Article Text

Abstract
Objective A nomogram for predicting the risk of mental health problems was established in a population of factory workers and miners, in order to quickly calculate the probability of a worker suffering from mental health problems.
Methods A cross-sectional survey of 7500 factory workers and miners in Urumqi was conducted by means of an electronic questionnaire using cluster sampling method. Participants were randomly assigned to the training group (70%) and the validation group (30%). Questionnaire-based survey was conducted to collect information. A least absolute shrinkage and selection operator (LASSO) regression model was used to screen the predictors related to the risk of mental health problems of the training group. Multivariate logistic regression analysis was applied to construct the prediction model. Calibration plots and receiver operating characteristic-derived area under the curve (AUC) were used for model validation. Decision curve analysis was applied to calculate the net benefit of the screening model.
Results A total of 7118 participants met the inclusion criteria and the data were randomly divided into a training group (n=4955) and a validation group (n=2163) in a ratio of 3:1. A total of 23 characteristics were included in this study and LASSO regression selected 12 characteristics such as education, professional title, age, Chinese Maslach Burnout Inventory, effort–reward imbalance, asbestos dust, hypertension, diabetes, working hours per day, working years, marital status and work schedule as predictors for the construction of the nomogram. In the validation group, the Brier score was 0.176, the calibration slope was 0.970 and the calibration curve of nomogram showed a good fit. The AUC of training group and verification group were 0.785 and 0.784, respectively.
Conclusion The nomogram combining these 12 characteristics can be used to predict the risk of suffering mental health problems, providing a useful tool for quickly and accurately screening the risk of mental health problems.
- mental health
- preventive medicine
- public health
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This is the first study to develop an easy-to-use nomogram to predict the mental health risks of factory workers and miners.
The area under the curve of training group and verification group were 0.785 and 0.784, respectively, showing moderate discriminatory and calibration power.
This nomogram model’s variables are more comprehensive, including demographics, burn-out, occupational stress and occupational hazards.
We had considered many influential factors, but we were still not certain whether all possible influences were covered.
There is a lack of external validation in other populations in other regions and countries.
Introduction
The WHO defines health as a state of complete physical, mental and social well-being and not merely the absence of disease or weakness.1 Obviously, health is an organic unity of physical and mental well-being. People with good mental health are the precondition for the normal operation of our society. However, with the acceleration of people’s pace of life, people are facing an increasing risk of poor health, which has become a global public health problem.2 Mental health problems can not only take a toll on physical health such as increasing the risk of communicable and non-communicable diseases and even causing unintentional or intentional harm to others,3 but can also have a negative impact on the economy. For example, mental health disorders represent a growing part of the global burden of disease,4 with statistics showing that nearly one billion people worldwide currently suffer from a mental disorder, and mental illness is ranked as one of the leading causes of the global burden of disease.5 Moreover, one study has estimated that due to the impact of mental illness, the global economy loses US$1 trillion every year.6
As researchers around the world have delved into the field of mental health, factors such as gender, income levels, environment and education have been found to be associated with people’s mental health problems.7–10 Moreover, employment is also strongly associated with quality of life, higher self-esteem and fewer psychiatric symptoms.11 In addition, in the context of the global challenges of climate change, an increasing number of scholars have been examining the epidemiological links between mental health and environmental factors. Some studies have suggested that mental health may be influenced by ambient temperature, and an association has been found between environmental pollutants, particularly fine particulate matter and mental health problems.12 A relevant study shows that with short-term exposure to ambient air pollution is associated with increased emergency room visits due to depression or suicide attempts.13 Furthermore, other factors associated with mental health include sleep, diabetes, coronary artery disease and cardiovascular disease.14 15 It is worth noting that job burn-out and occupational stress are closely linked to mental health. Job burn-out is an exhaustion state of physical and psychological that often occurs in the work environment, and has a high correlation with depression. A large study of physicians found that of the 10.3% who met criteria for a major depressive episode, 50.7% were also affected by symptoms of burnout (OR 2.99) and indicated that worsening depression leads to a higher likelihood of burnout symptoms.16 Occupational stress refers to a work environment where non-reciprocity of effort and reward may lead to strong negative emotions and distress. Related research has shown that the combination of high effort and low reward and overcommitment increases the risk of mental health problems such as depression.17 Apparently, it is necessary to include the Chinese Maslach Burnout Inventory (CMBI) and effort–reward imbalance (ERI) in this study to predict the risk of mental health problems among factory workers and miners. However, there are few studies that include these influences in a more comprehensive way in the practice of detecting mental health. Therefore, more accurate identification of mental health problems in populations requires a questionnaire that include a wider range of factors affecting factory workers and miners’ mental health problems.
Factory workers and miners are a special group of workers with a relatively low overall level of education and are highly prone to suffering from mental health problems due to limited social support, excessive workload and irregular lifestyles, as well as occupational hazards such as noise and coal dust that they inevitably need to face in their working environment.18 19 Through a review of the literature, our group found that coal dust, crystalline silica and noise pollution were common causes of health problems for workers in underground mines.20 And, exposure to coal mine dust is a significant cause of pneumoconiosis in coal miners.21 In addition, asbestos is one of the major occupational hazards in the daily work of workers in the construction and automotive industries.22 China has the world’s largest group of factory workers and miners, about 6 million,23 who are regularly involved in occupational hazards. Mental health problems which need to require a long process are known to be a syndrome caused by chronic stress. Factory workers and miners, represented by those engaged in coal mining, have a mental burden rating of 8.3, one of the highest mental burdens among 150 occupations.24 This explains the high level of mental health problems among mine workers in previous studies, making the identification and treatment of mental health problems even more important. Therefore, it is essential to provide a viable and easy-to-apply tool for identifying workers at risk of mental health problems and thus for timely interventions.
There are many studies on mental health25 26; however, the results of previous studies lack consistency and mostly discuss factors influencing mental health, and most of them are single-centre studies that focus on only certain aspects of mental health. Our study included common demographics, job burnout, occupational stress, chronic illness and occupational exposure factors to distinguish whether respondents suffered from mental health problems. In addition, there is a small body of literature that develops and validates a risk nomogram between depression and suicide to support timely intervention by clinicians. And the sample sizes of the two relevant studies were small, 474 and 273 depressed patients, respectively.27 28 Today, there is increasing recognition of the important role of mental health in achieving global development goals, and WHO has included mental health in the Sustainable Development Goals. However, there are no relevant studies that have used objective indicators for factory workers and miners to form a nomogram to predict mental health. Therefore, to bridge this gap in the literature and provide additional information for the prevention of mental health problems, we conducted a multicentre investigation to develop and validate an easy-to-use nomogram that combines objective information on demographics, job burnout, occupational stress and occupational hazards to comprehensively and accurately predict the prevalence of mental health problems among factory workers and miners.
Materials and methods
Calculation of sample size
The sample size formula for the present illness rate survey,  , p is the present-hazard rate, q=1 p, δ is the tolerance error, generally taken as 0.1 p,
, p is the present-hazard rate, q=1 p, δ is the tolerance error, generally taken as 0.1 p,  is the significance test statistic,
is the significance test statistic,  =1.96 for α=0.05, then the formula is calculated as,
=1.96 for α=0.05, then the formula is calculated as, . A cross-sectional study in Xinjiang showed that 38.27% of factory workers and miners had mental health problems.29 And a study revealed that 633 out of 1675 coal miners (37.8%) suffered from mental disorders between August 2018 and June 2019.30 In this study, we assumed a 30% prevalence of mental health problem to obtain the maximum required sample size. which would calculate a sample size of 934, taking into account non-response and a 20% loss of questionnaires, which would require approximately 1168 people.
. A cross-sectional study in Xinjiang showed that 38.27% of factory workers and miners had mental health problems.29 And a study revealed that 633 out of 1675 coal miners (37.8%) suffered from mental disorders between August 2018 and June 2019.30 In this study, we assumed a 30% prevalence of mental health problem to obtain the maximum required sample size. which would calculate a sample size of 934, taking into account non-response and a 20% loss of questionnaires, which would require approximately 1168 people.
Participants
Participants in this cross-sectional survey were factory workers and mines in the Urumqi region, and the survey covered all districts and counties in the Urumqi region to avoid selection bias as far as possible. Specifically, this survey was conducted by means of whole-group random sampling from January to May 2019, and a total of 202 enterprises were selected, including 21 in Tianshan District, 30 in Shaibak District, 24 in Xinshi District, 22 in Shuimogou District, 56 in Jingkai District, 37 in Midong District, 9 enterprises in Dabancheng District and 3 enterprises in Urumqi County.
The inclusion criteria were as follows: (1) workers working in mining enterprises or factories in Urumqi; (2) workers with a history of working for more than 1 year; (3) Workers with no history of mental illness and no history of taking psychotropic drugs.
The exclusion criteria were the following: (1) factory workers and miners in non-Urumqi area; (2) working history of factories and mining enterprises less than 1 year; (3) a confirmed diagnosis of a mental health problem and a history of treatment and use of psychotropic medication and (4) Questionnaires with missing data were excluded.
An online electronic questionnaire was created using the Questionnaire Star platform to collect data. In the introductory section of the electronic questionnaire, we provide a paragraph stating that volunteers can choose to continue answering the survey if they wish to participate and the relevant data will be used for scientific research, or refuse to answer if they do not wish to participate in the survey. In addition, this survey was conducted by trained surveyors who explained the purpose, meaning, content and requirements of the questionnaire to all participants and provided on-site instructions to ensure the return rate of the questionnaire. All participants understood the purpose of the study and were willing to participate in the study. A total of 7500 questionnaires were distributed and 7315 questionnaires were returned, representing a return rate of 97.5%. After checking the validity and integrity of the questionnaires, 7118 questionnaires were confirmed as valid, with an effective rate of 97.3%. A total of 7118 participants met the inclusion criteria and the data were randomly divided into a training group (n=4955) and a validation group (n=2163) (figure 1).

Flow diagram of the participants involved in this study.
Research methods
Assessment of mental health
The Symptom Checklist 90 (SCL-90), designed by Derogatis et al, was widely used in the mental health field,31 which contains 90 items across nine dimensions: somatisation, obsessive–compulsive symptoms, interpersonal sensitivity, depression, anxiety, hostility, horror, bigotry and mental illness. The SCL-90 has been used extensively in previous studies and has relatively high reliability and validity.32 The questionnaire uses a Likert 5-point scale, with a score of 0 point indicating none and 4 points indicating severe. A total score above 160, a score above 2 on any item, or a positive item above 43 indicates the presence of a psychological abnormality.33 In this survey, Cronbach’s α was 0.99, the half-reliability coefficient was 0.98 and the Kaiser-Meyer-Olkin (KMO)was 0.994.
Assessment of occupational stress
This survey evaluated occupational stress in factory workers and miners through the ERI model developed by Siegrist.34 The ERI scale consists of three subscales: effort (E, 6 items), reward (R, 11 items) and over commitment (6 items), for a total of 23 items. A Likert 5-level scoring method (1, ‘highly disagree’ to 5, ‘highly agree’) is used to grade the items in the questionnaire with the same weight for each item. The Effort–Return Index ERI=E/R×C, where C is the adjustment coefficient, and the value is 6/11. ERI values greater than 1, equal to 1, and less than 1 correspond to high pay–low return, pay–return balance and low pay–high return, respectively. Moreover, the higher the ERI value, the greater the occupational stress.35 In this survey, Cronbach’s α was 0.94, the half-reliability coefficient was 0.93 and the KMO was 0.956.
Assessment of job burn-out
In this survey, the CMBI revised by Li et al was used to assess job burn-out, which has good reliability and validity.36 CMBI is composed of 15 items in 3 dimensions: emotional exhaustion (5 items), depersonalisation (5 items) and reduced personal accomplishment (5 items). The score for each item ranges from 1 to 7, with 1 point indicating complete compliance and 7 points indicating complete non-compliance. According to the critical value (emotional exhaustion ≥25, depersonalisation ≥11, personal achievement reduction ≥16), the levels of occupational burnout are divided into none (all aspects are below the critical value), mild (any one aspect is equal to or above the critical value), moderate (any two aspects are equal to or higher than the critical values) and severe (three aspects are equal to or higher than the critical values).37 In this survey, Cronbach’s α was 0.89, the half-reliability coefficient was 0.86 and the KMO was 0.919.
Candidate predictors
Trained investigators obtained information on demographics, job burn-out, occupational stress, mental health and occupational exposure factors through on-site face-to-face collection of an electronic version of the questionnaire. Covariates included in this study: (1) demographic information: gender, ethnicity, education level, professional title, work schedule, marital status, monthly income, age, working years, labour contracts, working hours per day and working hours per week; (2) occupational exposure factors: coal dust, silica dust, asbestos dust, benzene, lead, noise and brucellosis; (3) questionnaires: ERI, CMBI; (4) chronic diseases: diabetes, hypertension. Information on four areas, including demographic information, questionnaires, occupational hazards and chronic diseases, were filled in by participants through their own responses on the questionnaire star.
Sex was defined as male or female; ethnicity was defined as Han and other; education level was defined as junior high school and below, high school, junior college or bachelor’s degree or above; labour contracts was defined as signed or unsigned; professional title was defined as no, primary, middle or senior; work schedule was defined as day shift, night shift, shift or day and night shifts; marital status was defined as unmarried, married, divorced or widowed; monthly income (yuan) was defined as <¥3000, ¥3000, ¥4000, ¥5000, ¥6000, ¥7000 or ¥8000; age (years) was defined as <25, 25, 30, 35, 40 or 45; working years was defined as 5, 5, 10, 15, 20, 25 or 30; working hours per day (hours) was defined as ≤7 or >7; working days per week (days) was defined as ≤5 or>5; exposure to coal dust, silica dust, asbestos dust, benzene, lead, noise, brucellosis were all defined as yes or no; ERI was defined as yes or no; CMBI was defined as none, mild, moderate and severe; hypertension and diabetes were both defined as yes or no.
Statistical analysis
Categorical variables were described as counts and percentages, and χ2 test or Fisher’s exact test was used to compare categorical variables between groups. Seventy per cent of participants were randomly assigned to the training cohort and 30% to the validation cohort. Variables were screened using a least absolute shrinkage and selection operator (LASSO) regression and multivariate logistic regression models were used to estimate risk ratios and corresponding 95% CIs of risk factors, from which predictive models were constructed. A nomogram for predicting was generated according to the selected characteristics. In addition, forest plot was drawn to visually depict the p value, OR and 95% CI for the selected validations. Statistically significant predictors were applied to develop a prediction model for the risk of mental health problems among factory workers and miners by introducing all selected factors and analysing the statistical significance levels of them. We used calibration plots and receiver operating characteristic (ROC) curves to show the calibration and discrimination of our final model. Brier scores for overall performance, calibration slopes were used to assess the predictable accuracy of the model. Decision curve analysis (DCA) was applied to calculate the net benefit of the nomogram. Statistical analysis was performed using the open-source R software V. 3.6.1 (http://www.r-project.org). The significance level (α) set at 0.05.
Patient and public involvement
Neither patients nor members of the public had any involvement in the design of this study.
Results
Participant characteristics
A total of 7118 participants met the inclusion criteria and the data were randomly divided into a training group (n=4955) and a validation group (n=2163). Over half of all participants (65.31%) were male, 57.31% of the population was over 35 years of age and 78.32% of the subjects were married, showing that factory workers and miners are generally older and most of them have spouses. The majority of them had completed high school (83.94%), while a smaller percentage had completed undergraduate education (22.98%), indicating that the group of factory workers and miners as a whole was not well educated. The total number of workers (n, %) exposed to coal dust, silica dust, asbestos dust, benzene, lead, noise and brucellosis in the factory and mining enterprises were 377 (5.3), 730 (10.3), 981 (14), 1981 (27.8), 373 (5.2), 4942 (69.4) and 121 (1.7), respectively, with the total number of workers exposed to noise amounting to 4942, or 69% of the total population surveyed. The demographic, job burn-out, occupational stress and occupational exposure factors for the training and validation groups are shown in table 1. The results showed that there were no significant statistical differences between the two groups of characteristic variables, except for coal dust and CMBI, indicating that the baseline levels were largely consistent between the two groups.
Characteristics of the study participants
Feature selection
The lambda was smallest at 0.01801 as seen from the lasso results when there were 12 characteristics, which were education, professional title, age, CMBI, ERI, asbestos dust, hypertension, diabetes, working hours per day, working years, marital status and work schedule based on the results of the questionnaires on demographics, occupational stress, job burn-out and occupational exposure factors (figure 2).

Feature selection using the LASSO binary logistic regression model. (A) Feature selection for the LASSO binary logistic regression model. The partial likelihood deviation (binomial deviation) curve was plotted against lambda by validating the optimal parameter lambda in the LASSO model. Dotted vertical lines were drawn based on 1 SE of the minimum criteria (the 1-SE criteria). (B) Feature selection was performed using the LASSO binary logistic regression model. A coefficient profile weas plotted based on the lambda series in (A), and 12 features with non-zero coefficients were selected by optimal lambda. CMBI, Chinese Maslach Burnout Inventory; ERI, effort–reward imbalance; LASSO, least absolute shrinkage and selection operator.
Results of logistic regression model
The 12 features obtained from the LASSO regression were incorporated into a multivariate logistic regression model and the regression results were shown in table 2. It was clear from the results that education, professional title, age, CMBI, ERI, asbestos dust, hypertension, diabetes, working hours per day, working years, marital status and work schedule were independent determinants of risk for mental health problems. In addition, there was no evidence of multicollinearity between the covariates included in the model. The forest plot showed that the selected 12 features all contain items with p<0.05, among which the degree of severe of CMBI (OR, 19.84; 95% CI, 13.88 to 28.34; p<0.001) had the greatest impact on the risk of mental health problems among factory workers and miners (figure 3).
Predictive factors of risk for mental health problems among factory workers and miners

The forest plot of the or of the selected feature. CMBI, Chinese Maslach Burnout Inventory; ERI,effort–reward imbalance.
Development of an individualised prediction model
Based on the results of the multivariate analysis, predictors such as education, professional title, age, CMBI, ERI, asbestos dust, hypertension, diabetes, working hours per day, working years, marital status and work schedule were included in the nomogram. A model incorporating the above independent predictors was developed and represented as a nomogram in figure 4. Each variable in nomogram was assigned a score, and the cumulative sum of each ‘point’ was the ‘total score’. The ‘total score’ corresponded to the ‘predictable likelihood’, which was the predicted probability of mental health problems among factory workers and miners as suggested by our design of the nomogram.

Developed mental health problems incidence risk nomogram. The mental health problems incidence risk nomogram was developed in the array, with education, professional title, age, CMBI, ERI, asbestos dust, hypertension, diabetes, working hours per day, working years, marital status, and work schedule incorporated. CMBI, Chinese Maslach Burnout Inventory; ERI, effort–reward imbalance.
As an example of the use of nomogram: a randomly selected sample from the training group, one with no professional title, day shift, no diabetes or hypertension, Junior college, <5 of working years, >7 of working hours per day, married, no exposed to asbestos dust, <25 years of age, no ERI, mild of CMBI, with a calculated total score of 174 and a corresponding risk probability of 8.27% for mental health problems.
The validation of calibration
Model validation was carried out in the validation group. The prediction accuracy of the model was assessed by two aspects. (1) The Brier score for overall performance, which assessed the difference between observed and predicted values, with values closer to 0 indicating better predictive ability. (2) The calibration slope used for modal calibration, which assessed the agreement between the observed and predicted values, with values closer to 1 indicating better performance. The accuracy measurements for the bias correction were validated by the model with a Brier score of 0.176 and a calibration slope of 0.970, respectively (figure 5). The prediction accuracy of the model was relatively high.

Calibration curves of the mental health problems incidence risk nomogram prediction in validation group. The x-axis represents the predicted risk of mental health problems. They-axis represents the actual diagnosed risk of mental health problems. The diagonal dashed line represents the perfect prediction of the ideal model. The solid lines represent the performance of the column plots, where closer to the diagonal dashed line indicates a better prediction. ROC, receiver operating characteristic.
The validation of discrimination
ROC was plotted for the training and validation groups, and the area under the curve (AUC) of training and the verification groups were 0.785 and 0.784, respectively (figure 6). The AUC of training and the verification groups were both greater than 0.750, showing a good discrimination.

ROC curves for training and validation groups. The y-axis represents the true positive rate of risk prediction. The x-axis represents the false positive rate of risk prediction. The ROC curves for the training and validation groups are shown in black and red. ROC, receiver operating characteristic.
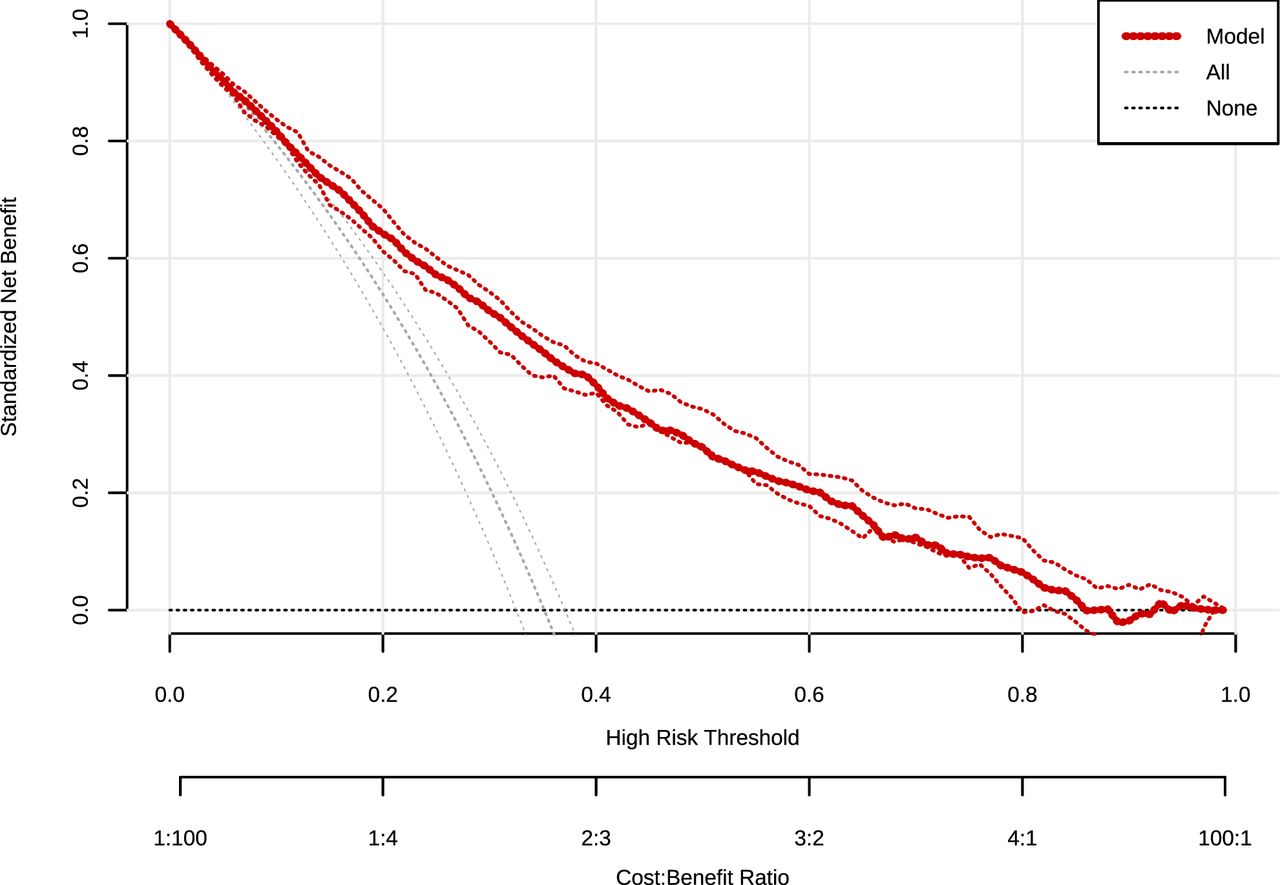
Decision curve analysis
As shown in the DCA of the risk of mental health problems nomogram in figure 7, the model for predicting the risk of mental health problems for factory workers and miners in this study was more practically relevant if the threshold probability of patients was >10%.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Decision curve analysis (DCA) for mental health problems incidence risk nomogram. The y-axis measures the net benefit. The solid red line represents nomogram of the risk of developing a mental health problem. The light blue dashed line represents the hypothesis that all participants were diagnosed with a mental health problem. The black dashed line represents the hypothesis that there is no risk of a mental health problem. The DCA showed that using this mental health problem incidence risk nomogram in the current study to predict mental health problem incidence risk increase in benefit than the intervention all patients or no intervention all patient if the threshold probability of a patients and a doctor is >10%.
Discussion
To our knowledge, this is the first study to develop an easy-to-use nomogram to predict the mental health risks of factory workers and miners. The nomogram developed using the training set data contain 12 items for education, professional title, age, CMBI, ERI, asbestos dust, hypertension, diabetes, working hours per day, working years, marital status and work schedule. In addition, validation has shown that nomogram model has good accuracy and discriminatory power. Our novel nomogram can be used in any setting to provide a rapid assessment of mental health risks and to help identify patients with mental health risks, saving time compared with previous mental health investigations and improving on the lack of entries in previous investigations related to the specific working environment of factory workers and miners. The AUC of training group and verification group were 0.785 and 0.784, respectively, showing moderate discriminatory and calibration power.
A review of the literature found that the vast majority of studies constructed nomograms to predict clinical disorders, with less literature used to predict psychological problems. In a study to predict the correlates of suicide attempts in a Chinese population with major depressive disorder, the C-index was 0.715 and the C-index in the internal validation set was 0.703, and the calibration curve of the column line plot also showed good agreement between the predicted and observed risk of suicide attempts. The variables in the nomogram included socio-demographic information and clinical variables including age, duration, number of episodes, age at onset, number of hospitalisations, characteristics of anxiety and psychiatric symptoms, marital status, income, education level and employment status.27 In another study that created a nomogram to predict the risk of psychosocial and behavioural problems in children and adolescents during the COVID-19 pandemic, the C index exceeded 0.800 and the calibration curve also showed good predictive accuracy. The variables covered three subject areas, namely demographic information, the psychosocial impact of the epidemic such as homework time and sedentary time, and the Child Behaviour Checklist score for the evaluation of psychological problems.38 In this study, 7118 participants were randomly divided into a training group (n=4955) and a validation group (n=2163) in a ratio of 3:1, involving a total of 23 features and 12 features were selected by LASSO regression. The nomogram could be a useful tool to better identify patients with mental health problems, as it not only covered comprehensive information, including demographic information, job burn-out, occupational stress, chronic diseases and occupational exposure factors closely related to factory workers and miners, but also was simple to operate and easy to use. In the validation group the Brier score was 0.176, the calibration slope was 0.970 and the calibration curve of nomogram showed a good fit. The AUC of training group and verification group were 0.785 and 0.784, respectively. Compared with the two studies above, our nomogram showed good accuracy and discrimination, and more comprehensive coverage in this nomogram model. Therefore, the possibility of early intervention for patients with high-risk mental health problems will be increased by covering multiple information and easy to use nomogram modal, especially for factory workers and miners with poor working conditions, relatively low levels of education and low patience.
Mental health problems were very common in the group of factory workers and miners, and the prevalence of mental health of them was found to be 37.08% in our study. Notably, the CMBI showed the most significant score (score=100) and the ERI also had a high score (score=43) in mental health problem incidence risk nomogram, which indicated that both of them were relatively important factors for mental health problems among the group of factory workers and miners. Our finding was consistent with other studies that had shown that occupational stress was a significant predictor of anxiety and was negatively associated with mental health. In addition, there is a high correlation between burnout and depression.39
In line with previous studies, working years was also an important influential factor in this study. Related study has shown that employment could improve patients’ mental health, while unemployment could lead to a deterioration in mental health.40 In China, workers’ working years is an important aspect of employment, and researchers have studied this aspect and found that precarious employment is a source of stress for individuals and predisposes them to mental health problems.41 In addition, environmental factors were also one of the influential factors of mental health problems in our study. Relevant studies have found that exposure to air pollution is associated with increased suicide risk and depressive symptoms.42 Hypertension and diabetes were the influential factors in this study. A study has shown that the prevalence of depression in adults with type 1 diabetes is approximately three times higher than in the non-diabetic population.43 Furthermore, there is a recognised association between hyperglycaemic and depression, but the underlying biological mechanisms of this association are unclear.44
Factory workers and miners were inevitably exposed to occupational hazards such as benzene and asbestos dust in their working environment. According to statistics, a total of nearly 2 million workers are exposed to various occupational hazards and over 16 million people worked in toxic and hazardous enterprises, involving more than 30 different types of operations, of which factory workers and miners is the one.29 Similarly, the occupational hazard asbestos dust was selected as a predictor of risk for mental health problems in this study. Our study found that the work schedules of factory workers and miners were vary and the phenomenon of night shifts was very common, which inevitably affected their normal sleep. Some studies have shown that sleep problem is a risk factor for a variety of mental health and chronic diseases. Lack of sleep or poor sleep quality could lead to abnormalities in the body’s self-regulatory functions and disturbances in the circadian rhythm of the biological clock, which in turn could suffer from negative emotions such as anxiety and depression.45 Professional title and education level were also important influences on mental health issues. In the workplace, generally speaking, the higher the professional title and education level, the higher the status of the worker in the company and the greater the role played in the position. The number of studies on socioeconomic status and mental health had increased in recent years. Some of these studies have shown that major depression is higher in the low socioeconomic status group.46 It has also been suggested that education itself is the best indicator of socioeconomic status.47 Marital status was one of the influential factors for mental health problems. Many studies have found an association between mental health and gender, marital status, lifestyle and working conditions, and it has been shown that poor mental health in women is associated with divorce or widowhood.48 In this study, working more than 7 hours a day was a determinant factor on mental health problems, which was consistent with other studies that had shown that long working hours could have a negative impact on employees' mental health and that excessive workloads could increase workers’ fatigue, which in turn could lead to anxiety and depression.49
In China, there are many problems in identifying people with mental health problems due to uneven and imperfect levels of medical development across regions. Some studies have shown that in mainland China, general practitioners, surgeons and primary healthcare workers often have little or no mental health training, which prevents them from providing basic mental health services.50 Non-mental health professionals in general hospitals learn about mental illness on their own, rather than learning about it during their formal education.51 Therefore, this study designed a simple and comprehensive nomogram to address the issue of timely detection and effective interventions for people with mental health problems, so that people at risk of mental health problems could easily calculate their probability of suffering from mental health problems without the help of medical staff. This study has several strengths. First, to our knowledge, this is the first model to develop and assess the likelihood of mental health problems in a group of factory workers and miners. Second, the nomogram in this study includes demographic information, job burnout, occupational stress, chronic illnesses and also occupational exposure factors that are closely related to factory workers and miners, allowing for a more accurate assessment of the risk of morbidity among them, as well as providing a methodological reference for other related studies.
Limitations
This study also has several limitations. First, we have considered many influential factors including demographics, job burnout, occupational stress and occupational exposure factors, but we are still not certain whether all possible influences are covered. Second, while the robustness of our nomogram was extensively validated internally in the same population, external validation is lacking for other populations in other regions and countries. Nomogram needs to be externally assessed in a wider population.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
The study was approved by the ethics committee of Urumqi Center for Disease Control and Prevention 20181123. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The authors are grateful to all participants and investigators.
References
Footnotes
YL and QL contributed equally.
Contributors YL, QL and TL are responsible for conceptualisation, and TL is the guarantor for the article; YL is responsible for methodology, software, formal analysis, resources and visualisation; QL and TL are responsible for the original draft preparation; QL and HY are responsible for reviewing; QL is responsible for editing; TL is responsible for supervision.
Funding This work was supported by the Natural Science Foundation of Xinjiang Uygur Autonomous Region (grant number 2020D01A27), the Postgraduate Innovation Project of Xinjiang Uyghur Autonomous Region (grant number XJ2021G215), the Outstanding Young Scientist Training Programme of Urumqi Science and Technology Talent Project (grant number N/A), Public Health and Preventive Medicine - Specialties of Higher Education Institutions in Xinjiang Uygur Autonomous Region in the 14th Five-Year Plan (grant number N/A).
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.