Article Text

Abstract
Introduction Migraine is a common neurological disorder with a higher prevalence occurring in women. Migraine without aura (MwoA) is the most common type of migraine. In recent years, the safety and effectiveness of acupuncture for migraines have been internationally recognised. Contralateral acupuncture (CAT) (Jùcì) is an ancient classic acupuncture technique from Huang Di Nei Jing that refers to the acupoints on the right side (healthy side) selected for diseases on the left (affected side) and vice versa. Some studies have shown that efficacy of CAT on the painful disorder is even better than ipsilateral acupuncture (IAT), but there remains a lack of high-quality evidence to support it.
Methods and analysis This is a single-centre, randomised and sham-controlled clinical trial in China with three parallel groups that aim to evaluate the efficacy of CAT in women with unilateral MwoA. 243 participants will be randomly divided into the experimental group (CAT group), control group 1 (IAT group) and control group 2 (sham acupuncture group) (1:1:1 allocation ratio). Each group will be given 30-minute treatment sessions, once every other day, approximately three times per week, for a total of 24 treatments and follow-up visits two times. The primary outcome is the changes in days of migraine attacks. The secondary outcomes are frequency of migraine attacks, intensity of migraine, migraine duration, the dose of intake of acute medication, the Migraine-Specific Quality of Life Questionnaire, the Migraine Disability Assessment Score, the Headache Impact Test-6 and the Pittsburgh Sleep Quality Index. The data will be collected at the baseline time (week 0), end of treatment (week 4–8) and the follow-up time (week 12–16). Adverse events will be collected and recorded during each treatment.
Ethics and dissemination Ethics approval was obtained from the Ethics Committee of the Sports Trauma Specialist Hospital of Yunnan Province (2021-01). All participants will provide written informed consent before randomisation. The results of this study will be published in a peer-reviewed journal and presented at conferences.
Trial registration number Chinese Clinical Trial Registration Center (ChiCTR2100051479).
- complementary medicine
- public health
- migraine
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This study will provide high-quality and up-to-date evidence to assess the efficacy of the contralateral acupuncture on unilateral migraine without aura (MwoA) and presents a treatment method for a choice of acupuncture at contralateral or ipsilateral for the treatment of MwoA.
The results of this trial will be a powerful validation of the classic traditional Chinese acupuncture theory.
The results of this study can provide a clinical basis for the treatment of other unilateral diseases and further research into the mechanisms of intercross regulation in the brain.
This study is limited as there was no positive drug control group.
This trial was not set up as a multicentre study and the results of the study may be influenced by geography.
Introduction
Migraine is a common neurological disorder characterised by recurrent, mostly unilateral, pulsating headache of moderate to severe intensity that is often accompanied by nausea and/or sensitivity to light and sound,1 2 which has a wide range of negative effects on the daily life of patients. Migraine without aura (MwoA) is the most common type of migraine, accounting for about 80%.1 It has been reported that migraine affects 1 in 10 people worldwide with a higher prevalence occurring in women,3 about two to three times that of men.4 5 Epidemiological surveys reported that the prevalence of migraines is about 9.3% (12.8% for women and 5.9% for men) in China.6 According to the global burden of disease calculation, migraine was recognised as the second most disabling condition worldwide in 2016.7 Increasing evidence shows that migraine is a strong risk marker for cardiovascular disease,8 9 psychiatric disorders10 11 and sleep disorders,12 13 and severe attacks may even lead to self-harm and suicide.14 Migraine causes the loss of 270 workdays per year per 1000 persons in the general population.15 Because of the high prevalence of migraine, the total annual cost for migraine was estimated to be $78 billion in the USA and €111 billion in Europe.16 17 The disability-adjusted life years and the financial burden of disease due to migraine are increasing year by year.18 19
At present, the treatment options for migraine are mainly based on prophylactic administration and pain medication during attacks.20 But the limitations include incomplete efficacy, side effects and contraindications, highlighting the need for non-pharmacological options for migraine treatment.21 Acupuncture has the advantage of being highly effective and safe in the treatment of migraines,22 23 which has been internationally recognised. One study showed better efficacy of manual targeting for the prevention of MwoA attacks relative to sham acupuncture and conventional treatment, which significantly reduced the days of migraine attacks.24 It has also been found in studies comparing the efficacy of acupuncture with sham acupuncture and waiting to treat migraine that long-term acupuncture treatment significantly reduced the frequency of migraine attacks, migraine days, pain intensity and medication use.25 Another study also showed that acupuncture is as effective as the best available medication and better than medication in terms of adherence and side effects.26
Contralateral acupuncture (CAT), also called opposing needling (Jùcì), is an ancient classic acupuncture technique introduced in classic Chinese literature on acupuncture (Huang Di Nei Jing) that is more than 2000 years old. It refers to the acupoints on the right side (healthy side) selected for diseases on the left (affected side) and vice versa.27 CAT has been used for a long time in China. Modern studies have shown that CAT has good efficacy in the treatment of painful disorders,28 29 and also shows a trend of positive efficacy in migraines. Some studies have even shown that CAT has better efficacy than ipsilateral acupuncture (IAT).30–32 However, credible evidence is insufficient and there is still a lack of high-quality randomised controlled trials to prove the effectiveness of the CAT.
As a type of acupuncture, the mechanism of action of CAT is related to the regulation of the relevant brain centres. An animal study has demonstrated that acupuncture points on the healthy side of rats with transient middle cerebral artery occlusion can effectively improve motor function and exert neuroprotection against ischaemia, and such effects may be mediated through the γ-Aminobutyric acid receptor-cyclic adenosine 3’,5’-monophosphate (cAMP)/protein kinase A/cAMP-responsive element binding protein signal transduction pathway.33 For the inflammatory pain model of rats, lesions of the rostral anterior cingulate cortex (ACC) completely abolished the anti-nociceptive of Electro-acupuncture effects of the healthy side but not the affected side.34 Another study also found that the ACC may play a direct role in the regulation of the brain by the CAT at ST38 in patients with shoulder pain.35
Migraine is characterised by a left–right distribution of pain, and there are also left–right differences in its pathogenesis. Some studies have shown left–right vascular shunting in migraine,36 left–right asymmetries in substances involved in pain, such as dimethylarginine,37 and differences in the left–right functional response of the central hemisphere.38 Whether there is modulation of the central brain mechanisms around acupuncture for migraine has not been confirmed by studies, but as a verification of the efficacy of CAT, migraine is certainly a good vehicle for the disease. To our knowledge, migraine is higher in women than in men, and the pain is more severe and more difficult to treat than in men.39 Previous studies have not studied MwoA in women separately. There is a need for a study of this particular cohort of women. In addition, most of the existing studies have demonstrated the efficacy of acupuncture for migraine through the IAT.24 40 A study comparing the efficacy of both CAT and IAT is necessary.
Objectives
The objective of this study is to evaluate whether CAT is more effective than IAT or sham acupuncture in reducing the days of migraine attacks in women with unilateral MwoA.
Methods and analysis
This study protocol was designed following the Standard Protocol Items: Recommendations for Interventional Trials guidelines41 (online supplemental file 1). The protocol of this study was approved by the Ethics Committee of the Sports Trauma Specialist Hospital of Yunnan Province (2021-03).
Supplemental material
Study design and setting
This trial was designed as a single-centre randomised and sham-controlled clinical trial to assess the efficacy of CAT on women with unilateral MwoA. This study will be conducted at the Second Affiliated Hospital of Yunnan University of Chinese Medicine. Two hundred forty-three women suffering from MwoA will be recruited. The study duration is about 20 weeks, which includes a pre-baseline period (4 weeks), two treatment periods (8 weeks) and two follow-up periods (8 weeks). The experimental group will receive acupuncture on the healthy side, control group 1 will receive acupuncture on the affected side and control group 2 will receive sham acupuncture on the healthy side. Each group will be given 30-minute treatment sessions, once every other day, approximately three times per week, for a total of 24 treatments, and follow-up visits will be conducted every 4 weeks for a total of two times. A flow chart of the research procedure is shown in figure 1. The schedule of patient enrolment, intervention and assessment is illustrated in table 1.
Study schedule for data measurements

Flow chart of the research procedure.
Recruitment and informed consent
All participants will be recruited from the outpatient Department of Neurology of the Second Affiliated Hospital of Yunnan University of Chinese Medicine and Kunming communities. A public recruitment advertisement for this trial will be designed to recruit the patients online or offline (eg, WeChat public account, websites). Neurologists will determine whether patients are eligible to participate in this study based strictly on inclusion and exclusion criteria. If patients who are interested and volunteer to participate in this trial meet the inclusion criteria, they will sign written informed consent before the start of the study. They will be fully informed of the research information including the study procedures, benefits and potential risks, except for the information about the needling site. They are free to withdraw from the study without penalty at any time without any negative impact on their future medical treatment.
Study population
Diagnostic criteria
Participants must meet the diagnostic criteria for MwoA in the International Classification of Headache Disorders (ICHD-3) developed by the International Headache Society in 2018,1 including the following five points:
At least five migraine attacks meeting the criteria of (2) and (4).
If untreated or unsuccessfully treated, each migraine attack lasts 4–72 hours.
In addition to the ‘unilateral’, at least one of the following three items are met: (1) throbbing; (2) moderate to severe headache (limitation or cessation of daily activities); (3) worsening of headache due to stairs or other similar daily physical activities or avoidance of daily activities due to headache.
At least one of the following two items is present during the migraine attack: (1) nausea and/or vomiting; (2) photophobia and phonophobia.
Cannot be attributed to other diagnoses in ICHD-3.
Inclusion criteria
Unilateral migraine, woman, age is between 18 and 60 years old (the starting age is less than 50 years old).
Meet the ICHD-3 diagnostic criteria for MwoA.
In the past 3 months, the number of monthly migraine attacks is greater than or equal to two times, and the days of migraine attacks are less than 15 days per month.
The severity of migraine attacks in the past 4 weeks (baseline period) is moderate to severe (average Visual Analogue Scale (VAS) score 4–9).
Have a history of migraine for more than 1 year.
Have not received acupuncture treatment within 1 month.
Volunteer to participate and sign the informed consent.
No other trials were taken within 3 months.
Excluded criteria
Patients with bilateral or alternating unilateral migraine.
People with a history of head trauma, other primary headaches and headaches of unknown diagnosis, or cervicogenic headache.
Combined with serious primary diseases such as cardiovascular and cerebrovascular, liver, kidney and haematopoietic systems and other organic diseases.
Combined with severe anxiety, depression, insomnia, and another psychiatric disease or intellectual disabilities, which cannot make them answer the questionnaire, or infection, bleeding disorders, allergies and skin diseases.
Pregnancy, lactation or those who have fertility requirements in the next 6 months.
Having the habit of taking analgesic and psychotropic drugs for a long time.
Cannot understand or record in the headache diary.
Those who have participated in similar research within 3 months.
Removed criteria
Patients who do not meet the inclusion criteria but are mistakenly enrolled.
Decide to withdraw from the study.
Occurrence of severe adverse events (AEs) or complications that result in stopping the trial.
Initiate other care such as changing their prophylactic medication, other physiotherapy or likewise, or refuse to give feedback on treatment information.
Randomisation and blinding
The participants will be randomised in a ratio of 1:1:1 to the experimental group (CAT group), control group 1 (IAT group) and control group 2 (placebo group). To avoid selection bias, random numbers will be generated by an independent research assistant using a computer and sealed in opaque envelopes. After participants accept the principle of random allocation, they will randomly select an opaque envelope and obtain an allocation sequence number, which will be recorded into a case report form (CRF) by a specially assigned person. The participants, researchers, outcome assessors and statisticians will be blinded to the group allocation throughout the study. Considering the particularity of sham acupuncture manipulation, it is difficult to blind acupuncturists in the treatment process. However, they will receive specialised training before participating and will not disclose the allocation status of the participants at any moment. The allocation will only be revealed under some AEs, such as severe infection, uncontrolled pain, etc. Throughout the trial, all participants will be treated in different rooms to prevent communication.
Intervention
The interventions are compliant with the Consolidated Standards of Reporting Trials42 and the Standards for Reporting Interventions in Clinical Trials of Acupuncture.43 Based on clinical experience, previous researches and the traditional Chinese medicine (TCM) theory that most migraines are Shaoyang meridian headaches, Shu and specific points of Shaoyang meridian will be selected as the prescription. It includes TE3 (Zhongzhu), TE5 (Waiguan), GB41 (Zulinqi), GB34 (Yanglingquan), GB20 (Fengchi) and GB8 (Shuaigu). All acupoints will be localised based on the WHO Standard Acupuncture Point Locations 2010 (ISBN: 9787117123327). Locations of the acupoints are presented in table 2 and figure 2.
Location of acupoints
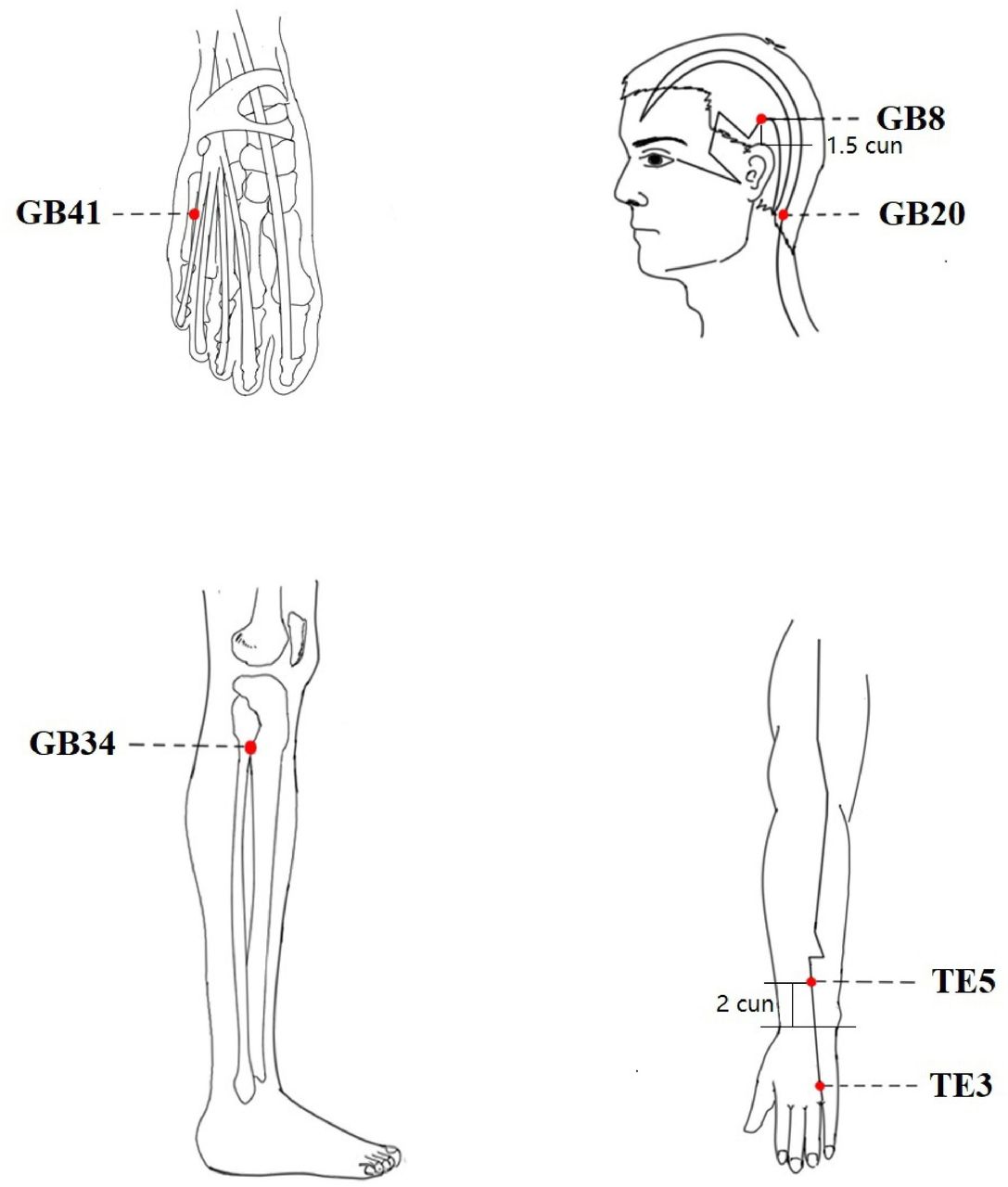
Location of acupoints.
Appliance selection
Park Sham Acupuncture Device (PSD) (see figure 3): includes transparent guide tube (Φ4×20 mm, Φ3×35 mm), double-sided tape (Φ1×15 mm) and the opaque plastic base (Φ4×15 mm, Φ5×10 mm), Suzhou Medical Supplies Factory, lot number 210401, China.
Acupuncture needle: use the Huatuo brand disposable acupuncture needles produced by Suzhou Medical Supplies Factory, China. Manufacturer’s license number: Su Food and Drug Administration (SFDA) of Machinery Production 20010020; Registration certificate number: 201622770970. Specifications of acupuncture are 0.30× (25 mm, 40 mm).
Blunt needle: use retractable stainless steel blunt needle (0.25×25 mm, 0.25×40 mm), Suzhou Medical Supplies Factory, lot number: 200304, China.

Park Sham Acupuncture Device.
Operation
Before the acupuncture operation, participants take a supine position and acupuncturists routinely disinfect the skin around the points. All three groups will use the PSD.
Experimental group
PSD+acupuncture needle will be used. After removing the skin side of the base of the PSD double-sided tape, import the disposable acupuncture needle, exposing the tip of the needle, it will be fixed on the acupuncture point and pierced into the skin, and the twisting, lifting and inserting, flat complementary and flat diarrhoea techniques will be performed to achieve the needling sensation.
Control group 1
The operation is the same as the experimental group.
Control group 2
The sham needle apparatus will be used. After removing the skin-facing double-sided tape on the base, a retractable blunt needle will be introduced, and the blunt needle tip will retract back into the hollow needle handle by force when it touches the skin and will not pierce the skin, but the participants will feel the sensation of the needle prick. The acupoints on the extremities will be glued to the skin by means of double-sided tape on the base, and on the head, which is affected by the hair; we will use hairpins to fix them (see figure 4).

Retaining needle. The person depicted is not a patient and the picture was taken with the participant’s knowledge.
In all three groups, the needles will be retained for 30 min per session, and the needle acupuncture will be performed every 15 min during the treatment. Treatments will be performed by qualified TCM acupuncturists with at least 3 years of clinical experience. They are all from the Department of Acupuncture of the Second Affiliated Hospital of Yunnan University of Chinese Medicine.
Concomitant medications
On the first visit, participants will provide information about other diseases they currently have and the corresponding medications used, including the name of the drug (or name of other therapy), indications, dosage unit, frequency of administration, route of administration, and start and end times of medication administration. All information will be recorded in the CRFs. In general, participants should not take any analgesic medication during the study period. However, according to the Chinese Migraine Guidelines (2016 edition),44 ibuprofen sustained-release capsules (manufacturer: Tianjin Smith Kline & French Laboratories, Tianjin, China; SFDA approval number: H20013062), like non-steroidal anti-inflammatory drugs, may be taken for pain relief when a migraine attack is unbearable. However, the usage must be recorded in the headache diary. All information about concomitant medications will be compared between the groups using the Χ2 test or Fisher’s exact test.
Outcomes
Primary outcome
The primary outcome is the change in days of migraine attacks, for which the headache diary is the source of data. The assessors will supervise and collect the records of participants completing their headache diaries from baseline to week 16 in a handwritten format, and assess their results. The headache diary is designed to record details of migraine attacks, including duration, frequency, location, intensity, any aura, cause and effect of the migraine and accompanying symptoms of each migraine attack. Participants will also record in the headache diary the intake of acute headache medication (including name, dose, time of dosing, time to pain relief and side effects of analgesic medication) for each migraine attack.
Secondary outcomes
The secondary outcomes are changes in frequency of migraine attacks, intensity of migraine, migraine duration, the dose of intake of acute medication, the Migraine-Specific Quality of Life Questionnaire (MSQ), Migraine Disability Assessment Score (MIDAS), Headache Impact Test-6 (HIT6) and Pittsburgh Sleep Quality Index (PSQI) at the baseline time (week 0), end of treatment (week 8–12) and the follow-up time (week 12–16). Blinding/credibility will be evaluated at end of treatment (week 8–12).
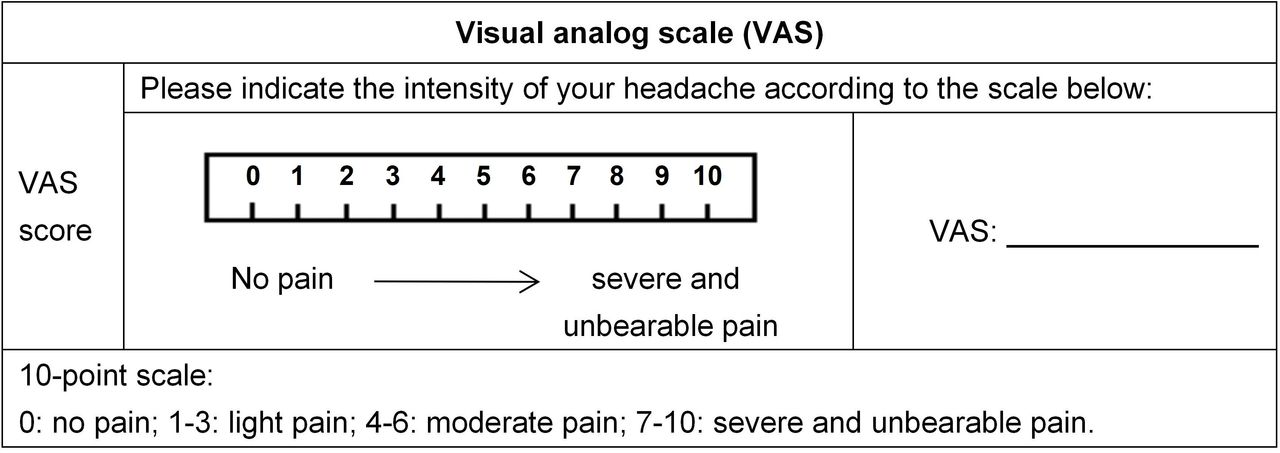
Migraine attack level is measured by using a VAS with scores 0–10. Participants will be asked to mark their level of pain on the VAS. They will not be allowed to access their previous VAS records during subsequent sessions. The VAS of pain is shown in figure 5.
The MSQ is a 14-item questionnaire that includes three domains. Scores range from 0 to 100, with higher scores indicating better quality of life.45
The MIDAS is a five-question scale with scores 0–27 indicating assessment of headache-related disability in terms of the number of days in the past 3 months and activity limitations due to the migraine.46
The HIT6 is a six-item questionnaire with scores 36–78. When the total score reaches 60, it indicates that the headache is having a serious impact on the patient’s life.47
The PSQI is designed to differentiate between ‘poor’ and ‘good’ sleep by measuring the quality and pattern of sleep over the past 4 weeks. The total score ranges from 0 to 21, with higher scores indicating poorer sleep quality.48
Blinding/credibility test is used to assess the success of blinding. After each session, the participants will be surveyed on whether they think they had undergone active treatment (‘yes’ or ‘no’) and how strongly they believed that active treatment was received (numerical rating scale 0–10).49 A simple de-blinding questionnaire will be provided to participants.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
The Visual Analogue Scale of pain.
These questionnaires will be repeatedly assessed by one physician who is blinded to group allocation to ensure consistency. The data will be compared across the three groups, that is, CAT versus sham acupuncture and IAT versus sham acupuncture.
Sample size
Following a previous study, after 8 weeks of treatment and 8 weeks of follow-up, the reduction in the average number of migraine days was 3.5±2.5 and 2.4±3.4 in the acupuncture group and the sham acupuncture group, respectively.24 Another study reported that acupuncture on the healthy side can be 20% more effective than acupuncture on the affected side.30 We anticipate that the change in the average number of migraine days in the opposing acupuncture group will be 3.9±2.5, the acupuncture on the affected side group will be 3.1±2.4, and in the sham acupuncture group, it will be 2.1±2.8. PASS V.11 software (NCSS, Kaysville, Utah, USA) was used to calculate that, based on 90% power to detect a significant difference (α=0.025, two-sided); 73 participants will be required for each group. Considering a 10% withdrawal rate, a sample of 243 participants (81 participants in each group) will be recruited.
Statistical analysis
The statistical analysis will be performed by independent statisticians who are blinded to group allocation and the intervention process. Before data analysis, the research group will draw up a statistical plan, including the required data and method of data processing.
The demographics, baseline characteristics and efficacy of acupuncture on the participants will be analysed with different methods by SPSS V.22.0 statistical software. Categorical data will be described as percentages (n%). Continuous data will be shown as mean±SDs and IQRs.
On whether the data are normally distributed, a t-test or Wilcoxon rank-sum test will be used for continuous data, and Χ2 test or Fisher’s exact test will be used for categorical data for baseline analysis. Comparisons among the three groups will be analysed by one-way analysis of variance (ANOVA), and non-parametric tests will be used when non-normally distributed. The primary outcome will be assessed using a one-way, repeated measures ANOVA to test the effect of time, group and time×group interactions on migraine attacks. Comparisons of categorical data among groups will be tested by Χ2 test or Mann-Whitney U test. Data analysis will be based on the intention-to-treat principle, two-sided tests will be used during the analysis and a p value of <0.025 will be considered as the threshold of statistically significant.
Patient and public involvement
Patients and the public will not be involved in the planning or design of the study. They will not be involved in the recruitment, conduct or report of the study. The study results will be disseminated to the participants and to the public in the form of educational talks and booklets or flyers and via publication of results.
Trial status
The trial was commenced on 30 September 2021 and is currently at the stage of recruiting patients. The anticipated date of recruitment completion is 30 December 2022 and the trial is expected to be completed by 1 October 2025.
Data management and confidentiality
Each participant’s CRF will be completed by the investigator in a timely and careful manner, including headache diary, assessment scales, combined medication use, treatment compliance, AE, etc. The investigator will only draw lines for any changes in the CRFs for information, record the modified data, sign and provide date so that the original records will not be erased or overwritten. The data collectors are responsible for keeping and managing various data and performing rigorous proofreading of the data, and those who have already passed one/two course/s of treatment should enter the efficacy statistics. The study director will regularly check the authenticity of the data collection. Personal information of all participants such as the name, phone number, ID number and medical records will be kept anonymous to prevent information leakage. All participants’ paper data will be kept by the researchers in a special cabinet and preserved for at least 5 years after publication. The Ethics Committee of the Sports Trauma Specialist Hospital of Yunnan Province will periodically review the progress of the trial and monitor the collection, allocation and concealment of data. The modification or termination of the trial can be implemented by the committee. The data monitoring committee is independent of the sponsor and has no conflict of interest.
AE reporting and safety monitoring
During the study, participants receiving acupuncture treatment may experience AEs, such as pain, subcutaneous congestion or haematoma, local infection, broken needles, even syncope or other severe events. Whether the AEs are related or not to the treatment in this study, they will be handled appropriately and timely and recorded in the CRFs carefully and reported to the study director and the Ethics Committee of the Sports Trauma Specialist Hospital of Yunnan Province. If the AE is severe and associated with the trial, the participant will be given appropriate treatment. During the study period, if participants develop any potential exacerbation of symptoms or develop other new serious illnesses that will affect the observation of the trial, they will be offered emergency treatment and then, based on physicians’ assessment of the condition, they will be stopped from treatment and the data will be extracted. All AEs will be compared between the groups using the Χ2 test or Fisher’s exact test.
Ethics and dissemination
This study has been approved by the Ethics Committee of the Sports Trauma Specialist Hospital of Yunnan Province on 9 September 2021 (2021-01) and conformed to the Declaration of Helsinki. All participants must provide written informed consent before participating in the trial (online supplemental file 2). Data handling will be done anonymously, and only the participant code will be available in the central database. All personal information on potential and enrolled participants out of the scope of this trial will not be collected, shared or maintained to protect confidentiality before, during and after the trial. The results of this study will be published in a peer-reviewed journal and presented at conferences.
Supplemental material
Discussion
In view of its high prevalence and impact on functional disability, migraine has a significant impact not only on individuals but also on the social economy.1 2
The clarification of the pathogenesis of migraine and the development of effective treatment are still major issues in migraine management. Acupuncture is now gaining attention as a green, safe and effective alternative therapy.
Studies have shown that acupuncture treatment of migraine can be involved in analgesia by stimulating the body’s release of related peptides, cytokines, hormones, neurotransmitters and other analgesic substances.50 The periaqueductal grey (PAG) is the main pain information processing centre and relay station,51 which produces analgesic substances such as 5-hydroxytryptamine, endogenous substance P and opioid peptides.50 52 PAG nerve fibres connect the telencephalic cortex and subcortex; mesencephalon, brainstem, spinal cord and cerebellum, as well as the analgesic pathways involved, are also important pathways regulated by acupuncture.53 54 It can be seen that acupuncture for migraines is closely related to the regulation of PAG. Whether the mechanism of the CAT for migraine is also acting through the regulation of PAG has not been confirmed by studies. Based on the fact that the PAG is the main pain information processing centre and relay station, it has its regulatory role, as well as the ‘hub’ function of upward and downward transmission and integration.51 Our previous study found that the reduced resting state functional connectivity between the PAG and rostral ACC/medial prefrontal cortex connections was associated with increased migraine headache intensity.55 Migraine has a left–right distribution of headache sites, so it is scientifically feasible to verify the effectiveness of the CAT by taking unilateral migraine as the study object.
According to the theory of acupuncture, following the meridians is the primary principle of acupuncture point selection. The distribution area of migraine belongs to the Shaoyang meridian of the TCM meridians, both the Sanjiao meridian of hand Shaoyang and the gall bladder meridian of foot Shaoyang pass through the migraine area, so the acupoints on these two meridians will be selected. Meanwhile, most of the previous studies on acupuncture for migraines also focused on the acupoints of Shaoyang meridian,24 40 and both Shu points and specific points have pain-relieving effects, so this study mainly used the Shu points and specific points of the Shaoyang meridian as the prescription for acupuncture.
In this study, the design of sham acupuncture was challenging to control. In previous migraine studies, non-acupoints insertion has been used as sham controls.56 57 However, some studies have shown that this acupuncture produces greater effects than medicated placebo.58 Another method of non-penetrating acupuncture has also been used in clinical trials in migraine, with the advantage of minimising the physiological effects produced by sham acupuncture.59 However, some researchers have also suggested that non-penetrating acupuncture is prone to blinding bias, especially as Chinese people generally expect acupuncture to achieve a special feeling, thus this method may not be feasible.25 60 There does not appear to be a good sham-needle approach that is effective in avoiding the production of blind deflection and also approaches the effect of medicated placebo. Considering the effect of non-acupoints insertion modalities on efficacy, we chose to use non-penetrating acupuncture with blunt needles as a control. For minimising bias caused by unblinding, we requested that the acupuncturist touch the blunt needles to the surface of the acupoint as much as possible so that the patients could feel a slight stinging feeling to reduce the differences in acupuncture sensation, and designed a blinding evaluation scale to ensure the validity of the blinding.
This study protocol can be seen in light of some limitations. First, even non-insertion with blunt needles in the skin may induce widespread peripheral, segmental and central physiological responses of unpredictable magnitude. Second, this study did not use a positive drug and a placebo drug as control groups, which carries some risk in terms of efficacy and blinded assessment. Third, due to financial and manpower limitations, this trial was not set up as a multicentre study and the results of the study may be influenced by geography.
Our study design presents a treatment method for a choice of acupuncture at contralateral or ipsilateral for the treatment of MwoA. First, by comparing the efficacy of the CAT group and IAT group, it can be concluded whether CAT is more effective and provide a basis for clinical decision-making; comparing the CAT group with the placebo group can further support the efficacy of CAT. Second, the results of this study will be a powerful validation of the classic traditional Chinese acupuncture theory and will provide support for the succession and development of acupuncture in Chinese medicine. Third, the results of this study can provide a clinical basis for the treatment of other unilateral diseases and further research into the mechanisms of intercross regulation in the brain.
In summary, previous acupuncture trials have demonstrated that acupuncture is effective on MwoA.24–26 However, most of the trials were on IAT and there is a lack of evidence to support the effectiveness of CAT. Taking women with MwoA as the study participants, the purpose of this trial is to evaluate whether CAT is more effective than IAT or sham acupuncture in women with unilateral MwoA, to provide an effective way to choose CAT or IAT for the treatment of MwoA, and to provide a clinical basis for the treatment of other unilateral diseases and further research into the mechanisms of intercross regulation in the brain.
Ethics statements
Patient consent for publication
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
QL and JF contributed equally.
Contributors QL and JF contributed equally to this work and are co-first authors. TG and LZ are co-corresponding authors. TG, LZ, QL and JF contributed to the protocol design and writing of the manuscript. CX is responsible for monitoring the processes of the trial. YW is responsible for the design of randomisation. SZ, YZ and MK are responsible for data entry. XZ is responsible for acupuncture treatment. XZ and YS are responsible for guidance and statistics. All authors approved the final manuscript.
Funding This work was supported by the National Key R&D Program of China (2019YFC1709700), the Youth Special of Yunnan Province Ten-thousand Plan (YNWR-QNBJ-2019-257), Science and Technology Innovation Team for Acupuncture, Moxibustion and Tuia Prevention and Treatment of Neurological Diseases in Yunnan Universities (2019YGC04), Scientific and technological innovation team of classical needling and acupoint matching application of Yunnan Provincial Education Department in 2022.
Disclaimer The funding agencies do not play any role in the design, collection, analysis or writing manuscripts of the study.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.