Article Text

Abstract
Purpose The rationale behind the SUDden cardiac Death in the Young (SUDDY) cohort was to provide a complete nationwide, high-quality platform with integrated multisource data, for clinical and genetic research on sudden cardiac death (SCD) in the young, with the ultimate goal to predict and prevent SCD.
Participants The cohort contains all SCD victims <36 years, in Sweden during the period 2000–2010. We assigned five population-based controls per case, together with parents of cases and controls, in total 15 633 individuals. Data of all individuals were extracted from multiple mandatory registries; the National Patient Registry, the Medical Birth Registry, the Prescribed Drug registry, the Cause of Death registry, the Multigeneration Registry, combined with socioeconomic data from Statistics Sweden. From SCD victims, the autopsy report, medical records, ECGs, parental information and biological samples were gathered.
Findings to date We identified 903 individuals diagnosed with SCD (67% men, 33% women). The cases comprised 236 infants <1 year of age (26%), 90 individuals aged 1–15 years (10%), 186 individuals aged 15–25 years (21%) and 391 aged 25–35 years (43%). Hospitalisations and outpatient clinic visits due to syncope were significantly more common among cases than controls. DNA obtained from dried blood spots tests (DBS) stored from birth was equally suitable as venous blood samples for high-throughput genetic analysis of SCD cases.
Future plans We will explore the SUDDY cohort for symptoms and healthcare consumption, socioeconomic variables and family history of SCD. Furthermore, we will perform whole exome sequencing analysis on DNA of cases obtained from DBS or postmortem samples together with parental blood samples in search for gene variants associated with cardiac disease. The genetic analysis together with data compiled in the nationwide cohort is expected to improve current knowledge on the incidence, aetiology, clinical characteristics and family history of SCD.
- FORENSIC MEDICINE
- GENETICS
- Cardiology
- Forensic pathology
- EPIDEMIOLOGY
- CARDIOLOGY
Data availability statement
Data are available upon reasonable request. Due to legislation the data is not freely accessible. However, within a collaboration aggregated data would be available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
The SUDden cardiac Death in the Young cohort represents all sudden cardiac death (SCD) cases from the entire country during 11 years, limiting ascertainment bias, and the selection of cases are thoroughly reported.
SCD victims were matched to five population-based controls, parents of cases and controls were included. Data of all individuals were extracted from multiple mandatory registries, from SCD cases, the autopsy report, and clinical data were collected.
The high proportion of autopsies (87%) and the low risk of missed cases are important factors for the strength of the study.
Limitation is the retrospective nature of the cohort and that the underlying cause of death based on clinical or forensic autopsies may be incorrect.
We have applied a ‘sudden’ criterion for inclusion in the cohort that may cause that some cases have been missed.
Introduction
Sudden cardiac death (SCD) is a major public health threat in the general population, with a reported annual incidence ranging from 50 to 100 per 100 000 individuals.1–3 The incidence increases with age and although rare in young individuals, SCD accounts for a large proportion of natural sudden deaths in the young (<36 years of age).3–7 Coronary artery disease (CAD) is the most common cause of SCD in older age groups. Present knowledge on the aetiology of SCD in the young is incomplete as the cause of death is often based on autopsies and histopathological reports alone that cannot always determine the cause of death.1 6 8Several studies have suggested that major causes of SCD in the young are inherited gene variants that predispose to fatal arrhythmias,4 5 9–12 bringing a risk of disease and death also to family members.13–16 Systematic clinical evaluations and genetic investigations could identify SCD cases caused by pathogenic gene variants, allowing for a subsequent presymptomatic screening of relatives at risk.7 13–17 Another challenge is to identify individuals at risk for SCD without prior family history of the disease. This requires identification of signs (including ECG) and symptoms preceding death.18 19 The true incidence of SCD as well as the frequency of underlying genetic factors in SCD is still largely unknown, due to differences in study design and case ascertainment criteria, small number of cases and difficulties in detecting all cases.3 20 21 Furthermore, the clinical routine does not include saving samples suitable for molecular genetic analysis.1 14–17 To overcome this, comprehensive registries have been proposed as best standards,4 19 22 exemplified herein by a complete population-based cohort of SCDs. The aim of the SUDden cardiac Death in the Young (SUDDY) cohort is to gather a detailed knowledge that can be helpful in the preventive work against SCD in the young.
Cohort description
The SUDDY cohort was established in 2017, and the database is held at Uppsala University, Sweden. This cohort is, as far as we know, the first complete nationwide population-based case-control study of SCD. The cohort comprises all individuals age 0–35 years diagnosed with SCD between 1 January 2000 and 31 December 2010 (table 1).
Baseline data for 903 afflicted cases of sudden cardiac death in persons age 0–35 year-olds in Sweden during 2000–2010
For each case, five population based controls were assigned from Statistics Sweden (SS),23 matched by sex, age and county (geographical area of residency, at time of death). Parents of cases and controls are also included. The total cohort consists of 15 633 individuals (figure 1). Data related to these individuals were extracted from multiple mandatory national registries (tables 2–5).
Data sources used in the study
Number of individuals with information from mandatory national registers
Number of cases with sudden cardiac arrest identified in The Swedish Registry for Cardiopulmonary resuscitation by witnessed cardiac arrest and given cardiopulmonary resuscitation
Diagnoses and number of individuals born in Sweden with data gathered from the Swedish Medical Birth Registry

The SUDden cardiac Death in the Young cohort enrolment flow chart. A total coverage of all sudden cardiac deaths (SCD) in Sweden during 11 years (2000–2010): 903 victims of SCD, 0–35 years of age, 4513 population-based controls, extended to 15 633 individuals including parents of cases and controls.
The causes attributed to SCD, based on autopsy reports and medical records, were sudden arrhythmic death syndrome (SADS), sudden infant death syndrome (SIDS), myocarditis, cardiomyopathies, congenital malformations of the heart, CAD and thoracic aortic dissection (TAD) (table 1, online supplemental table 1). Data management and statistical analyses were performed using R V.4.0.3.24
Supplemental material
Follow-up includes an interview-based questionnaire with first-degree relatives or partners, and later a clinical assessment visit for family members for genetic counselling, and for some of them predictive genetic testing, risk stratification, prevention and therapy. First-degree relatives of one diagnosis at a time are invited to participate. So far, a total of 73% of first-degree relatives in the arrhythmogenic right ventricular cardiomyopathy (ARVC) group have agreed to participate.
Data sources used in the study
Since 1947, every individual born in or living permanently in Sweden is given a unique 10-digit personal identification number (PIN).25 Also individuals born abroad with a PIN was included in the study (online supplemental table 2). We used the PIN to link study subjects to different national registers, and for retrieval of data from medical records of SCD cases (tables 2–5, online supplemental table 1 and 2). To optimise the identification of cases diagnosed with SCD within our population, we used three registers for best case selection: the Swedish National Board of Forensic Medicine (SFM) database, the Cause of Death Registry (CDR) and the National Patient Registry (NPR) (figure 1).
The registry of Swedish National Board of Forensic Medicine
The SFM registry comprises all individuals who underwent a forensic autopsy in Sweden. The registry contains coded death diagnoses according to the International Classification of Diseases (ICD), a short medical background and circumstances of death. The forensic report contains police reports, result of histopathology, toxicology screen and in addition often clinical records and interviews with relatives. The autopsies follow a standardised and detailed protocol according to consensus guidelines.26 A forensic autopsy is performed in all cases of unnatural deaths, and in most cases of unwitnessed out of hospital deaths that cannot be explained by the medical history of an individual. We used the SFM registry to identify cases in our cohort, and to retrieve data from the forensic reports.
Governmental registers held at the National Board of Health and Welfare (NBHW) and the agency SS
The Swedish Cause of Death Registry
Since 1952 all deaths in Sweden are registered in the CDR.27 There is a specific underlying cause of death recorded in 96% of individuals registered in the CDR.28 When an individual dies, a physician issues a cause of death certificate, which includes, name, PIN, place and date of death, the main diagnosis and secondary diagnoses relevant to the death, onset, course and durations of the underlying conditions. The cause of death certificate also includes previously known diagnosis and the type of autopsy performed, if any. The CDR was used to identify the cases in our cohort, and to retrieve the cause of death in deceased parents (tables 2 and 3).
The Swedish National Patient Registry
The NPR was established 1964, and has complete national-wide coverage since 1987.29 More than 99% of all somatic and psychiatric hospital discharges diagnoses are registred in the NPR, and a validation by the NBHW showed that 85%–95% of all diagnosis in the inpatient registry are valid.30 NPR also includes all data from public hospital-based outpatient care givers since 2001. However, primary care is not covered in the NPR. The NPR contains information on all inpatient and outpatient hospital visits, including ICD codes for each visit (ICD 8; 1969–1986, ICD 9; 1987–1996 and ICD 10 from 1997). Using the NPR, we retrieved previously known diseases for cases, controls and parents (tables 2 and 3). The NPR was also used to identify all individuals without the ‘sudden’ criteria, comprising cases diagnosed with Wolf-Parkinson White syndrome, TAD and CAD at any time, to increase the number of cases and to identify predisposing pathogenetic factors.
The Swedish Prescribed Drug Registry
The Prescribed Drug Registry includes data on all dispensed prescription drugs in Sweden since 1 July 2005.31 All drugs are classified according to the Anatomical Therapeutic Chemical classification system. Data on all dispensed prescription drugs were extracted for cases and controls.
The Swedish Medical Birth Registry
The Medical Birth Registry (MBR) was established in 1973,32 and includes all pregnancies that leads to birth and includes stillborn children after gestational week 22+0 since 1 July 2008, and before 2008 after 28+0 gestational weeks. MBR includes information on the pregnancy, the mother, previous pregnancies, labour, the new-born child, health of the new-born and presence of any congenital malformation.33 So far, cases diagnosed with SIDS and CAD, and their corresponding controls, were linked to MBR (table 5).
The Multigeneration Registry
The Multigeneration Registry (MGR) contains information on all residents born from 1932 and onwards as well as their relationship with biological and/or adoptive parents.34 MGR was used to identify parents of cases and controls (tables 2 and 3, online supplemental table 1). If a parent was connected to more than one child, case or control, information on the parent was gathered separately for each child. If a case had an adoptive parent, the case’s information was gathered but not from the biological parent, assuming that the child was in care of the adoptive parent.
The Register of the Total Population and Population Changes
The Register of the Total Population and Population Changes (TPR) was established 1967. TPR includes data on name, age, sex, place of birth, place of residence, civil status, citizenship, family relationship and migration.33 The registry was used to identify individuals, making up the control group (tables 2, 3 and 5, online supplemental table 1). For each case, five controls from the population have been drawn matched on sex, year of birth and county (geographical area of residency, at time of death). In a single case, three controls were identified. Each control subject was used only once, and not for different cases. Cases were not used as controls. The date of death serves as reference date in the cases whereas in controls the reference date was defined as the date when the control was of the same age as the corresponding case at death.
The Swedish Longitudinal Integrated Database for Health Insurance and Labour Market Studies
The Longitudinal Integrated Database for Health Insurance and Labour Market Studies (LISA) was established 1990.35 36 LISA contains annual data on aspects of labour, educational level, civil status, sick leave, income and family income. The cases, controls and parents were linked to LISA (tables 2 and 3).
The Swedish Registry for Cardiopulmonary Resuscitation
The Swedish Registry for Cardiopulmonary Resuscitation (SRCR) is a quality registry established 1990, and includes all out-of-hospital cardiac arrests given cardiopulmonary resuscitation (CPR), and since 2006 all in-hospital cardiac arrests given CPR and/or defibrillation.37 The SRCR was searched for cases in the cohort who received CPR (table 4). Data from SRCR together with the medical report and cardiac rhythm recorded by the emergency staff were gathered.
The Swedish Registry of Congenital Heart Disease
The Swedish Registry of Congenital Heart Disease (SWEDCON) is a Swedish quality register and includes data from all seven tertiary centres on congenital heart disease since 1998. SWEDCON contains information on diagnosis, interventions, symptoms, ECG, echocardiography, medications and social variables. We searched SWEDCON for data on cases included in the SUDDY cohort with congenital cardiac malformations.
Forensic and clinical autopsy reports
The forensic autopsy report contains a police report, results from examination of the body, histopathology, toxicology screen and often medical records and interviews with witnesses and relatives. The clinical autopsy comprises examination of the body and results from histopathological investigations. A pathologist with expertise in heart pathology is re-evaluating the histopathological slides of the individuals diagnosed with SADS, cardiomyopathy and myocarditis.
Other data sources used in the study
Electrocardiograms from military conscription: all ECG recorded at the time of conscription to military service were collected for 179 male cases. Military conscription was mandatory for 18 year olds in Sweden between 1901 and 2010.
Medical records: by using the unique PIN of each case, we collected medical records from hospitalisations and outpatient visits recorded in the NPR. To access medical records in Sweden, an application is sent to the corresponding healthcare region which grants permission after assessing that patient confidentiality is protected. After permission is granted, medical records from each patient are directly requested from the Hospital department where visits were recorded. Information on symptoms, known disorders and on-going medical surveillance, results from physiological and imaging studies, and circumstances preceding death were extracted.
Family survey: the closest living relatives of the deceased such as parents, spouses, siblings or adult children have been invited (so far ARVC, hypertrophic cardiomyopathy (HCM) and TAD) to answer an interview-based questionnaire, including symptoms and family history, and to provide peripheral blood samples for genetic analyses.
Existing samples and biological material
According to Swedish routine clinical practice, tissue specimens embedded in paraffin after formalin fixation (FFPE) from individuals subject to autopsies are archived at the local departments of forensic medicine and clinical pathology biobanks. Dried blood spot samples (DBS; Guthrie cards) from the national new-born screening programme are stored since 1975 at the PKU Biobank at the Centre for inherited metabolic diseases at Karolinska University Hospital, Stockholm, Sweden. In selected cases, we collected samples of heart and other available tissues archived as FFPE blocks or as fresh-frozen samples from national biobanks, as well as DBS samples for further molecular genetic analysis. DNA-extraction protocols were optimised to maximise the yield of non-fragmented high-quality DNA. Library preparation methods for whole exome sequencing (WES) were optimised for small amounts of fragmented DNA followed by high-throughput sequencing and bioinformatic analysis by in silico filtering of genes most relevant to SCD.38 39 We are performing WES of index patients and trios (ie, the deceased case and both parents) depending of the availability of DNA samples. Trio WES is a robust strategy that enables the possibility to identify de novo mutations or the mode of inheritance and has a higher diagnostic rate. GATK haplotype caller is used for variant calling. For variant annotation and filtering we will use Moon (2022 Diploid), a software package that autonomously returns candidate disease variants from Next Generation Sequencing (NGS) data using artificial intelligence and structured phenotype information entered as Human Phenotype Ontology terms. Variants will be classified according to the American College of Medical Genetics criteria.40 Results will be returned within the context of standard clinical genetic counselling (figure 2).

The SUDden cardiac Death in the Young cohort workflow of genetic studies. Trio or singleton whole exome sequencing analysis will be performed on dried blood spots or available postmortem samples, together with samples from parents and siblings. Identification of pathogenic and likely pathogenic variants in sudden cardiac death (SCD) cases will provide possibilities for predictive testing to at-risk relatives for prevention and treatment. Selected gene variants of uncertain significance may be further studied by functional studies or segregation analysis to clarify their role in SCD.
Population definition, selection procedure and disease definition
We performed a nationwide search for all SCD in individuals age 0–35 years, between 2000 and 2010 with a forensic autopsy. A forensic pathologist identified all cases meeting the inclusion criteria in the SFM registry. Furthermore, the CDR was scrutinised for all deaths in individuals of the same age and within the same time span for relevant ICD 8–10 codes to include also all individuals with a clinical autopsy and or no autopsy performed.41 We excluded all unnatural deaths, such as murder, suicide, accidents, drowning and intoxication (F10-F19, I26 and V01-Y98), and all non-cardiac diagnoses. All autopsy reports were independently reviewed by two physicians, to identify cases meeting the inclusion criteria. Likewise, two physicians independently reviewed all death certificates. In cases of disagreement, the autopsy reports or death certificates were re-evaluated to reach a consensus. Generally accepted criteria for definitions were used. SCD is defined as an ‘unexpected death due to cardiac cause within one hour after onset of symptoms in a person with known or unknown cardiovascular disease’, or if death was un-witnessed as ‘a person last seen alive and in good health <24 hour before being found dead’.1 Diagnoses of cases in the cohort were mostly autopsy-based (forensic autopsy 66.8%, clinical autopsy 20.6%). SCD cases without an autopsy with a previous clinical diagnosis of cardiovascular disease were included. Autopsy was performed according to national consensus documents and a Swedish accreditation standard protocol. Histological evaluations were performed to support the diagnoses in all subjects with a forensic autopsy and in most of cases with a clinical autopsy. The forensic autopsies in the study were performed or supervised by a limited number, approximately 20, experienced forensic pathologists, located in six regional departments. For each case included in the study, five controls were randomly assigned at SS. Furthermore, parents of both cases and controls were identified via the MGR. Cases, controls and their parents were then linked to Swedish healthcare registers (tables 2 and 3). Data were made pseudoanonymous, by replacing the PIN with a unique study number prior to making data available for the study team. The key linking the PIN with the unique study number is not available for the study team and held at SS.
Patient and public involvement
There were not any involvement in the design or conduct of the study by patients or public.
Findings to date
We identified 903 individuals, 609 (67%) men and 294 (33%) women, with SCD aged 0–35 years between 2000 and 2010. The median age at SCD was 22 years. We found 236 infants <1 year of age (26%), 90 individuals aged 1–15 years (10%), 186 individuals aged 15–25 years (20.6%) and 391 individuals 25–35 years (43.3%) (table 1). A forensic autopsy was performed in 603 cases (67%), a clinical autopsy in 186 (21%) and no autopsy in 114 cases (12%). In total, 136 SCD cases were identified in the SRCR. The event was witnessed in 67 individuals (53%), and in 105 cases (79.5%) CPR was given before the ambulance arrived (table 4). Among the cases, 93% were born in Sweden, and 7% abroad, 90% of controls were born in Sweden and 10% abroad (online supplemental table 2). To demonstrate the breadth of aims that can be addressed with the use of data in the SUDDY cohort, we have summarised four projects, two previously published.41 42
1: Incidence and aetiology of SCD
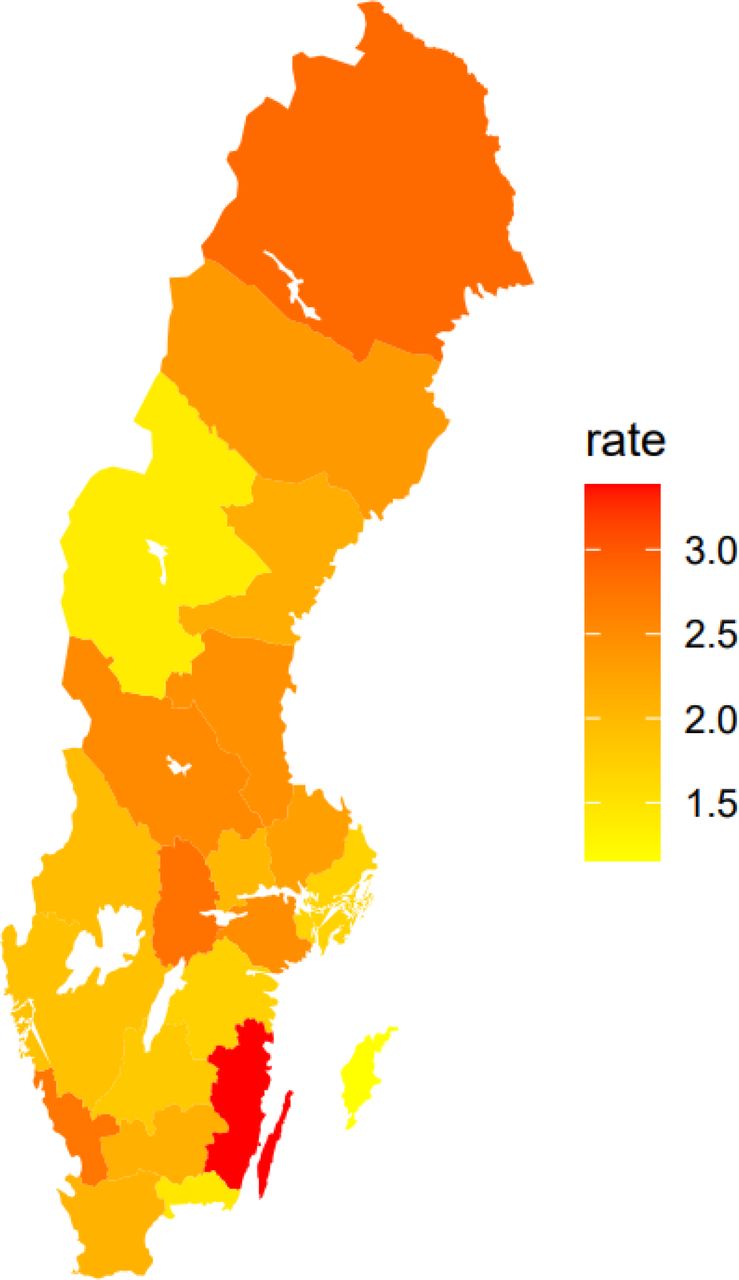
The incidence of SCD in the age span 1–35 years old was 1.3 per 100 000 person years, and 1.8 among individuals aged 15–35 years.41 The incidence of SIDS was 2.07 per 10 000 born per year. In the entire cohort (0–35 years old), the incidence, divided per county and by the number of inhabitants, was highest in the county of Kalmar with 3.376 per 100 000 inhabitants, and lowest in the county of Gotland with 1.160 per 100 000 inhabitants (figure 3). The most frequent diagnoses was SIDS, followed by SADS, CAD, myocarditis, congenital malformations, TAD, unspecified cardiomyopathy, HCM, ARVC and DCM (table 1, online supplemental table 1).
{kind=link}
{kind=link}
{kind=link}
Incidence of sudden cardiac death, 0–35 year olds, in Sweden 2000–2010, per county and per 100 000 inhabitants of age 0–35 years old.
2: Exercise related SCD
Sixty-two individuals died during physical exercise, including 21 competing athletes (one woman), and 41 recreational athletes (four women), the three most common diagnoses being SADS, HCM and ARVC.42 An ‘athlete’ was defined as a person who participated in organised team or individual sport activity that required regular practice and competition.42 Exercise-related SCD in cases aged 10–35 years (n=514) occurred in 12% of the subjects. A higher percentage of exercise related SCD was observed in athletes compared with non-athletes. When comparing the number of SCDs/year in young athletes in the 2000s with the 1990s the numbers have been almost halved.10 42
3: Hospitalisations and medical history
In the SUDDY cohort, hospitalisations were substantially more common among cases than controls prior to death, a surprising and unexpected result. We searched the NPR for hospitalisations and out-patient visits with ICD 8, 9, 10 codes for syncope (ICD10: R559, ICD9: 7802, ICD8: 78059), dizziness (ICD10: R42, ICD9: 7804, ICD8: 7800) and irregular heartbeat (ICD10: R002, ICD9: 7850, ICD8: 7851). We identified 24 (2.7%) cases and 17 (0.4%) controls (p<0.001), being hospitalised due to any of these diagnoses. A total of 19 (2.2%) cases were hospitalised due to syncope compared with 10 (0.2%) of controls (p<0.001), and 11 cases (2.1%) had an outpatient clinic visit due to syncope, compared with six (0.2%) controls (p<0.001). Any hospital admission was seen in 562 (62%) cases, and outpatient visits in 651 (81%) of the cases. An outpatient visit 5 days prior death was seen in 50% of cases. These striking results highlight the existence of symptoms and high frequency of hospital visits in SCD cases when compared with controls. This implies that there are risk parameters to consider for the identification of some individuals at risk and, thus, to offer prevention for SCD.
4: Molecular autopsy
DNA samples from SCD cases are seldom available as blood samples are not routinely collected at the time of death and FFPE samples contain fragmented DNA of poor quality. We therefore investigated whether DNA from DBS archived from the metabolic screen at birth could be used in the postmortem genetic investigations of SCD cases. The quality of DNA retrieved from DBS passed quality assessment for next generation sequencing. WES on DNA from DBS samples in 18 young cases of SCD, attributed to ARVC (figure 2), showed an average mean target coverage of 160X comparable to DNA extracted from peripheral blood from parents 155X, and >97% of target regions for DBS and blood had coverage over 30X. Thus, DNA obtained from DBS is highly suitable for next-generation sequencing analysis in SCD cases. WGS performance in DBS samples paired with venous blood samples has been studied before and DBS samples was found to be a robust alternative to blood for WGS.43 Analysis of data from WES obtained from DBS and FFPE in cases is ongoing in search for gene variants associated with cardiac disease (figure 2).
Strengths and limitations of this study
The SUDDY cohort has a complete coverage of all SCDs in the young in Sweden together with data from different nationwide mandatory registries. This completeness is unique. The study and data collected spans a period of 11 years and represents a spectrum of parameters that allows for the analysis of risk factors associated with SCD. The combined data, including ongoing genetic analyses, will improve knowledge on the aetiology of SCD in the young. The medical history, symptoms, healthcare consumption, educational level, socioeconomic related variables and hereditary burden in SCD, was in each case matched to five population-based controls for appropriate comparisons. Furthermore, parents of cases and controls are included in the SUDDY cohort. The selection of included SCD subjects is thoroughly reported,41 in contrast to other studies where inclusion/exclusion criteria are rarely reported in detail, and there is a solid knowledge about all cases. For example, there were subjects with autopsy and comorbidity not considered as a likely cause of death (eg, psychiatric disease and diabetes) included. We also included age group 0–1 which is rarely done in populations studies of SCD. We restricted SCD cases to age below 36 years since hereditary factors are more likely to be the cause of SCD in a large proportion of young cases. Furthermore, in this age group it is possible to use stored formalin fixed paraffin-embedded tissue, DBS samples from the newborn screening, and samples from living parents for molecular autopsy. In contrast, in cases >35 years of age CAD is the most common cause of SCD, and hereditary factors will be less prevalent and biological samples are more difficult to obtain. In Sweden, DBSs are collected at birth since 1975, an exclusive source for postmortem diagnostics, when no DNA-friendly material, just FFPE samples are saved at autopsy. Genetic analyses might enable us to modify diagnoses, and give a more specific diagnosis, for example, in cases with SIDS, SADS and non-specific cardiomyopathy. Numerous ethical considerations have been raised to deal with during the collection of data and building the SUDDY cohort database. For parents recruited to the study the investigation will raise memories of the tragic event, they may face genetic sequence variants that might not be harmful but still could be worrying, and genetic studies may reveal incidental findings. Therefore, results were/will be returned within the context of standard clinical genetic counselling, to help first-degree relatives to understand, adapt and adjust to consequences of genetic findings. Carriers of a pathogenic variant are referred for prevention and if needed treatment. Handling highly sensitive data (register data, genetic information) that consequently may interfere with a person’s integrity is another ethical concern. A nationwide as well as regional multidisciplinary network of cardiologists, and clinical geneticists exists, and we wish to include clinical and forensic pathologists in the network to improve the diagnosis of SCD. These expert networks should have mandate to perform postmortem genetic testing, to organise preventive strategies for family members, and ensure the prevention and treatment are implemented. Another task for a nationwide collaboration between expert networks could be to endorse a prospective registry aiming to improve diagnostics, and prevention of SCD. The high number of autopsies (forensic autopsy 66.8%, clinical autopsy 20.6%) and the limited risk of missed cases are important strengths of the study. SCD cases without an autopsy had a former clinical cardiovascular diagnosis. However, the postmortem investigation of SCD is a challenging task particularly in apparently young healthy individuals. In many cases, despite thorough investigation (external examination, anamnesis, autopsy, histological examination, toxicology), the cause of death cannot be fully established. This underlines the need for including other strategies in the investigation of sudden deaths. When no structural changes are identified, the underlying cause may still be a cardiac disease, such as ion channel diseases or cardiomyopathies with undetectable changes, but may also have non-cardiac causes, such as epilepsy, diabetes or the use of drugs not detected in toxicological analyses. The diagnostic problem in the investigation of SCD was described by the British pathologist Davis: ‘Giving the cause of sudden death for purposes of death certification is an exercise in probabilities rather than certainties’.44 The main limitations of the study were the retrospective nature of the cohort, and that the collection ended 2010. The underlying cause of death based on clinical or forensic autopsies still may be incorrect. In 12.6% of cases no autopsy was performed and the underlying causes of SCD are based on medical records only. Non-genetic factors may be the reason for SCD in a large proportion of patients such as myocarditis. Thus, the genetic analysis and the methods outlined are not expected to identify the primary cause of SCD in all cases. Another limitation is the lack of core lab of autopsy investigation of young SCD victims in Sweden. Furthermore, we have applied a sudden criterion for inclusion in our cohort and some relevant cases may have been missed. That has been a debate about the definition of ‘sudden death’ for many years. To classify unwitnessed death as sudden is very difficult, and authors have or have not classified these cases as sudden. In witnessed SCDs, we used the definition ‘death within one hour of symptoms onset’ and in unwitnessed SCDs ‘when the victim was in good health 24 hour before the event’,1 without knowing the duration of symptoms prior death in the latter. The SUDDY cohort is based on information gathered from different mandatory registries and sources (table 2). The variables defined from mandatory national registers as, for example, hospitalisations and dispensed drugs are considered complete by definition for the period in which the register was available nationwide and mandatory (eg, hospitalisations from 1987, dispensed drugs from July 2005). The cohort is matched for year of birth and the reference date is set as the date when the control was of the same age as the case. The parents ‘inherits’ the reference date from its child hence the distribution of the reference dates is similar in the different groups as can been seen in online supplemental figure 1. The missing pattern of the variables from the mandatory registers therefore follows the same pattern in different groups (online supplemental figure 1).
Supplemental material
Collaborators
The operational group of the SUDDY-cohort welcome collaboration and interest of colleagues in this field of research, questions and request for specific projects can be addressed to the corresponding author.
Conclusion
The SUDDY cohort linked to Swedish national, government-administered health registers allows us to study medical histories, the use of prescribed drugs, socioeconomic variables and hospital utilisation of cases and controls. In addition, use of molecular autopsy enables us to make more specific diagnoses. This is important as symptoms and healthcare consumption prior to death, socioeconomic differences, hereditary patterns and genetic causes are still not fully explored in the context of SCD.
From our initial data, we conclude that hospitalisations and healthcare contacts are more common among cases when compared with controls. Signs such as ECG-changes and symptoms preceding death were found in most cases, and heredity for SCD or a cardiac disorder was more common in cases than controls. We also found that DNA extracted from DBS samples of SCD cases collected at birth, in some cases more than 40 years ago, works equally well as fresh blood samples for whole exome sequencing.
Data availability statement
Data are available upon reasonable request. Due to legislation the data is not freely accessible. However, within a collaboration aggregated data would be available.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Umeå university Regional Ethical Review Board, Umeå, Sweden and later Uppsala University Regional Ethical Review Board, Uppsala, Sweden Reference number ethics approval: Dnr: 2017/430 and Dnr:2017/431. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The authors would like to thank Dr Peter Krantz, Department of Forensic Medicine, Lund University, Lund, Sweden, for selecting cases, and evaluating the forensic report of all SCDs from the registry of Swedish National Board of Forensic Medicine included in the study. We would also like to express our gratitude to the family members of the deceased for their cooperation and support.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors Conception and design of the SUDDY database study: AW, PK, E-LS (principal investigator). E-LS is the guarantor for the SUDDY database study. Contribution to the study design, and important intellectual input: EH, ND, AS, ADV, BS, JK, MB. Database care: BS. Preparation of figures: ADV, E-LS. First manuscript draft: E-LS. All authors provided review of the manuscript and approved the final version.
Funding This project was funded by grants from Marcus Borgström, The Swedish Society of Medicine, Norrbotten County council, the Swedish Research Council 2020-01947 (ND), Uppsala University Hospital, and Uppsala University, Sweden. Internal funding Region of Western Sweden (ALFGBG-720691) (MB).
Map disclaimer The depiction of boundaries on this map does not imply the expression of any opinion whatsoever on the part of BMJ (or any member of its group) concerning the legal status of any country, territory, jurisdiction or area or of its authorities. This map is provided without any warranty of any kind, either express or implied.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.