Article Text

Abstract
Objectives To understand which organisational–structural characteristics of nursing homes—also referred to as long-term care facilities (LTCFs)—and the preventative measures adopted in response to the pandemic are associated with the risk of a COVID-19 outbreak.
Setting LTCFs in Lazio region in Italy.
Design The study adopts a case–control design.
Participants We included 141 facilities and 100 provided information for the study. Cases were defined as facilities reporting a COVID-19 outbreak (two or more cases) in March–December 2020; controls were defined as LTCFs reporting one case or zero. The exposures include the structural–organisational characteristics of the LTCFs as reported by the facilities, preventative measures employed and relevant external factors.
Results Twenty facilities reported an outbreak of COVID-19. In binary logistic regression models, facilities with more than 15 beds were five times more likely to experience an outbreak than facilities with less than 15 beds OR=5.60 (CI 1.61 to 25.12; p value 0.002); admitting new residents to facilities was associated with a substantially higher risk of an outbreak: 6.46 (CI 1.58 to 27.58, p value 0.004). In a multivariable analysis, facility size was the only variable that was significantly associated with a COVID-19 outbreak OR= 5.37 (CI 1.58 to 22.8; p value 0.012) for larger facilities (>15 beds) versus smaller (<15 beds). Other characteristics and measures were not associated with an outbreak.
Conclusion There was evidence of a higher risk of COVID-19 in larger facilities and when new patients were admitted during the pandemic. All other structural–organisational characteristics and preventative measures were not associated with an outbreak. This finding calls into question existing policies, especially where there is a risk of harm to residents. One such example is the restriction of visitor access to facilities, resulting in the social isolation of residents.
- COVID-19
- GERIATRIC MEDICINE
- Quality in health care
- Infection control
Data availability statement
Data are available in a public, open access repository. The database generated from the authors of this study is available at Open Science Framework (OSF) (www.osf.io) [dataset] [30] Orlando, S., A. Abbondanzieri, and G. Cerone, Dataset of characteristics of nursing homes and early preventive measures associated with risk of infection from COVID-19 in Lazio region, Italy. 2021. Available from: https://doi.org/10.17605/OSF.IO/RHB8E.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
Data collected on facilities included in the study covers a relatively broad spectrum of facilities’ characteristics and measures used to avoid COVID-19 contagion.
The random opening of only some facilities to visitors has allowed a natural experiment to assess whether these openings have increased the risk of contagion.
Being a retrospective observational study, we could not randomise and control the data available.
The measures collected in the study were self-reported.
The relatively small size of the sample may have contributed to the non-significance of some of the associations explored.
Introduction
Older adults living in nursing homes, also referred to as long-term care facilities (LTCFs) in this document, have been struck by the COVID-19 pandemic.1 2 A report based on data from European Centre for Disease Prevention and Control shows that in Europe, between 31% and 66% of deaths caused by COVID-19 were among this group.3 In Canada, the estimate is 50%,4 and in the USA, it is 40%.5 These data show the need to protect this population by improving the safety of LTCFs, especially in Europe, where 65 000 LTCFs with around 3.5 million beds are present.6 In addition to the impact of the virus on health, some preventative measures taken in response to COVID-19 have caused unintended harm to the residents of the nursing homes. Preventing family visits to facilities increased the risk of social isolation and all-cause mortality.7–12
This study aims to explore which structural and organisational characteristics of LTCFs (eg, size of facility) as well as preventative policies implemented since the onset of the COVID-19 pandemic (eg, restriction of visitors to the facility) are associated with the risk of a COVID-19 outbreak, compared with facilities that avoided infections.
Two rapid systematic reviews on this topic have been conducted to date.13 14 Data have been drawn from 118 studies based in 19 countries across the two studies, with most studies being drawn from the USA. The remainder of the studies is drawn from North and South America, Europe and Asia.
Findings from the review indicate that larger facilities15 16 and staff working across multiple facilities were risk factors for a COVID-19 outbreak.17 18 From our in-depth analysis of studies included in this review, it is apparent that findings are mixed: for example, there is evidence for an association between ownership of the facility (private, public or no-profit) in four out of eight studies that explored this characteristic16 19–25; the number of beds in a facility or facility size were associated with COVID-19 outbreak in three of six studies,16 19–21 23–25 bed occupancy in two of the studies which assessed it,19 22 and the presence of disadvantaged individuals in three out of five studies were associated with a COVID-19 outbreak.16 19 21–23 25
As such, there is no clear evidence on the relationship between characteristics of the LTCFs and the risk of a COVID-19 outbreak from the existing literature. The lack of consistency in study findings raises questions about the reliability of measures employed in each of the studies and any global differences in the effectiveness of these findings. Moreover, the reviews in this area underscore the limitations of studies in this area—currently, systematic reviews are mainly based on observational studies—there are few randomised controlled trials exploring the effectiveness of policies to mitigate the impact of the pandemic on nursing home residents. Additionally, there is a substantial reliance on studies in the USA, with relatively fewer studies across different continents. Given the markedly different approaches to the pandemic both between and within countries, studies in other regions are required.
This study sought to add to the existing literature on this topic by exploring the relationship between the organisational aspects of LTCFs or policies specific to COVID-19 and the risk of a COVID-19 outbreak in Italy. This study is the first one to have explored this relationship in Italy.
The findings of this study add to the current understanding of factors that increase and mitigate the risk of COVID-19 outbreaks in LTCFs. Findings will also explain the role of structural–organisational characteristics and preventative policies in mitigating the impact of catastrophic events in general.
Materials and methods
A retrospective case–control study in an Italian region was conducted to investigate the characteristics of LTCFs associated with an increased risk of COVID-19 outbreak in the facility. This case–control study is reported as per Strengthening the Reporting of Observational Studies in Epidemiology reporting guidelines.
Participants
Cases were defined as a group of facilities in which LTCFs between March and December 2020 reported an outbreak. Controls were defined as a group of facilities where an outbreak did not occur over the same period. The period over which cases could occur includes the start of the COVID-19 epidemic in Italy with the consequent lockdown and the so-called ‘second wave’ of infections from September to December 2020, when a peak of infection and excess mortality was registered.26
The general population to which this study refers are Italian older adults (over 65) living in LTCFs. This term refers to all types of structures housing individuals who cannot dwell independently in their communities. We adopted the definition of an outbreak in a residential setting as the presence of two or more test-confirmed cases of COVID-19 within 14 days.27
The study was based on existing data collected by the Azienda Sanitaria Locale (in Italian) which translates to a Local Health Unit—referred to as LHU hereon—in English. The LHUs are a network of population-based local health authorities managed by regional governments. The LHUs are autonomous and public services. Service is provided either through the LHU’s own facilities or contracts with private providers.
Among the surveyed facilities, the following were selected for data analyses: nursing homes, assisted-living facilities, rest homes and LTCFs hosting exclusively older adults (<65 years old). Facilities that cater specifically to younger adults were excluded from our sample. Facilities that cater to specific health conditions or rehabilitation communities for drug addicts often admit younger patients. Thus, they too were excluded from the analytic sample. The data for this study were obtained from LTCFs in Lazio—a region in central Italy.
The statistical analysis considered each facility as a unit of analysis. The dependent variable (outcome) was the presence of an outbreak, defined as two or more cases of COVID-19 confirmed by a laboratory test among the residents in the facility. Facilities reporting an outbreak are hereafter described as ‘cases’, and facilities with no outbreaks ‘controls’.
The exposures were derived from (1) structural–organisational characteristics of the facilities, (2) policies put in place by the facilities as a response to COVID-19 and (3) factors related to the area in which the facility is located.
Shortly after the outbreak of the COVID-19 pandemic in Italy, The LHU surveyed LTCFs on their policies and practices with respect to COVID-19. The LTCFs were required to rate their preparedness based on 19 items (pertaining to structural–organisational characteristics and preventative measures in place in response to the pandemic). The self-rated level of preparedness per each of the participating LTCFs was provided to us as part of this study.
Examples of structural–organisational aspects of facilities include the size of facilities (eg, number of beds in a facility), how many rooms were single or shared rooms and whether the facility was privately or publicly owned. Policies adopted in response to COVID-19 include isolating residents who tested positive for COVID-19 (termed presence of Isolation environment hereon), a grey area (an area in which staff could sanitise and change their clothing after they had visited those infected with COVID-19), separate entrances for staff who were and were not in touch with residents and active surveillance for staff and residents (regular temperature checking and, when available, regular testing for COVID-19). Please see online supplemental table 1 for a complete list of items (in both Italian and English), the source of data and response options for each of these items.
Supplemental material
The LHU assigned a 3-point score to each of the 19 items in the facility questionnaire.
Each item could be assigned a score of 0, 1 and 2. The numbers 0, 1 and 2 indicated the absence, partial presence and presence, respectively, of the 19 items.
A cumulative ‘risk score’ across all 19 items was calculated. Scores could range from 0 (where all characteristics were absent) to 38 (where each of the items scored two) were all characteristics were present. The 19 items were also explored as binary variables. The latter two categories for each item were merged into one category, considering the level of partial presence as absence, and in the numerical variables, the intermediate level as the highest.
In addition to the 19 structural–organisational characteristics obtained from the LHUs, 4 characteristics (external and internal to the facility, obtained from the LHU epidemiological surveillance department) were explored as risk factors for an outbreak. These include: (1) Incidence of COVID-19 in the facility’s catchment area, (2) the presence of at least one member of staff who tested positive for COVID-19, (3) the number of days the facility was open to visitors during post lockdown in Italy, during the period of June–September and (4) whether the facility was in an urban or rural setting. Except for the incidence of COVID-19 in the facility’s catchment area, all additional variables were categorical. Further details on these variables can be seen in online supplemental table 1.
A binary logistic regression model evaluated the association between potential risk factors (each item of the questionnaire, the overall risk score and the four additional variables) with the probability of reporting at least two positive cases among residents. We calculated the median difference between groups and the CI with the 2-sample Hodges-Lehmann estimator for continuous variables such as risk score and incidence. P value at 95% significance is calculated with Wilcoxon rank-sum test with continuity correction. A Wilcoxon rank-sum test was used for binary variables to compare each variable between the cases and controls since the assumptions for a parametric test were not met. ORs of being in the cases group were calculated for categorical variables, and the related statistical significance was assessed with Fisher’s exact test. We also performed a multivariable analysis with logistic regression to evaluate the adjusted effect of some variables.
We included in the model the variables found to be significant in the binary logistic regression analysis plus some variables that were considered important from a clinical point of view, as recommended in recent papers.28 Such variables include active surveillance of personnel, the use of personal protective equipment and the incidence of COVID-19 in the facility area. The presence of a staff member who had tested positive for COVID-19 was not included because it was considered a proxy of the outcome.
All analyses have been performed with statistical software ‘R’ V.4.1.1.29 The database with information collected during the LHU survey and the information on the COVID-19 outbreaks in the facilities, and the code written for the statistical analysis are publicly available at Open Science Framework.30
Patient and public involvement
No patient involved.
Results
The LTCFs surveyed by the LHU included 185 facilities. Forty-four were excluded since they did not meet the inclusion criteria for LTCFs in this study (described earlier in the methods section). Among these, 100 (70.9%) provided data for the survey on the risk assessment and were included in the analysis. Overall, 20 of them (20.0%) reported a COVID-19 outbreak and were selected as cases, while the remaining 80 (80.0%) represented the controls group. A flow chart shows the exclusion of facilities (figure 1). The reasons why 41 structures (29.1%) did not provide all the data required by the risk assessment are unknown. However, we executed a Fisher test to see if not providing risk assessment data increased the likelihood of being in the group of facilities with an outbreak. The proportion of outbreaks in the group of facilities that provided the data was 20%, while those that did not provide it was 22.0% (p=0.82), and therefore not significantly different.

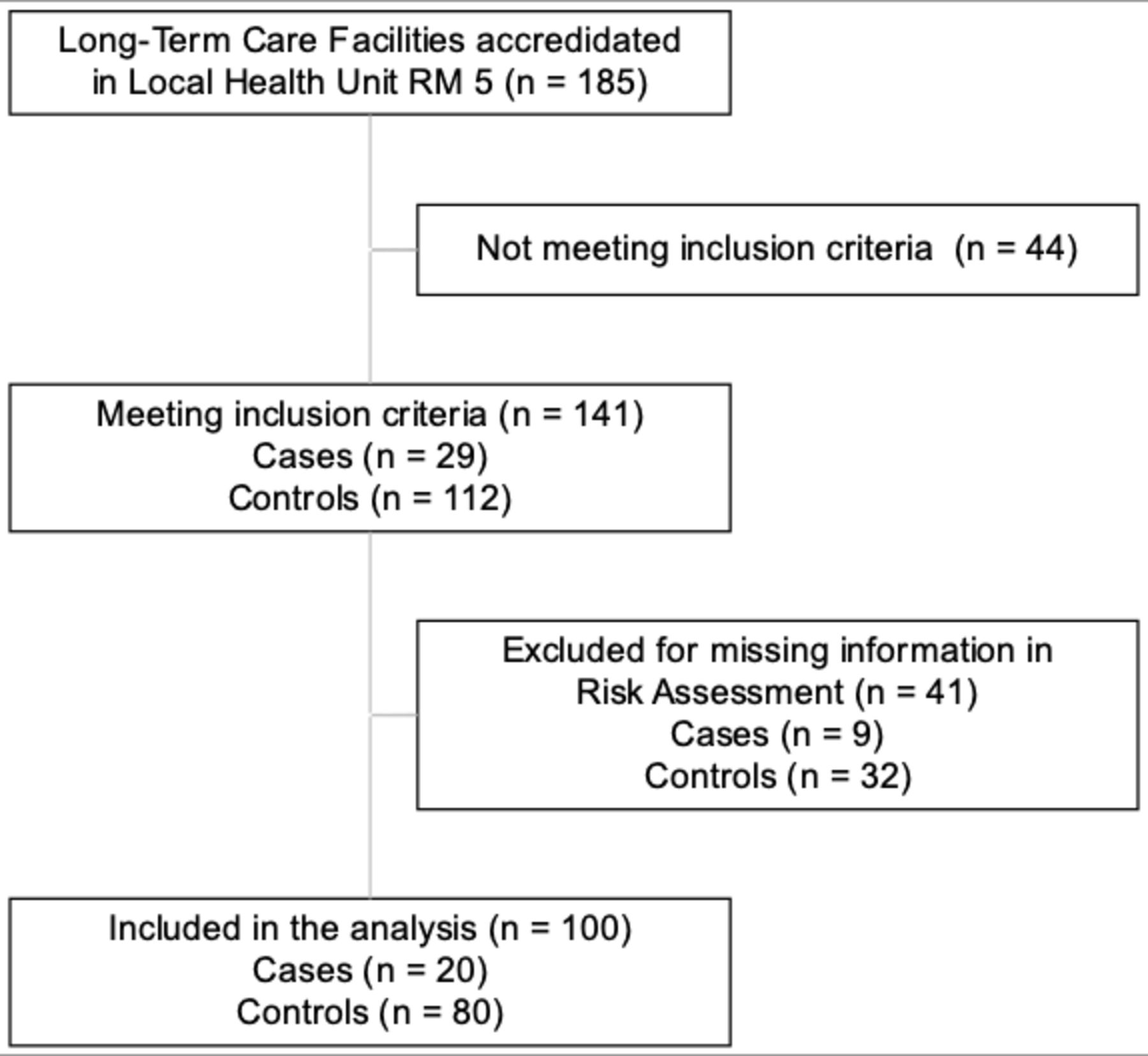{kind=link}
Flow chart.
Table 1 reports the list of variables representing the characteristics of the LTCFs informed by the risk assessment or other sources. Descriptive statistics (frequencies and means) are shown for each of these variables; the binary logistic regression results, which explore the relationship of each of these variables with the outcome, are also shown.
Descriptive statistics of variables by group and binary logistic regression analysis. Fisher’s exact test for binary variables and Wilcoxon rank-sum test for continuous variables
The presence of a member of staff who had tested positive for COVID-19 was strongly associated with the risk of infection among residents (154.7 OR, p<0.001). Given the strength of this association, we considered this variable a proxy of the outcome and, as such, decided not to include this variable in subsequent analyses.
The admission of new residents was associated with an increased risk of an outbreak (OR=6.46, p<0.01); A higher risk of the outbreak was observed among facilities with more than 15 beds compared with those with less than 15 beds (OR=5.6, p<0.01).
Table 2 reports the results of the multivariable analysis. After adjusting for all other factors, the number of beds expressing the facility’s size remained the only variable significantly associated with a COVID-19 outbreak. The risk of reporting an outbreak was 5.37 times greater (95% CI 1.58 to 22.8) in facilities with more than 15 beds compared with those with less than 15 beds. The admission of new patients is no longer significant after adjustment for other variables.
Multivariable analysis with logistic regression
Overall, the model had a good predictive capacity—the Hosmer-Lemeshow goodness-of-fit test indicated a p value greater than 0.05.
Discussion
The findings of this study suggest that the risk of an LTCF outbreak is strongly linked to infections in staff. The risk of an outbreak was 154% higher among LTCFs where at least one staff member had an infection. Staff to patient transmission is the most plausible explanation for this relationship. While patient-to-staff transmission cannot be ruled out, it is unlikely: for around 87% of the facilities, patients were not allowed to leave the facility post pandemic and thus could not have contracted the virus from outside.
The admission of new residents since the start of the pandemic and larger facility size (as indicated by the number of beds in the facility) were also associated with a higher risk of an LTCF outbreak. This finding may be explained because patients with COVID-19 were more likely to be admitted to LTCFs, rather than in hospitals, where it was not feasible to implement the required security restrictions.24
Notably, a higher risk of the outbreak associated with new admissions to a facility was no longer significant after adjustment for the size of the facility (as shown by the number of beds). Therefore, the relationship between new admissions and the risk of an outbreak was not independent of the association between larger facilities and the risk of an outbreak.
The risk of larger facility size with outbreaks is consistent with existing studies investigating the correlation between the size of LTCFs and the risk of COVID-19 outbreaks. Two studies in the USA and one in the UK identified a greater risk of infection associated with the size of the facilities,16 20 22 and an extensive survey involving more than 5000 LTCFs in the UK found the same association.20 In two studies, LTCFs with at least one infection have a higher number of beds, but the statistical analysis was not performed.21 23 Allowing new admissions was also a risk factor in the UK study, although with a lower risk compared with our data.20
Importantly, this study did not find any evidence for an increased likelihood of an outbreak among LTCFs, which allowed entry of visitors during the summer. A commonly discussed guideline concerning nursing homes is the exclusion of visitors from nursing homes. Studies suggest that this measure has reduced the quality of life among elderly residents, and in some cases, it may have increased all-cause mortality.3 31 While physical isolation is a necessary measure to contain the spread of COVID-19, it is known that social isolation causes a deterioration in health.3 8 10 12 32 In the general population, social isolation has also been associated with an increased risk of contagion from COVID-19.33 Existing evidence has consistently shown beneficial effects of social networks on well-being among residents in nursing homes.7 34
An explanation for a perceived lack of effectiveness for these measures could be due to a lack of proper implementation of these measures by LTCFs, or a lack of adherence to these measures from residents. Therefore, policies are needed to support tighter control of staff health and adherence to prevention protocols. Moreover, it is necessary to verify the quality of staff training.
The findings of this study may help inform the guidelines for preparedness in the case of epidemics in LTCFs. In 2020, several bodies issued guidelines for this purpose.35–38 However, a review of these documents noted that they are not the result of a rigorous development process, and there are significant gaps.39 It is necessary to review the guidelines addressed to nursing homes concerning staff and visitors and new admissions in the short term. The staff is likely to be the main channel of contagion, and the potential ineffectiveness of measures such as the adoption of personal protective equipment or the systematic screening of the staff’s health was not expected.
In the long run, it is necessary to reconsider the size of LTCFs. Throughout Europe, larger facilities are commonly adopted to reduce unit costs in health provision. Given the potential for large facilities to increase risks to residents in a pandemic, a move toward smaller institutions should be considered. As with the abolition of orphanages for children or asylums for the mentally ill, many countries, including Italy, have intended to replace larger care institutions for the elderly with smaller ones. Our findings reinforce the importance of doing so.
Strengths and limitations
A strength of this study is that the data collected by the local health unit covered a relatively broad spectrum of LHU characteristics. Another strength is that the data were collected for epidemiological surveillance purposes and not for risk analysis, eliminating possible bias in responses for fear of legal consequences. Finally, a strength is that the random opening of only some facilities to visitors has allowed a natural experiment to assess whether these openings have increased the risk of contagion.
Among limitations, some are related to the study’s design. Given that the study is based on existing data, we had no control over which data were collected. A measure of adherence to protocols among residents and staff, for example, was an important omission in this study.
The measures collected in the study were self-reported. There is potential for facilities to report in a way that makes them appear more favourable and rigorous in their approach to COVID-19 policies, questioning the reliability of the exposures.
A further limitation is that the sample of facilities was not randomly drawn from the general population (the Italian LTCFs). They were drawn from one area, limiting the generalisability of the study findings. Furthermore, the relatively small size of the sample may have contributed to the non-significance of some of the associations explored. The potential for selection bias due to the high number of facilities that did not respond to the LHU survey (29.1%) is acknowledged. Although the proportion of COVID-19 cases in this group did not differ significantly from the facilities included, it is possible that the non-respondents may have adopted risky procedures that they did not want to report. We cannot rule out the possibility that the exclusion of these studies altered the results.
Finally, a limitation is that the survey on the characteristics of LTCF was carried out only once, in April–May 2020, while the data on outbreaks were collected up to December. Therefore some characteristics may have changed in the months following the survey. The limitation concerns only some measures that could be implemented quickly. Other aspects, including the size of the structure or the number of staff employed, have most likely not changed because they cannot be changed in a few months.
Conclusions
LTCFs for older adults have been disproportionally affected by the COVID-19 pandemic worldwide. In this case–control study of 100 LTCFs for Italian older adults, we found that the risk of a COVID-19 outbreak was higher among large facilities.
We also found some evidence to suggest that admission of new residents during a pandemic could increase the risk of an outbreak, though this appeared to be a practice inherent in larger facilities.
No other structural–organisational characteristics were associated with the risk of a COVID-19 outbreak in this study.
Pandemic preparedness guidelines should recommend caution in the admission of new residents during a pandemic. Recommendations that may not be effective should be reviewed, significantly where their implementation may harm residents, such as prohibiting visitor access to facilities. A reform to the care system for adults is advised, with recommendations for a move toward small-size facilities.
Data availability statement
Data are available in a public, open access repository. The database generated from the authors of this study is available at Open Science Framework (OSF) (www.osf.io) [dataset] [30] Orlando, S., A. Abbondanzieri, and G. Cerone, Dataset of characteristics of nursing homes and early preventive measures associated with risk of infection from COVID-19 in Lazio region, Italy. 2021. Available from: https://doi.org/10.17605/OSF.IO/RHB8E.
Ethics statements
Patient consent for publication
Ethics approval
In accordance with University of Tor Vergata guidelines, ethical clearance was not required, given that the study employed pre-existing anonymised data with authorisation to access the data from the relevant service providers.
Acknowledgments
The data used were provided by the Local Health Unit called Azienda Sanitaria Locale Roma 5 in the Lazio region in Italy. We thank the health director Dr Velia Bruno for allowing access to the data.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors Conceptualisation, SO; Data curation, GC, AA; Formal analysis, SO, FC; Methodology, SO, TM; Supervision, LP, MCM; Validation, GL; Writing—original draft, SO, TM; Writing—review & editing, SM, GL. All authors have read and agreed to the published version of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.