Article Text

Abstract
Objective The COVID-19 pandemic necessitated the use of telemedicine to maintain continuity of care for patients with cardiovascular diseases (CVDs). This study aimed to demonstrate the feasibility of implementing a nurse-led teleconsultation strategy for CVD management during the COVID-19 pandemic in India and evaluated the impact of nurse-led teleconsultations on patient treatment satisfaction.
Design, setting and participants We developed a two-stage teleconsultation strategy and tested the feasibility of implementing a nurse-led teleconsultation strategy to manage CVD in a northern state (Punjab) in India. A multidisciplinary team of experts developed the treatment protocol used for teleconsultations to manage CVD. Nurses were trained to provide teleconsultation, triaging of patients and referrals to the physicians. Patients with CVD who had an outpatient visit or hospitalisation between September 2019 and March 2020 at the Dayanand Medical College Hospital, Ludhiana, India, were contacted by phone and offered teleconsultations. Telemedicine strategy comprised: stage 1 nurse-led teleconsultations and stage 2 physician-led teleconsultations. Descriptive analysis was performed to report the proportion of patients triaged by the two-stage telemedicine strategy, and patient’s clinical characteristics, and treatment satisfaction between the nurse-led versus physician-led teleconsultations.
Results Overall, nurse-led stage 1 teleconsultations were provided to 12 042 patients with CVD. The mean (SD) age of the participants was 58.9 years (12.8), and men were 65.4%. A relatively small proportion of patients (6.3%) were referred for the stage-2 physician-led teleconsultations and of these only 8.4% required hospitalisations. During stage 1 nurse-led teleconsultations, patients were referred to the physicians due to uncontrolled diabetes (24.9%), uncontrolled hypertension (18.7%) and congestive heart failure (16.2%). The patient’s treatment satisfaction was similar between the nurse-led versus physician-led teleconsultations (p=0.07).
Conclusion This study showed that a nurse-led telemedicine strategy is feasible to implement in a resource-constraint setting for triaging patients with CVD and reduces physician’s burden.
- telemedicine
- adult cardiology
- coronary heart disease
- organisation of health services
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This is one of the first studies from India that evaluated the role of nurse-led telemedicine strategy for cardiovascular disease care during the COVID-19 pandemic, with a large sample size.
By systematically conducting telephone follow-ups with patients in a two-step approach, we were able to demonstrate a pyramid-based care delivery model, where only few patients required physician consultations and hospitalisation.
Another strength of this study is the use of standardised treatment protocol, and data collection instruments for all patients and rigorous training provided to the nurses and physicians involved in the implementation of telemedicine strategy.
An important limitation of this study is that the findings are solely based on a single-centre implementation of telemedicine strategy, which may not be generalisable to other populations.
Introduction
The COVID-19 pandemic has led to emergence of several challenges in providing care to both chronic and newly diagnosed patients with cardiovascular diseases (CVDs). In India, the first COVID-19 confirmed case was detected in the state of Kerala on 30 January 2020.1 In view of its worldwide spread, WHO declared COVID-19 outbreak as pandemic on 11 March 2020.2 In the wake of COVID-19 pandemic, a nationwide lockdown was imposed on 25 March 2020 by the Indian government. During the complete lockdown for more than 2 months, only the emergency services were allowed while maintaining the social distancing norms. Given the high prevalence of CVD in India (>54 million),3 the nationwide COVID-19 pandemic related lockdowns have impacted the care by preventing both routine inpatient and outpatient care.
Furthermore, the COVID-19 pandemic-related mobility restrictions, non-availability of nearby healthcare facilities especially in rural areas, need for social distancing, patients’ fear of acquiring infection from healthcare facilities, necessitates the use of telemedicine strategy to provide timely care for patients with CVD. Telemedicine refers to providing remote essential medical consultations aided by the advanced technology. In India, telemedicine is not a popular mode of providing healthcare services due to physician’s time constraints, less familiarly with the telemedicine principles and technology and partly due to the absence of standard guidelines on the application of telemedicine for CVD management. The pyramid model has been previously used in public health programme.4 Traditionally, a four-tier pyramid is depicted by the population wide interventions with maximum impact at base followed by primary, secondary and tertiary interventions in that order tapering up to the apex of it.5 We proposed a three-tier pyramid model to deliver teleconsultations for patients with CVD during a pandemic situation within the already constraint healthcare delivery system. The base of the pyramid is represented by the nurse-led teleconsultation for screening bulk of the patients followed by the waist represented by the physician-led teleconsultation and the apex represented by the tertiary care referral. This study describes the implementation of a nurse-led teleconsultation strategy to manage CVD during the COVID-19 pandemic and related lockdowns in India and evaluate the impact of nurse-led telemedicine strategy on patient’s treatment satisfaction.
Methods
Study setting and population
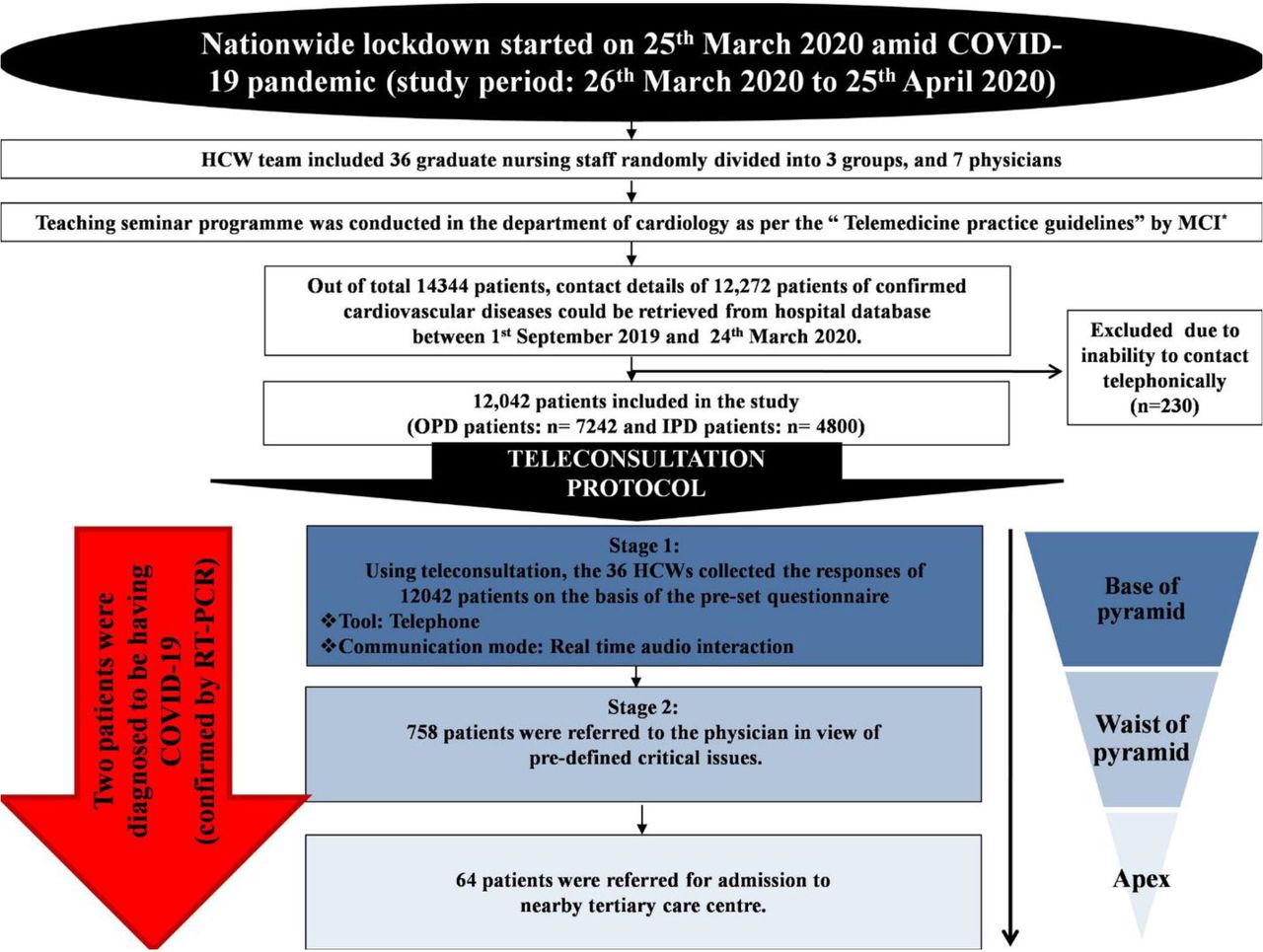
This study was conducted in a northern state (Punjab) in India during the first wave of COVID-19 pandemic and ensuing nationwide lockdown over 4 weeks between 26 March 2020 and 25 April 2020. We gathered the contact information of all the patients with CVD who attended the Dayanand Medical College (DMC) hospital, Ludhiana, Punjab, India in the past 6 months, that is, between 1 September 2019 and 24 March 2020 as these patients were expected for the next clinic visit. All patients with CVDs including coronary heart disease, heart failure, hypertension, peripheral vascular diseases, cardiomyopathies and arrhythmic disorders were included in this study. The patients with mechanical prosthetic valve or those receiving oral anticoagulation therapy were excluded from the study as these patients attended a dedicated Valve clinic at the DMC Hospital and were followed up using a different treatment protocol conducted in a separate research study.6 Of the total 14 344 patients who had previously attended DMC hospital between Sep 2019 and Mar 2020, the full contact details of 12 042 patients could be retrieved. All these patients constituted the sampling frame for this nurse-led teleconsultation-based feasibility study. Of these, 7242 patients had attended the outpatient facility and 4800 patients had a recent hospital admission. The detailed medical records of all in-patient department (IPD) patients were retrieved from the hospital database. The study design and sample selection are shown in figure 1.
{kind=link}
Flow chart of the study design. For hypertension: critically high (SBP ≥160 mm Hg and DBP ≥100 mm Hg), Intermediate high (SBP 130–159 mm Hg and DBP 80–99 mm Hg), controlled (SBP<130 mm Hg and DBP<80 mm Hg). For Diabetes: critically high (RBS ≥300 mg/dL), intermediate high (RBS 200–299 mg/dL), controlled (RBS <200 mg/dL). DBP, diastolic blood pressure; DM, diabetes mellitus; HCWs, healthcare workers; HTN, hypertension; IPD, inpatient department; OPD, outpatient department; RBS, random blood sugar; RT-PCR, reverse transcription PCR; SBP, systolic blood pressure.
Nurse-led teleconsultation strategy
Given the ubiquitous use of mobile phones and relative paucity of video enabled smart phones or tablets, we used simple mobile phones as the tool for teleconsultation services. The real-time audio interaction was the preferred mode for care delivery. The teleconsultation-based care delivery was implemented by a team of trained healthcare workers (HCWs) consisting of 36 nursing staff randomly divided into three groups, and seven consultants in the field of medicine. As per the teleconsultation guidelines endorsed by the Indian Ministry of Health and Family Welfare, we conducted a 1-week long teaching seminars for the physicians and nurses to standardise our treatment protocols and to improve their understanding of the teleconsultation principles used in this study.7 The patients’ records were retrieved and reviewed by the trained nursing staff from the hospital medical records and electronic database from the last 6 months (September 2019–March 2020). Teleconsultation approach comprised of two stages. During stage 1, all patients (n=12 042) were teleconsulted using the prespecified questionnaire (online supplemental file 1) by 36 nursing staff. The stage 1 questionnaire was focused on patient’s demographic information, clinical symptoms, recent values of blood pressure (BP), and blood glucose, medicines-related issues, exercise and patients’ well-being score (0–10). This stage 1 was led by nursing staff and supervised by a physician in-charge. In the next stage (stage 2), based on predefined cut-offs the patients shortlisted by the nursing staff were referred for teleconsultation by physicians. In stage 2, the physician-led teleconsultation focused specifically on the clinical complaints for which the patients were referred after screening from stage 1 and were either teleconsulted as per the guidelines or were referred to nearby tertiary care centre as per the clinical condition. This study used the previously described three-tiered pyramid model approach for teleconsultation: pyramid base was formed by stage 1, waist formed by stage 2, and apex formed by the patients referred for the hospital admission at tertiary care centre.
Supplemental material
Data collection and measurements
All the patients were equally distributed to 36 trained nurses. We administered a set of questionnaires to collected patient-reported outcomes, the response of which was recorded telephonically. Briefly, the questionnaire focused on the clinical symptoms, BP control status (BP recorded within last 1 week), diabetes control status (blood sugar level recorded within last 2 weeks), medication availability and compliance to that, medication history and well-being score. The patients were asked to get themselves checked for BP and random blood sugar (RBS) level either by home monitors (if available) or from nearby clinic/ laboratory and provide the information to the interviewer on a follow-up interview. The patient well-being score used was an 11-point score ranging from 0 to 10 that was categorised as: very high (9–10), high (7–8), medium (5–6) and as low (0–4).8 A contact number of a mobile number was provided to all the patients as a 24-hour help-line number to ensure medical assistance whenever needed.
Fever was defined if body temperature was ≥38°C. Influenza-like illness was defined as ‘an acute respiratory illness with a measured temperature of ≥ 38°C and cough, with onset within the past 10 days’.9 For BP, the controlled status was defined as systolic BP (SBP) of ≤130 mm Hg and diastolic BP (DBP) of <80 mm Hg while BP cut-off for physician’s referral (labelled as critically high) was defined as SBP of ≥160 mm Hg and DBP ≥100 mm of Hg. BP readings in between these values were defined as intermediate high. For diabetes mellitus, controlled status was defined as RBS <200 mg/dL while the RBS cut-off for physician’s referral (labelled as critically high) was defined as ≥300 mg/dL. The RBS readings in between these values were defined as intermediate hyperglycaemia. These limits were defined based on expert consensus meeting. Regular exercise was defined if the patient was doing yoga as advised at the time of discharge or at least >30 min of moderate activity10 for at least five times a week (preferably daily). The compliance to medication was referred to the adherence to the medication for the last 2 weeks prescribed to the patient.11
Further, in a randomly selected subsample of 1200 patients from the study population we assessed the difference in patient’s perceived treatment satisfaction between the nurse-led teleconsultations and physician-led teleconsultations. This subset of patients were distributed among the nursing staff and physicians. All these patients were tele consulted by using a pretested questionnaire (online supplemental file 2) to assess: (1) patient satisfaction level with nurse-led vs physician-led teleconsultations and (2) impact of COVID-19 pandemic on CVD patients. A modified version of the treatment satisfaction questionnaire for medication12 was used to assess the treatment satisfaction in the preceding 30 days.13 The patient’s level of satisfaction with was assessed on a scale of 0–6, where 0=very dissatisfied and 6=very satisfied. The impact of COVID-19 on the patient’s mental health was assessed using a pre-tested questionnaire and it focused on the stress from work or other responsibilities, ability to cope with the ongoing pandemic stress and overall health status on a scale of 0–100.
Supplemental material
Statistical analysis
We used SPSS statistics V.16.0 for windows for data analysis. The continuous variables were expressed as mean±SD and median (IQR) for normally distributed or skewed data, respectively. Categorical variables were expressed as percentage (%). The statistical difference between the treatment satisfaction levels for the teleconsultation by physician and nursing staff was performed by using Mann-Whitney U test as the data were skewed. The skewness of the given data was checked with Kolmogorov-Smirnov test. The difference between two variables was considered significant if the two-sided p value was <0.05.
Patient and public involvement
Patients and community members were not directly involved in the development of the telemedicine-based treatment protocol. However, the study was explained to the participants and verbal consent obtained prior to provision of teleconsultations and study related data collection.
Results
Overall, 12 042 patients who previously attended either outpatient department (OPD) or IPD between September 2019 and March 2020 at the DMC hospital, Punjab, were invited to participate in this study. The schematic flow of patients screened and provided teleconsultations at various stages of this pyramid-based healthcare delivery model utilising nurse-led teleconsultations (stage 1) and physician-led teleconsultations are shown in figure 1. Of the total 14 344 patients eligible for the teleconsultations, contact details of 12 272 patients with CVD were obtained, and of these 12 042 consented to participate in this study. Of these, 7242 patients (60%) were from the OPD and 4800 (40%) patients were from the IPD. The study participants’ demographic and clinical characteristics are shown in table 1. The mean (SD) age of the participants was 58.9 years (12.8) and about two-thirds were men. The most common comorbidities reported were hypertension (45.8%) and diabetes (41.9%). Very few participants (≤1% each) reported clinical signs or symptoms such as chest pain, breathlessness and palpitations. Nearly half of the study participants were monitoring BP at home and one-third participants (reported self-monitoring for blood glucose. In addition, relatively small proportion of participants required referral to the physicians due to uncontrolled BP or uncontrolled blood glucose. Difficulty in access to medicines was reported by nearly 5% patients with CVD during the COVID-19 pandemic. The difficulty in access to medicine was attributed to multiple factors such as non-availability of the local pharmacies in the villages (most of the study participants were from villages), non-availability of few specific cardiac medicines in the nearby pharmacies or due to the absence of a caregiver or helping hands in the family. The self-reported adherence or compliance to prescribed therapy was significantly high (>87%) and two-thirds of the study participants reported performing regular physical activity. However, less than half of the participants with CVD reported taking cardioprotective drugs such as aspirin, beta-blockers and statins. On 11-point well-being score assessment, most participants reported a relatively high well-being score between 7 and 8.
Characteristics of study participants during the nurse-led stage-1 teleconsultations
Of the total screened participants, a relatively small proportions (6.6%) required the next stage 2physician-led teleconsultations. The most common reasons for the referral to stage-2 physician-led teleconsultations included uncontrolled blood sugar (~25%), uncontrolled BP (19%) and congestive heart failure (16%) (table 2). Of those, who received physician teleconsultations, only a small number (n=64 patients, 8.4%), required hospital admission for diagnostic evaluation and management of acute coronary syndrome or worsening heart failure symptoms. In addition, two patients were identified via teleconsultation to have COVID-19 infection diagnosed by reverse transcription PCR assay.
Reasons for patient referrals to the stage-2 physician-led teleconsultations
Further, the analysis on the impact of COVID-19 pandemic among patients with CVD showed that majority of the respondents (88%) did not feel the stress from work or other responsibilities during COVID-19 pandemic. Also, two-thirds participants reported that they could very easily cope with stress during the pandemic. Overall mean (SD) health status reported by the patients on a scale of 0–100 was 88.4 (6.8) (table 3).
Impact of COVID-19 pandemic on the patients with cardiovascular diseases
Lastly, our analysis focused on the difference in the perceived treatment satisfaction between the nurse-led and physician-led teleconsultations demonstrated that significantly greater proportion of patients reported high satisfaction with the treatment provided using the telemedicine strategy. Importantly, the treatment satisfaction score did not significantly differ between the nurse-led versus physician-led teleconsultations (92.8% vs 95.2%, p=0.075) (table 4). These data suggest that the nurse-led teleconsultations was very well received or accepted by the patients with CVD and was found to be feasible to implement in a resource-constraint setting.
Comparison of patient’s treatment satisfaction between the nurse-led versus physician-led teleconsultations
Discussion
To the best of our knowledge, this is the first study to demonstrate that nurse-led teleconsultation strategy can be successfully delivered to provide timely and effective care for patients with CVD in India during the COVID-19 pandemic. Amidst COVID-19 pandemic, there were several challenges in providing healthcare services like decreased availability of HCWs, shortage of resources and fear of acquiring infection. Due to the restrictions posed by the government authorities in order to decrease virus transmission, access to both elective outpatient and emergency services were restricted.14 This led on to instantaneous and unanticipated cancellation of the face-to-face consultation visits of the patients thereby impeding the delivery of healthcare services for those who needed it.14 Due to lack of health system preparedness and the lack of conventional telemedicine facilities, immediate application of telemedicine which is not routinely used especially in country like India was not possible.15
In this study, despite operational difficulties we were able to rapidly create a team of nursing staff and physicians in a short time and developed standard treatment protocols to provide care for patients with established CVD. It was also important to ensure that rapid response to the COVID-19 pandemic and related lockdown, do not affect the quality of care provided by our team of nurses and physicians, therefore, we conducted appropriate training sessions for the entire team of HCWs and clinicians.16 Furthermore, to expedite the process of teleconsultation, as we envisaged reaching out to large number of patients to provide healthcare services, we created a novel three-tier pyramid model for teleconsultation. Pyramid model has been used in various fields of medicine and for public health action framework,5 as well as an inverted pyramid for improving handover care.17 Apart from the conventional four-tiered pyramid model, Grizzell’s six-tier interventional pyramid model and five-tier health impact model have also been studied in literature.4 This pyramid model-based study clearly demonstrated that large number of patients could be managed by a trained nursing staff, whereas a relatively small proportion of patients required physician consultation and hospital admission. By implementing this pyramid model of healthcare delivery using trained and supervised nurse-led teleconsultations, we could successfully triaged and provided timely care for large number of patients within a short period.
Considering the patient treatment satisfaction score, most patients (92.8%) were satisfied with the teleconsultation strategy, and the patient’s treatment satisfaction level was comparable between nurse-led versus physician-led teleconsultations. These findings are consistent with prior reports that show a good satisfaction level with the use of telemedicine in various disease conditions.18 19 Further, this study demonstrated that nurse-led teleconsultations during pandemic situation when health resources were already overwhelmed, could be of vital importance without compromising the efficacy of the care delivery model. Our pyramid-based model of teleconsultation also identified two confirmed cases of COVID-19 infection and both were referred to nearby tertiary care centre for appropriate care.
Due to the critical nature of CVD, associated comorbidities, elderly patients with multiple disabilities, and with possibility of acute decompensation if left unattended, these patients need frequent and regular monitoring of various health parameters. Thus, the use of telemedicine strategy provided the much-needed healthcare services required to manage these patients with CVD. Several systematic reviews and meta-analyses have shown a significant reduction in mortality and hospital readmissions with the use of telemonitoring among chronic heart failure patients.20–22 Utilisation of telemedicine in ST-segment elevation myocardial infarction care has also shown a substantial improvement in health outcomes.22 The role of telemedicine has also been studied for active surveillance of patients on anticoagulation therapy during COVID-19 pandemic.23 During disaster situation and public health emergency, as imposed by COVID-19 pandemic, the telemedicine strategy not only helps in remote triaging the patients and easy accessibility to routine medical care but also prevents the transmission of virus by decreasing person-to-person contact.24 25
A major limitation of this study is that we have implemented only the audio mode of teleconsultations and physicians expressed some hesitancy in proving teleconsultations on audiomode only. However, in this study, we did not collect qualitative interview data on the experiences of providers delivering care using the telemedicine strategy. Virtual teleconsultation has added advantages like reading the patients’ facial expression, observing some physical signs, perceived psychological satisfaction of the patients.26 27 However, due to low internet connectivity and low penetration of android-based mobile phones in the study location, we could not implement the video bases virtual teleconsultations. On the contrary, the use of telephone-based ‘audio only’ consultation has constituted most virtual visits even in the USA during unprecedented times of COVID-19 pandemic.28 Virtual consultations could certainly be explored for its clinical use in urban and rural areas to further improve the efficacy and impact of teleconsultations as care delivery model.24 29
Implications of study findings
Given the unprecedented and rapidly evolving COVID-19 pandemic situation in India and the need to keep vulnerable patients (and clinicians) at home and away from the healthcare facilities to decrease risk of virus transmission, there has been a rapid increase in use of telemedicine. A new belief on telemedicine strategy requires many clinicians and health workers to develop skills to obtain objective information from these types of telephone visits. Although eliciting a complete medical history and adjudicating medication lists and allergies are crucial activities of teleconsultation visits, additional information from a telehealth physical examination can be useful, if virtual clinic visit can be delivered. A focused general physical examination over the teleconsultation or virtual clinic visits either confirms clues suggested by the patient’s medical history or provides data that can direct specific clinical tests or treatments. Our experience is that patients with CVD respond positively to these initiatives unequivocally to both the nurse-led as well as physician-led teleconsultations. Thus, performance of a teleconsultation strategy to manage patients with CVD may be considered as an essential element in the context of post pandemic healthcare delivery models in India. Given the fragmented and heterogeneous healthcare delivery system in India, with large share of private healthcare market, identifying appropriate reimbursement models to promote telemedicine strategy needs further exploration. Future research may also focus on evaluating the effectiveness of telemedicine on clinical outcomes in a large, randomised trial. Also, the costs of delivering such a nurse-led teleconsultations and pyramid-based care delivery model are currently unknown in the Indian context, so a future study should evaluate the cost of delivering such a care delivery model to inform its nation-wide expansion and scale-up if found to be successful.
Conclusions
This study demonstrated the feasibility to implement a pyramid model-based nurse-led telemedicine strategy during the COVID-19 pandemic and related lockdowns in India. Large number of patients with CVD were given teleconsultations in a stepwise approach with optimal utilisation of the available healthcare providers (ie, trained and supervised nursing staff and physicians), with comparable patient treatment satisfaction level between the nurse-led versus physician-led teleconsultations. Further, to optimise existing healthcare resources a hybrid model of care combining physical clinic visits for critical cardiac care and telemedicine strategy for routine follow-ups based on hub-and-spoke model could be considered, beyond the pandemic and in post-COVID India.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study is approved by the institutional ethics committee of Dayanand Medical College, Ludhiana, Punjab, India Ref. No. DMcH/DrEclzozo/ 677.
Acknowledgments
KS is supported by funding from the Fogarty International Centre, National Institutes of Health (NIH), US (grant award: 1K43TW011164).
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors BM, BS, AG, GS, SA, AS, RT, STC, NA and GSW contributed to the conception and design of the study. BM, BS, KS, NN, AR, DP had a role in the acquisition, analysis or interpretation of data. KS, BS and BM drafted the manuscript, and all authors critically revised the manuscript. All authors provided technical and material support and approved the final manuscript. BM accepts full responsibility for the work and/or the conduct of the study, had access to the data, and approved the decision to publish.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Disclaimer The funding agency had no role in the design, conduct, or analysis of the study, and no role in the decision to submit the manuscript for publication. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.