Article Text

Abstract
Objective To provide an accurate assessment of the prevalence of breast fibroadenoma in a large population and to confirm the diagnostic accuracy of ultrasound for fibroadenoma.
Design This was a cross-sectional survey.
Setting This research was conducted at Nanfang Hospital, Guangzhou, Guangdong, China.
Participants A total of 11 898 women aged 18–40 years who underwent breast screening between 1 January 2019 and 31 December 2019 were included in the fibroadenoma prevalence study. From 1 June 2019 to 31 December 2019, 342 breast lesions with pathology reports and preoperative ultrasound images were collected for diagnostic fibroadenoma testing (vs histological diagnostic testing).
Primary outcome measures Pearson’s χ2 test was performed to compare the prevalence of different lesions between age groups, and descriptive statistics were used to report the clinical characteristics of fibroadenoma. For ultrasound diagnosis, fibroadenoma was defined as a well-circumscribed lesion with round or oval shape, consisting of a homogeneously hypoechoic or isoechoic solid mass, located parallel to the chest wall with a smooth margin and no posterior shadowing. Diagnostic test results for breast fibroadenoma were stratified by diagnostic type (histological vs ultrasound).
Results Of the women aged 18–40 years, 27.6% (3285/11 898) had an ultrasound diagnosis offibroadenoma. Of these, the prevalence of fibroadenoma was stable across age groups (p=0.14) and did not differ between the left and right sides of the breast. Almost two-thirds of women presented with a single fibroadenoma, and most fibroadenomas did not exceed 1 cm in size. The sensitivity and specificity for fibroadenoma were 97.0% (95% CI for sensitivity: 93.7% to 98.8%) and 91.4% (95% CI for specificity: 85.4% to 95.5%) for ultrasonography, respectively.
Conclusions The prevalence of fibroadenoma in South China is as high as 27.6%, and ultrasound could be used as a tool to diagnose fibroadenoma.
- epidemiology
- ultrasonography
- breast imaging
Data availability statement
Data are available on reasonable request. Data are available on reasonable request by contacting JD.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
Our study had extremely low rates of missing data, and ultrasound data were collected and revised by trained breast sonographers.
The study population was from a single medical centre in Guangzhou city, however, the size and the diversity of the population compensate for this limitation to a great extent.
Some participants in this study might have undergone breast screening owing to having specific symptoms, this might have increased the prevalence of fibroadenoma in the study population.
As the study was performed only on healthy women who underwent physical examination, a large-scale screening study is required to evaluate an asymptomatic population and predict the prevalence of breast fibroadenoma.
The study’s findings might not be generalisable to older age groups and geographical regions outside China.
Introduction
Fibroadenoma is the most common benign breast tumour in women and is characterised by the proliferation of epithelial and stromal components of the terminal ductal unit.1 The underlying pathogenesis of fibroadenoma is unclear but is generally thought to be associated with baseline hormone levels, rates of change in hormone levels, obesity and family history.2 3 Although fibroadenoma is a benign fibroepithelial lesion that does not progress,4 it is still worthy of attention because of its high prevalence and impact on women’s quality of life and mental health. In addition, histologically confirmed fibroadenoma shares many risk factors with breast cancer, suggesting that fibroadenoma may be a risk factor for breast cancer.5
Although a rapid increase in breast cancer incidence in recent decades has been reported, the rate of fibroadenoma has not been determined.6 Most studies have focused on the histopathological characteristics of benign breast disease, and few have assessed the clinical features of fibroadenoma. Fibroadenoma was initially reported to have an incidence of 7%–13%.7 In the 20th century, estimates of fibroadenoma incidence of between 15% and 23% were obtained from small and medium sample size autopsy studies.6 However, to date, there has been no study of fibroadenoma incidence in a representative population in China. It is difficult to estimate the incidence of benign breast disease in the general population, because women who are diagnosed and receive medical care are a select subset. Fibroadenoma is not a life-threatening condition, and thus, it does not necessarily come to medical attention. Improved health consciousness has led to an increase in the number of clinicians performing breast ultrasounds, resulting in an apparent increase in the incidence of fibroadenoma among younger women. This is worthy of further investigation. In addition, a study showed that prevalence may differ between sides, and that peak age depends on racial or ethnic group.8 We conducted a cross-sectional study with a large sample size to assess the prevalence and clinical characteristics of fibroadenoma in a Chinese population.
Fibroadenoma most frequently occurs in women in their 20s and usually presents as a well-defined, mobile, painless mass.9 Fibroadenoma can be diagnosed through clinical breast examination, breast ultrasonography and fine-needle aspirate cytology.5 Most fibroadenomas do not require surgical treatment and can be managed conservatively, only requiring excision if they become large or symptomatic.10 As breast fibroadenoma is a benign tumour, it is not feasible or necessary to perform a biopsy in all patients for diagnosis. Biopsies are clinically challenging and entail unnecessary physical, psychological and financial burdens.9 Therefore, in practice, ultrasonography is commonly used for diagnosis. Several studies have suggested that modern ultrasonography performed by experienced breast radiologists is a reliable technique for diagnosing fibroadenoma.11–13 The sensitivity and specificity of ultrasonography for fibroadenoma were found to be 85.7% (95% CI for sensitivity: 77.9% to 93.5%) and 71.4% (95% CI for specificity, 47.8% to 95.1%), respectively, in a study from South Africa.13 Moreover, a prospective study of 149 subjects from Nigeria reported a sensitivity of 93.3% and a specificity of 58.8%,14 and a German study found a specificity of 88.2% for ultrasound diagnosis of fibroadenoma.11 These findings suggest that ultrasonography can be used to predict the prevalence of fibroadenoma in women in the real world to better guide clinical practice.
In this study, ultrasonography was used to make predictive diagnoses in women who underwent breast screening at the Department of Health Management at Nanfang Hospital in 2019. We predicted the prevalence of fibroadenoma and analysed the characteristics of the fibroadenomas that were diagnosed. In addition, sample size estimates were made for the diagnostic test, and sufficient numbers of patients were assembled. We compared the diagnostic accuracy of ultrasonography for breast fibroadenoma with histology to demonstrate that ultrasound diagnosis is feasible and accurate.
Materials and methods
Study population
This study conformed to the principles embodied in the Declaration of Helsinki. To investigate the prevalence and clinical characteristics of fibroadenoma in a healthy physical population undergoing examination in the Guangdong province of China, 11 898 consecutive women aged 18–40 years who underwent routine breast screening at the Department of Health Management, Nanfang Hospital, from 1 January 2019 to 31 December 2019 were included in the study. Ultrasound images were retrospectively reviewed and analysed independently by two trained breast sonographers. All lesions were reviewed and analysed independently by two trained breast sonographers. Disagreements between the sonographers were resolved by consensus review.
Patient and public involvement
There was no patient or public involvement in the design, conduct, reporting or dissemination of our research.
Diagnostic testing and the standard reference
A total of 329 consecutive female patients (18–40 years) who underwent core needle biopsy or excisional biopsy at the Breast Centre, Nanfang Hospital, from 1 June 2019 to 31 December 2019 were included in the study. Indications for biopsy were the patient preference, clinical concerns or the presence of a suspicious lesion on X-ray mammography or ultrasound. The biopsy procedures were performed by an experienced surgeon team at the Breast Centre, and the lesions were removed as completely as possible. Samples from surgery were observed by two pathology experts via histopathological identification to confirm fibroadenoma of the breast. Pathological reports were retrieved from the hospital database system, and the findings were compared with preoperative ultrasound images analysed independently by two trained breast sonographers. Ten patients were excluded from the study owing to a lack of preoperative ultrasound images at our centre. Finally, 319 patients and 342 histologically confirmed lesions, comprising 203 fibroadenomas and 139 non-fibroadenomas, were retrospectively analysed (a flow chart is shown in online supplemental figure 1).
Supplemental material
Flow chart of the diagnostic process:From 1 June 2019 to 31 December 2019, 342 breast lesions with pathology reports and preoperative ultrasound images were collected for diagnostic fibroadenoma testing (versus histological diagnostic testing)The sample size for the diagnostic test was calculated based on prevalence and testing characteristics defined by the sensitivity and specificity of ultrasonography for the diagnosis of fibroadenoma. Based on previous studies,10 12 ultrasonography was assumed to have a sensitivity of 90% and specificity of 80%. With an estimated prevalence of fibroadenoma of 20%, the sample size needed for this study was calculated using PASS V.15 (NCSS) to achieve a confidence level of 95% and a margin of error of 10%. The estimated minimum sample size was 44 subjects with fibroadenoma and 70 subjects without fibroadenoma.
Ultrasound examination and index test
Breast ultrasound examination is typically performed with the patient in a supine position with the ipsilateral arm raised and a pillow placed under the shoulder. Ample acoustic gel is applied between the transducer and the skin, and the probe is usually moved in a systematic radial fashion toward the nipple, with any identified lesions documented as a position on a clock face and designated by the number of centimetres from the nipple. The imaging study was performed using dedicated breast diagnostic ultrasound equipment (IU-22, Koninklijke Philips N.V., Amsterdam, Netherlands; Aixplorer, Supersonic Imagine SA, Aix-en-Provence, France) with 12.5 MHz linear array transducers. When suspicious breast lesions were found, the ultrasound images were analysed independently by two trained breast sonographers. Classic imaging features of breast fibroadenoma are as follows: (1) well-circumscribed lesions, (2) round or oval shape, (3) homogeneously hypoechoic or isoechoic solid mass, (4) parallel to the chest wall with a smooth margin and (5) no posterior shadowing. In the diagnostic test, results from the ultrasonic analysis were summarised into two categories: fibroadenomas and non-fibroadenomas.
Statistical analysis
The SPSS V.15.0 (SPSS) was used for data analysis. Statistical tests were two sided and used a significance level of p<0.05. The healthy physical-examination population was classified into five age categories (18–20, 21–25, 26–30, 31–35 and 36–40 years). Pearson’s χ2 test was performed to compare the prevalence of different lesions among the age groups. In addition, descriptive statistics were used to report the clinical characteristics of fibroadenoma (distributions of fibroadenoma side, number and size). Then, cross-tabulation of histological vs ultrasound diagnosis was performed. The sensitivity, specificity, positive and negative predictive values, and area under the receiver operating characteristic curve were calculated for ultrasound diagnoses of fibroadenoma. Agreement between ultrasound and histological diagnosis was measured using Cohen’s kappa (κ) statistic, where κ values of 0.41–0.60 indicated ‘moderate agreement,’ 0.61–0.80 indicated ‘substantial agreement’ and 0.81–1.00 indicated ‘near-perfect agreement.’ A p<0.05 was considered to indicate statistical significance.
Results
Prevalence of fibroadenoma in a healthy population undergoing examination
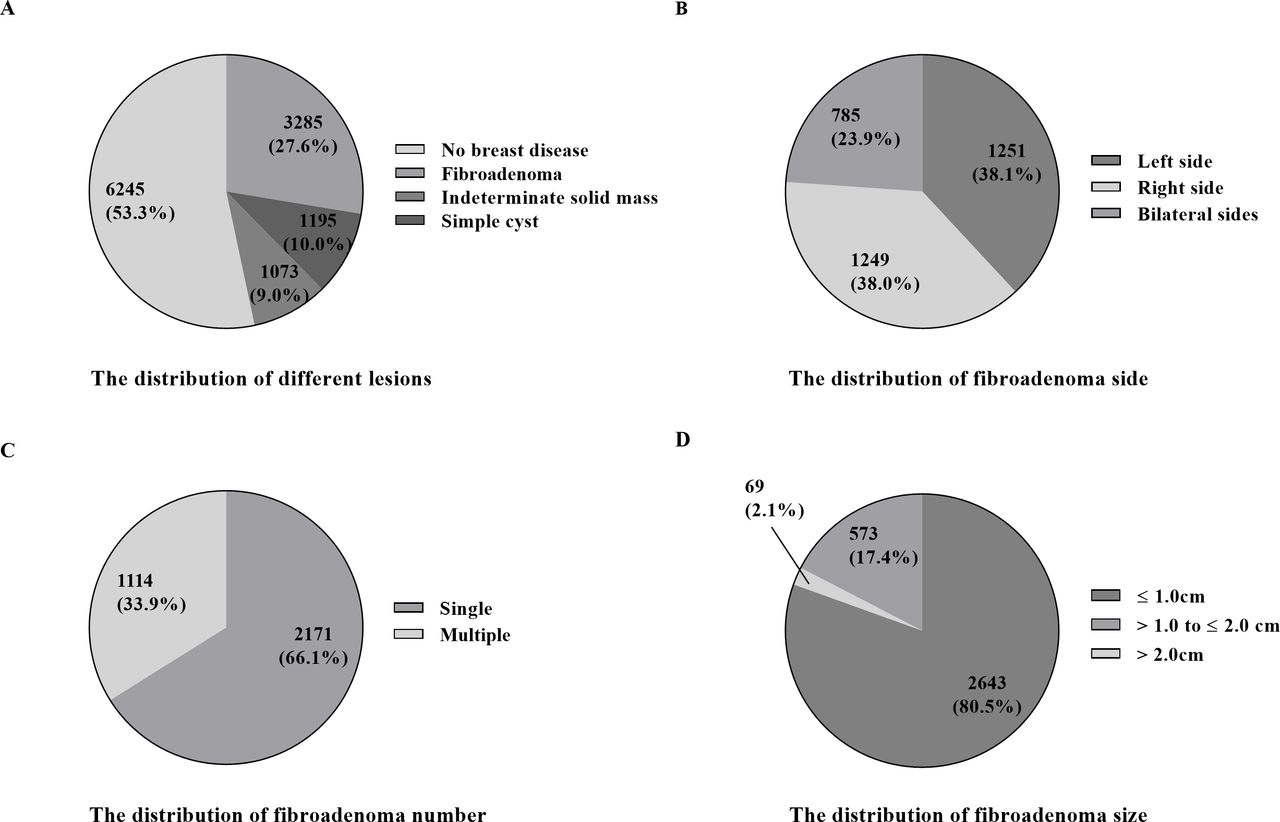
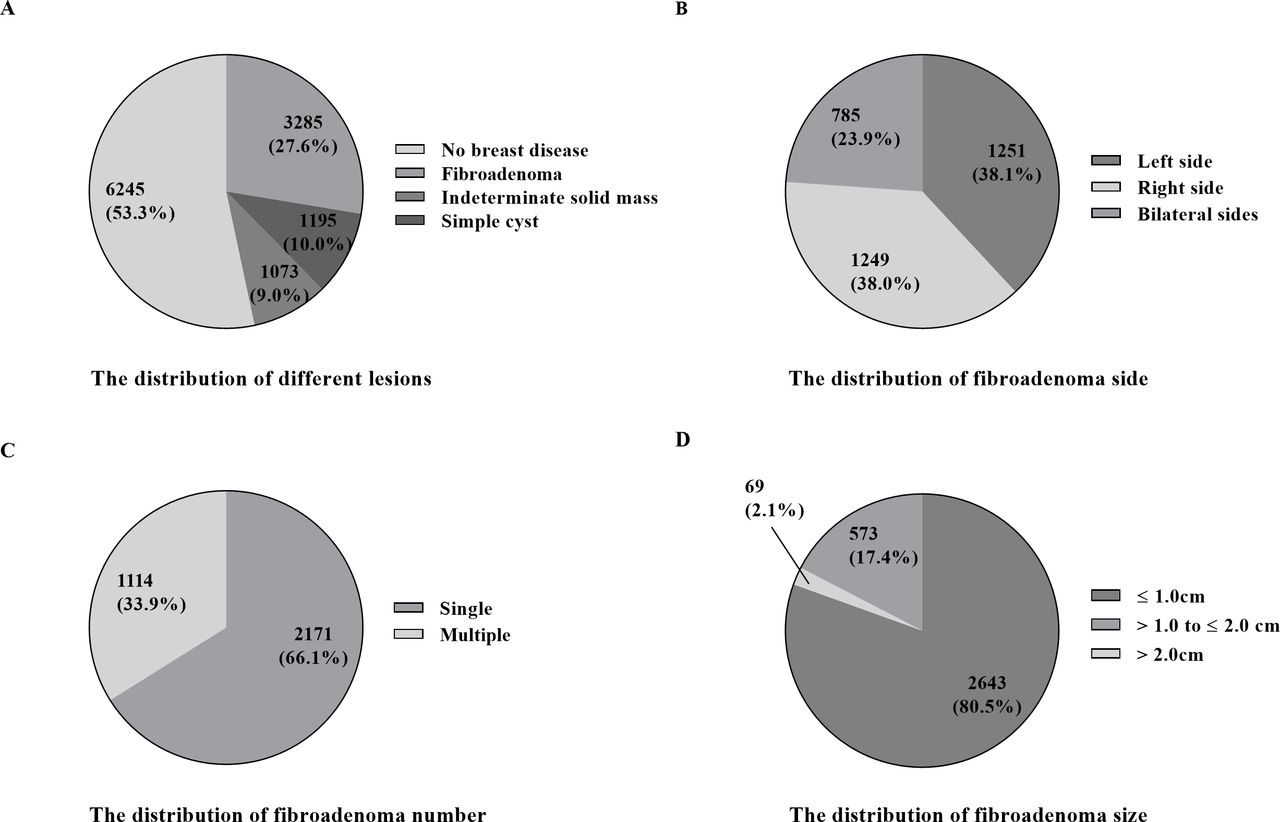
A total of 11 898 women were included. The study population’s age ranged from 18 to 40 years, with a mean age of 31.3±5.15 years. Of this population, 6345 (53.4%) women did not have breast disease based on the ultrasound diagnosis, whereas fibroadenoma was diagnosed in 3285 (27.6%), a simple cyst in 1195 (10.0%) and indeterminate solid masses in the remaining 1073 (9.0%) (figure 1A).
{kind=link}
Prevalence of different lesion types (A), distribution of fibroadenoma side (B), distribution of fibroadenoma number (C), and distribution of fibroadenoma size (D) in a healthy physical-examination population aged 18–40 years.
Patients were classified into five categories based on age (18–20, 21–25, 26–30, 31–35 and 36–40 years), with 133 (1.1%), 1758 (14.8%), 3521 (29.6%), 3492 (29.3%) and 2994 (25.2%) in each age group, respectively. Table 1 shows the age distribution of the prevalence of various lesions stratified by age. The rates of fibroadenoma were 19.5%, 27.4%, 27.1%, 27.6% and 28.8% in women aged 18–20, 21–25, 26–30, 31–35 and 36–40 years, respectively, and the prevalence was stable across age groups (p=0.14).
Age distribution of the prevalence of different lesions in a healthy physical examination population in the Guangdong province of China
The fibroadenoma was left sided in 38.1% (1251/3285), right sided in 38.0% (1249/3285) and bilateral in 23.9% (785/3285) of patients (figure 1B). A total of 2171 (66.1%) patients had single fibroadenomas, whereas 1114 (33.9%) had multiple fibroadenomas (figure 1C). Among the patients with unilateral fibroadenomas, 1096 (50.5%) had fibroadenoma solely on the left side, and 1075 (49.5%) had fibroadenoma on the right side. The size range of fibroadenomas was 3–42 mm, with a mean size of 8.2±4.2 mm. The majority of fibroadenomas (80.4%) did not exceed 1 cm; 17.4% ranged in size from 1 to 2 cm, and only 2.1% were larger than 2 cm (figure 1D).
Breast ultrasonography diagnostic accuracy
A total of 319 patients presented with breast lumps and underwent core needle biopsy or excision biopsy. All lesions were returned with pathological reports. Fibroadenoma was diagnosed for 203 (59.4%) lesions based on histological examination. Preoperative ultrasound images for each lesion were then retrieved, and 209 (61.1%) samples were identified as fibroadenoma and 133 (38.9%) as non-fibroadenoma based on ultrasound diagnosis. As shown in table 2, of the 209 study participants who were diagnosed with fibroadenoma by ultrasonography, 94.3% had fibroadenoma confirmed by histological diagnosis, whereas six and four participants were diagnosed with phyllodes tumours and tubular adenoma, respectively. Of the 133 study participants who were not diagnosed with fibroadenoma by ultrasonography, 127 (95.5%) did not have fibroadenoma confirmed by histological diagnosis, whereas the remaining six did have a fibroadenoma diagnosis. The sensitivity and specificity of ultrasonography for fibroadenoma (vs histological diagnosis) were calculated as 97.0% (95% CI 93.7% to 98.8%) and 91.4% (95% CI 85.4% to 95.5%), respectively. The positive and negative predictive values for ultrasonography were 94.3% and 95.5%, respectively (table 3). As shown in table 4, the ultrasound and histological diagnoses were concordant in 324 (94.7%) cases, with minor discrepancies in 18 (5.3%) cases. The concordance rate of ultrasonography and biopsy for fibroadenoma was 94.7% (κ=0.890, p<0.01).
Ultrasound diagnoses of the 342 histologically confirmed cases observed at the breast centre, Nanfang hospital between 1 June 2019 and 31 December 2019
Sensitivity and specificity of breast ultrasonography for the diagnosis of fibroadenoma
Diagnostic concordance of fibroadenoma using ultrasonography and histological tests
Discussion
The prevalence of breast fibroadenoma in women aged 18–40 years in our study was 27.6%, which represents accurate epidemiologic data for this benign breast tumour. In addition, ultrasonography showed high concordance with histological diagnosis, indicating that ultrasonography is an accurate diagnostic procedure for fibroadenoma, with high sensitivity and specificity in the absence of breast biopsy.10 15
To date, this was the largest-sample-size single-centre study to assess the prevalence of fibroadenoma. We found a higher incidence of fibroadenoma than the maximum of 25% reported in a previous study.16 The frequency of fibroadenoma in women aged 19–70 years was reported to be approximately 9% in 1974–1975 and 1984–1985 based on the review of benign breast biopsy specimens in Japan.6 One possible reason for the lower incidence of fibroadenoma compared with our study was that fibroadenoma was diagnosed using small-sample retrospective pathological data in previous studies. There may have been a high number of undiagnosed fibroadenomas among these real-world data. Of note, 34 of the lesions we reported appeared as lobulated hypodense masses, of which 30 were classified as fibroadenomas.
In diagnostic testing, the histology results differed in 12 of the 203 fibroadenomas diagnosed by ultrasonography, and none were malignant, indicating that ultrasonography had a positive predictive value of 94.3%. Nevertheless, there remain limitations of ultrasound diagnosis of fibroadenoma. We found that fibroadenomas were usually indistinguishable from phyllodes tumours and tubular adenoma on ultrasonography. Phyllodes tumours, which are typically observed in women aged 35–55 years and are usually large with a median size of 4 cm, require positive surgical revision because they correlated with larger size and malignancy and have a higher risk of local recurrence than fibroadenoma.9 Accurate diagnosis is essential to prevent both overtreatments of fibroadenoma and undertreatments of phyllodes tumour. A study found that preoperative fine-needle aspiration could help to distinguish these lesions.14 Tubular adenoma, an uncommon benign neoplasm of the female breast, usually presents as a markedly hypoechoic, circumscribed but unencapsulated mass, consistent with the ultrasonic features described by a previous study.17 Ultrasonography can help to identify the benign nature of this breast lesion; however, final confirmation is possible only after histopathological study. Overall, our study’s findings suggest that ultrasonography could be beneficial for the diagnosis of fibroadenoma, in agreement with previous studies reporting similar diagnostic accuracy for ultrasonography.
Ultrasonography achieved an excellent positive predictive value, with very small differences between actual and predicted values. In addition, the prevalence of fibroadenoma was stable across age groups and did not show any age-related difference. However, an early study in 1968 reported that the peak incidence of fibroadenoma occurred at age 20–29 years, with few cases occurring after age 50,18 consistent with other follow-up studies.12 By contrast, we did not find a statistical difference in age of onset. There was also no overall difference in prevalence between left-sided and right-sided fibroadenomas, although a recent prospective study of 145 patients with histological diagnosis reported that fibroadenoma was more common on the left side (48.9%).12 Multiple fibroadenomas were identified in 33.9% of the patients in this study, a higher value than that noted previously.19 Studies have shown that fibroadenoma may remain static or reduce in size over 5 years, and breast cancer arising in fibroadenoma was thought to be a random occurrence, tending to occur in women aged 40 years and over.20 These findings suggest that the fibroadenoma cases in our study could avoid excision and receive conservative therapy.
We found that the prevalence of indeterminate solid masses (9.0%) was higher in women aged 18–40 years. These masses do not present all the morphological characteristics of fibroadenoma on ultrasound images; therefore, these masses are classified as Breast Imaging Reporting and Data System (BI-RADS) 4 lesions because they carry similar risks of malignancy, higher than those of fibroadenoma. In our study, 10 of these masses were classified as BI-RADS 4 lesions because they mainly presented with poorly defined spiculated or angular margins (7/10), calcification in the nodule (5/10), an irregular shape (6/10) or no capsule (10/10). According to traditional views, histological characterisation is mandatory for these BI-RADS 4 lesions; the choice of therapy can be decided on evaluation of the specimens.21 However, recent studies have indicated that elastography may be a useful tool for distinguishing small, oval or round triple-negative breast cancers from fibroadenomas; this may help avoid biopsies of benign masses.15 22 The remaining 1063 breast solid masses were probably benign, having a low (<2%) risk of malignancy; for these masses, definitive management depends on whether they are upgraded to malignant or downgraded to benign lesions.23 For such cases, close short-term imaging follow-up would be ideal, especially in the initial 6 months after diagnosis.24 Follow-up based on imaging rather than biopsy for lesions sonographically described as probably benign will reduce medical costs and unnecessary invasive procedures.
The limitation of this study is that it was conducted at a single centre, which may have introduced a sampling bias. Women who are symptomatic are more likely to undergo a breast ultrasound in an outpatient department; therefore, symptomatic women were not included in the analysis. It is highly probable that some study participants underwent breast screening as a result of being symptomatic. However, even given this potential bias in the study population, it is likely that the prevalence of fibroadenoma identified in this study was much closer to the prevalence in real populations than the lower rates reported by previous small and medium sample size studies. In addition, Guangzhou is the capital of Guangdong province and the third-largest city in China, and a large proportion of the population living in Guangzhou comes from other areas. The Department of Health Management performed a survey of the population undergoing health examination between 2009 and 2018. Of the 916 066 individuals included, 37.5% of women who underwent physical examination came from other cities other than Guangzhou, and 17.7% came from provinces other than Guangdong province. Thus, the prevalence of breast fibroadenoma in our study is representative of Guangdong province and is likely to be representative of a larger cohort of the Chinese population.
Mammography is widely used as a screening tool for women aged over 40 years, whereas ultrasonography is recommended for screening of women younger than 40 years. However, mammography is not sufficiently accurate for a diagnosis of fibroadenoma. Herein, the study population was limited to women aged 18–40 years; therefore, our findings cannot be generalised to women outside this age group.
Conclusion
In summary, our study demonstrated that ultrasonography was an accurate tool for the clinical diagnosis of fibroadenoma. Using this method, the prevalence of fibroadenoma was shown to be as high as 27.6% in a healthy population in South China.
Data availability statement
Data are available on reasonable request. Data are available on reasonable request by contacting JD.
Ethics statements
Patient consent for publication
Ethics approval
The Nanfang Hospital Institutional Review Board approved this study (Protocol #NFEC-2020-266). The requirement for patient consent was waived by the Nanfang Hospital Institutional Review Board.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
LZ, XZ and SJ are joint first authors.
Contributors JD is responsible for the overall content as guarantor who accepts full responsibility for the finished work and/or the conduct of the study, had access to the data, and controlled the decision to publish. LZ conceived the project, drafted the study design, collected data, described and revised the ultrasound data, conducted analysis, interpreted data, and drafted the paper. XZ conceived the project, drafted the study design, collected data, conducted analysis, interpreted data, and drafted the paper. SJ conceived the project and drafted the paper. SR collected data and drafted the paper. HM collected data and described and revised the ultrasound data. YL edited the study design, drafted the protocol and interpreted data. CY edited the study design and interpreted data. JD conceived the project, edited the study design, collected data, conducted analysis, interpreted data and drafted the paper. All authors revised the paper critically for important intellectual content and approved the final version.
Funding This work was funded by the President Foundation of Nanfang Hospital, Southern Medical University, China (grant number 2020C032).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.