Article Text

Abstract
Background Hepatitis B and HIV care share health system challenges in the implementation of primary prevention, screening, early linkage to care, monitoring of therapeutic success and long-term medication adherence.
Setting Arua regional referral hospital (RRH) and Koboko district hospital (DH), the West Nile region of Uganda.
Design A cross-sectional hospital-based cost minimisation study from the providers’ perspective considers financial costs to measure the amount of money spent on resources used in the stand-alone and integrated pathways.
Data sources Clinic inputs and procurement invoices, budgetary documents, open market information and expert opinion. Data were extracted from 3121 files of HIV and hepatitis B virus (HBV) monoinfected patients from the two study sites.
Objective To estimate provider costs associated with running an integrated HBV and HIV clinical pathway for patients on lifelong treatment in low-resource setting in Uganda.
Outcome measures The annual cost per patient was simulated based on the total amount of resources spent for all the expected number of patient visits to the facility for HBV or HIV care per year.
Results Findings showed that Arua hospital had a higher cost per patient in both clinics than did Koboko Hospital. The cost per HBV patient was US$163.59 in Arua and US$145.76 in Koboko while the cost per HIV patient was US$176.52 in Arua and US$173.23 in Koboko. The integration resulted in a total saving of US$36.73 per patient per year in Arua RRH and US$17.5 in Koboko DH.
Conclusion The application of the integrated Pathway in HIV and HBV patient management could improve hospital cost efficiency compared with operating stand-alone clinics.
- health economics
- health policy
- organisation of health services
- quality in health care
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
Cost data were collected on-site alongside the pilot integration activities.
This is the first study that provides a good framework for other studies.
Potential long-term outcomes of the integration not considered in the analysis.
Missing patient records resulted in incomplete cost computation in some areas.
Background
Hepatitis B virus (HBV) infection remains a major public health problem affecting close to one-third of the world’s population. WHO estimates 257 million HBV infections globally and also estimated 1.35 million deaths in 2015.1 HBV coinfection with HIV is common and it is estimated that among the 36.7 million people living with HIV globally, about 2.7 million are also infected with HBV with the greatest burden (69%) occurring in sub-Saharan Africa.2 In Uganda, approximately 4.1% of the population is estimated to have chronic HBV infection with a much higher prevalence in the mid-north (4.6%) and lowest in the southwestern region of 0.8%.3 The WHO global health sector strategy on viral hepatitis that aims at achieving a 90% reduction in new cases of chronic hepatitis B and C and a 65% reduction in mortality due to hepatitis B and C by 2030 requires innovative approaches to increase access to care.4
Despite the availability of comprehensive WHO guidelines on HBV testing, care, and management for low-income settings, these are faced with numerous implementation challenges.1 5 Healthcare systems across the globe have innovated approaches to address such challenges through planning and integration of national responses to viral hepatitis.6 One such strategy is integrating Hepatitis B care into well-structured HIV care services. The two diseases overlap in their main modes of transmission and favourable treatment outcomes with antiviral drugs.7 HIV and Hepatitis B care face common health system challenges in terms of the successful implementation of primary prevention, screening, diagnosis, linkage to care; therapeutics and monitoring of therapeutic success, as well as addressing the need for long-term medication, counselling and adherence. In Uganda, HIV care has a well-defined model of care with well-established structures and units throughout the country. On the other hand, HBV care is rudimentary without a clearly defined model for linkage to care, adherence counselling, follow-up mechanisms and monitoring for complications such as cirrhosis and liver cancer. Although HIV care has been integrated with tuberculosis among other ailments, HBV has never been integrated. Integrated pathways have been reported to reduce costs and resource utilisation7 and there is growing interest in exploring methods through which care pathways for people with related comorbid health problems may be integrated.
A major impediment to effective integration is the limited number of models to demonstrate how to optimally deliver a simplified integrated model of care8 and how best to leverage existing health services and infrastructure.9 Integrated pathways have been reported to reduce costs and resource utilisation10 and there is growing interest in exploring methods through which care pathways for people with related comorbid health problems may be integrated.11 Therefore, to inform current resource allocation policies on accelerating and scaling up Hepatitis B care in Uganda and sub-Saharan Africa at large, the ‘2for1’ pilot study established a demonstration of integrated HIV and HBV clinical care pathway in the high HBV burden setting. The pilot study developed a simplified model of an integrated care pathway across the entire continuum of care for HIV and HBV. In this paper, we report on provider costs incurred per patient per year in a stand-alone pathway before the pilot and costs in an integrated HBV and HIV clinical pathway for patients on lifelong care and treatment in the pilot sites.
Methods
Study site
This study was conducted in the West Nile region of Uganda. West Nile is a region in north-western Uganda comprising eight districts with a total population estimate of 1.9 million. The subregion is bordered by the Democratic Republic of Congo to the south and west, South Sudan to the north and the Albert Nile to the east. The town of Arua is the largest city in the sub-region and lies approximately 420 km by road north of Kampala, the capital of Uganda. West Nile is one of the regions with the highest prevalence of Hepatitis B in the country.3 The study was specifically conducted in Arua Regional Referral Hospital (RRH), a high-volume facility and Koboko District Hospital (DH), a low-volume facility.
Study population
The study population comprised hepatitis B infected patients and HIV positive patients attending Arua RRH and Koboko DH. Hepatitis B infected patients on treatment and those on monitoring were both considered in the analysis. We reviewed and extracted data from 3121 files of patients from the two study facilities for both the HIV and HBV patients. However, Hepatitis B and HIV coinfected patients were already receiving care in the HIV clinic and thus were considered in the HIV arm of the analysis. The health system in these facilities is facing challenges in managing HBV-infected patients due to inadequate funding and limited human resource. Integration of hepatitis B care into the better resourced and fairly well funded HIV care clinical pathway could be a potential intervention to improve the poor hepatitis B health outcomes in the region.
Study procedure
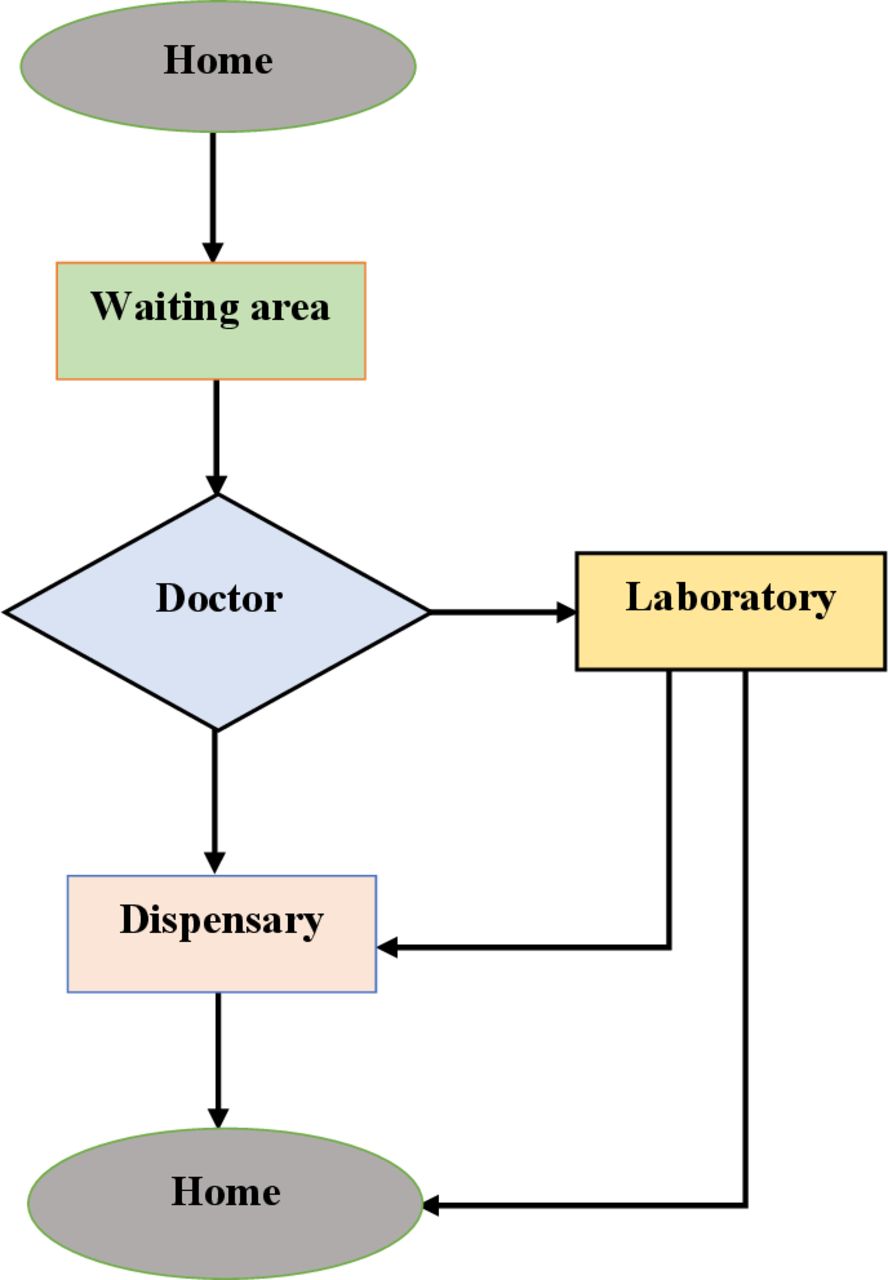
This study was part of the broader pilot project conducted in Arua RRH and Koboko DH to demonstrate a simplified integrated service model across the continuum of hepatitis B care embedded in the existing HIV clinic. Data collection and analysis were done in two phases spaced 6 months apart. The first phase was done in the stand-alone HIV and Hepatitis B clinics. In this phase, we mapped the care pathway for HBV and HIV monoinfected patients in their respective stand-alone clinics (figure 1) and then determined the total direct costs associated with managing patients. In the study’s second phase, the HBV clinic services were merged into the HIV clinic. We subsequently mapped the flow for both HBV monoinfected and HIV infected patients in the merged clinic in both hospitals (figure 2). We costed the integrated pathway throughout the continuum of care for both HBV monoinfected patients and HIV infected patients. The outcome measure is the effect of the integration of HBV and HIV care on the cost per patient per year.

Arua Hospital hepatitis B stand-alone pathway.

Koboko Hospital hepatitis B stand-alone pathway.
Description of costing clinical pathways
This study compared the costs of operating stand-alone versus integration pathways. The two study sites were operating separate clinics for hepatitis B and HIV-positive clients. The project piloted the integration of the Hepatitis B clinics into the HIV ART clinics. The analysis compared the costs of running the stand-alone clinics (shown in figure 1 for Arua RRH and figure 2 for Koboko DH) and the integrated clinics (shown in figure 3 for Arua RRH and figure 4 for Koboko DH).

Arua regional referral hospital integrated HIV and hepatitis B pathway. HBV, hepatitis B virus; OPD, out patient department.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Koboko hospital integrated HIV and hepatitis B pathway. HBV, hepatitis B virus; OPD, out patient department.
Data collection
The first phase of data collection was done in the stand-alone clinics and the second phase in the integrated clinics. In both facilities, we sought expert opinions from key staff who were purposively selected to provide information about the respective costing elements. These included: medical superintendents, hospital administrators, nurses, clinicians, laboratory technicians and accountants. This was done to ascertain types and, in some cases, amounts of on-site resources (eg, staff salaries and benefits, medications, recurring consumables, and administrative costs). Costs for off-site resources (eg, linkage officers, community outreaches and transportation costs) were not determined because they were not directly linked to the clinical pathway. In addition, we reviewed administrative records such as delivery notes, invoices, payment vouchers and budgets to ascertain staff salaries and allowances for support staff, costs of medications and laboratory tests, costs of consumables and utilities, costs of transportation, and equipment. Finally, we conducted time use surveys in each section of the pathway in both clinics before and during the integration to establish the proportion of total work time clinic staff spent providing care and determined the average time per patient.
Costing inputs
The study captured financial costs to determine the amount spent on resources used in the running of the stand-alone and the integrated clinical pathways. These were inputs used in the delivery of services along the pathway that could be directly assigned to patients. We considered case-specific direct costs that were collected based on the services received by the patient along the pathway before and during the integration. From the patient files reviewed, we retrieved the laboratory tests done, the drug regimen and the departments attended during clinic visits. For example, an HBV-infected patient on treatment required services of the pharmacist while the patient on monitoring did not. These inputs included: physical infrastructure used for client care; medical equipment; medical consumables and supplies used; laboratory testing; drugs; and staff time in caring for clients. Labour costs of administrative staff; overhead expenses (such as office supplies and communication expenses), biosafety requirements and data management systems. There were no user fees involved. Drug costs within the hospital were only considered if they were part of the HBV or HIV treatment regimen. Additional detail about the specific cost inputs is found in online supplemental file 1.
Supplemental material
Cost data sources
Cost estimates were obtained from clinic inputs and procurement invoices. Additional information was obtained from budgetary documentation reviews, procurement guides, and publicly available product information. Expert opinion was sought from suppliers, implementing partners, local distributors, and health workers. Previous costing studies were reviewed to validate some of the estimates.11 More cost data were obtained from the hospital administration and accounts department, implementing partners, available literature, National Medical Stores and Joint Medical Stores price catalogue, health facility records such as delivery notes, budgets, and invoices among others.
Costing approach
This study predominantly used an activity-based costing approach except for some overheads where a top-down analysis was used.12 The purpose of the costing was to identify the least costly alternative of the patient pathways with the potential to reduce the cost per patient per year. The costing approach was based on the concept that activities consume resources to produce an output. We measured the cost and performance of activities, resources and cost objects. Resources were assigned to activities, then activities were assigned to cost objects based on their use. In this study, the entire treatment process was divided into several activities at different sections of the pathway. We modelled the total annual costs per patient as a sum of the five cost categories: personnel, medications, laboratory testing, other recurrent costs (utilities and consumables), and fixed costs along the clinical pathway. The analysis adopted the healthcare providers’ perspective to determine and illustrate cost variations from the stand-alone pathways to the integrated pathway. A cost-minimisation analysis, a form of economic evaluation that compares costs of alternative interventions that have equal effects was used to guide the measurement and comparison of costs of the stand-alone and integrated care pathways. This was chosen on assumption that patient outcomes were the same in the stand-alone and in the integrated pathways.
Quantification and valuation of inputs
The costing model involved only health facility inputs. Resources associated with the stand-alone and integrated pathways were measured through observation of standard operating procedures as health workers and supporting staff performed their duties in respective sections within the pathway. Staff salary, for example, was allocated based on the time spent on the reference case (described in the assumptions) as a proportion of monthly worktime. The useful life span of medical equipment used was considered according to the manufacturers’ instructions where possible or an estimated period from expert opinion. Building space occupied was given an assumed expected lifetime of 30 years. All costs were estimated as of mid-year prices of 2020 and converted to US dollars using published Bank of Uganda exchange rate of US$1USD=UGX3700. The time horizon for cost analysis was 1 year and thus discounting for future costs was not done. We estimated per person per year (pppy) costs obtained as a total of the costs incurred for all clinic visits in 1 year based on expected patient attendance. The model did not include the long-term effects of missed appointments or unintentional delays in the pathway.
Sensitivity analysis was done to determine the influence of refill visits, patient numbers, and price of consumables on the overall cost per patient per year. Sensitivity analysis was majorly centred on the varying number of patients per month and the varying number of clinic visits per year. Clinic visits for HBV stable patients ranged from once a year to six times a year, while HIV stable patients’ clinic visits ranged between 2 and 6 times a year. The visits depended on the patient medical condition as determined by the medical team from time to time. We also varied the costs of consumables because their values were majorly obtained from expert opinion and fluctuating market prices.
Assumptions
We used the Consolidated Health Economic Evaluation Reporting Standards (CHEERS) reporting guidelines13 to verify and ensure standard reporting of this work. We assumed an average number of four visits per year for both HBV and HIV stable patients since the frequency of appointments varied based on patients’ level of adherence, rate of missing appointments, viral load levels and distance to the facility among others. We assumed a male HBV and HIV mono-infected patient on first-line treatment as a reference case in assigning the costs. In the cost-minimisation analysis, we assumed equivalence in patient health outcomes for the stand-alone and the integrated pathways since the medication received by the patients was the same in both pathways. The study also assumed that all the overhead costs of infrastructure, laboratory tests, drug prescriptions, sample collection requirements and biosafety requirements were equal for the stand-alone and integrated pathways in both facilities. The useful life of the medical equipment was assumed to vary between 2 and 5 years and 20% of that use was allocated to HBV patients in the stand-alone clinics since the clinic used to operate 1 day a week (five working days) in both facilities. The useful life of the furniture in the clinics was assumed to vary between 5 and 10 years depending on the type and 100% of that use was allocated to patient use. We also assumed that the stand-alone clinics were independent of each other and that all patients from the HBV clinics were integrated into the existing HIV clinic structures. This assumption may have affected the overall accuracy of the cost estimates made in this study.
Patient and public involvement
No direct patient and public involvement was done in this study.
Results
In the stand-alone pathways, an average of 1982 and 480 HIV clients were seen at Arua RRH and Koboko DH ART clinics respectively. After 6 months during the second phase of the study in the integrated clinics, the number had increased to 2300 and 578 clients in Arua RRH and Koboko DH respectively. Similarly, HBV-infected patients increased from 144 to 163 in Arua RRH and from 72 to 80 in Koboko DH, in the stand-alone and the integrated pathways, respectively. The increase in the number of patients occurred due to the enrolment of new clients to care. The costing model accounted for the resources associated with the stand-alone and integrated pathways provided in the summary cost input (online supplemental file 2) and all the patients enrolled at the costing time points of the pathways.
Supplemental material
Average per Patient per year costs (US$)
The total cost per patient per year for Arua RRH is shown in table 1. In the stand-alone Hepatitis B clinic and HIV clinic the costs were US$163.59 and US$176.52, respectively. After the integration, the total cost per patient lowered to US$151.95 and US$172.63 per year for HBV and HIV patients, respectively. There was an overall cost reduction of 7.1% per HBV patient shifting from the stand-alone (US$163.59) to the integrated pathway (US$151.95). The major cost variation occurred in personnel costs, fixed costs, consumables and utilities. Personnel costs per patient were reduced by 50.5% (US$28.40 in the stand-alone to US$13.76 in the integrated pathway). The task-shifting to and disintegration of the services concentrated to the highly paid physician to low carder personnel in the integrated pathway coupled with sharing of resources led to reduction of costs. Similarly, the costs for consumables and utilities for HBV patients increased by 64.8% in the integrated pathways due to increased services received such as counselling, linkage to care, and laboratory services offered in the integrated pathway. On the other hand, the overall cost per HIV patient was reduced by 2.2% (US$176.52 in the stand-alone to US$172.63 in the integrated pathway). There were cost reductions in all the cost centres except for drugs and Laboratory tests. Personnel costs were reduced by 12.4%, fixed costs by 21.7%, and consumables and utilities by 18.6%.
Per patient per year costs in Arua RRH
In Koboko hospital, the cost estimates shown in table 2 indicated that the total cost per HBV and HIV patient per year in a stand-alone pathway was US$145.76 and US$173.23, respectively. There was an overall cost increase of 3.2% per HBV patient shifting from the stand-alone (US$145.76) to the integrated pathway (US$150.4). On the other hand, the overall cost per HIV patient was reduced by 1.2%. On the other hand, the overall cost per HIV patient was reduced by 1.2%. The increase in HBV per patient cost is indicated by the increase in the number of services obtained in the integrated pathway, while the reduction in HIV per patient cost is attributed to the sharing of services in the integrated pathway.
Per patient per year costs in Koboko hospital
Integration cost efficiency
Cost-saving resulting from the integration shown in table 3 indicates that Arua RRH registered a cost-saving of $32.84 from personnel, fixed costs, consumables and utilities used to run the stand-alone HBV clinic. After the integration of HBV patients into the HIV clinic, the cost per HIV patient was reduced by US$3.89. Thus, the integration resulted in a total saving of US$36.73 per patient per year. In Koboko DH had a total cost saving of US$17.5 per patient per year accruing from savings from Personnel, fixed costs, consumables and utilities (US$15.36 incurred in running the stand-alone HBV clinic, plus US$2.14 from reduction in the cost per HIV patient). The increased number of patients sharing resources such as personnel, building space, equipment and utilities contributed to a reduction in the costs.
Annual cost saving per patient following integration
Sensitivity analysis
The major contributor to uncertainty in the costs per patient per year was the number of scheduled appointments for refill visits for patients on treatment and review visits for HBV patients on monitoring. Table 4 shows that the major cost per patient variation was among HBV patients whose costs varied from US$74.53 to US$246.44 and US$68.98 to US$219.28 in Arua and Koboko hospitals, respectively. Integration resulted in the reduction of this variation by US$15 and US$5 per patient in Arua and Koboko hospitals, respectively. Integration did not have any significant change in cost per HIV patient.
Annual cost variation per patient
Discussion
The study found that the high-volume facility (Arua RRH) had a higher cost per patient in both clinics than did the lower volume facility (Koboko DH). The annual cost per HBV patient was US$163.59 (Arua RRH) and US$145.76 (Koboko DH) while the cost per HIV patient was US$176.52 (Arua RRH) and US$173.23 (Koboko Hospital). The high cost per patient in Arua RRH was due to the higher qualification of the healthcare workers that earned higher salaries and the increased number of services received compared with Koboko DH. The total cost per patient estimates in this study fell within the ranges of per-patient costs estimated in previous HIV studies12 and slightly below other studies that used the societal perspective.13 14 Related analysis from previous estimates has shown that the annual cost of WHO-recommended first-line therapy for HBV monoinfection with tenofovir was US$427 per patient, per year with the lowest price for tenofovir being US$38.15 In addition, estimates from Iran indicated that the total cost of treatment strategies for HBV varied significantly from US$73 to US$8256.16 Our findings further show that drug costs and laboratory tests were major contributors to increased patient care costs in the pathways in both ways, as has also been reported in a study in HIV clinics in Uganda.14
This study further found that integration of the HBV and HIV clinics resulted in a reduction in cost per HBV patient in a high-volume facility and a slight increase in the low volume facility due to economies of scale. In a high-volume facility, the total annual cost per HBV patient was reduced by 7.1% (US$11.66) and 2.2% (US$3.89) for HIV patients. In a low-volume facility, the cost per HBV patient increased by 3.2% (US$4.64) and lowered by 1.2% (US$2.14) per HIV patient. The lowering of costs demonstrates the evidence that integrated clinical pathways have the potential of achieving lesser costs.17 18 Sharing of resources (personnel, infrastructure, utilities and consumables) in the integrated pathway resulted in the lowering of costs for HIV patients in both facilities. Variable costs changed proportionally with service units (the number of patients) while fixed costs did not change as has been reported in other studies19; For example, the cost for equipment is fixed and did not increase even when more patients are enrolled in care. Consequently, the average fixed cost per patient decreased with a growing patient number as costs were distributed among more patients. The increase in HBV costs in a low-volume facility is explained by the increase in personnel costs, fixed costs, consumables, and utilities. HBV monoinfected patients received additional service packages in the integrated clinic. In particular, patients received HIV testing without additional costs and additional blood draws or waiting time for results. Patients received health education on HIV risk reduction, their records were properly managed, and there was quicker linkage to care and prompt follow-up through the HIV-established structures. HBV-infected patients got access to counselling services from experienced HIV counsellors. Related studies among HIV patients have reported that these service packages will, in a long run improve adherence, reduce stigma and minimise lost to follow-up of patients.20 On the other hand, HIV-infected patients benefit from the integration as they gained awareness about HBV and its prevention, minimise fear, and reduce myths about HBV. The synergy brought by the integrated model will result in overall improved awareness and engagement for the prevention of HBV and HIV among the monoinfected person. Further research will be required to find out if the integration will result in an improvement in the quality of services and patients’ outcomes.
Since the integration involved only patients but not resources used in stand-alone clinics, findings indicate that integration was cost-efficient in both facilities with the potential of being cost-effective. The integration resulted in total savings of US$36.73 per patient per year in Arua RRH and US$17.5 per patient per year in Koboko DH. Savings accrued from personnel, fixed costs, consumables and utilities incurred in running the stand-alone HBV clinic and sharing resources in the integrated HIV clinic. In the context of these facilities with fewer unstable patients for both HBV and HIV and where most clients are stable on treatment, long-term costs of care may reduce further. The findings demonstrate potential for scale-up and sustainability in both high-level and low-level facilities in Uganda and sub-Saharan Africa at large. This will become possible since stable HBV clients return for review only once a year resulting in a reduced need for frequent monitoring laboratory tests and health worker time. This is particularly important as the HIV service model has many years of experience and integration will further streamline processes for patient flow, and increase both the efficiency of health worker time and quality of services. Further research is needed to demonstrate the cost-effectiveness of the integrated model.
Limitations of the study
These findings are limited first by the data perspective used in this study; the providers’ perspective may not provide a holistic view of costs as would, the societal perspective.21 In addition, we excluded project inputs from implementing partners such as additional staff and top-up allowances provided to staff because these inputs were from other projects and were not necessarily contributing to sustained care in the pathways. The exclusion of this input could have lowered the real cost per patient per year estimated in this study at the time of the study. Second, the lack of patient records in the stand-alone clinics could have resulted in underestimation or overestimation of the number of patients which could have affected the outcome of the analysis. Third, given that we performed a cost-minimisation analysis primarily, the study did not explicitly quantify benefits and resultant patient outcomes from the stand-alone and integrated clinics. The analytical model assumed equal clinical outcomes regardless of the setting and pathway. The assumptions used in the costing are only applicable at the time of the study as costs and patient needs are constantly changing. Therefore, these findings should be interpreted based on the assumptions made at the time of the study. Nevertheless, to the best of our knowledge, our study is the first to establish the costs of integrated HIV-HBV clinical pathways in sub-Saharan Africa using primary data from a facility-based implementation. Existing economic evaluations of HBV interventions in low-income and middle-income countries focus on the prevention of HBV infection through vaccination.22–24 This study provides a good framework for other studies was well. The costing methodology is replicable in a similar setting with a high HBV burden.
Conclusion
The HIV and HBV integrated clinical pathway provides a streamlined care pathway for HBV patients and ensures cost savings. This rigorous analysis has shown that the application of integrated Pathways in HIV and HBV patient management could improve hospital cost efficiency compared with operating separate clinics. Given that the integration of HBV and HIV treatment into one pathway demonstrates a cost-efficiency in both lower and higher-level facilities with functional structured HIV clinics, this model has significant potential for scalability to other facilities of the same level.
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information.
Ethics statements
Patient consent for publication
Ethics approval
The study was approved by the School of Medicine Research Ethics committee (SOMREC) of Makerere University College of Health Sciences (approval code is REC REF 2018-185) and was also registered with Uganda National Council for Science and Technology-UNCST (approval code is Ref SS 4986). Study participants signed a written informed consent to participate. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
Management and Administration of Arua regional referral hospital and Koboko district referral hospital who provided all the support for the project.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors DLE and JNM collected the data, performed the analysis, and drafted the manuscript together with CW. ES, JA, AK, PE, AM, RB, KM and PO extensively reviewed the manuscript and approved the final version. PO is the guarantor for the study.
Funding This study was funded by Gilead Sciences, Funding number IN-US-320-5326.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.