Article Text

Abstract
Objectives We investigated machinelearningbased identification of presymptomatic COVID-19 and detection of infection-related changes in physiology using a wearable device.
Design Interim analysis of a prospective cohort study.
Setting, participants and interventions Participants from a national cohort study in Liechtenstein were included. Nightly they wore the Ava-bracelet that measured respiratory rate (RR), heart rate (HR), HR variability (HRV), wrist-skin temperature (WST) and skin perfusion. SARS-CoV-2 infection was diagnosed by molecular and/or serological assays.
Results A total of 1.5 million hours of physiological data were recorded from 1163 participants (mean age 44±5.5 years). COVID-19 was confirmed in 127 participants of which, 66 (52%) had worn their device from baseline to symptom onset (SO) and were included in this analysis. Multi-level modelling revealed significant changes in five (RR, HR, HRV, HRV ratio and WST) device-measured physiological parameters during the incubation, presymptomatic, symptomatic and recovery periods of COVID-19 compared with baseline. The training set represented an 8-day long instance extracted from day 10 to day 2 before SO. The training set consisted of 40 days measurements from 66 participants. Based on a random split, the test set included 30% of participants and 70% were selected for the training set. The developed long short-term memory (LSTM) based recurrent neural network (RNN) algorithm had a recall (sensitivity) of 0.73 in the training set and 0.68 in the testing set when detecting COVID-19 up to 2 days prior to SO.
Conclusion Wearable sensor technology can enable COVID-19 detection during the presymptomatic period. Our proposed RNN algorithm identified 68% of COVID-19 positive participants 2 days prior to SO and will be further trained and validated in a randomised, single-blinded, two-period, two-sequence crossover trial.
Trial registration number
ISRCTN51255782; Pre-results.
- COVID-19
- Health informatics
- VIROLOGY
- Public health
- Infection control
- Health & safety
Data availability statement
Data are available on reasonable request. Anonymised data that underlie the results reported in this article are available on justified request to the corresponding author.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
Large sample size from a well-characterised and healthy national cohort.
Wearable device technology combined with machine learning to monitor health parameters related to early detection of COVID-19 infections.
Solely data from laboratory confirmed COVID-19 infections were used.
Data from one single study centre may limit the generalisability of our findings.
Small subsample of COVID-19 positive cases with sufficient high-quality data.
Introduction
One of the primary ways of controlling the spread of SARS-CoV-2 involves identification, tracing and isolation programmes implemented in several countries.1 With multiple SARS-CoV-2 variant strains emerging, countries have prioritised vaccine rollouts, searches for alternatives to quarantine and identification of individuals with COVID-19. Reverse transcription-polymerase chain reaction (RT-PCR), serological testing, surveys, temperature measurements and symptom checks are used to detect COVID-19.2 However, these methods are usually unable to identify presymptomatic or asymptomatic individuals.
Recent studies have highlighted the need to identify potential cases prior to symptom onset (SO) to prevent virus transmission.2 3 Asymptomatic patients are likely to ignore safety precautions, leading to increased virus transmission. Detection of COVID-19 during the asymptomatic or presymptomatic stage facilitates early isolation, thereby limiting contact with susceptible individuals. Commonly reported COVID-19 symptoms include fever, coughing, chest tightness, difficulty breathing, fatigue, dyspnoea, myalgia, sputum production, headache and gastrointestinal symptoms.4 5 While molecular tests are continuously used to confirm infections, the logistics and costs of repeat tests across populations are prohibitive.6 Recently, scientists have called for further research investigating whether wearable medical devices such as Ava-bracelets and direct-to-consumer products such as Fitbit,7 8 smartwatches8 9 and other activity trackers10 could be used for such surveillance.11
Here, we assess the use of an existing regulated wearable medical device (Ava-bracelet) to analyse COVID-19-related changes in various physiological parameters across four infection-related periods: incubation, presymptomatic, symptomatic and recovery. To our knowledge, this is the first prospective study to measure physiological changes in respiratory rate (RR), heart rate (HR), HR variability (HRV), wrist-skin temperature (WST) and skin perfusion to develop an algorithm to detect presymptomatic COVID-19 infection.
Methods
Study design and participants
Participants from the ongoing observational population-based prospective cohort study (Genetic and Phenotypic Determinants of Blood Pressure and Other Cardiovascular Risk Factors (GAPP); n=2170) in the Principality of Liechtenstein were invited to participate in the current study (COVI-GAPP).11 Active since 2010, the GAPP study was designed to understand the development of cardiovascular risk factors in the general population better (ie, healthy adults aged 25–41 years).12 The exclusion criterion regarding participation in the COVI-GAPP study was individuals who did not provide written informed consent. The first COVI-GAPP participants were enrolled in April 2020, and the data used for this interim analysis was collected through March 2021 (n=1163). This COVI-GAPP interim analysis was preplanned as a pilot study to provide an initial algorithm for the COVID-RED project (n=20 000), a randomised, single-blinded, two-period, two-sequence crossover trial.13
Bracelet, app and participant compliance
The Ava-bracelet (version 2.0; Ava AG, Zurich, Switzerland) is an FDA-cleared and CE-certified fertility aid bracelet that complies with international regulatory requirements and applicable standards.14 15 The wrist-worn tracker is commercially available at US$ 279 and consists of three sensors that measure five physiological parameters simultaneously: RR (breaths per minute), HR (beats per minute), HRV (ms), WST (°C) and skin perfusion (online supplemental figure S1). Although the Ava-bracelet measures multiple forms of HRV, we focused on two time-dependent and one frequency-dependent measurements: SD of the normal-to-normal interval (SDNN), root mean square of successive differences (RMSSD) and HRV ratio (see online supplemental material). In addition to the physiological parameters of interest, the Ava-bracelet measures sleep quantity (duration) and sleep quality using a built-in accelerometer. Prior studies have demonstrated how device data can inform a machine-learning algorithm that detects ovulating women’s most fertile days in real time with 90% accuracy.16 Worn only while asleep, the Ava-bracelet saves data every 10 s and requires at least 4 hours of relatively uninterrupted sleep. The participants synchronised their bracelets with a complementary smartphone app on waking, transferring data from the device to Ava’s backend system.
Supplemental material

COVI-GAPP participants (n=1163) wore a certified medical device at night while they slept, syncing it to a complementary smartphone application on waking. The device and app were originally designed for fertility tracking in naturally menstruating women but adapted for the purposes of this study. Instead of real-time fertility indications, participants saw ‘Fertility Unknown’ on syncing (A). Additionally, the in-app daily diary asked participants about potential confounds (B) and COVID-19 symptoms (C) rather than fertility-related questions.
Although no study-specific adjustments were applied to the hardware of the Ava-bracelet, the complementary app had a customised user functionality developed by the manufacturer specifically for the COVI-GAPP study. Participants could still see and monitor changes in the physiological parameters in the app; however, they did not receive messages or algorithm-driven interpretations of their data (figure 1A). Participants recorded behaviours that may have interfered with the physiological parameters of interest (eg, alcohol, medication and drug intake), as such substances can alter central nervous system functioning (figure 1B).17 The daily diary in the custom app enabled participants to record COVID-19-related symptoms (figure 1C). To ensure the highest quality data, the study team reviewed a weekly compliance log that indicated which participants had synced their Ava-bracelets with the app during the preceding week.18 The study team followed up with the participants individually to mitigate operational challenges or log in issues.
SARS-CoV-2 antibody testing and RT-PCR testing
SARS-CoV-2 antibody tests were assessed at baseline (starting April 2020) and during follow-up (starting December 2020) by the medical laboratory Dr. Risch Ostschweiz AG (Buchs SG, Switzerland). The tests were assessed with an orthogonal test algorithm that employed electrochemiluminescence assays. These assay test for pan-immunoglobulins directed against the N antigen and the receptor-binding domain of the SARS-CoV-2 spike protein.19 Seroconversion was assumed if the first blood sample was negative for SARS-CoV-2 antibodies and the second sample was positive.
If participants had any symptoms during the study period, they were encouraged to visit the Liechtenstein National Testing Facility for RT-PCR testing. The testing facility was open daily allowing for higher testing frequencies than that in other European countries.20 RT-PCR was performed on either the COBAS 6800 platform (Roche Diagnostics, Rotkreuz, Switzerland) or the TaqPath assay on a QuantStudio 5 platform (Thermo Fisher Scientific, Allschwil, Switzerland).20–22 Participants diagnosed with COVID-19 contacted the study team to discuss their symptoms and health statuses. Additionally, participants provided their date of SO and overall symptom duration, enabling us to calculate the symptom end (SE) date.
Questionnaires
For the second antibody test, all participants were asked to complete a questionnaire providing personal information (age, sex), smoking status (current, past, never), blood group (A, B, AB, 0, unknown), number of children, exposure to household contacts who tested positive for COVID-19, working with people who have tested positive for COVID-19, and vaccination status. We calculated the body mass index (BMI) based on the height and weight collected from the GAPP database.
Statistical analysis
The primary objective was to determine whether different physiological parameters deviated from the baseline during COVID-19 infection. This information was used to develop a model for predicting COVID-19 infection before SO. To evaluate whether RR, HR, HRV, WST and skin perfusion deviated from baseline measurements during the four infection-related periods, we categorised the daily parameter measurements as occurring at baseline if the day (d) was >10 days prior to SO (ie, d>SO-10), the incubation period as SO-10 ≤d < SO-2, and the presymptomatic period as SO-2 ≤d < SO. We chose a cut-off of −2 days based on previous reports of infected participants becoming contagious 2 days before SO.23 Because the participants’ reported symptom durations varied, the measurements were categorised into the symptomatic infection category if SO≤d ≤ SE. Finally, the parameters collected after SE were classified as being in the recovery period (d>SE).
Development of a machine-learning algorithm for detecting presymptomatic COVID-19 infection
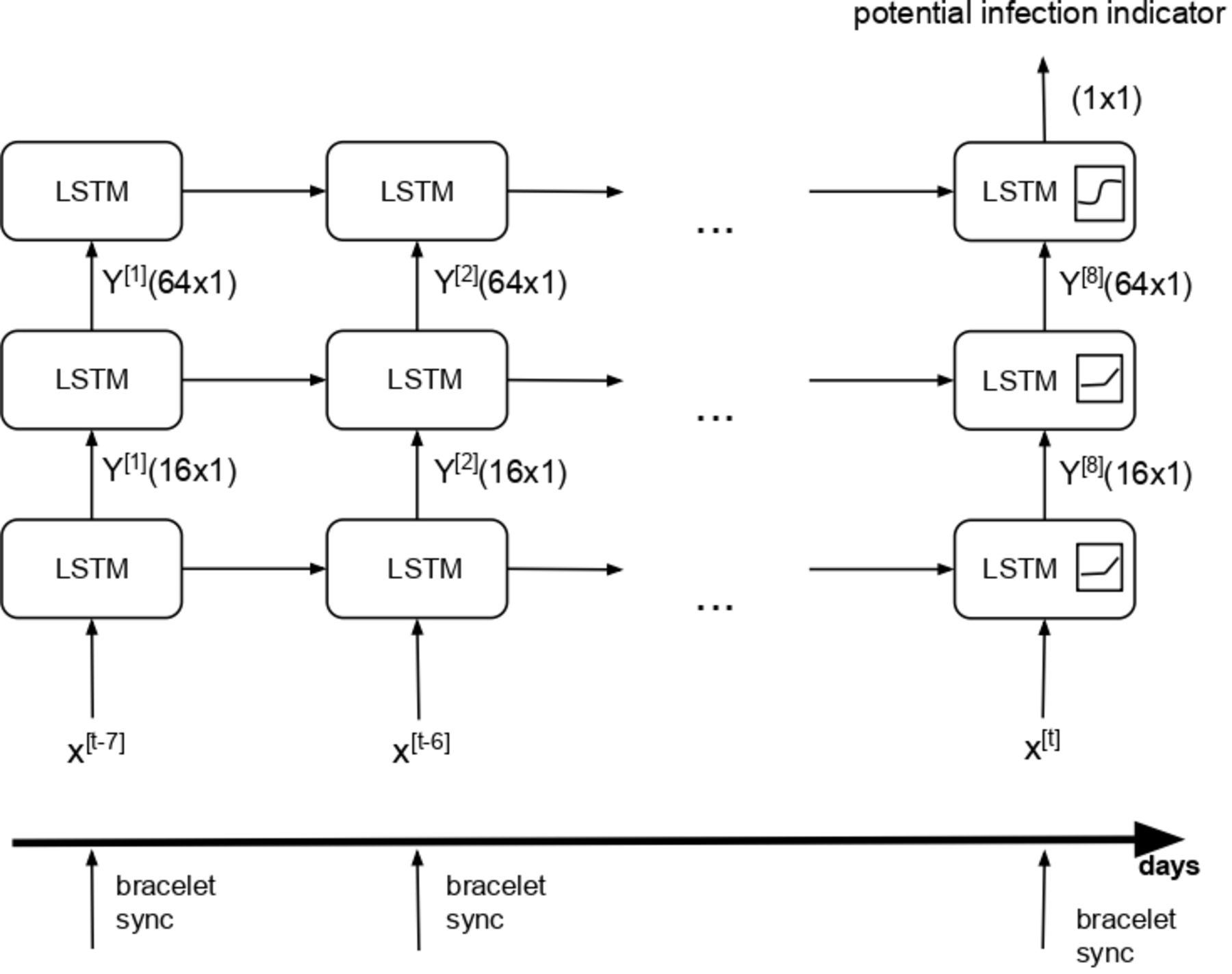
We chose a recurrent neural network (RNN) with long short-term memory (LSTM) cells for the binary classification of an individual as healthy or infected (positive for COVID-19) on a given day. LSTM networks have proven to be highly accurate in recognising time series patterns and events across large datasets.24 The internal structure of such networks can memorise states and easily fetch or activate them, even if they were created many epochs ago. The LSTM network we implemented consisted of two hidden layers with 16 and 64 cells (figure 2). Its output activation was a sigmoid function, whereas the recurrent activation was a hyperbolic tangent (tanh) function. The output was limited to a range between 0 and 1 to ensure that the model yielded an overall probability of infection on a given day. A potential COVID-19 infection was indicated when this probability exceeded 0.5.

Recurrent neural network (RNN) architecture for the detection of a presymptomatic case of COVID-19. The RNN consisted of two hidden layers and one output layer. The first hidden layer contained 16 and second layer contained 64 long short-term memory (LSTM) units. The LSTM output activation was a sigmoid function, while the recurrent activation on hidden layers was the rectified linear unit function. The input of RNN was eight consecutive values of physiological signal originating from eight consecutive nights of data. The output was an indication about the potential COVID-19 infection.
Data processing and multilevel model specification
All data processing and analyses were performed in R (version3.6.1) and Python (version3.6). Preprocessing of the data was performed to remove potential artefacts and ensure consistency with best practices25 (see online supplemental materials for detailed description). Further, we ran a series of multilevel models with random intercepts and slopes to determine the differences in physiological parameters during the infection-related periods compared with baseline. Given our continuous criterion, we modelled our outcomes of interest using residual maximum likelihood estimation and Satterthwaite df. Four binary variables were created, indicating the infection period to which a given measurement belonged (1=belonging to that period, 0=not belonging to that period). The reference baseline-period measurements were encoded as zero across all four binary variables. The reported results included unstandardised regression coefficients for each effect. When multiple models were possible for the same parameter, we chose the model using the percentile of the data (stable maxima) with the best fit (see online supplemental materials). To ensure a family-wise alpha level less than or equal to 0.05, we implemented Bonferroni correction for the seven analysed parameters (corrected alpha level of p=0.007) and adjusted the definition of marginal significance accordingly (ie, 0.007≤p ≤ 0.05).
Data preparation and feature extraction for algorithm development
The Ava-bracelet records over a million data points per use. Therefore, we first identified the features that are most predictive of COVID-19. We normalised the night-time WST, RR and HR values to prime our model to detect deviations from baseline measurements and ensure greater stability in the measurements (eg, to minimise interparticipant variability). Next, we compared the predictive performance of the raw features before engineering the novel composite features. We conducted a principal component analysis decomposition to test the correlation between the day of SO and other binary-labelled features (eg, alcohol consumption). We also examined the correlation between WST and other physiological parameters to determine the potential autocorrelation prior to the model specification.
Training process
To limit our analysis to symptomatic COVID-19 cases, participants had to report the date of SO and record at least 28 days of bracelet data prior to that date. The full 4 weeks of data were required to ensure accurate baseline readings and enable the algorithm to account for cyclical variations in parameters attributable to monthly hormonal changes. Thus, each participant included in the analysis had at least 29 consecutive days of data recorded using the bracelet. We partitioned the data into 8-day sequences, enabling the algorithm to compare the physiological parameters across 8-day windows. This means that each user had more negative (class 0; ‘healthy’ days) sequences in the distribution3 11 18 19 25 26 than positive sequences (class 1; ‘infected’ days (eg, SO-10 to SO-2) as shown in figure 3). We selected a binary cross-entropy loss function for the RNN by using a stochastic gradient descent (SGD) optimiser. Owing to the sample size, we set the learning rate to 0.007 and 2000 epochs, while also enabling an early stopping mechanism to prevent model overfitting. We trained our RNN 10 times, randomly splitting our sample into a training set (70% of participants) and a test set (30% of participants) for each instance. We report the metrics of the best-performing RNN model selected according to the following recall equation:
overall_recall = ((recall_class_1_train+recal_class_0_train) * 0.7 + (recall_class1_test+recall_class_0_test) * 0.3)/2

Class depiction based on the recurrent neural network (RNN). Here, class 0 represents healthy days and class 1 represents the presymptomatic phase of COVID-19 (SO-10 to SO-2). Vectors of marked classes represent training input for the RNN. SO, symptom onset.
Finally, because of the number of COVID-19 cases compared with healthy days in our dataset, we upsampled instances of class one through duplication, such that it was represented in our training set 1.15 times more than a given negative sequence (ie, class 0). Thus, the SGD optimiser treated the two classes as roughly equal and no longer overweighted the importance of the parameters predicting a healthy 8-day period. By training this LSTM model, we sought to leverage deep learning to predict the presymptomatic onset of COVID-19.
Patient and public involvement
No patient or public involvement.
Results
Participants
A total of 1163 participants (mean age=44.1 years, SD=5.6; 667 (57%) females) were enrolled in the COVI-GAPP study (figure 4). Of these participants, 127 (10.9%; 95% CI (9.3 to 12.8)) contracted COVID-19 during the study period. Ten infected participants were hospitalised for short-term monitoring, with breathing difficulties and fever as the main reported symptoms. Three asymptomatic infected participants were retrospectively identified using antibody tests. As seen in table 1, there were no differences in the sex ratio, age, BMI or smoking status between individuals who did or did not test positive for COVID-19 during follow-up (all p≥0.30). A significantly higher proportion of participants who contracted COVID-19 reported household contacts (n=58 of 1036 seronegative participants vs 53 of 127 seropositive participants; p<0.001) or work colleagues who also had COVID-19 (n=230 of 1036 seronegative participants vs 49 of 127 seropositive participants; p<0.001). On average, COVI-GAPP participants wore the Ava-bracelet for 1370.8 hours over the course of the study (SD=802.7), for a total of 1 453 006 hours. Of the 127 participants who tested positive for COVID-19, either through RT-PCR and SARS-CoV-2 antibody tests or antibody tests only, 66 users had worn their bracelet at least 29 days prior to SO which enabled sufficient data quality. Among these 66 participants, COVID-19 infection was confirmed by RT-PCR test and SARS-CoV-2 antibody test (n=48) or solely by antibody test (n=18).

Study flow chart. From 2170 GAPP participants, 1163 participants were enrolled in the COVI-GAPP study. A total of 127 participants presented laboratory-confirmed COVID-19 disease and from these, a total of 66 positive tested participants had complete bracelet data available used for the algorithm development.
Overall participant characteristics stratified according to whether they contracted COVID-19
Participants with confirmed COVID-19
Table 2 shows the clinical characteristics of COVID-19 positive participants, stratified according to their compliance with wearing the Ava-bracelet prior to SO. A series of 26 analyses of variance and chi-square tests with Bonferroni correction revealed that only BMI varied significantly between the two groups; noncompliant participants had a higher mean BMI (25.8 kg/m2, SD=4.0) than their compliant peers (23.8 kg/m2, SD=3.7; F(1, 116)=10.39, p=0.002).
Clinical characteristics of participants who contracted COVID-19 stratified according to whether they did (compliant group) or did not (non-compliant group) wear the bracelet regularly
Compliant participants with confirmed COVID-19
Among the 66 compliant participants with COVID-19, 13 248 nights of data were collected (mean duration=200 nights, SD=47; range 72–284 nights) for a total of 124 079 hours (mean hours per participant=1880, SD=461.8). The compliant participants had a mean age of 42.9 years (SD=5.6) and most had never smoked (n=57; 86%). Their COVID-19 symptoms lasted for an average of 8.5 days (SD=5.0; range 1–25 days). Table 2 shows the frequency of the self-reported symptoms.
Physiological changes during the clinical course of COVID-19
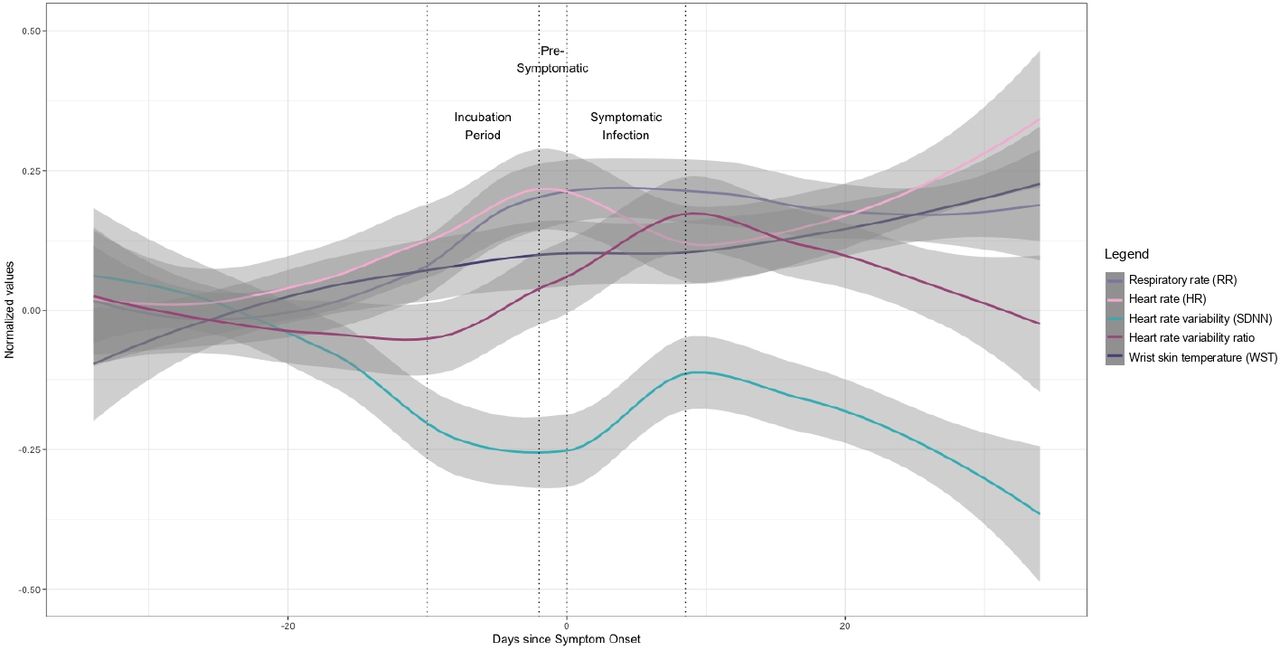
Employing multilevel modelling, we observed significant changes in five (RR, HR, HRV, HRV ratio and WST) of the seven device-measured physiological parameters during the incubation, presymptomatic, symptomatic and recovery periods of COVID-19, compared with baseline. Table 3 lists the unstandardised coefficient values for each statistical model. The complete course of the different physiological parameters is shown in figure 5.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
The wearable device can detect changes in five physiological parameters across the clinical course of COVID-19. The values of each physiological parameter (with 95% CIs) collapsed across individuals (n=66) were normalised using baseline measurements and are shown centred around participant-reported symptom onset (SO). SDNN, SD of the normal-to-normal interval.
Multi-level linear mixed models reveal the relationship between COVID-19 phases and physiological parameters
Respiration rate
COVID-19 positive participants had a significantly higher RR during the symptomatic period than at baseline ( = 15.1 breaths/min, SE=0.26; p<0.0001). Controlling for intraindividual variance, the nightly RR increased by 1.0 breaths/min (SE=0.18; p<0.0001). There were no significant differences in the RR detected between the baseline and other periods (all p≥0.114).
= 15.1 breaths/min, SE=0.26; p<0.0001). Controlling for intraindividual variance, the nightly RR increased by 1.0 breaths/min (SE=0.18; p<0.0001). There were no significant differences in the RR detected between the baseline and other periods (all p≥0.114).
Heart rate
At baseline, the participants had a resting nightly HR of 55.4 beats per minute (bpm; SE=0.83; p<0.0001). During the incubation period, individuals’ HR increased significantly by 0.87 bpm (SE=0.29; p=0.004). HR remained elevated in the presymptomatic period, expected to be 1.0 bpm higher than that at baseline (SE=0.36, p=0.007). HR continued to increase following SO, beating 2.2 bpm faster than at baseline (SE=0.48, p<0.0001). Finally, even after SE, participants had a significantly elevated HR (+0.87 bpm higher than baseline; SE=0.22, p=0.0002).
HRV: SD of the NN interval
Compared with a baseline SDNN of 59.6 ms (SE=1.4, p<0.0001), participants had significantly decreased SDNN in the incubation ( = −1.5 ms, SE=0.59, p=0.0149), presymptomatic (
= −1.5 ms, SE=0.59, p=0.0149), presymptomatic ( = −1.7 ms, SE=64; p=0.0086) and symptomatic (
= −1.7 ms, SE=64; p=0.0086) and symptomatic ( = −1.4 ms, SE=0.73; p=0.0499) periods. Following SE, SDNN returned to baseline levels (
= −1.4 ms, SE=0.73; p=0.0499) periods. Following SE, SDNN returned to baseline levels ( = −0.9 ms, SE=0.51, p=0.0787).
= −0.9 ms, SE=0.51, p=0.0787).
HRV: root mean square of successive differences
Our analyses did not reveal any significant phase-based differences in RMSSD for COVID-19 positive participants during their infection (all p≥157) compared with baseline ( = 43.7 ms, SE=1.2; p≤0.0001).
= 43.7 ms, SE=1.2; p≤0.0001).
HRV ratio
As with SDNN, multilevel analysis revealed a marginally significant decrease in HRV ratio during the incubation ( = −0.01, SE=0.01; p=0.0361) and presymptomatic periods (
= −0.01, SE=0.01; p=0.0361) and presymptomatic periods ( = −0.02, SE = −0.01; p=0.0165) compared with baseline (
= −0.02, SE = −0.01; p=0.0165) compared with baseline ( = 0.50, SE=0.02; p<0.0001). No significant difference in HRV ratio emerged between baseline and the symptomatic or recovery periods (all p≥0.5474).
= 0.50, SE=0.02; p<0.0001). No significant difference in HRV ratio emerged between baseline and the symptomatic or recovery periods (all p≥0.5474).
Wrist skin temperature
Over and above participant level variance, WST increased by 0.13°C (SE=0.04; p=0.001), 0.18°C (SE=0.05; p=0.001) and 0.3°C (SE=0.05; p<0.0001) during the incubation, presymptomatic and symptomatic periods, respectively, compared with baseline ( = 35.3°C, SE=0.06; p<0.0001). WST remained elevated by 0.2°C relative to baseline, even during the recovery period (SE=0.03; p<0.0001).
= 35.3°C, SE=0.06; p<0.0001). WST remained elevated by 0.2°C relative to baseline, even during the recovery period (SE=0.03; p<0.0001).
Skin perfusion
No changes in skin perfusion were observed when comparing measurements during infection (all p≥339) with baseline values ( = −0.01, SE=0.0; p<0001).
= −0.01, SE=0.0; p<0001).
Model specification and algorithm performance
The best-performing RNN consisted of composite features derived from the maximum nightly WST and median nightly RR, averaged across the preceding three-night window. Other parameters were excluded. Table 4 summarises the model performance metrics for the training and testing samples. Class 1 represented an 8-day long training instance extracted from day 10 to day 2 before SO. Class 0 represented a training instance extracted from all other 8-day long consecutive measurements. The training set consisted of 40 days of measurements from 66 participants with a 70:30 train-test split. Sensitivity is reflected in the recall of class 1, whereas specificity is determined by the recall of Class 0. Training the algorithm to detect COVID-19 1 day before SO did not improve recall (data not shown).
Performance metrics of the algorithm in the detection of COVID-19 2 days prior to symptom onset class 1 represented an 8-day long training instance extracted from day 10 to day 2 before SO
In the test set, the algorithm detected 68% of COVID-19 cases 2 days prior to SO.
Discussion
Our main objective was to assess the use of existing medical-grade technology in the early detection of changes in physiological parameters related to COVID-19, thereby facilitating early isolation and testing of potentially affected individuals to limit the spread of the SARS-CoV-2 virus. Our RNN algorithm, trained and tested using a 70:30 split, identified 68% of COVID-19 cases up to 2 days before SO in 66 participants with an accurate false-positive rate and laboratory-confirmed cases of SARS-CoV-2. Therefore, we demonstrated that a wearable sensor bracelet implemented alongside a machine-learning model has the potential to detect COVID-19 infections prior to SO.
Our research is one of the first prospective cohort studies using wearable sensor technology to gather real-time continuous physiological data on which a machine-learning algorithm for COVID-19 presymptomatic detection was trained. Previous studies have evaluated the use of different wearable devices and machine learning to identify COVID-19 infections based on self-reported COVID-19 infections.7 8 25–31 Mishra et al,9 for example, evaluated the use of resting HR data from 32 infected Fitbit users to detect COVID-19 cases in real time and identified 62.5% of the cases before SO. Similarly, Miller et al 32 used RR, HR and HRV data from 271 WHOOP strap wearers to identify 20% of participants who developed COVID-19 before SO and 80% by day 3 after SO.
Only laboratory-confirmed SARS-CoV-2 infections were used in this study to ensure more conclusive results. Our RNN algorithm detected 68% of laboratory-confirmed cases before SO, with additional statistical analyses revealing significant changes in the HR, HRV and WST, across the disease trajectory. Furthermore, our algorithm included more concurrent physiological parameters than previous studies, such as nightly RR, WST and cardiac data.7 9 31–35 Unlike previous studies that performed retrospective measurements, our system could detect infections before SO. Uniquely, our research repurposed a previously existing CE-marked medical device for a novel purpose, illustrating a relatively inexpensive technique for detecting presymptomatic COVID-19. This machine-learning algorithm can be applied to any sensor device that measures the same physiological parameters.
Our findings suggest that a wearable-informed machinelearning algorithm may serve as a promising tool for presymptomatic or asymptomatic detection of COVID-19. However, RT-PCR testing remains the most effective method to confirm COVID-19 infections. A systematic review of wearable sensors in detecting COVID-19 reported these investigations as promising but also highlighted the need for investigations in broader populations.36 Based on this interim analysis, a 20 000-person randomised controlled trial is underway to test the real-time efficacy of the RNN algorithm which can act on real-time machine-learning-driven alerts about the likelihood of a COVID-19 infection before symptoms are reported.13 The initial results from this larger trial are expected in December 2022, with a wider validation and more practical implications of the first presented data approach. In addition, detecting other illnesses using wearable-informed machine-learning algorithm is promising.28 30
The strengths of our study include its population-based design and recruitment from a well-defined and well-characterised healthy cohort. A small subsample of COVID-19 positive users with sufficient high-quality data (wearing the Ava-bracelet ≥28 days prior to SO), reliance on data from a single national centre and lack of ethnic diversity may limit the generalisability of our findings. Additionally, we could not exclude imprecision or misclassification errors related to the symptoms experienced, dates of SO and/or SE. We acknowledge that our sensitivity was less than 80%. We expect to improve the algorithm‘s performance further in a larger cohort within the setting of the COVID-RED study (n=20000). Furthermore, our investigation was based on data from individuals younger than 51 years who typically show less severe symptoms. The algorithm could perform better in older people with more severe clinical manifestations. This question will also be addressed within the framework of the COVID-RED study.13 Finally, one could argue that about half of the individuals identified as positive by the bracelet did not show SARS-CoV-2 infection in subsequent laboratory testing, and an unnecessary testing burden could arise from this fact. The positivity rates of PCR testing (ie, approximately 15%, depending on disease prevalence)37 38 in symptomatic outpatients routinely tested during the pandemic which were considerably lower than the 50% observed in asymptomatic Ava-bracelet users. Hence, the Ava-bracelet could be regarded as progress when compared with the current testing routine.
Overall, the COVI-GAPP study showed that presymptomatic detection of COVID-19-related changes in physiological parameters using a sensor bracelet is feasible. We found significant changes in HR, HRV and WST occurring in COVID-19 positive patients during the presymptomatic period compared with baseline measurements, over and above the effects of intrapersonal variability. A novel machine-learning algorithm detected 68% of laboratory-confirmed SARS-CoV-2 infections 2 days before SO. Wearable sensor technology is an easy-to-use, low-cost method for enabling individuals to track their health and well-being during a pandemic. Our research shows how these devices, partnered with artificial intelligence, can push the boundaries of personalised medicine and detect illnesses prior to SO, potentially reducing virus transmission in communities. Future research should focus on how medical-grade wearable sensor technology can aid in combatting the current pandemic by monitoring sensor data.
Data availability statement
Data are available on reasonable request. Anonymised data that underlie the results reported in this article are available on justified request to the corresponding author.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by KEK, Zurich, Switzerland (BASEC 2020-00786).
Acknowledgments
We thank the GAPP participants who enrolled in this study. Additionally, the authors thank the following for their contributions to the study: The local study team in Vaduz, FL, the different teams at the Dr Risch Medical Laboratories in Vaduz and Buchs, CH. We would also like to thank the Coobx AG in Balzers, FL, for the provision of 3D printed bracelet extensions for persons with large wrists. Addressing data protection issues, we acknowledge the substantial collaborative support of the Elleta AG as well as the national data protection agency in Liechtenstein. We thank the government of the Principality of Liechtenstein, the health ministers, and the Liechtenstein Office of Public Health for their support. Finally, special thanks are due to the Princely House of Liechtenstein, which gave decisive support that enabled the initiation of this project.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
MR, KG, DEG, MC, DC, BMG and LR are joint first authors.
MR, KG, DEG, MC, DC, BMG and LR contributed equally.
Collaborators COVID-19 remote early detection (COVID-RED) consortium:Maureen Cronin; maureen.cronin@avawomen.com; Ava AG, Gutstrasse 73, 8055 Zürich, SwitzerlandBrianna Goodale; brianna.goodale@avawomen.com; Ava AG, Gutstrasse 73, 8055 Zürich, SwitzerlandVladimir Kovacevic; vladimir.kovacevic@avawomen.com; Ava AG, Gutstrasse 73, 8055 Zürich, SwitzerlandKirsten Grossmann; Kirsten.Grossmann@risch.ch; Dr Risch Medical Laboratory, Wuhrstrasse 14, 9490 Vaduz, Liechtenstein; Faculty of Medical Sciences, Private University in the Principality of Liechtenstein, Dorfstrasse 24, 9495 Triesen, LiechtensteinLorenz Risch; lorenz.risch@risch.ch; Dr Risch Medical Laboratory, Wuhrstrasse 14, 9490 Vaduz, Liechtenstein; Dr Risch Medical Laboratory, Lagerstrasse 30, 9470 Buchs, Switzerland;Center of Laboratory Medicine, University Institute of Clinical Chemistry, University of Bern, Inselspital, 3010 Bern, SwitzerlandMartin Risch; martin.risch@ksgr.ch; Central Laboratory, Kantonsspital Graubünden, Loësstrasse 170, 7000 Chur, Switzerland; Dr Risch Medical Laboratory, Wuhrstrasse 14, 9490 Vaduz, Liechtenstein; Dr Risch Medical Laboratory, Lagerstrasse 30, 9470 Buchs, SwitzerlandOrnella Weideli; Ornella.Weideli@risch.ch; Dr Risch Medical Laboratory, Wuhrstrasse 14, 9490 Vaduz, LiechtensteinStefanie Aeschbacher; Stefanie.Aeschbacher@usb.ch; Cardiovascular Research Institute Basel (CRIB), University Hospital Basel, University of Basel, Spitalstrasse 2, 4056 Basel, SwitzerlandDavid Conen; David.Conen@phri.ca; Population Health Research Institute, McMaster University, 237 Barton Street East, Hamilton, ON L8L 2X2, CanadaRegien Stokman; regien.stokman@juliusclinical.com; Julius Clinical, Broederplein 41-43, 3703 CD Zeist, The NetherlandsBilly Franks; billy.franks@juliusclinical.com; Julius Clinical, Broederplein 41-43, 3703 CD Zeist, The NetherlandsHans Van Dijk; hans.vandijk@juliusclinical.com; Julius Clinical, Broederplein 41-43, 3703 CD Zeist, The NetherlandsPaul Klaver; paul.klaver@juliusclinical.com; Julius Clinical, Broederplein 41-43, 3703 CD Zeist, The NetherlandsEric Houtman; eric.houtman@juliusclinical.com; Julius Clinical, Broederplein 41-43, 3703 CD Zeist, The NetherlandsJon Bouwman; jon.bouwman@juliusclinical.com; Julius Clinical, Broederplein 41-43, 3703 CD Zeist, The NetherlandsKay Hage; kay.hage@juliusclinical.com; Julius Clinical, Broederplein 41-43, 3703 CD Zeist, The NetherlandsLotte Smets; lotte.smets@juliusclinical.com; Julius Clinical, Broederplein 41-43, 3703 CD Zeist, The NetherlandsMarcel van Willigen; marcel.vanwilligen@juliusclinical.com; Julius Clinical, Broederplein 41-43, 3703 CD Zeist, The NetherlandsMaui Chodura; maui.chodura@juliusclinical.com; Julius Clinical, Broederplein 41-43, 3703 CD Zeist, The NetherlandsNiki de Vink; niki.devink@juliusclinical.com; Julius Clinical, Broederplein 41-43, 3703 CD Zeist, The NetherlandsTessa Heikamp; tessa.heikamp@juliusclinical.com; Julius Clinical, Broederplein 41-43, 3703 CD Zeist, The NetherlandsTimo Brakenhoff; timo.brakenhoff@juliusclinical.com; Julius Clinical, Broederplein 41-43, 3703 CD Zeist, The NetherlandsTitia Leurink; titia.leurink@juliusclinical.com; Julius Clinical, Broederplein 41-43, 3703 CD Zeist, The NetherlandsWendy van Scherpenzeel; wendy.vanscherpenzeel@juliusclinical.com; Julius Clinical, Broederplein 41-43, 3703 CD Zeist, The NetherlandsWout Aarts; wout.aarts@juliusclinical.com; Julius Clinical, Broederplein 41-43, 3703 CD Zeist, The NetherlandsSantiago Montes; santiago.montes@roche.com; Roche Diagnostics Nederland B.V., Transistorstraat 41, 1322 CK Almere, The NetherlandsAlison Kuchta; alison.kuchta@roche.com; Roche Diagnostics Nederland B.V., Transistorstraat 41, 1322 CK Almere, The NetherlandsChristian Simon; christian.simon.cs1@roche.com; Roche Diagnostics Nederland B.V., Transistorstraat 41, 1322 CK Almere, The NetherlandsLea Berkhout l.berkhout@sanquin.nl; Sanquin Research, PO Box 9190, 1006 AD Amsterdam, The NetherlandsTheo Rispens; T.Rispens@sanquin.nl; Sanquin Research, PO Box 9190, 1006 AD Amsterdam, The NetherlandsAntonella Chiucchiuini; antonella.chiucchiuini@takeda.com; Takeda Pharmaceuticals, Digital Clinical Devices, Cambridge, Massachusetts, USAAriel Dowling; ariel.dowling@takeda.com; Takeda Pharmaceuticals, Digital Clinical Devices, Cambridge, Massachusetts, USASteve Emby; steve@marloweconsulting.com; Takeda Pharmaceuticals, Digital Clinical Devices, Cambridge, Massachusetts, USAAnnemarijn Douwes; a.r.degroot-11@umcutrecht.nl; UMC Utrecht, Heidelberglaan 100, 3584 CX Utrecht, The NetherlandsGeorge Downward; g.s.downward@umcutrecht.nl; UMC Utrecht, Heidelberglaan 100, 3584 CX Utrecht, The Netherlands; Julius Global Health, the Julius Center for Health Sciences and Primary Care, University Medical Center, Universiteitsweg 100, 3584 CG Utrecht, The NetherlandsNathalie Vigot; n.c.s.vigot@umcutrecht.nl; UMC Utrecht, Heidelberglaan 100, 3584 CX Utrecht, The NetherlandsPieter Stolk; p.stolk@umcutrecht.nl; UMC Utrecht, Heidelberglaan 100, 3584 CX Utrecht, The NetherlandsDiederick Grobbee; d.e.grobbee@umcutrecht.nl; UMC Utrecht, Heidelberglaan 100, 3584 CX Utrecht, The Netherlands; Julius Global Health, the Julius Center for Health Sciences and Primary Care, University Medical Center, Universiteitsweg 100, 3584 CG Utrecht, The NetherlandsDuco Veen; d.veen-5@umcutrecht.nl; UMC Utrecht, Heidelberglaan 100, 3584 CX Utrecht, The NetherlandsHans Reitsma; j.b.reitsma-2@umcutrecht.nl; UMC Utrecht, Heidelberglaan 100, 3584 CX Utrecht, The NetherlandsJanneke Wijgert, van de; j.h.h.vandewijgert@umcutrecht.nl; UMC Utrecht, Heidelberglaan 100, 3584 CX Utrecht, The NetherlandsMarianna Mitratza; m.mitratza@umcutrecht.nl; UMC Utrecht, Heidelberglaan 100, 3584 CX Utrecht, The Netherlands; Julius Global Health, the Julius Center for Health Sciences and Primary Care, University Medical Center, Universiteitsweg 100, 3584 CG Utrecht, The NetherlandsPatricia Bruijning; p.bruijning@umcutrecht.nl; UMC Utrecht, Heidelberglaan 100, 3584 CX Utrecht, The NetherlandsCharisma Hehakaya; c.hehakaya@umcutrecht.nl; UMC Utrecht, Heidelberglaan 100, 3584 CX Utrecht, The NetherlandsDaniel Oberski; d.l.oberski@uu.nl; UMC Utrecht, Heidelberglaan 100, 3584 CX Utrecht, The NetherlandsAmos Folarin; amos.folarin@kcl.ac.uk; National Institute for Health Research Maudsley Biomedical Research Centre, King’s College London, London, UKInstitute of Health Informatics, University College London, London, UKRichard Dobson; r.dobson@ucl.ac.uk; Institute of Health Informatics, University College London, London, UKSpiros Denaxas; s.denaxas@ucl.ac.uk; Institute of Health Informatics, University College London, London, UKPablo Fernandez Medina; p.medina@ucl.ac.uk; Institute of Health Informatics, University College London, London, UKEskild Fredslund; esfr@vive.dk; VIVE - The Danish Center for Social Science Research, Aarhus, DenmarkJakob Kjellberg; jakj@vive.dk; VIVE - The Danish Center for Social Science Research, Copenhagen, Denmark.
Contributors All authors critically reviewed and approved the final version of this manuscript and had final responsibility for the decision to submit for publication. Conceptualisation: MRi, HR, RT, PK, TBB, BF, MM, GSD, AD, SM, MC, DEG, DC and BMG, LR; Data curation: KG, SA, MRi and BMG; Formal analysis: MRo, KG, MRo, DL, VK and BMG; Funding acquisition: MRo, MC, DEG, DC and LR; Investigation: KG, SA, OCW and MM; Methodology: MRi, PK, TBB, BF, GSD, SM, MC, DEG, DC, BMG and LR; Project administration: KG, OCW, SM, MC and DEG; Re-sources: MRo, KG, SA, OCW, MK, NW, CR, DH and TL; Supervision: MRi, SA, HR, RT, MC, DEG, DC, BMG, LR; Validation: KG, NW, CR, DH, MRi, VK and DL; Visualisation: KG and FP; Writing—original draft: MRo, KG, FP, MC, DC, BMG, LR; writing—review and editing: MRi, KG, SA, OCW, MK, FP, NW, CR, DH, TL, HR, RT, MRi, VK, AM, DL, PK, TBB, BF, MM, GSD, AD, SM, MC, DEG, DC, BMG and LR. All authors read and agreed to the publisher version of the manuscript. LR is acting as guarantor.
Funding The COVI-GAPP study received grants from the Innovative Medicines Initiative (IMI grant agreement number 101005177), the Princely House of Liechtenstein, the government of the Principality of Liechtenstein, and the Hanela Foundation in Aarau (Switzerland). None of the funders played a role in the study design, data collection, data analysis, data interpretation, writing of the report, or decision to publish.
Competing interests LR, and MR are key shareholders of the Dr Risch Medical Laboratory. DC has received consulting fees from Roche Diagnostics, outside of the current work. MR, DL, VK, AM, MC, and BMG are employed by Ava AG. The other authors have no financial or personal conflicts of interest to declare.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.