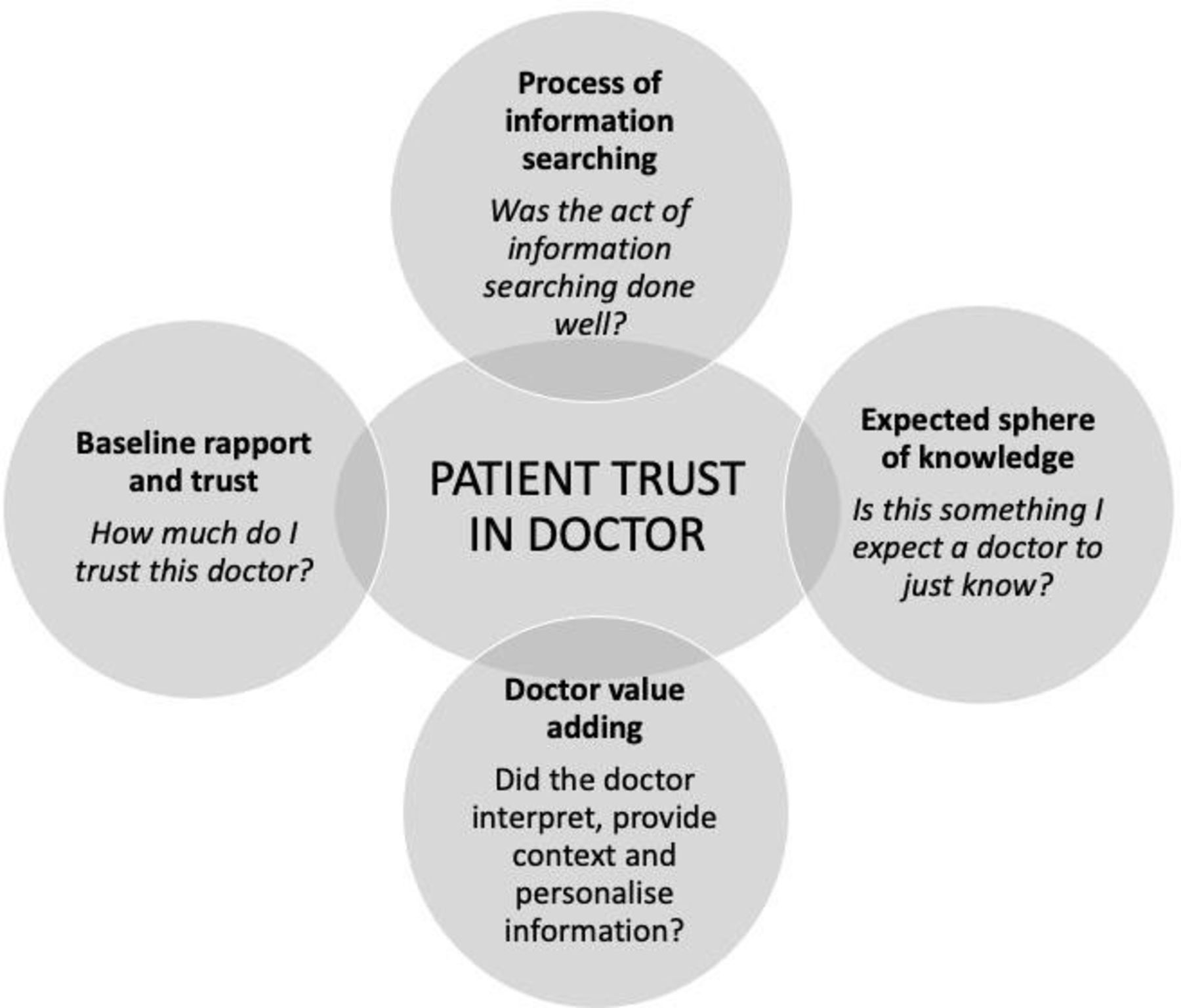
One overarching theme permeated the data: How a doctor’s need to look up information impacts on impressions of competence and trust in the advice that is given. The four themes presented here all relate to how accessing point-of-care information impacts on patients’ trust in their doctor. Our interpretation of the interaction of the four themes is presented in a graphical model (figure 1).
{kind=link}
Impact of accessing information at the point-of-care on patients’ trust in the doctor.
Theme 1: baseline trust
The patient’s trust in their doctor prior to entering the consultation influenced their views of their doctor’s need to access information. If a patient had strong trust, the impact was thought to be minimal. Conversely, if the patient had limited trust, accessing any kind of information may have a large impact on the confidence a patient has in the doctor’s competence. Four key factors emerged that influence the level of this ‘baseline trust’: the emotional state of the patient, the rapport a patient has with their doctor, a sense of cultural safety and a general trust in medicine.
Emotional state
Participants who identified having some anxiety regarding their health felt that doctors’ information seeking impacted their confidence.
If [the doctor searched] something I was particularly concerned or worried about I might consider getting a second opinion from another doctor just to be sure. I get a bit anxious about things sometimes. (Interview 1)
Other participants identified that entering a consult with a feeling of vulnerability also influenced their perception of the doctor’s competence should they need to seek information.
Rapport
Strong rapport with the doctor allays any doubts that might arise from accessing information at the point-of-care. Looking up information is to some degree always seen as poor practice from the patient’s point of view; however, a strong therapeutic relationship can allow the doctor to navigate the consultation without degrading trust.
The rapport I have with her outweighs any of those doubts and I can feel her care and concern for me. So, regardless of her competence, I do trust her and go back to her and I’m not going to be looking for another GP unless there’s some instance where it’s preposterously incompetent. But that, of course, hasn’t happened. So yeah, I feel like I can overlook that. (Interview 6)
Cultural safety
Participants from different cultural backgrounds reported trusting Australian doctors to be more challenging than doctors from their home country. These participants reported higher expectations of the doctor’s knowledge and lower tolerance for the doctors need to access information.
Trust in medicine
Participants who displayed high general trust in medicine felt that doctors are generally trying to do their best for their patients. They felt that information available at the point-of-care was part of the tool kit of a modern doctor and thus acceptable practice.
Well, I know they’re not perfect, and I know that they try their best to get the right information. (Interview 13)
Theme 2: doctors’ sphere of knowledge
In general participants preferred doctors just to know everything regarding healthcare without having to search. Some participants felt their doctor should essentially be all-knowing while others felt a doctor could not know everything. There was an overarching expectation that doctors have a foundational knowledge or approach to medicine and searching for questions that were perceived to be within this domain impacted on trust.
I’d hope and expect a GP to have a decent idea, or a few good guesses. Somewhere to start with, rather than what I would see as jumping straight onto the search engine and saying, tell me what I should diagnose him with, Internet? (Interview 1)
Several factors influenced the expectations of a doctor’s knowledge. First, the doctors age or perceived experience; older doctors were expected to have greater knowledge and experience compared with younger doctors and hence have less need to access information.
I’d be more concerned if it was an older doctor doing that… You’ve been around for a while. Do you keep on top of your knowledge base? Maybe a little bit more forgiving if it was a trainee doctor or something. (Interview 1)
A second component was the practice environment. Doctors were expected to have knowledge applicable to their specific environment, for example, university healthcare and rural settings.
This doctor would be familiar with the sort of stuff that would commonly crop up in the population. [For example] if I went to the Uni Health Centre, and the doctor I saw didn’t know how to treat me for stress, or for other common issues for 18- to 30-year-olds. I’d be wondering if they were new, at the very least. (Interview 1)
Generally, participants don’t know what the specific question the doctor is searching for but did speculate as to acceptable and unacceptable situations. Patients felt that a doctor looking up perceived common conditions or basic knowledge impacted their trust in the doctor’s advice as this was seen as similar to searching online themselves.
If it was something easy … I’d be like, okay, why do you have to look that up; you should know this, you’re a doctor. (Interview 16)
Searching common conditions also worried some patients.
If you go in for something simple, like a headache or muscle pain and they started looking it up. You might feel a bit worried that it might be more serious than that. (Interview 4)
Conversely, patients felt less worried about doctors searching for information that was perceived to be rapidly changing or novel. Cutting edge procedures, recently published research or new medications along with travel and COVID-19 advice were all acceptable situations.
Theme 3: doctors should add value
The general expectation is that doctors’ skills are superior to a layperson’s in searching for and interpreting medical information. Patients also expect doctors to have access to higher quality information sources than publicly accessible. In consultations where a doctor is able to effectively add value, patients feel empowered to make informed decisions about their own healthcare.
Superior searching skills
Participants felt that a trained doctor would be able to add value in their consultations through an ability to search reputable sources in an efficient and effective way.
I wouldn’t think that a layperson like me would get the information that a doctor would. Because he [would] probably have further avenues to investigate which I wouldn’t have access to, or at least not know about. (Interview 11)
Younger participants particularly felt that using the Google search engine was poor practice as this is available to everyone and not considered a sophisticated or appropriate way to access medical information.
Superior interpretation
When a doctor accesses information at the point-of-care, patients expect an individualised interpretation and explanation.
I would expect a more advanced interpretation. Not just reading it out. I would expect that she would use whatever the search engine generated but then elaborate on that in a way that I couldn’t if I was just Googling directly myself… If I feel that she’s plugging it into her own clinical reasoning and putting it in the bigger puzzle of my whole case history and profile and tailoring it to me and then explaining it to me in a way that’s relevant to the bigger picture, then I would be quite happy for her to be Googling. (Interview 6)
Access to high quality information sources
The source of information also impacted on patient perceptions of their doctor’s competence. Some participants conflated all information available online with misinformation. Others suggested books to be a more reputable source of medical information and something that would only be available through a doctor.
You want them to be able to know where to look for this information and I can trust the information I’m going to get from that source. … because there’s a lot of misinformation. And otherwise, I’d be doing that. (Interview 7)
Theme 4: the process of accessing information
Participants felt that the process of accessing information influenced their overall perceptions of trust in their doctor.
Assessment prior to search
Participants identified a doctor’s haste to access information had a deleterious effect on their overall trust. They want to feel they have been thoroughly assessed and their concerns heard. Accessing information at an early point in the consultation could be seen as a demonstration of poor clinical reasoning, prematurely arriving at a diagnosis or having inadequate clinical skill.
I mean, hopefully the first thing they’re doing is not Googling it, hopefully the first thing they’re doing is looking at it or asking you about it. (Interview 7)
Communication skills
The impact of the computer on a doctor’s attention was identified by participants as a barrier to establishing rapport. In the situation where a doctor accesses information, attempting to multitask through half listening, half reading was considered rude and frustrating. The computer can dominate the doctor’s attention leaving the patient feeling unheard and dissatisfied.
It all ties in with communicating well. [If the GP] turns their back on you and goes straight on to the computer I think, that’s actually quite rude. (Interview 12)
Participants wanted to be included in the process of information seeking. They reported curiosity in what the doctor was searching as this was directly related to their personal healthcare. Sharing the computer screen was seen as an ideal way to remain involved in the consultation.
It’s important for me to understand exactly what’s happening with my body, and what I’m doing to it. So that’s why I would really want to know if she was searching it up. (Interview 13)
How a doctor phrased their need to access information was recognised as a key component in protecting patient trust. Using phrases such as ‘double checking’ or ‘confirming’ were considered best practice. If a doctor shared their hypothesis prior to searching, participants felt reassured that the doctor was refreshing previously acquired knowledge and not learning something new. An explanation of the source of information, using terms like ‘guidelines’, ‘medical journals’ or ‘research institute’, was reassuring. Participants ideally wanted their doctor to think out loud as to the reasons for searching. Failing to do so could be construed as being dishonest or hiding knowledge limitations.
I’m watching them Google it, but they’re not going to tell me…They’re doing it but they’re pretending that they’re not doing it… You’re not only, not willing to admit that you don’t know this, but you’re willing to potentially misinform me, just to cover your own lack of knowledge… It’s [a] lack of transparency. (Interview 7)
Be confident
Participants mentioned a doctor’s impression of confidence influenced their views of competence. They preferred a doctor to be honest in uncertainty and transparent about limitations of knowledge but appreciated if this was accompanied by confidence in finding an answer. Doctor’s honesty and transparency helped allay fears that they may not be providing adequate care and confirm they were aware of their short comings.
If they’re open and honest, which is what I would expect, then yeah, it’s okay… [Also] I suppose its confidence; confidence in themselves, confidence in their own ability. And that transfers to the patient. (Interview 14)
A doctor displaying uncertainty with low confidence had a large impact on overall trust.
Time taken
The more time a doctor took to search, the less confidence the patient had. Conversely, finding information too quickly may be seen superficial or rushed.
The time it took to find out made me lose a bit of confidence in a sense. Because the longer you go on, the more you’re left with your mind racing through all these thoughts. (Interview 4)
Frequency
Repeatedly searching for information was seen as a sign of poor knowledge base. Other participants suggested that through their doctor regularly accessing information they had become accustomed to the practice and have subsequently come to accept that this is part of a modern medical consultation.
I’m now used to the protocol with [my doctor]. I understand what they’re doing. (Interview 12)
A teachable moment
Accessing information at the point-of-care was considered as an ideal opportunity to educate the patient on how and where to access high quality and up-to-date information. It was also seen as an important part of educating the patient on the fact that looking things up can be part of high-quality care and improving a patient’s future tolerance of a doctor accessing point-of-care resources.
It’s a good moment to actually teach the patient. Okay, when you Google something, don’t go to something like that, go to something like this. (Interview 3)
Discussion
Summary
This is the first qualitative study to explore patient perceptions of doctors’ information seeking at the point-of-care. The central theme emerging from the interviews was how information seeking impacts on impressions of a doctor’s competence and trust in the advice given. Generally, patients want to have high confidence in their doctor. We identified four major themes that influence their trust: the trust a patient has in the doctor prior to the consultation, whether the doctor is expected to know the answer to a question without searching, whether by searching the doctor has added value, and the process of accessing the information. These four themes can increase or decrease patient perceptions of trust when it comes to a doctor accessing information at the point-of-care.
Comparison with existing literature
The impact of the computer and electronic medical record use on patients’ perceptions of their doctor has been relatively well studied. Many of our findings are consistent with previous studies which allows us to infer that the factors that patients perceive to impact on confidence and trust when the computer is being used are the same factors that apply when a doctor is seeking information. A doctor’s body language,15–17 making the patient feel heard through avoiding multitasking with the computer18 and explaining the role of the computer in the consultation19–21 are themes also found in our data. Shaarani et al identified a pre-existing relationship between doctor and patient improved tolerance of the computer in the consultation.21
Cook et al asked doctors about the perceived barriers and enablers to point-of-care information seeking. Physicians identified accessing information at the point-of-care to be an ideal opportunity to learn with patients and engage them in the process of searching. Demonstrating confidence and being candid about not knowing the answers to all questions (particularly if the query was something perceived to be outside of the doctor’s sphere of knowledge) were prominent themes.22 Our findings now provide the patients perspective and can give physicians more confidence that the strategies identified by Cook et al are what patients want when faced with a doctor seeking information during the consultation.22
Participants in our study were interested in knowing the source of information. Kahane et al who asked patients to rate their confidence in doctors who sought information and sources of that information, demonstrated greater patient confidence when the source of information was unknown.11 Both studies have found that patients were less satisfied when doctors sought information from online search engines (ie, Google) and impressed when the information source was a medical textbook.11
Strengths and limitations
This is the first qualitative study to explore patient perceptions of doctors’ information seeking at the point-of-care and thus provides a unique perspective on this issue. The strength of our study was achieving thematic saturation within the broad sample of practices and participants from a diverse range of age groups, educational levels and socioeconomic locations. The use of simulated consultation videos as vignettes to provoke opinions also provided depth to our data.
A key limitation of our study is the possibility that unequal power dynamics may have influenced the data. The participants (general practice patients) may have felt that they could not fully express negative views during an interview with a practicing doctor due to fears of judgement or offence. Another limitation is the possible differences between gender groups. We acknowledge that previous research has shown differences in gender groups, however as this was an exploratory study we did not seek to differentiate between men and women.
Implications for research and practice
Navigating point-of-care information seeking and implementing effective strategies to manage this process is important for clinicians in the digital age. Our themes interact dynamically to reflect patient trust in their doctor (figure 1). Clinicians need to be aware of how to modulate the themes that are dynamic (adding value, process) and be wary of the themes that they may have less ability to control (baseline trust, sphere of knowledge).
There appears to be a mismatch between doctor and patient perceptions of information seeking at the point-of-care. Other data has presented information seeking by doctors as a cognitive skill,22 whereas patients view this process as a communication skill. Patients do not place high value on the type of question asked (eg, diagnostic, management, prognostic), but expect a clinician to focus on the communication and interpersonal skills of the consultation before they will feel comfortable for the doctor to access information. This process of a clinician ‘earning the right’ to search can be achieved through building rapport and trust, then bringing the patient along on the journey of searching. Listening, assessing thoroughly and being honest and transparent about the need to seek information are the most useful skills. These communication skills need to be taught in medical and specialist training as the need for clinicians to access information at the point-of-care and remain up-to-date with emerging medical evidence is only likely to increase over the time.
Clinicians seeking information during a consultation need to be mindful of the factors over which they have less control. An understanding of the footing on which the consultation starts is key and may require clinicians to be particularly careful around new patients. Doctors working in specialised clinics or environments with specific patient groups also need to pay greater attention to the communication and interpersonal skills involved in information seeking. However, an understanding of patient views of the questions that a doctor might search, needs further investigation. Defining what patients believe constitutes basic or complex knowledge would be helpful in guiding clinicians in seeking acceptable information during consultations.
The next step for researchers is to explore how the lessons from our study can be implemented into the clinical environment. Research exploring the implementation of our findings into practice, measuring both clinician and patient views may shed further light on this complex but expanding component of the consultation.
Conclusion
Building and maintaining patient trust is key to positive perceptions of clinicians’ information seeking at the point-of-care. Communication and interpersonal skills are fundamental in forging this trust. A doctor’s ability to listen, understand the patients agenda and appear open and transparent regarding the need to search, all contribute to a positive experience.
Data availability statement
No data are available.
Ethics statements
Patient consent for publication
Ethics approval
Ethics approval was obtained from The University of Queensland human research ethics committee (#2021/HE000756).
Acknowledgments
We acknowledge the participants who volunteered their time to contribute to this piece of research.
References
Footnotes
Contributors The first author (IT) primarily designed, conducted, analysed and authored this research. IT accepts overall responsibility of this work as guarantor. The coauthors (BM and MLvD) provided oversight and supervision to the project in addition to significant intellectual and editorial input in analysis and authorship.
Funding This research project is supported by the Royal Australian College of General Practitioners with funding from the Australian Government under the Australian General Practice Training programme. Grant/award number – N/A.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.