Article Text

Abstract
Objective To investigate the risk factors for and the consequences (ie, substance use disorders (SUD), depression, personality traits) of traumatic brain injury (TBI) in young Swiss men.
Design This is a three-wave cohort study. Risk factors were measured at baseline (2010–2012) and at follow-up 1 (FU1; 2012–2014), while the consequences and TBI were measured at follow-up 2 (FU2; 2016–2018).
Setting Switzerland.
Participants All participants at FU2 (Mage=25.43, SD=1.25) of the Cohort Study on Substance Use Risk Factors (N=4881 young Swiss men after listwise deletion).
Measures The outcomes measured were TBI, SUD (ie, alcohol, nicotine, cannabis, other illicit drugs), depression and personality traits (ie, sensation seeking, anxiety-neuroticism, sociability, aggression-hostility) at FU2. The predictors were previous TBI (lifetime TBI but not in the past 12 months at FU2), SUD, personality traits and sociodemographics (highest level of achieved education, age, linguistic region) measured at FU1.
Results At FU2, 3919 (80.3%) participants reported to never have had TBI, 102 (2.1%) have had TBI in the last 12 months (TBI new cases), and 860 (17.6%) have had TBI during their lifetime but not in the 12 months preceding FU2 (previous TBI). Low educational attainment (OR=3.93, 95% CI 2.10 to 7.36), depression (OR=2.87, 95% CI 1.35 to 6.11), nicotine dependence (OR=1.72, 95% CI 1.09 to 2.71), high sociability (OR=1.18, 95% CI 1.07 to 1.30), high aggression-hostility (OR=1.15, 95% CI 1.06 to 1.26) and high sensation seeking (OR=1.33, 95% CI 1.04 to 1.68) at FU1 were significantly associated with TBI new cases at FU2. Previous TBI was significantly associated with nicotine dependence (OR=1.46, 95% CI 1.16 to 1.83), depression (OR=2.16, 95% CI 1.56 to 2.99) and aggression-hostility (B=0.14, 95% CI >0.00 to 0.28) at FU2.
Conclusion Low educational attainment and depression are the most significant risk factors associated with increased odds of future TBI, while depression, nicotine dependence and high aggression-hostility are the main consequences of previous TBI. TBI should be considered an underlying factor in the treatment of depression, SUD or unfavourable personality profiles.
- Adult psychiatry
- Substance misuse
- Impulse control disorders
- Personality disorders
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
The study evaluates concomitant risk factors and consequences of traumatic brain injury (TBI) in a large cohort of young Swiss men.
There are many characteristics evaluated across three waves other than TBI, such as personality traits, depression, substance use disorders and sociodemographic characteristics.
The study duration was long, with 8 years from baseline to the second follow-up visit.
Even though there were many characteristics included, we could not control for all possible confounders.
Only young male participants were included, limiting generalisability to female and older participants.
Introduction
Traumatic brain injury (TBI) is defined as an alteration in brain function, or other evidence of brain pathology, caused by an external force.1 It is one of the major causes of injury-related deaths in Europe2 and a source of lifelong disability for many of the survivors.3 A major epidemiological study found significant regional differences in incidence, mean length of hospital stay and admission rates in patients with TBI, while hinting that many patients who suffer TBI and its consequences might go undiagnosed.2 TBI has been associated with an increased risk of neurodegenerative diseases (Alzheimer’s disease, Parkinson’s disease),4 cognitive impairments (attention, memory, arousal, concentration, executive functioning),5 affective disorders, anxiety and psychosis,6–8 substance use disorders,9 and personality changes.10 Putative risk factors for TBI include pre-existing psychiatric illnesses (particularly depression),11 substance use disorders12 and personality disorders,13 low socioeconomic status, male sex, young age,14 and previous head injury.15
It is readily apparent that there is significant overlap and interplay between some of the risk factors and consequences of TBI, namely personality traits, substance use disorders and mental disorders.16 Mood and anxiety disorders occur in higher than average rates both preinjury17 and postinjury,18 with depression being the most prevalent in both cases.11 Antisocial personality disorder, associated with personality features that predispose to at-risk behaviour, such as high impulsivity, aggression and sensation seeking, is a significant risk factor for TBI.13 In turn, changes in personality could arise secondary to TBI.19 Substance use disorders are both a frequent cause and a potential complication of TBI,20 as injury significantly limits access to rehabilitation and recovery services. Some studies have reported higher than average rates of preinjury11 and postinjury20 alcohol and drug abuse, while others suggest that substance use patterns are not significantly influenced by TBI.21 22
Young men are disproportionately affected by TBI,23 with the male to female ratio ranging from 1.2:1.024 to 4.6:1.025; therefore, it is particularly important to investigate the causes and consequences of TBI in this group. Risk factors particular to this population include mental disorders,13 14 low socioeconomic status,26 low cognitive function,27 alcohol or substance use disorders,11 12 and the predilection to engage in high-risk activities and behaviours, such as professional contact sport, construction and military.28–30
Drawing on previous research, we selected a number of relevant variables, namely educational attainment, as a proxy for cognitive function,31 substance use disorders (alcohol, cannabis, nicotine), use of other drugs, depression and various personality traits (sociability, aggression-hostility, anxiety-neuroticism and sensation seeking) and examined the interplay between these factors in a cohort of young Swiss men. Our goals were to investigate these variables (1) as risk factors for TBI and (2) as consequences of TBI. While most of these have been evaluated separately in previous studies, there is a need for a bidirectional approach and a longitudinal design. To the best of our knowledge, although the influence of TBI on personality is well documented, there are no available data on preinjury personality traits in affected individuals. By analysing these parameters longitudinally in the same cohort, we aim to reduce the confounding effects of sociodemographic differences and baseline pathology as much as possible and thus place a solid foundation upon which future research may build strategies for the prevention and management of TBI.
Methods
Study design and participants
We analysed data from the Cohort Study on Substance Use Risk Factors, a longitudinal study from Switzerland designed to investigate the risk and protective factors related to substance use in emerging adulthood. The full details of the study are described elsewhere.32–34 In Switzerland, all men must undergo the army recruitment process to determine their eligibility for military or civil service. Between August 2010 and November 2011, all young men reporting to the recruitment centres of Lausanne (French-speaking), Windisch and Mels (German-speaking) were invited to participate in the study. A total of 7556 men gave written consent to participate in the study. Since there was no a priori selection, the sample can be considered representative of German-speaking and French-speaking Swiss young men. Data were collected at three time points, beginning in 2010: baseline (2010–2012), follow-up 1 (FU1; 2012–2014) and follow-up 2 (FU2; 2016–2018). This information is presented in figure 1.
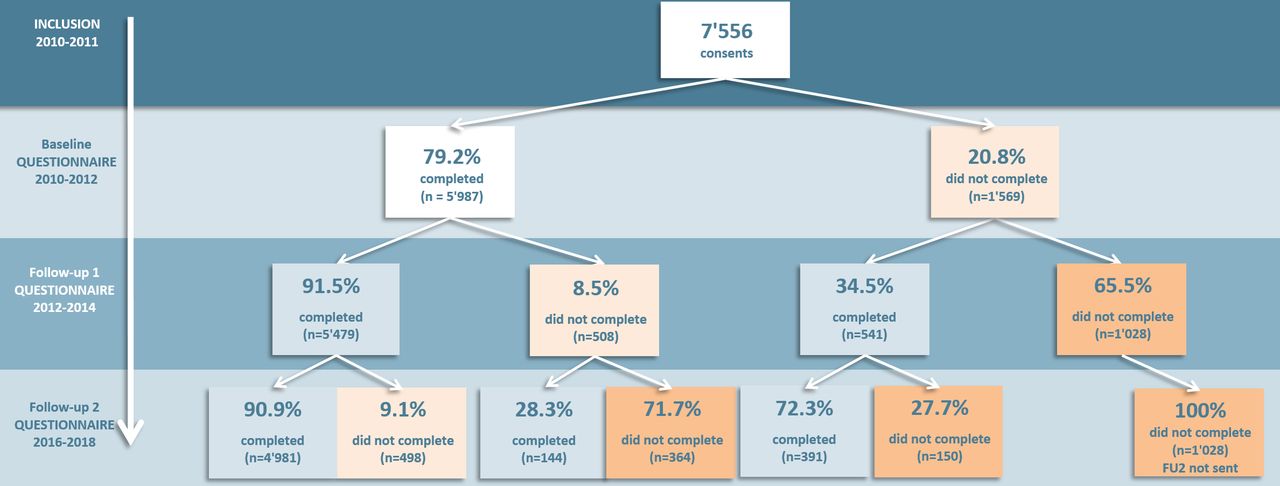
Number of participants according to each time point. FU2, follow-up 2.
TBI in the previous 12 months and before was evaluated only at FU2. Thus, in the present study, only participants who completed the FU2 questionnaires were considered (n=5516, 73% of consenters). Compared with participants who did not complete the FU2 questionnaire, those who completed the FU2 questionnaire were significantly more educated, less likely to report depression, nicotine dependence (ND) and cannabis use disorder (CUD), were younger, and reported lower levels of aggression-hostility at FU1 (all p<0.001).
Patient and public involvement
No patients nor any other members of the public were involved in the design, development of the research question, conduct, reporting or dissemination plans of our research. Study participants were regularly informed about the findings by means of brochures or leaflets, or they could find the study results on the study’s web page.
Design of the study
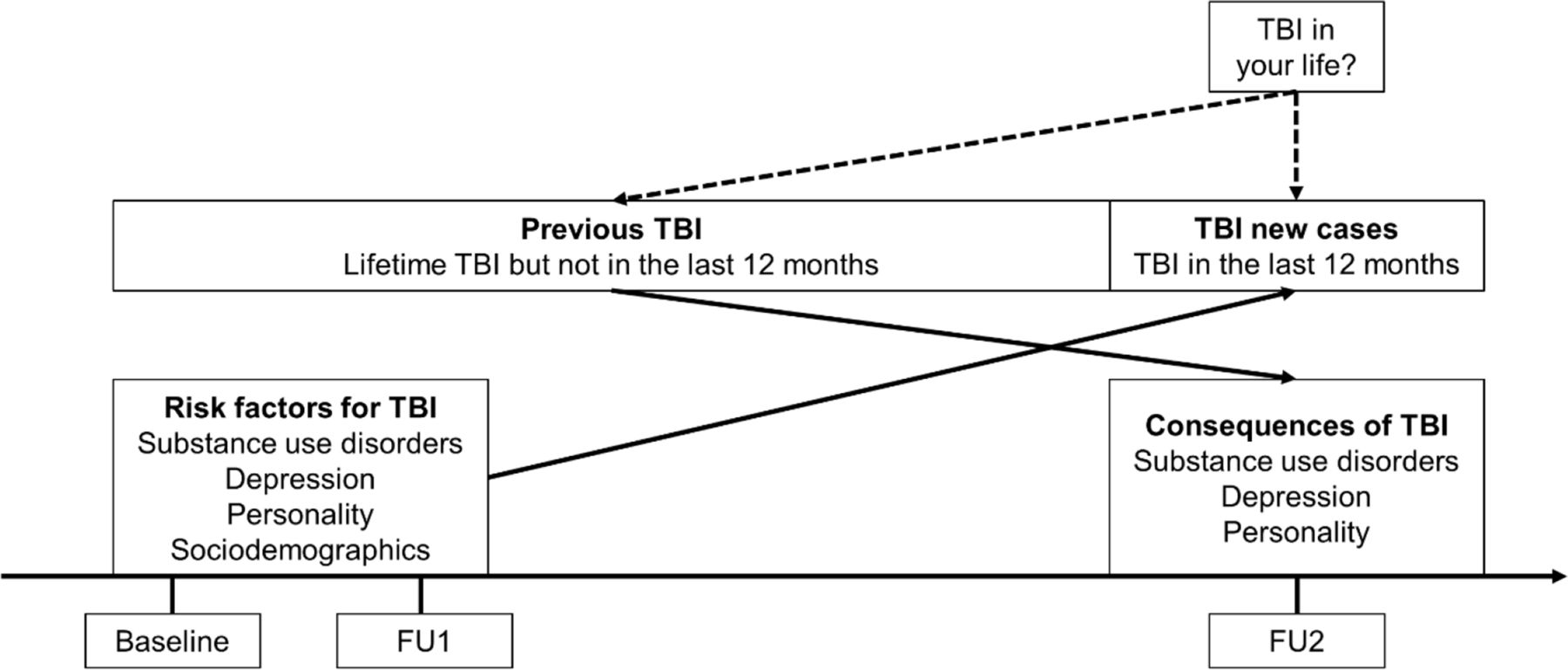
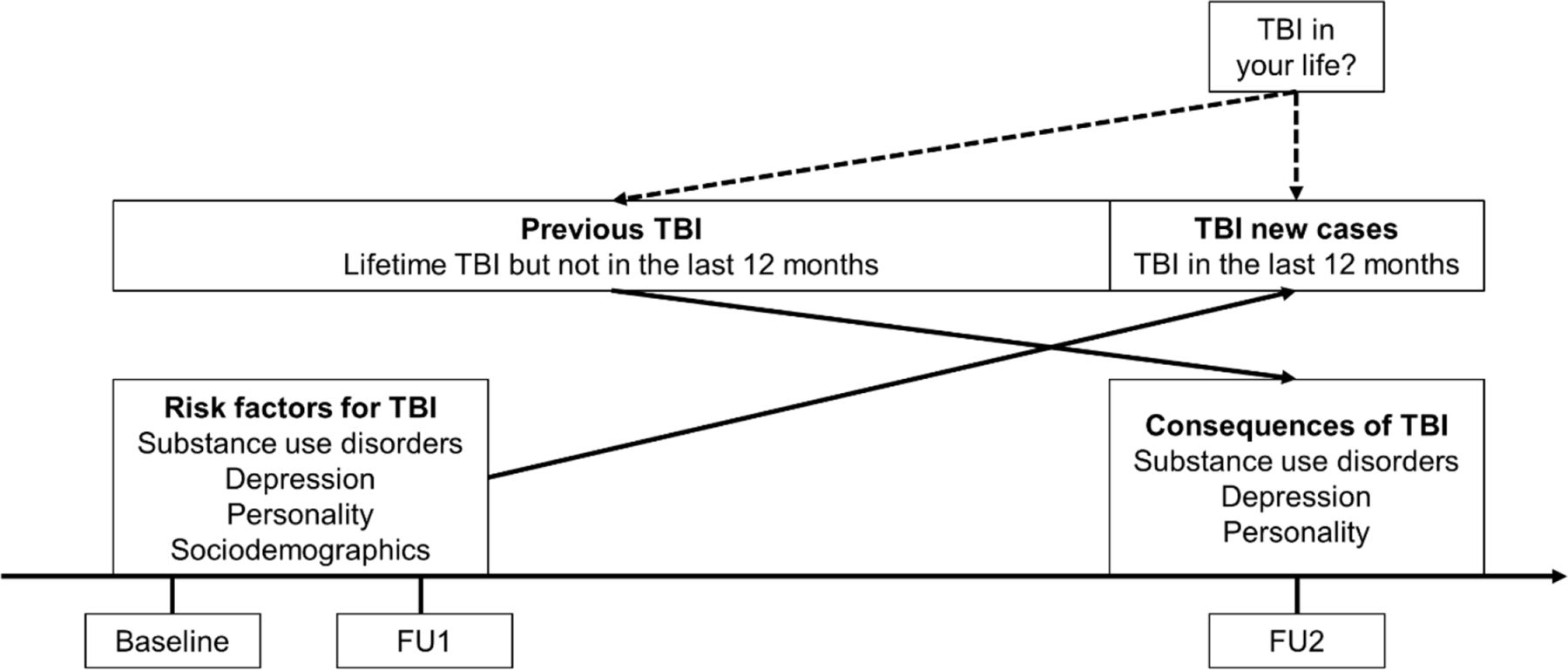
To reduce response burden, not all questions were measured in all waves. For example, personality was only measured at baseline and FU2. By contrast, substance use disorders, sociodemographics and depression were measured in all waves. Risk factors measured closest to FU1 (ie, at FU1 when available or at baseline) were selected to predict TBI in the 12 months preceding FU2 (TBI new cases). By contrast, TBI occurring before 12 months preceding FU2 (previous TBI) was used to predict the consequences of TBI measured at FU2. Thus, personality measured at baseline and substance use disorders, sociodemographics and depression measured at FU1 were used to predict new cases of TBI at FU2, whereas personality, substance use disorders and depression measured at FU2 were used to investigate the consequences of TBI preceding FU2. This allows to fit the temporal criteria for the risk factors and consequences of TBI: risk factors precede TBI new cases, and previous TBI precedes consequences measured at FU2. Figure 2 depicts the design of the study.
{kind=link}
{kind=link}
Design of the study. FU1, follow-up 1; FU2, follow-up 2; TBI, traumatic brain injury.
For participants with missing values on FU1 risk factors (ie, substance use disorders, sociodemographics and depression) and non-missing values on the same variables available at baseline, last observation carried forward (LOCF) was used to impute missing values at FU1 (n=236, 4.3%).
Measures
TBI was measured at FU2 as in Ilie et al35 by asking the participants the following: ‘We are interested in any head injuries that resulted in you being unconscious (knocked out) for at least 5 minutes, or you had to stay in the hospital for at least 1 night because of it. Did you have this type of head injury in your life?’ Response choices were (1) yes, I’ve had a head injury like this in the last 12 months, (2) yes, I’ve had a head injury like this in my life, but not in the last 12 months, or (3) No, I’ve never had a head injury like this in my life, reflecting (1) new cases of TBI (all cases occurring only in the 12 months preceding FU2, with no TBI prior to that time point), (2) previous TBI (before 12 months preceding FU2) and (3) non-TBI (participants who had never experienced TBI).
Alcohol use disorders (AUD) were measured at FU1 and FU2 using the 11 criteria for AUD, based on the Fifth Edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5).36 Participants were asked whether they had experienced any criterion in the previous 12 months. Questions (yes–no format) were taken from Knight et al,37 except the craving criteria which we developed. AUD was considered as met when at least four DSM-5 criteria were endorsed, reflecting moderate or more severe AUD.36
ND was assessed at FU1 and FU2 using the six-item Fagerström Test for Nicotine Dependence.38 A continuous score ranging from 0 to 10 was computed according to the scoring procedure proposed by the authors and ND was considered as met for scores of 3 or above, corresponding to low or more severe ND.39
CUD was evaluated using the Cannabis Use Disorder Identification Test40 at FU1 and FU2. This is a 10-item assessment tool asking participants about symptoms of CUD during the previous 12 months, yielding a score ranging from 0 to 40. A score of 8 or above was used to define CUD status.40
Use of other illicit drugs was measured at FU1 and FU2. Participants were asked about their use of other substances than alcohol, tobacco and cannabis in the previous 12 months. Questions included use of natural hallucinogens (magic mushrooms, psilocybin, peyote, mescaline); other hallucinogens (eg, LSD - lysergic acid diethylamide, PSP/angeldust - phencyclidine, 2-CB - 2,5-dimethoxy-4-bromophenethylamine, 2-CI - 2-(4-Iodo-2,5-dimethoxyphenyl)ethan-1-amine); Salvia divinorum; speed; amphetamine, methamphetamine and amphetamine sulfate; crystal meth; poppers; solvent sniffing; ecstasy and MDMA (methylenedioxymethamphetamine); cocaine, crack and freebase; heroin; ketamine and dextromethorphan; GHB (gamma-hydroxybutyric acid)/GBL (gamma-butyrolactone)/1-4 butanediol; research chemicals; and spices or similar substances. A dichotomous variable reflecting use versus no use of any of these substances was created.
Depression was assessed at both FU1 and FU2 with the Major Depression Inventory, which is based on the major depression symptoms of the 10th Edition of the International Classification of Diseases (ICD-10).41 It consists of 10 items (questions 8 and 10 have two subitems: ‘a’ and ‘b’; the highest score of each subitem is used when calculating the final score) each evaluated on a 6-point scale from 0 ‘At no time’ to 5 ‘All the time’, gathering a total possible score of 50 points. The cut-off of 26 proposed by Bech et al41 to diagnose was used to define moderate or more severe depression.
Individual differences in sensation seeking at baseline and FU2 were assessed using the eight-item Brief Sensation Seeking Scale.42 Each item was evaluated on a 5-point scale ranging from 1 ‘strongly disagree’ to 5 ‘strongly agree’. A mean score ranging from 1 to 5 was computed so that high scores reflect high levels of sensation seeking.
Individual differences in anxiety-neuroticism, sociability and aggression-hostility were measured using the cross-cultural shortened form of the Zuckerman-Kuhlman Personality Questionnaire43 at baseline and FU2. Each scale comprised 10 items in a true/false format. A summary score ranging from 0 to 10 was computed so that high scores reflect high levels of the measured personality trait.
Sociodemographics included highest level of achieved education (primary schooling: 9 years; vocational training: >9–12 years; postsecondary schooling: 13 years or more including high school, which can be only 12 years in some cantons), age and linguistic region.
Statistical analysis
Descriptive statistics were used to characterise the sample. First, we explored the putative risk factors for developing TBI using new cases (n=102) and non-TBI (n=3919) using logistic regression. As a first step, simple logistic regression was used to test the bivariate associations of each predictor variable with TBI new cases (model 1). Then, all associations were adjusted for sociodemographics (age, highest level of education and linguistic region) in model 2. Results were reported using OR and the corresponding 95% CI.
Second, to explore whether TBI was a risk factor predicting future conditions, we tested whether previous TBI (n=860) versus non-TBI (n=3919) was associated with the criterion variables at FU2 (AUD, ND, CUD, other illicit drug use, depression, personality traits). Three regression models were used for each criterion variable. Model 1 (bivariate) tested the bivariate association of previous TBI (vs non-TBI). Model 2 (baseline adjustment) tested the association of previous TBI (vs non-TBI), adjusted for FU1 (or baseline) values of the criterion variable. Baseline adjustment allows the removal of the stable portion of the criterion variable so that the association of previous TBI can be interpreted as prediction of relative change in the criterion variables.44 Model 3 (fully adjusted) tested the association of previous TBI (vs non-TBI), adjusted for baseline values of the criterion variable, for FU1 (or baseline) variables significant in the analyses on risk factors for TBI and for sociodemographics. Dichotomous criterion variables were analysed using logistic regression and continuous criterion variables using linear regression. Although continuous variables were not normally distributed (Shapiro-Wilk=0.001), assumptions of linear regression (normality of residuals and homoscedasticity) and logistic regression showed no violations. OR (for logistic regression) and unstandardised coefficients (for linear regression) and the corresponding 95% CI were reported for each model. Statistically significant values were considered at p<0.05. All analyses were performed using IBM SPSS Statistics V.26.
Results
Descriptive statistics for the samples
Participants with missing values on at least one of the variables of interest (n=635, 11.5%) were excluded. Compared with participants with missing values, complete cases were significantly more often German-speaking, more educated, less likely to report use of other illicit drugs, AUD, ND and CUD, were younger, and reported lower levels of aggression-hostility at FU1 (all p<0.027).
The final analytical sample comprised 4881 cases. From this sample, a total of 3919 (80.3%) participants reported to never have had TBI (non-TBI) and 962 (19.7%) had suffered TBI at some point in their life by the age of 25. A total of 102 (2.1%) reported to have had TBI in the last 12 months (TBI new cases), whereas 860 (17.6%) had TBI during their lifetime but not in the 12 months preceding FU2 (previous TBI). The mean age of the total sample was 21.29 years (SD=1.26) at FU1 and 25.43 (SD=1.25) at FU2. Descriptive statistics of non-TBI, TBI new cases and previous TBI, together with the n and percentage for substance use disorders, depression, education and linguistic region, and the mean and SD for age, sensation seeking, anxiety-neuroticism, sociability and aggression-hostility scores, are listed in table 1.
Descriptive statistics
Putative risk factors for TBI
The results of the logistic regression models of the risk factors for TBI are reported in table 2. In bivariate analyses (model 1), vocational training and primary schooling (as opposed to postsecondary schooling), ND, depression, sociability, aggression-hostility and sensation seeking were significantly associated with increased odds of new cases of TBI. Adjusting for sociodemographics in model 2 did not alter the results.
Putative risk factors for TBI
Consequences of TBI
The results of the analyses of the consequences of previous TBI (TBI before 12 months preceding FU2) are reported in table 3. In bivariate analyses (model 1), as opposed to non-TBI, previous TBI was associated with increased odds of reporting AUD, ND, CUD, use of other illicit drugs and depression and higher scores in aggression-hostility and sensation seeking. In model 2 (baseline adjustment), only the associations of previous TBI with ND, depression and aggression-hostility remained significant, whereas the positive association with neuroticism-anxiety became significant. In model 3 (fully adjusted), adjusted for FU1 (or baseline) values of the criterion variable, for FU1 (or baseline) variables significant in the analyses on risk factors for TBI and for sociodemographics, only the associations of previous TBI with ND, depression and aggression-hostility remained significant.
Consequences of TBI
Discussion
The results of our study indicate that an important number of young men are affected by TBI. Out of 4881 subjects analysed, 962 (19.7%) had suffered TBI at some point in their life by the age of 25. Of these, 102 (2.1%) occurred less than 1 year before questioning (1-year incidence), which matches the data from similar studies.45 The higher prevalence found by our study compared with that found by examining medical records is most likely the consequence of using self-report questionnaires, as patients tend to report more symptoms of TBI on questionnaires than in open interviews.46
Our paper is one of the few that simultaneously assessed the risk factors and the consequences of TBI in the same cohort in order to ascertain the interplay between the two and the potential implications. To the best of our knowledge, this is the first time that the premorbid personality of TBI victims is assessed by standardised psychometric instruments. Of the parameters evaluated, sociability and sensation seeking were unidirectionally associated with TBI (being risk factors for but not consequences of TBI), while ND, depression and aggression-hostility were bidirectionally related (risk factors for and consequences of TBI). Thus, correctly identifying and mitigating these factors in vulnerable populations should be prioritised for both primary and secondary prevention.
Risk factors for TBI
We used educational attainment as a partial proxy for cognitive functioning31 and socioeconomic status,47 which are known risk factors for TBI,27 and found low educational attainment to be a major predictor of future TBI.
Depression is documented as a major predictor of TBI11 17 and our results are in line with previous research. Impaired serotoninergic function is a putative cause of depressive disorders and is also associated with aggression and drug abuse.48 Thus, it can be speculated that individuals at risk of TBI may suffer from a pre-existent dysfunction in serotonin neurotransmission, which may be involved both in mood and impulse control, which may be further heightened by TBI.49
We found that particular personality traits carry an increased risk of TBI, namely high sociability, aggression-hostility and sensation seeking. This is not surprising as high scores in these dimensions are independent predictors of high-risk behaviours that can lead to TBI. In particular, all three traits are related to alcohol consumption, high aggression-hostility is related to reckless driving, and drug use is related to high sensation seeking.50
Participants with AUD and CUD or who used other illicit drugs had higher odds of suffering from TBI than patients without TBI, but the difference was not statistically significant. However, it must be noted that our sample size of TBI victims with substance use disorders was relatively small. Previous studies have yielded conflicting results: while most studies reported substance use disorders to be highly prevalent preinjury,11 51 some found no association.52 Only ND has been significantly associated with increased risk of TBI in our study population, which is consistent with results from previous studies.9 The statistical significance of ND may be partly due to the higher number of subjects with ND as opposed to the relatively low number of subjects with AUD, CUD or other types of substance disorders in our cohort.
Consequences of TBI
Depression was a major consequence of TBI in our studied population even after controlling for pre-existing depressive disorder and other potential confounders such as low education, personality traits and substance abuse. Depression might be a consequence of a decline in quality of life and functionality, but its prevalence does not seem to be related to injury severity53 as one would expect if this were the case. Another explanation is that post-TBI depression is the result of trauma-induced neurotransmitter imbalances and alteration of neural circuit plasticity.49 Antidepressant drugs are efficient in treating depression,54 and it stands to reason that adequately conducted treatment should reduce the risk of TBI; however, concrete data on this topic are not available.
Changes in personality following TBI have been widely documented. Poor impulse control, affective instability and emotional lability are all common.55 Our study found that previous TBI is associated with higher scores in aggression-hostility, even after baseline adjustment. This suggests that TBI may lead to long-lasting changes in personality that can further diminish the patient’s quality of life and prospects of recovery. One possible explanation is that trauma causes a long-term decrease in serotonin neurotransmission, which leads to poor impulse control and depression.56 An additional argument for this theory is the fact that selective serotonin reuptake inhibitors have shown some efficacy in treating post-TBI aggression,57 but this could also be due to the alleviation of depressive symptoms, which are known to compound aggression in TBI.58
In our study population, previous TBI has not been associated in a statistically significant manner with subsequent alcohol, cannabis or other drug-related disorders, but was associated with higher rates of ND. Other longitudinal studies suggest that alcohol and substance use briefly decreases after an injury and tends to gradually return to baseline levels.21 22 ND was higher among victims of TBI than in non-TBI, even when accounting for baseline use, which is consistent with previous studies.9 A potential explanation is the potential of nicotine to attenuate TBI-induced cognitive deficit secondary to neurobiological alterations in the expression of the nicotinic cholinergic receptor.59 However, this does not explain increased ND preinjury.
Limitations
Our study has several limitations, mostly pertaining to the studied cohort. While young men are more often affected by TBI, the epidemiological patterns and consequences of TBI in this population are not necessarily shared by other demographic groups. Female victims differ significantly in measures of severity and mortality.60 Similarly, elderly patients exhibit markedly different causes and outcomes of TBI than the young.61 There were significant differences in FU1 variables between participants who did and did not complete the FU2 questionnaire and between participants included in the analyses and those excluded due to missing values. This may be indicative of a possible selection bias. Another shortcoming was the small number of new TBI cases with alcohol and drug use disorders, which did not allow us to draw definitive conclusions regarding their status as a risk factor for TBI, as well as the absence of data on other known risk factors such as socioeconomic status and race. Social deprivation not only increases the odds of suffering from TBI, but also significantly influences patterns of care and recovery.61 As we enquired only about TBI that involved loss of consciousness, our results might not be entirely applicable to mild cases without altered consciousness. The lack of information on the experience of previous TBI, the cause of trauma, the time passed since the injury and the severity and management of physical and neurological sequelae may generate significant heterogeneity in our cohort. We also cannot exclude that the lack of accounting for unmeasured confounding factors (eg, previous TBI, medications, attention deficit hyperactivity disorder, race, socioeconomic status), as well as measurement errors of some measured confounders, may partially have biased the results. Furthermore, measures were self-reported and thus subject to memory and social desirability biases.
Using the simple imputation method of LOCF for some variables missing at FU1 could render biased results and this should be taken into consideration when interpreting our results. For example, depression or substance use disorder which are not constant over time as risk factors for TBI. On the other hand, we did not consider the application of LOCF for sociodemographic characteristics to increase the risk of bias.
Conclusion
Our study offers a unique longitudinal perspective on the relationship between the risk factors for and the consequences of TBI in a cohort of young men. In doing so, we hope to outline the parameters that can be targeted by therapeutic interventions in order to reduce the risk of sustaining such an injury and mitigate its long-term impact where it has already occurred. Screening for and treating depressive disorders may be among the most effective measures for both primary and secondary prevention of TBI. Conversely, screening for TBI when encountering patients with depression, substance abuse and personality changes should be strongly considered. However, other factors, especially those pertaining to educational attainment and personality traits, are more challenging to intervene on. Further studies are needed in order to formulate a more comprehensive management strategy for TBI.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and the Cohort Study on Substance Use Risk Factors was approved by the Lausanne University Medical School’s Ethics Committee for Clinical Research (reference number 15/07). Participants gave informed consent to participate in the study before taking part.
References
Footnotes
Contributors VPM designed the study. VPM, AER, ANP and RMP wrote the article. JS, GG and J-BD reviewed the manuscript and gave final approval for publication. VPM was the guarantor for the study.
Funding This work was supported by the Swiss National Science Foundation (grant numbers FN 33CS30_177519, FN 33CS30_148493, FN 33CS30_139467, FN 33CSC0-122679).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.