Article Text

Abstract
Objective There are numerous studies reporting a disproportionally high prevalence of thrombophilia in women with a history of recurrent miscarriage (RM), which has led to overdiagnosis and treatment without an improvement in clinical outcomes. The objective of our study was to assess the prevalence of inherited and acquired thrombophilia in a large cohort of women with a history of early RM using internationally agreed diagnostic criteria and inclusion parameters and compare it to the meta-analysis results of existing literature.
Design Retrospective cohort study and systematic review of literature.
Setting This is a retrospective cohort study set-up in two dedicated tertiary centres for women with RM in Southwest London and Surrey. We reviewed all the available literature related to causes of RMs. We ascertained the prevalence of thrombophilia in the study population and compared it with historical and published prevalence in the general population.
Participants 1155 women between 2012 and 2017. All patients had three or more first trimester miscarriages and a full thrombophilia screen.
Results The overall prevalence of thrombophilia in our study population is 9.2% (106/1155) with 8.1% (94/1155) of cases positive for inherited thrombophilia, which is similar to the general population; Factor V Leiden (4.9%; 57/1155) and prothrombin gene mutation (2.9%; 34/1155) were the most common inherited thrombophilias, while only 1% (12/1155) tested positive for acquired thrombophilia. Persistent positive lupus anticoagulant (LA) was found in 0.5% (6/1155) and persistent positive anticardiolipin (ACL) antibodies with a value ≥40 U/mL was found in 0.5% (6/1155) of patients. Tests for LA/ACL were performed a minimum of 12 weeks apart thus meeting the revised Sapporo criteria for a diagnosis of antiphospholipid syndrome.
Conclusion The findings of our study demonstrate that the prevalence of inherited thrombophilia is similar in women with RM to that in the general population. Similarly, the prevalence of acquired thrombophilia, using the revised Sapporo criteria, in the cohort of RMs is similar to that in the general population. Therefore, we do not recommend investigation or treatment of inherited or acquired thrombophilia in women with RM.
PROSPERO registration number CRD42020223554.
- OBSTETRICS
- Anticoagulation
- Maternal medicine
- Reproductive medicine
Data availability statement
No data are available. Data is available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
The examination of a large cohort of pregnancies with three or more recurrent miscarriage (RM) in specialist dedicated clinics; accurate and systematic investigation of aetiological causes of early RM including inherited and acquired thrombophilia.
Use of a standardised method of analysis of results; using the same reference range to mitigate errors introduced due to variation in laboratory reporting such as adherence to the diagnostic criteria of the revised Sapporo criteria.
Systematic review of literature using standard criteria and statistical analysis.
The retrospective nature of the study and lack of contemporaneous data from control pregnancies; however, the latter is not a part of routine clinical practice.
Studies included in this review were restricted to women with three or more first trimester miscarriages and those that a minimum of 100 women in the miscarriage arm.
Introduction
Recurrent miscarriage (RM), which affects 1% of couples trying to conceive, is defined as the loss of three or more consecutive pregnancies from the time of conception up to 24 completed weeks of gestation.1 There are differences in recommendations from professional bodies with regards to the definition of RM, with some requiring two or more clinical pregnancies with ultrasound or histological confirmation of pregnancy loss, whereas others requiring three or more losses after a positive pregnancy test with no specification of the need for clinical confirmation.1 2 These variations in definitions may potentially affect the prevalence of underlying causes of RM in various studies, as the aetiology of biochemical pregnancy loss may be different compared with loss in the second trimester.
Many factors have been studied as possible causes of RM such as anatomical, endocrine, immunological, genetic and thrombophilia (inherited and acquired) disorders. The inherited thrombophilia includes causes such as the presence of Factor V Leiden (FVL) and prothrombin G20210A mutation (PGM), antithrombin and protein C and S deficiencies, whereas acquired thrombophilia includes the presence of lupus anticoagulant (LA), anticardiolipin (ACL) and anti-beta 2 glycoprotein antibodies. There are many studies reporting a disproportionally high prevalence of thrombophilia in women with a history of RM, which has led to this condition being frequently overdiagnosed.3–6 These studies included women at various gestations and the number of pregnancy losses as well as those identified as having acquired thrombophilia based on values that do not meet the diagnostic criteria. This has led to unnecessary investigations and empirical treatment without improvement in clinical outcomes.7–9 In contrast, there is evidence from studies suggesting that the prevalence of inherited thrombophilia in women with RM is similar to the general population and that its presence in women with RM is more likely to be an association rather than causation.4 8–11
The objective of our study was to assess the prevalence of inherited and acquired thrombophilia in a large cohort of women with a history of early RM using internationally agreed diagnostic criteria and inclusion parameters. We also undertook a systematic review of literature and meta-analysis for studies that reported data regarding inherited and acquired thrombophilia for women with RM and control population.
Methods
Cohort study
Setting
This is a retrospective cohort study set-up for women with RM in Epsom and St Helier University Hospitals NHS Trust and the Centre for Reproductive Immunology and Pregnancy, London, and Surrey. We reviewed all the available literature related to causes of RMs. We ascertained the prevalence of thrombophilia in the study population and compared it with historical and published prevalence in the general population.
Participants
A total of 1155 women between 2012 and 2017. All couples who have a history of three or more recurrent first trimester losses are eligible for referral to these specialist RM clinics. We record parental demographic information, medical, surgical and gynaecological history and offer comprehensive investigations which include testing for inherited and acquired thrombophilia.
Inclusion and exclusion criteria
The study population included women with a history of three or more first trimester miscarriages and those who had available results for inherited and acquired thrombophilia. We excluded cases that had incomplete results for the thrombophilia screen.
Patient and public involvement
No patients were involved in the conduct or design of the study.
Outcome measures for inherited and acquired thrombophilia
The investigations included in this paper are for homozygous or heterozygous mutations in FVL and PGM. Comparison of prevalence of FVL and PGM was made with prevalence in women with RM and controls reported in literature. Data of other inherited thrombophilia were available for a proportion of study cohort study population but were not reported or analysed due to the rare incidence in the population.
The investigations for acquired thrombophilia included testing for LA and ACL. We ensured strict criteria for defining a positive antibody test, and therefore by implication, an acquired thrombophilia was present if the result fulfilled the revised Sapporo criteria.12 A positive LA test was defined as the presence of positive result on two occasions at least 12 weeks apart. The LA screen consisted of a dilute Russell’s viper venom time (dRVVT) and an activated partial thromboplastin test test.13 The normal result for both screening tests was a ratio of ≤1.6. If either test was >1.6, a correction was carried out. The test was considered positive if the correction test is >10%. Similarly, a positive ACL antibody test was defined as presence of IgG or IgM antibodies measured using a standardised ELISA with a level ≥40 U/mL on two occasions at least 12 weeks apart.
Systematic review and meta-analysis
Study registration
This study was registered with International Prospective Register of Systematic Reviews.
Data sources and searches
A search of MEDLINE and Embase via the NICE Healthcare Databases Advanced Search interface and a Cochrane database search was performed using Medical Subject Heading (MeSH) terms including exp THROMBOPHILIA/, *‘FACTOR V LEIDEN’/, *‘ANTIBODIES, ANTICARDIOLIPIN’/and *‘PROTHROMBIN GENE MUTATION’/. The search was very specific and to ensure as much relevant literature on the search topic was retrieved, the major search option was used for the MeSH terms to ensure that the focus of the papers was that particular term. Example terms where the major option was chosen includes *‘LUPUS COAGULATION INHIBITOR’/, *‘ANTIBODIES and ANTICARDIOLIPIN’/. A limit of English language, and all papers related to humans and papers dated from 1990 to 2020 were applied. Studies included in this review consisted of observational, case control, prospective and retrospective cohort studies that had women with three or more first trimester miscarriages and those that a minimum of 100 women in the miscarriage arm. Four independent reviewers (AA, MS-E, HJ and HS) applied the inclusion criteria to the identified articles from the search and crossed checked the selection process between them. Our search identified 2000 citations; details of search criteria are outlined in (online supplemental file 1) and process of article selection are detailed in figure 1. There was a variation in antiphospholipid antibody levels as well as the interval between tests. After applying the diagnostic criteria, the final analysis included 12 papers; 10 on inherited and 2 on acquired thrombophilia.
Supplemental material

Flow chart of Healthcare Database Advanced Search (HDAS) demonstrating process of selection of studies included in the systematic review.
Statistical analysis
For all studies in the systematic review, the summary statistics for prevalence of FVL and PGM were derived in the RM and control groups. These individual study statistics were then combined to obtain a pooled summary estimate which was calculated as a weighted average of the individual study estimates in the RM and control groups using both fixed and random-effects model. The fixed-effects model weighs each study by the inverse of its variance and only considers variability in results within studies and not between studies. The random-effects model allows for between-study variability in results by weighting studies using a combination of their own variance and the between-study variance. To determine whether there was a significant difference in the prevalence of thrombophilia between the RM and control groups, we estimated the difference in prevalence (95% CI) between the RM group and control group for each study using the incidence-rate difference (IRD) meta-analysis; the individual summary statistics of difference in prevalence in each study were combined to calculate a weighted pooled estimate for FVL and PGM with IRD meta-analysis. We also estimated the effect size of the significance of difference in prevalence by calculating relative risk (RR) (95% CI) for each study and then a weighted pooled estimate from the RR for each study. Forrest plots of summary statistics for each study and final pooled estimates were constructed using data from the random-effects models.
The heterogeneity between studies was estimated using Cochrane’s heterogeneity statistic Q, which was calculated as the weighted sum of squared differences between individual study effects and the pooled effect across studies, with the weights being those used in the pooling method (R). Inconsistency between study results was assessed using the I2 statistic, which was calculated as I²=100%×(Q–df)/Q, where Q is the Cochrane’s heterogeneity statistic and df the df. The statistical software package StatsDirect V.2.7.9 (StatsDirect, Cheshire, UK) and MedCalc Statistical Software V.16.4.3 (MedCalc Software, Ostend, Belgium) were used for data analysis.
Results
Study population
There was a total of 1267 women with a history of three or more consecutive early RM in our study population. We excluded cases with missing data and duplicates (n=112) and included data from 1155 women. The overall prevalence of thrombophilia in our study population was 9.2% (106/1155) of which most cases were positive for inherited thrombophilia 8.1% (94/1155) and 1.0% (12/1155) tested positive for acquired thrombophilia. The median age was 37 years (IQR 33–40) and 66.6% (769/1155) of the cohort had no previous live birth.
Inherited thrombophilia
The most common inherited thrombophilia was FVL heterozygous mutation, which was noted in 4.8% (55/1155) followed by heterozygous PGM which was identified in 2.9% (34/1155) of patients. There was no significant difference in the prevalence of FVL mutation in our study versus that reported in literature in the RM group ((4.8%) 55/1155 vs (5.8%) 92/1584, respectively; p=0.263) as well as the prevalence of FVL in RM group versus that of control population from literature ((4.8%) 55/1155 vs (4.9%) 47/966, respectively; p=0.354) (figure 2). Similarly, there was no significant difference in the prevalence of PGM mutation in our study versus that reported in literature in the RM group ((2.9%) 34/1155 vs (3.7%) 29/786, respectively; p=0.436) as well as the prevalence of PGM in RM group in our study versus that of control population from literature ((2.9%) 34/1155 vs (2.4%) 22/914, respectively; p=0.541) (figure 2). Only one woman had compound heterozygous for FVL and PGM and one homozygous FVL result. The meta-analysis of proportions demonstrated that the weighted pooled prevalence of FVL in the RM and control group was 5.8% (95% CI: 4.6% to 7.1%) and 5.2% (95% CI: 3.3% to 7.5%), respectively. There was no significant difference in the weighted pooled prevalence of FVL in the RM and control group (0.4 (95% CI: −1.6 to 2.3); Z-test=0.396, p=0.692) (online supplemental table 2). Similarly, there was no significantly increased risk of RM in women with FVL (RR=1.02 (95% CI: 0.71 to 1.48); p=0.906) (online supplemental table 2, figure 3). The meta-analysis of proportions demonstrated that the weighted pooled prevalence of PGM in the RM and control group was 3.9% (95% CI: 2.7% to 5.4%) and 2.6% (95% CI: 1.6% to 3.7%), respectively (online supplemental table 3). There was no significant difference in the weighted pooled prevalence of PGM in the RM and control group (1.2% (95% CI: −0.4% to 2.8%); Z-test=1.463; p=0.143) (online supplemental table 3, figure 4). Similarly, there was no significantly increased risk of RM in women with PGM (RR=1.50 (95% CI: 0.86 to 2.60); p=0.154) (figure 4).

Prevalence of Factor V Leiden (FVL) mutation (A) and prothrombin gene (PG) mutation (B) in our study in women with recurrent miscarriages (crossed bar) compared with prevalence reported in literature in recurrent miscarriages (grey solid bar) and general population (black solid bar).
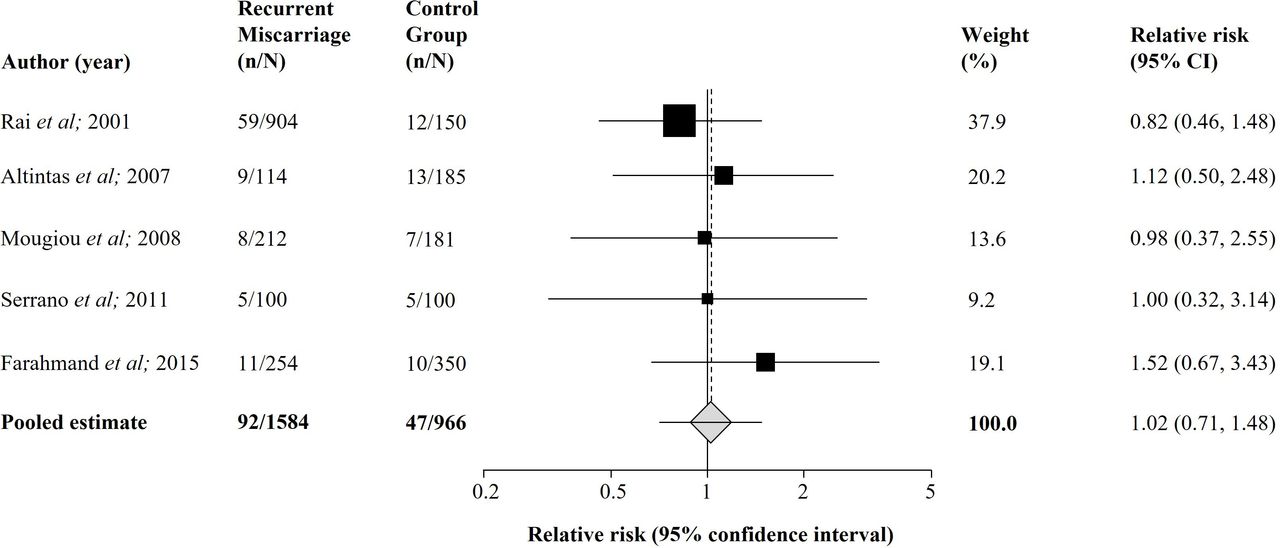
Forest plot demonstrating summary statistics (relative risk (95% CIs)) derived from a random effects model for prevalence of Factor V Leiden in women with recurrent miscarriages compared with the control population. Study weights derived from random effect model.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plot demonstrating summary statistics (relative risk (95% CIs)) derived from a random effects model for prevalence of prothrombin gene mutation in women with recurrent miscarriages compared with the control population. Study weights derived from random effect model.
Acquired thrombophilia
An initial positive LA test was found in 18 patients, of these, only a third remained positive on repeat testing, giving an LA prevalence of 0.5% (6/1155). A total of 23/1155 (2.0%) patients had two positive ACL tests performed a minimum of 12 weeks apart, based on a laboratory cut-off value of ≥10 U/mL. Of these, two patients had a value ≥40 U/mL on initial or repeat testing, and four had two results with a value ≥40 U/mL giving an ACL prevalence of 0.5% (6/1155). The data concluded the total prevalence of antiphospholipid syndrome is 1.0% (12/1155).
Discussion
Principal findings of the study
The findings of our study demonstrate that the prevalence of inherited thrombophilia in a large cohort of women with a history of early three or more RM is similar to that of the general population, and that the prevalence of acquired thrombophilia is low and not significantly different than the prevalence reported in the general population. Women and their clinical practitioners should be aware that the contribution of inherited and acquired thrombophilia in causing early RM is extremely low, and hence empirical testing and treatment for thrombophilia, such as low dose aspirin and low molecular weight heparin should not be advised, unless there is unequivocal clinical and laboratory evidence of established disease.
Strengths and limitations
The strengths of our study are the examination of a large cohort of pregnancies with three or more RM in specialist dedicated clinics; accurate and systematic investigation of aetiological causes of early RM including inherited and acquired thrombophilia; use of a standardised method of analysis of results; using the same reference range to mitigate errors introduced due to variation in laboratory reporting; and the adherence to the diagnostic criteria of the revised Sapporo criteria. The limitations of our study are the retrospective nature of the study and lack of contemporaneous data from control pregnancies; however, the latter is not a part of routine clinical practice. Studies included in this review were restricted to women with three or more first trimester miscarriages and those with a minimum of 100 women in the miscarriage arm. The minimum number of 100 women in the study arm could be seen as a limitation.
Comparison with other studies
Our findings are consistent with results of other studies, including large systematic reviews and meta-analyses, which report no significant difference in the prevalence of inherited thrombophilia in women with a history of RM compared with controls.7 14–16 In one large case–control study of 1111 women examining the prevalence of FVL mutation in women with early and late RM compared with controls, the authors reported no significant difference in the prevalence of FVL mutation in early or late RM and controls, which was 3.3%, 3.9% and 4.0%, respectively.14
Our literature search identified five suitable publications for FVL prevalence14 17–20 and five for PGM prevalence.17–21 The prevalence of FVL in the miscarriage control group is 5.2% compared with 7.7% in the general population,14 17–20 while the prevalence of FVL in our miscarriage population is 4.8%. Similarly, the prevalence of PGM in the miscarriage control group is 2.6% compared with 3.7% in the general population,17–21 with our miscarriage population at 2.9%. Therefore, this suggests that there is no significant association of heterozygous FVL or PGM with RM.
In contrast, older studies have reported a high prevalence of inherited thrombophilia in women with RM and therefore advocate routine testing and treatment.22–24 There is large variation however in the prevalence of FVL and PGM in the general population.25 This is most likely due to genetic variations with more prevalence seen in the Levant region and Europe compared with the USA and the Far East. Despite the widespread practice of screening and treatment, the European Society for Human Reproduction and Embryology26 and the American Society for Reproductive Medicine guidelines2 do not recommend screening for inherited thrombophilia. At present the Royal College of Obstetricians and Gynaecologists recommends screening only if women present with pregnancy loss in the second trimester despite little evidence to support this.1
Similar to inherited thrombophilia, there is controversial evidence about the association between acquired thrombophilia and RM, with some studies reporting a strong association,27 28 whereas others question this association.29 30 The prevalence of antiphospholipid antibodies in the healthy general population is 1%–5%.31 The prevalence of acquired thrombophilia in women with RM in our study population (1%) is similar or lower when compared with healthy pregnant controls in other studies with a prevalence of ACL IgM at 3%, ACL IgG antibodies at 1%32 and 1.4% of LA and ACL,33 respectively. A frequently cited study by Rai et al reported a prevalence of antiphospholipid antibodies in women with RM as high as 15%.34 However, this predated the original Sapporo criteria published in 1999 and hence included levels of antiphospholipid antibodies that were even lower than 10 U/mL, which is the laboratory threshold for diagnosis, as well as less than a 12-week interval between the tests. Applying the revised Sapporo criteria (2006) with the higher laboratory level (40 U/mL) to this study, the number of patients with raised ACL IgG antibodies will reduce from 15 to 4, and the number of raised IgM will reduce from 9 to 3 out of a total of 500 patients giving a prevalence of raised ACL antibodies of 1.4% (7/500) compared with the 5.5% (24/500) quoted in the original paper. With regards to LA, the new revised criteria states that levels of dRVVT ratio should be ≥1.2. If this is applied, the number of patients with positive LA will reduce from 46 to 9 which would give a prevalence of 1.8% (9/500) compared with 9.6% (46/500) quoted in the original paper. Hence the revised total prevalence for the Rai et al paper would boast at best a prevalence of 3.2% which most likely would reduce further if the 12-week interval is applied, and not the widely quoted 15%. A more recent study examined the association of antiphospholipid syndrome and RM using the revised Sapporo criteria for diagnosis and reported that this is present in only 2% of the population of RM,30 while another study reported 0.2% prevalence of LA.29
Our results are consistent with these findings and reiterate that the prevalence of acquired thrombophilia in women with RM is extremely low and is similar to the general population. This was highlighted in the recent recommendations from the 14th International Congress on Antiphospholipid Antibodies Task Force report, which stated that studies reporting the association between antiphospholipid antibodies and RM are heterogeneous with considerable variation in the definition of RM and in the cut-offs used for defining what constitutes positive antibody levels. They concluded that the association between antiphospholipid antibodies and RM remains inconclusive and further research is required to establish recommendations.35
Conclusion
The prevalence of inherited and acquired thrombophilia in women with history of RM in the first trimester of pregnancy is similar to that of the general population. The prevalence of acquired thrombophilia is only 1% in our study and between 0.2% and 2% in other good quality publications that adhered to the appropriate diagnostic criteria, which implies that the prevalence of not just inherited but also acquired thrombophilia in women with a history of RM is similar to that of the general population.
Therefore, we do not recommend routine investigation or treatment of thrombophilia in women with history of RM, and specifically do not recommend empirical thromboprophylaxis with low molecular weight heparin based on obstetrical history in the absence of any clinical evidence of thrombophilia. Further research should be carried out into other aetiologies of RM such as immunological factors and other treatment options.
Data availability statement
No data are available. Data is available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by NHS Health Research Authority (HRA) (IRAS ID: 281484, REC reference: 20/HRA/6376).
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors HS and AA performed part of the analysis and drafted the manuscript. HS devised the study idea and facilitated data acquisition. MS-E, SH, AE and RV assisted with the data collection. AA, MS-E, HJ and HS reviewed all the papers from the searches. RA advised on study design and provided statistical analysis. HS, AA and RA contributed to interpretation of the data and revising the manuscript. The final version was approved by all authors. HS is the author acting as guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.