Article Text

Abstract
Objective This review aimed to investigate the effects of the maternal and child health (MCH) handbook and other home-based records on mothers’ non-health outcomes.
Design Systematic review.
Data sources PubMed, Web of Science, CINAHL, Academic Search Complete, PsycArticles, PsycINFO, SocINDEX, CENTRAL, NHS EED, HTA, DARE, Ichuushi and J-STAGE through 26 March 2022.
Eligibility criteria for selecting studies Original research articles examining home-based records and mothers’ non-health outcomes published in English or Japanese across various study designs.
Data extraction and synthesis Two independent reviewers extracted relevant data and assessed the risk of bias. We assessed the certainty of evidence for each study using the Grading of Recommendations Assessment, Development, and Evaluation approach. Due to the heterogeneity of the included studies, we conducted a narrative synthesis of their findings.
Results Of the 4199 articles identified, we included 47 articles (20 in Japanese) in the review. Among the different types of home-based records, only the MCH handbook provided essential information about the mother–child relationship, and its use facilitated the mother–child bonding process. Mothers reported generally feeling satisfied with the use of home-based records; although their satisfaction with health services was influenced by healthcare providers’ level of commitment to using these records. While home-based records positively affected communication within the household, we observed mixed effects on communication between mothers/caregivers and healthcare providers. Barriers to effective communication included a lack of satisfactory explanations regarding the use of home-based records and personalised guidance from healthcare providers. These records were also inconsistently used across different health facilities and professionals.
Conclusions The MCH handbook fostered the mother–child bond. Mothers were generally satisfied with the use of home-based records, but their engagement depended on how these records were communicated and used by healthcare providers. Additional measures are necessary to ensure the implementation and effective use of home-based records.
PROSPERO registration number CRD42020166545.
- PUBLIC HEALTH
- SOCIAL MEDICINE
- Community child health
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This systematic review examined a relatively large number of studies that were published in English or Japanese and encompassed several study designs, to highlight the effects of the MCH handbook and other home-based records on mothers’ non-health outcomes.
Unlike past reviews, this systematic review focuses on non-health outcomes as a measure of the effectiveness of these records.
The majority of the studies were observational and qualitative, which leads to potential biases and low certainty of evidence.
Due to marked heterogeneity across studies regarding the study designs, intervention types and comparator groups, a narrative synthesis was conducted.
Introduction
Over 163 countries worldwide have made use of home-based records to improve maternal, newborn and child health (MNCH).1 Home-based records are handheld records used by mothers or caregivers in households to record essential information related to MNCH, including visits to a healthcare provider, vaccination history and the child’s developmental milestones.1 The design and content of these records vary considerably across countries and regions. While their use is nearly universal in some countries, it tends to be limited in others.1 The records are available in paper or electronic format, complement facility-based records, and can be either single focus or multifocus. Single-focus records contain information relevant to one health topic or population group (eg, antenatal care notes, vaccination-only cards, growth charts), while multi-focus records consist of chronologically ordered information pertaining to more than one health topic and can be used for an extended period.2 The difference in focus as per health topic or population group resorted to policy debates on whether home-based records should be developed and distributed per mother or child.3 Due to problems encountered in full integration (eg, poor coordination across stakeholders), most countries prefer to implement program-specific, stand-alone home-based records for MCH services.3
The Maternal and Child Health (MCH) handbook is an example of multifocus records. Its use originated in Japan in 1948 and it is known to be the first integrated home-based record covering the entire spectrum of pregnancy, childbirth, infancy and childcare until 6 years of age.4 The integration may have facilitated the continuum of care5 and might help achieve the Sustainable Development Goal (SDG) 3—ensuring healthy lives and promoting well-being for all at all ages.6 As part of universal healthcare, this handbook is distributed to pregnant women in Japan when they register their pregnancy.7 This record is shared between mothers and healthcare providers and contains educational messages related to MNCH. Mothers bring it when receiving MNCH services and healthcare providers complete the medical charts in the handbook.8 Following decentralisation in 1991, Japanese municipalities started distributing the handbook and may add more information from the 48-page national version to meet their local needs and socioeconomic changes.4 8 It has been theorised to contribute to Japan’s decreased infant mortality, which may have encouraged several countries to adopt the handbook.7 To date, more than 50 countries worldwide have used the MCH handbook and found it to be useful.4 This is especially true for countries where access to healthcare services is restricted.9
Previous systematic reviews have evaluated the impact of home-based records on MNCH and reported improvements in the uptake of antenatal care services, childhood vaccinations and newborn and childcare practices.5 10 11 Studies in Myanmar and Palestine also showed a positive association between using the MCH handbook and receiving high-quality maternal health services.8 12 These are considered essential indicators for evaluating the effectiveness of home-based records for MNCH. However, these reviews have failed to offer any insights related to non-health outcomes, such as communication within the household, communication between mothers/caregivers and healthcare providers, mother–child bonding, and satisfaction with health services and home-based records.1 This is despite the WHO’s (WHO) recommendation regarding the use of non-health outcomes for evaluating the effectiveness of home-based records for MNCH.1 For example, a systematic review by Magwood et al suggested that home-based records could empower women and children and act as a point of commonality between patients and healthcare providers.13 While they presented compelling results, they did not find any evidence pertaining to mother–child bonding and there was a lack of in-depth discussion about communication and satisfaction with these records. Exploring these non-health outcomes can be crucial for providing a more holistic picture of the effectiveness of home-based records and result in insights of theoretical and practical relevance.14–17 This would capture the user experience to help improve the implementation of home-based records. Moreover, non-health outcomes may impact health outcomes,14 although more studies need to be conducted to clarify this effect.
The review mentioned above by Magwood et al included only qualitative studies available in English, without taking into consideration essential findings resulting from quantitative studies. The lack of data saturation or richness is a limitation of qualitative studies and will affect the certainty of evidence.18 Quantitative studies may bring evidence on real-life outcomes of records as they provide more information on actual adherence. Furthermore, given that Japan developed and popularised the use of the MCH handbook, the inclusion of studies published in Japanese can lead to an enhanced understanding of how users perceive home-based records.
In light of these gaps left unaddressed by existing literature, this study aimed to investigate the effects of the MCH handbook and other home-based records on mothers’ non-health outcomes, through a review of studies published in English and Japanese. This systematic review was conducted as part of a larger systematic review aimed at exploring the roles of the MCH handbook and other home-based records on MNCH.
Methods
Patient and public involvement statement
Patients and/or the public were not involved in this review.
The protocol was (online supplemental file 1) conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) reporting guidelines.19
Supplemental material
Selection criteria
Study inclusion criteria
This review included research studies published in English or Japanese and conducted using various study designs, such as randomised controlled trials (RCTs), observational studies (quasi-experimental, cohort and cross-sectional), case studies and qualitative studies. We excluded books, conference abstracts, editorials, letters, protocols and systematic reviews. We defined the inclusion criteria based on the Population, Intervention, Comparator, Outcome framework.
Participants
We included studies conducted with parents, including mothers or other caregivers of newborns and children. Both health and community settings were considered in this review.
Intervention
The intervention consisted of home-based records managed or kept by mothers or caregivers in the form of hard copies. These records included women-held maternity records, child health books, vaccination-only cards and integrated MCH books (ie, the MCH handbook). We excluded patient diaries, mobile health interventions (apps, text messages) and provider-held records, such as electronic medical records and web-based summaries of patients’ appointments.
Comparison
The comparator included standard care provided to mothers or caregivers before or after childbirth, conventional information or the absence of any home-based records. We also included studies that did not include a comparison group.
Outcome
We followed the WHO guidelines for defining non-health outcomes.1 These included communication within the household, communication with healthcare providers, satisfaction with home-based records and satisfaction with services/provider performance.1 Communication within the household refers to how home-based records improved partner/family members’ involvement in pregnancy and childcare, while communication with healthcare providers covers counselling sessions using the records and mothers’ engagement. Satisfaction with home-based records refers to mothers’ perceived agreement with its content (eg, health or recording information). In contrast, satisfaction with services/provider performance refers to mothers' perceived use of the records to deliver MCH services. As an additional outcome, we included mother–child bonding based on the assumption that the integration of the mother’s and child’s records in the MCH handbook can foster a stronger mother–child bond. We defined ‘mother–child bonding’ as the development of a core relationship between mother and child.20 This bond is unidirectional (from mother to child), shapes during pregnancy and continues developing until early childhood.21–23
Search strategy
Two authors (RRC and JLS) developed a search strategy using Medical Subject Headings terms and keywords (online supplemental file 2), without restrictions on date. Electronic databases were searched for articles published in English and Japanese until 26 March 2022. For articles published in English, RRC and JLS searched the following databases: MEDLINE, CINAHL, Web of Science, PsycArticles, PsycINFO, SocINDEX, Academic Search Complete, Cochrane Central Register of Controlled Trials, NHS Economic Evaluation Database, Health Technology Assessment database and the Database of Abstracts of Reviews of Effects.
Supplemental material
A different set of authors (JLS and MKK) searched Japanese databases, including Igakuchuo-zasshi (Ichushi; https://search.jamas.or.jp/) and J-STAGE (https://www.jstage.jst.go.jp/), to search for articles published until March 26, 2022. Both these databases publish over 300 000 articles annually from 2500 Japanese biomedical journals.
Furthermore, three authors (RRC, JLS and MKK) searched grey literature using the WHO databases, United Nations Children’s Fund, the European Centre for Disease Prevention and Control, the US Center for Disease Control and Prevention and the Japan International Cooperation Agency. The authors also manually searched the reference lists of articles, whose full texts had been retrieved, to identify additional relevant articles. All records identified through the search were uploaded to a reference-managing software package (Endnote V.X9) to facilitate the identification and selection of articles eligible for inclusion in this review.
Evidence retrieval
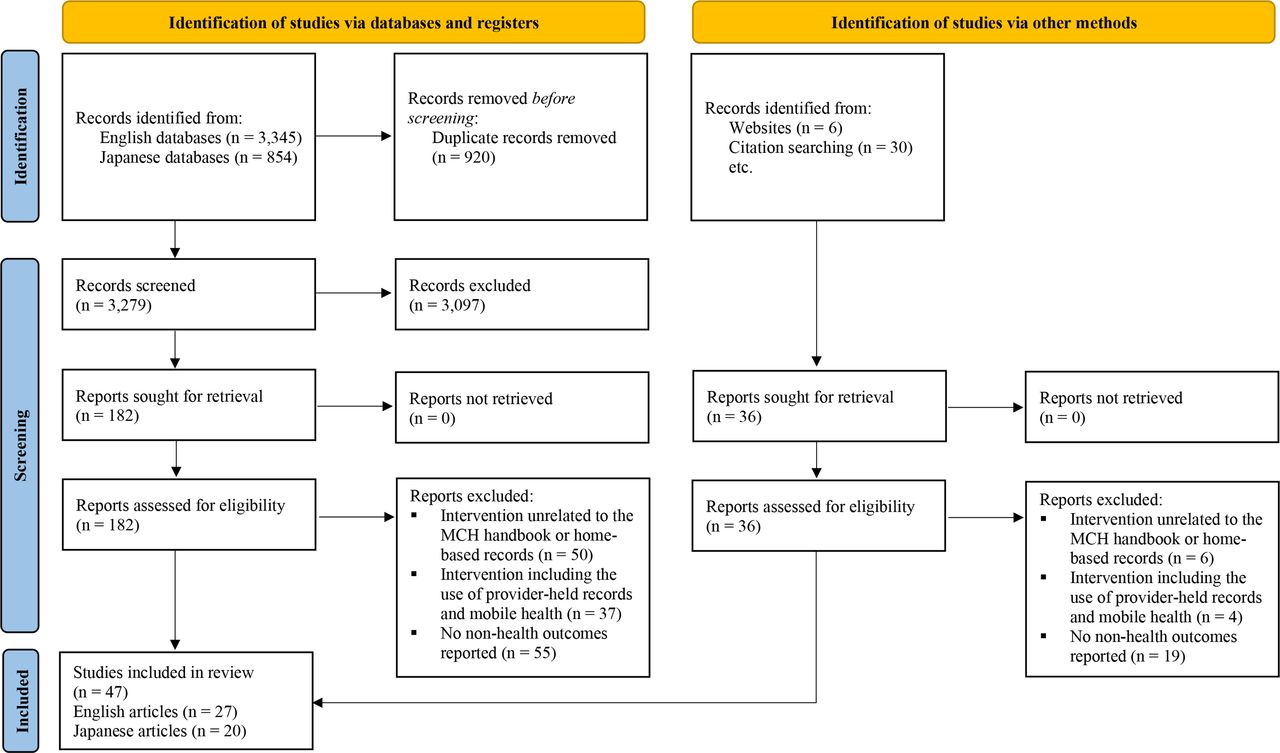
The search strategy yielded 4199 articles from both English and Japanese databases; additionally, 36 articles were identified through manual searching. Of these, 854 were articles published in Japanese. After removing duplicate entries, a total of 3315 articles remained. Subsequently, RRC and JLS assessed the English articles to determine their eligibility, while MKK and JLS assessed the Japanese articles. This was done by screening the titles and abstracts of the studies in a blinded, standardised manner. Any disagreements were resolved through discussion among the three authors until a consensus was reached or by consulting a fourth author (MJ or AS). A total of 3097 articles were excluded following the initial screening.
In the next stage of screening, the three authors obtained the full texts of the remaining 218 articles from the University of Tokyo Library System, National Diet Library Online and Keio University KOSMOS System. Consequently, 171 articles were excluded for the following reasons (online supplemental file 3): intervention unrelated to the use of home-based records (n=56), intervention involving provider-held records and mobile health (n=41) and outcomes not pertaining to communication, satisfaction and mother–child bonding (n=74). Finally, 47 articles (including 20 Japanese articles) were deemed eligible for inclusion in the narrative synthesis. Figure 1 shows the PRISMA flow diagram of the screening process.
Supplemental material
{kind=link}
PRISMA flow diagram of the screening process. MCH, maternal and child health; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Data extraction
The three authors (RRC, JLS and MKK) created a library using the Endnote referencing software consisting of PDF versions of the included articles. We extracted and independently entered the following data in a Microsoft Excel sheet: citations (ie, name of the first author, publication year, title, and journal name), study design, country and settings, population and sample size, type of home-based records used, comparator and relevant outcomes (online supplemental file 4). The same authors discussed the strategies and presentation of the results throughout the data extraction process.
Supplemental material
Quality appraisal
The authors (MKK and JLS for Japanese articles; RRC and JLS for English articles) independently assessed the risk of bias in the included studies. For RCTs, we used the revised Cochrane Risk of Bias Tool (RoB 2) to evaluate the overall risk of bias based on five domains: randomisation process, deviations from the intended intervention, missing outcome data, outcome measurement and selective reporting of results.24
For non-RCTs, we used the following risk of bias assessment tools: Risk Of Bias in Non-randomized Studies - of Interventions for non-randomised studies,25 Critical Appraisal Skills Programme checklist for qualitative studies,26 National Institutes of Health quality assessment tool for observational cohort and cross-sectional studies,27 and the mixed-methods appraisal tool for mixed-method studies.28 Disagreements were discussed and resolved through a consensus between the authors. Additionally, we used the Grading of Recommendations Assessment, Development and Evaluation (GRADE) framework to assess the certainty of the evidence in quantitative studies,29 and the GRADE-CERQual (confidence in the evidence from reviews of qualitative research) framework for qualitative studies.30
Synthesis of findings
All the authors participated in the data analysis. We conducted a narrative synthesis owing to the heterogeneity of study designs among the included studies and the lack of pooled data for a meta-analysis. Therefore, we followed the synthesis without meta-analysis reporting guidelines (online supplemental file 5) for the narrative synthesis of findings,31 instead of the PRISMA guidelines (online supplemental file 6). To evaluate the effects of the intervention (home-based records), we conducted a detailed examination of the numeric and textual summary of the findings and conclusions of the included studies. We coded the outcomes as having a positive, mixed or no effect. We considered an outcome to have a ‘positive effect’ if the home-based record showed a statistically significant effect (eg, women experienced more partner involvement) and narrative findings indicated positive results (eg, healthcare providers explained what is being recorded). We coded an outcome to have a ‘mixed effect’ when it showed some evidence of the usefulness of the record but not necessarily a significant effect. When there was no significant effect and narrative findings reported negative results (eg, perceived lack of communication with healthcare providers), we considered the outcome as ‘no effect.’ We grouped the studies for synthesis based on the following research questions:
Supplemental material
Supplemental material
Do home-based records (intervention) improve communication, satisfaction and mother–child bonding, as opposed to the non-use of home-based records (control)?
Does a different type of home-based record (intervention) improve communication, satisfaction and mother–child bonding, compared with a standard home-based record (control)?
We presented the direction and magnitude of the effect (effect sizes that cannot be meta-analysed) in the GRADE table (online supplemental file 7). We also presented the qualitative evidence profile in the GRADE-CERQual table (online supplemental file 8). We ordered the heterogeneity of the included studies according to the participants, methods and outcomes reported. We prioritised studies based on their study design, risk of bias assessment and relevance to the research question.
Supplemental material
Supplemental material
Results
Study characteristics
Online supplemental file 4 presents a summary of study characteristics.
Study designs
Among the included studies, there were 4 RCTs, 4 quasi-experimental studies (open, non-randomised trials), 6 cohort studies, 17 cross-sectional studies, 3 mixed-method studies (pre–post intervention and qualitative evidence), 9 qualitative studies and 4 case studies.
Location
We used the World Bank definition to categorise countries according to income levels.32 Thirty-three studies were conducted in high-income countries (HICs): Japan (n=18), the UK (n=7), Australia (n=4), the USA (n=2), New Zealand (n=1) and Norway (n=1). Fourteen studies were conducted in low-income and middle-income countries (LMICs): two studies in South Africa, one each in Ethiopia, Palestine, Iran, Bosnia and Herzegovina, Thailand, Indonesia, Vietnam, Bangladesh, Mongolia, Brazil, and Dominican Republic, and one multicountry study.
Study participants
We noted differences in the inclusion criteria for the study participants. Across studies, mothers were enrolled at different points in time either during pregnancy, childbirth or postbirth. One multicountry study targeted both literate and illiterate mothers who lived in communities with easy or low access to healthcare services.33 Other studies targeted women from an ethnic minority group,34 women who had experienced miscarriages,35 36 as well as parents of children with special educational needs.37 Studies were primarily conducted in health facilities, although a few were conducted in community settings. The sample sizes also varied greatly (range: 1–250 000) among included studies.
Types of interventions
We identified differences in the type of home-based records used by mothers or caregivers. Among the 47 studies included in the review, 25 involved the use of the MCH handbook. The remaining studies used other types of home-based records, including plunket books, road-to-health (RTH) booklets, maternity case notes, child personal health records, speaking books and patient passports. Some studies did not include a comparison group (n=33) when evaluating the intervention, while others compared users of home-based records with non-users of records or standard care groups. Thus, the studies considered home-based records as a single intervention when reporting their findings. We have presented the findings from the English and Japanese articles separately (tables 1–2).
English articles included in the review
Japanese articles included in the review
Risk of bias in included studies
The risk of bias varied among the included studies. Online supplemental file 9 shows the risk of bias assessment of RCTs, observational studies, qualitative studies and mixed-method studies. Based on the RoB 2 algorithm, the four RCTs showed a high overall risk of bias, mainly because of concerns in the randomisation process and challenges with the blinding/masking of assessors owing to the nature of the intervention. For non-RCTs, we observed methodological issues and a lack of information and adjustment for potential confounding variables.
Supplemental material
Communication within the household
Four studies published in English reported the effects of home-based records on communication within the household (table 1).38–41 Of these, three reported positive effects, but one did not. In Palestine and Indonesia, women who shared the MCH handbook with their husbands experienced greater involvement from their partners during pregnancy, delivery and childcare (GRADE certainty of evidence: very low).38 39 Husbands expressed support by way of saving money for the delivery (OR=1.82, 95% CI 1.20 to 2.76), keeping their babies warm (OR 1.58, 95% CI 1.02 to 2.46), and providing developmental stimulation (OR 1.62, 95% CI 1.06 to 2.48).39 Moreover, pregnant women in Australia found handheld maternity records to be beneficial because they could go through the records at home with their husbands and could share information with their grandparents and friends (GRADE-CERQual certainty of evidence: very low).40 In Palestine, such sharing of information helped reduce misconceptions related to pregnancy and child care among family members.38
Communication between mothers/caregivers and healthcare providers
Nineteen studies reported the effects of home-based records on communication between mothers/caregivers and healthcare providers.33 34 37 38 40–54 Of these, eleven reported positive effects, five showed mixed effects, and three showed no effect. One RCT conducted in the UK reported that women having access to their complete records found it easier to talk to doctors and midwives (RR 1.73, 95% CI 1.16 to 2.59, GRADE certainty of evidence: very low) than the other group comprising cooperation card holders.41 Similarly, few qualitative studies also found home-based records to be an effective tool for communication and relationship building with healthcare providers (GRADE-CERQual certainty of evidence: low).40 42 47 49 51 In Ethiopia, pregnant women and mothers had the opportunity to ask questions related to a child’s development during ‘speaking book’ sessions and received solutions to throat and tooth related problems experienced by infants.49
However, other studies reported mixed or no effects of home-based records on communication with healthcare providers. In a study in the UK, some parents (22%) indicated that they had not been given a satisfactory explanation on how to use the personal child health record (PCHR) when it was issued.46 Additionally, health visitors were more likely to make use of PCHRs than other healthcare providers.46 In South Africa, there were marked differences in the usage of RTH cards between private and public clinics; relatively few mothers in private clinics (31% vs 74% in public clinics) received an explanation regarding the RTH card, and the interpretation of the weight chart tended to be ignored in private clinics (92% vs 42% in public clinics).43 A qualitative study conducted with ethnic minority women in Vietnam suggested healthcare providers’ reliance on written information (MCH handbook) over interpersonal communication.34 The participants further indicated that the health information they received (verbally and in written) was often non-specific and not adjusted for their personal circumstances.34
Satisfaction with the information provided by the home-based records
Nineteen studies reported on mothers’ satisfaction with the information provided by home-based records.33 43–46 49 53 55–66 Among these, 12 reported positive effects, 6 reported mixed effects and 1 showed no effect. One RCT conducted in Norway reported that 65% parents were satisfied with the use of parent-held records and 92% were in favour of making it available permanently.44 Satisfaction and support were particularly high among parents of children with chronic diseases.44 In Japan, observational studies have reported the usefulness of the MCH handbook in providing information regarding the child’s health, growth and vaccination history.61 62 However, one study highlighted the following recommendations made by parents to make the MCH handbook more ‘user-friendly’: an appropriate size, easy-to-understand expressions, and better and more relevant information for parents.64 In a study conducted in Mongolia, an MCH handbook user suggested the handbook should leave space for the doctor to offer some advice, especially for the father (such as showing support and information on tobacco and alcohol use), instead of only providing information.53
Satisfaction with the services/provider performance
Nine studies reported on mothers’ satisfaction with health services received through home-based records.51 67–74 While four studies reported positive effects, five reported mixed effects. In Japan, interest in the MCH handbook was higher at the time of a check-up, as opposed to a consultation, among both healthcare providers and parents.71 For mothers, the pages filled out by healthcare providers were the most useful, such as delivery records, vaccination records and neonatal records.74 The section that was least useful to mothers was the one related to child and maternal oral hygiene.72 In Australia, most parents and the community health staff liked personal health records and used them frequently, while most private doctors did not find them useful.67
Mother–child bonding
Eight studies published in Japanese reported on the positive impact of the MCH handbook on mother–child bonding (GRADE certainty of evidence: very low).35 36 74–79 In Japan, mothers who used the MCH handbook were found to be more likely to pass on the handbook to their children at the time of their marriage or pregnancy.74 75 The handbook offered guidance on some healthy behaviours (eg, self-care, disease management) that could be passed on to future generations,75 and could also predict the course of pregnancy and delivery for the next generation of daughters.76 For mothers who had experienced neonatal death, the MCH handbook served as an aide-memoire because it had the newborn’s footprint and handprint, as well as words of gratitude for the mother had written at the time of the child’s birth.35 36 For mothers who had experienced a natural disaster (eg, earthquake, tsunami), losing their MCH handbook, and hence, all pregnancy and child health records, was painful.77 Nurses also introduced the MCH handbook to reduce adoptive parents’ anxiety and foster good parent–child relationships.78 Furthermore, children of mothers who wrote at least one record of being worried or anxious in the MCH handbook, were more likely to develop maladaptive behaviour at school compared with children of mothers who wrote nothing or did not receive the handbook (p<0.05).79
Discussion
This systematic review provided evidence of the effects of the MCH handbook and other home-based records on mothers’ non-health outcomes. We found positive effects of these records on communication within the household and on mother–child bonding, but mixed effects on mothers’/caregivers’ communication with healthcare providers. Mothers were generally satisfied with the content of the record, but they suggested making it more user-friendly. Their satisfaction with healthcare services, following the use of these records, was associated with providers’ commitment to use or refer to records during check-ups and consultations. However, we noted inconsistency in the use of home-based records across health facilities and professionals.
Of the different types of home-based records, only the MCH handbook may have fostered mother–child bonding. This finding is new and is only found in Japanese articles. Various ways could explain how the use of the MCH handbook facilitated mother–child bonding. First, the handbook was considered a special gift, filled with parental love and mothers’ messages for their children, given to children during their marriage or pregnancy.74 75 Mothers in Japan wrote down their worries, joy, and expectations from pregnancy and child rearing in the handbook, along with some healthy behaviours that could be passed on to the next generation.75 80 Losing these handbooks to a natural disaster was a painful experience for Japanese mothers, as it meant losing all their pregnancy and child health records.77 Second, the handbook could be used to predict the child’s school adaptation,79 and the possible course of pregnancy and delivery for the daughter.76 That is, school maladaptation was evident among children whose mothers had recorded at least one incident of worry or anxiety in the MCH handbook. This can be attributed to the fact that the emotional bond with the mother is critical for the child’s social, emotional and cognitive development.81–83 Thus, the mother’s worry or anxiety is likely to hinder the development of such a bond, leading to difficulties in adaptation for the child. Third, it served as an aide-memoire for mothers who had experienced neonatal death.35 36 Mothers’ words of gratitude written in the handbook served as evidence of the bonds formed during pregnancy. Finally, the handbook served as a tool to help reduce parental anxiety and build good parent–child relationships, even among adoptive parents.78 Overall, the findings showed that the MCH handbook is an essential source of information to learn more about the mother–child relationship. The bonding formation may be attributed to the integration of MCH records and how mothers in Japan use the handbook.
Mothers were generally satisfied with home-based records and were in favour of making them available permanently. Satisfaction and support were exceptionally high among parents of children with chronic diseases.44 However, several issues were noted regarding the design and content of these records. Accordingly, participants in one study suggested making the MCH handbook more user-friendly by choosing an appropriate size, using easy-to-understand expressions, and including more relevant content for parents.64 In Mongolia, users suggested the inclusion of blank space for doctors’ notes, advice for fathers, and information on tobacco and alcohol use.53 Such feedback from end-users and communities should be incorporated into the design and content of home-based records to ensure that these records align with the local context and individual needs, and are, therefore, more likely to be adopted and used in the long term.
Healthcare providers’ commitment to using home-based records was found to influence mothers’ satisfaction with health services. For Japanese mothers, the information (pertaining to delivery, vaccination, neonatal health, etc) in the handbook filled out by healthcare providers was the most useful.74 Alternately, information related to child and maternal oral hygiene in the handbook was least useful.72 Thus, mothers were more satisfied with health services when they received health information directly from their healthcare providers. Furthermore, in South Africa, mothers were unsure of what to do with the weight-for-age chart, immunisation schedule and milestone section.43 Unused sections may be perceived as being unnecessary and may undermine the value of the entire record. Hence, it is crucial that both mothers and healthcare providers be encouraged to fully use these records.
However, we observed inconsistencies in the use of records across health facilities and professionals, which might discourage mothers from using home-based records. Private clinics and hospitals were less likely to use the records than public and primary care settings.43 46 67 Moreover, doctors (eg, general practitioners, paediatricians) were less likely to use and refer to home-based records than nurses and health visitors during check-ups and consultations.57 67 69 This finding is consistent with that from a previous systematic review.11 Generally, community nurses are the most likely professionals to use/refer to the home-based records in the health facilities.11 Such reluctance from doctors to fill out a home-based record may arise if they are not properly oriented to see the benefits of using these records for themselves and their patients.
Home-based records were regarded as being effective tools for communication and relationship building between mothers/caregivers and healthcare providers.40 42 47 49 51 However, the healthcare provider’s attitude towards home-based records acted as a barrier to communication. While some providers did not provide a satisfactory explanation for using the records when they were issued to mothers,46 others relied primarily on the written information in the MCH handbook and neglected interpersonal communication.34 Furthermore, ethnic minority women in Vietnam reported receiving health information from providers that was non-specific and not relevant to their context.34 For instance, they were not given specific dietary advice and told to eat from all food groups and take iron supplements when they ‘lack blood,’ which is unclear how they would assess this themselves.34 This finding is new and requires special attention. That is, it is imperative that the handbook offers personalised guidance, especially for women with lower education and from minority populations. This can help build trust and strong partnerships between mothers and healthcare providers and reduce barriers for women in accessing healthcare.38 84 85
Lastly, home-based records provided a mechanism to improve communication within the household and clarify pregnancy-related and child care-related misconceptions among family members. For instance, in Palestine and Indonesia, women who shared the MCH handbook with their husbands experienced greater involvement from them during pregnancy, delivery and childcare.38 39 In Australia, home-based records provided opportunities for pregnant women to share their journeys with their husbands, grandparents and friends.40 These findings are consistent with a review conducted by Magwood et al.13 Given that previous studies have identified the influence of mothers-in-law and gender roles as barriers to husbands’ involvement in childcare,86–88 use of home-based records may help overcome these barriers to increase husbands’ involvement.
This systematic review, however, has several limitations. First, we obtained our results primarily from observational and qualitative studies, as only four RCTs were available for this review. The Cochrane Handbook recommends including observational studies if RCTs cannot completely answer the research question.89 While the findings from observational and qualitative studies provide evidence necessary to answer our research question, these findings should be interpreted with caution owing to potential biases and low certainty of evidence according to the GRADE and GRADE-CerQUAL criteria. Second, we could not perform a subgroup analysis to compare HIC and LMIC or a network meta-analysis to compare different types of home-based records due to an insufficient number of studies. Thus, we only summarised the data based on the country where the study was conducted and the types of home-based records used. Third, we observed marked heterogeneity across studies regarding the study designs, intervention types and comparator groups, all of which may have modified the study outcomes. Hence, we conducted a narrative synthesis, and evaluated the risk of bias and certainty of evidence for all included studies.
Despite these limitations, this systematic review had its own strengths in that it examined a relatively large number of studies that were published in English or Japanese and encompassed several study designs, to highlight the effects of home-based records on mothers’ non-health outcomes.
Conclusion
The effectiveness of home-based records can be measured using mothers’ non-health outcomes. Among them, the MCH handbook fostered mother–child bonding. This outcome could be added to the WHO’s recommendations on home-based records for MNCH. Healthcare providers may choose to refer to the mothers’ notes in the MCH handbook to address issues in the bonding process. Mothers were generally satisfied with the use of home-based records, but their engagement depended on how these records were communicated and utilised by healthcare providers. Thus, various types of training must be conducted at the local level across health facilities and for all healthcare professionals to orient them to the use and benefits of home-based records and, therefore, help them provide patient-centred care. Moreover, we should monitor and evaluate the use of the MCH handbook and other home-based records to ensure their effective implementation. Policymakers need to consider the non-health-related value of home-based records and ensure that mothers and their children are not left behind in the era of SDGs.
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information.
Ethics statements
Patient consent for publication
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors Conceptualisation: RRC, JLS, MKK, AS, EY, MB and MJ; data curation: RRC, JLS and MKK; formal analysis: RRC, JLS, MKK and AS; funding acquisition: AS and MJ; investigation: RRC, JLS and MKK; methodology: RRC, JLS, MKK, AS, EY, MB and MJ; project administration: AS and MJ; supervision: MJ; validation: AS, EY, MB and MJ; visualisation: RRC and AS; writing-original draft: RRC; writing-review and editing: RRC, JLS, MKK, AS, EY, MB and MJ; Guarantor: MJ. All authors critically reviewed and approved the manuscript.
Funding This research was funded by the Program of Bilateral Health and Medical Cooperation between Japan and the Russian Federation, Ministry of Health, Labour and Welfare, Japan.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.