Article Text

Abstract
Introduction Patellofemoral pain (PFP) is a chronic condition that affects up to 25% of the general population and has a negative impact on functionality and quality of life due to the high levels of pain experienced by these patients. In order to improve pain and function, rehabilitation programmes that combine adjunctive treatments with exercise therapy are often used in research and clinical settings. However, despite the variety of adjunctive treatments available, their effectiveness when compared with exercise therapy has yet to be elucidated. Thus, the aim of this study is to evaluate the effectiveness of adjunctive treatments plus exercise therapy versus exercise therapy, and determine the relative efficacy of different types of adjunctive treatments plus exercise therapy for individuals with PFP.
Methods and analysis A systematic review and network meta-analysis will be conducted based on the Cochrane Collaboration recommendations and reported in line with Preferred Reporting Items for Systematic Review and Meta-Analysis guidelines. We will search Embase, PubMed (MEDLINE), CENTRAL, CINAHL, PEDro, SPORTDiscus, Web of Science and OpenGrey. It will be included randomised controlled trials that compared adjunctive treatment plus exercise therapy to placebo adjunctive treatment plus exercise therapy or exercise therapy. The outcomes of interest will be pain and function, with no restrictions on language, setting or year of publication. Study selection will be performed by two independent reviewers, based on the eligibility criteria. Risk of bias will be assessed using the Physiotherapy Evidence Database scale and the evidence summarised via the Grading of Recommendation, Assessment, Development and Evaluation approach. A Bayesian network meta-analysis will be performed to compare the efficacy of different adjunctive treatments plus exercise therapy. Consistency between direct and indirect comparisons will be assessed.
Ethics and dissemination No ethical statement will be required for this systematic review and meta-analysis. The findings will be published in a relevant international peer-reviewed journal and presented at conferences.
PROSPERO registration number CRD42020197081.
- PAIN MANAGEMENT
- Musculoskeletal disorders
- REHABILITATION MEDICINE
- SPORTS MEDICINE
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This systematic review will include any adjunctive treatment and exercise therapy programme available that assessed outcome measures of pain and/or function.
Randomised controlled trials with no restrictions on setting or year and language of publication will be included.
This protocol will reduce the possibility of duplication and is written and reported in line with Preferred Reporting Items for Systematic Review and Meta-Analysis guidelines.
The Physiotherapy Evidence Database scale and Grading of Recommendation, Assessment, Development and Evaluation approach will be used to evaluate risk of bias and quality of evidence for the outcomes reported, respectively.
The feasibility of this systematic review depends on the availability and homogeneity of trials and access to the data reported in the studies assessed.
Introduction
Patellofemoral pain (PFP) is a common chronic musculoskeletal condition characterised by pain around or behind the patella during activities that load the patellofemoral joint, such as squatting, stair ambulation and running.1 It affects both the general and athletic population, with an annual prevalence of approximately 23% of adults and 29% of adolescents in the general population, and 5.1%–14.9% in adolescent amateur athletes over one season.2
According to the literature, 57% of this population may experience persistent symptoms and unfavourable outcomes in 5–8 years.3 4 The severity of pain and symptoms associated with this musculoskeletal disorder negatively affect quality of life by limiting the ability to perform activities of daily living and occupational tasks and reducing participation in physical activity.5 6
Focusing on the rehabilitation of this population, some systematic reviews have evaluated the effectiveness of several adjunctive treatments combined with exercise therapy7–20 and/or multimodal physiotherapy programmes.7–12 14–16 20 These adjunctive treatments include patellar taping,7–12 14 knee10 12 14 and foot8 10 14–16 orthoses, electromyography biofeedback,8 14 17 dry needling19 and neuromuscular electrical stimulation.8 14 20 In general, there is limited and inconclusive evidence to draw conclusions regarding the effectiveness of these adjunctive treatment modalities for pain and function outcomes.
Although systematic reviews have investigated the effectiveness of including different adjunctive treatments in multimodal physiotherapy and/or exercise programmes, we feel it is relevant to synthesise the evidence based on an analysis of primary studies that evaluate the effectiveness of combining only one adjunctive treatment with exercise programmes, that is, not concomitantly including other treatment modalities, in order to assess the real effect of adding an adjunctive treatment in clinical practice. Another noteworthy point is that the comparative effectiveness of all the adjunctive treatments available combined with exercise programmes has never been studied. As such, conducting a network meta-analysis (NMA) provides an opportunity to combine direct and indirect evidence on treatment comparisons in a single analysis. Additionally, NMA can provide an estimate of the treatment most and least likely to be effective for a given outcome.
Thus, given the wide range of exercise programmes and adjunctive therapies available in both clinical and research settings, it is pertinent to summarise the findings of randomised controlled trials (RCTs) that evaluated the effects of combined interventions on pain and function, regardless of modality, using NMA. It is also important to assess whether including adjunctive treatment in exercise programmes is effective in a clinical setting, since its implementation requires the availability of material and therapist training to ensure the technique is correctly applied.
As such, the aim of this systematic review is to evaluate the effectiveness of adjunctive treatments combined with exercise therapy vs exercise therapy, and determine the relative efficacy of different types of adjunctive treatments plus exercise therapy for individuals with PFP using a Bayesian NMA.
Methods
The protocol was developed according to the Preferred Reporting Items for Systematic Review and Meta-Analysis Protocol (PRISMA-P)21 and Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for NMA (PRISMA-NMA).22 The protocol followed the Cochrane Handbook guidelines for Systematic Reviews of Interventions,23 and it was registered with the International Prospective Register of Systematic Reviews (PROSPERO).
Eligibility criteria
Inclusion criterion
Type of studies
Studies will be considered eligible for inclusion if they are RCTs that compare an intervention group (adjunctive treatment plus exercise therapy) with a control group (placebo adjunctive treatment plus exercise therapy or exercise therapy alone).
Type of population
Participants must have been diagnosed with PFP in line with the current recommendations for PFP diagnosis, whose core criterion is pain around or behind the patella, aggravated by at least one activity that load the patellofemoral joint during weight bearing on a flexed knee (eg, squatting, stair ambulation, jogging/running, and hopping/jumping).1
Type of intervention
The aim of the RCTs included in this review should be to assess the potential additional effect of the adjunctive treatment on exercise therapy. To that end, it is vital that both the intervention and control groups be submitted to the same exercise programme, with the adjunctive therapy being the only difference between them. Strength, stretching, endurance, power and proprioception exercises will be considered for the exercise programme.
With respect to adjunctive treatment, the following will be considered:
Non-pharmacological interventions such as patellofemoral knee orthoses (bracing), visual and EMG biofeedback, patellar taping, foot orthoses, manual therapy (mobilisation/manipulation), needling therapies (acupuncture and dry needling), patient education, behavioural/psychological therapy, weight loss intervention and any other complementary therapies.
Biophysical agents: shortwave, ultrasound, cryotherapy, phonophoresis, iontophoresis, electrical stimulation and laser therapy and any other complementary therapies.
Comparison of interest
Placebo adjunctive treatment plus exercise therapy or exercise therapy alone.
Outcome measures
Studies that assess pain and function through validate measures within PFP population will be included. Whenever possible, outcomes will be assessed in the short (<3 months), medium (3–12 months) and long terms (≥12 months), as described by Lack et al 24 and the ‘2019 Patellofemoral Pain Clinical Practice Guideline’.25
Exclusion criteria
Studies that examine other conditions (eg, patellar dislocation, patellar subluxation, patellofemoral osteoarthritis, patellar tendinopathy, Osgood-Schlatter disease, iliotibial band syndrome, Sinding-Larsen-Johansson syndrome or clinical evidence of meniscal injury, ligament instability or joint effusion) or assess participants who have undergone surgery, have reported pain from the lumbar spine, hips, ankles or feet, and those with symptomatic osteoarthritis in any lower limb joint will be excluded.
Search strategy
Electronic searches will be carried out on the PubMed (including MEDLINE), Cochrane Central Register of Controlled Trials (CENTRAL), Embase (via Elsevier), Physiotherapy Evidence Database (PEDro), CINAHL, SPORTDiscus (both via EBSCO) and Web of Science (via Clarivate Analytics) databases. In regard to grey literature, OpenGrey.eu will be searched to identify unpublished studies. The Patient Intervention Comparison Outcome (PICO)25 framework was used to formulate the research question for this study: ‘Is adjunctive treatment combined with exercise therapy more effective at improving pain and function in people with PFP than placebo adjunctive treatment plus exercise therapy or exercise therapy alone?’ The search strategy for each of the data sources was developed by two researchers (LRS and RFCMP) and can be viewed in online supplemental appendix 1. There will be no restrictions on the setting, language or year of publication. The electronic searches will be complemented by manual searches through the lists of references of the articles included.
Supplemental material
Data management
The search results will be entered into State of the Art through Systematic Review reference management software, in order to identify and eliminate duplicates.
Study selection and data extraction
Study selection
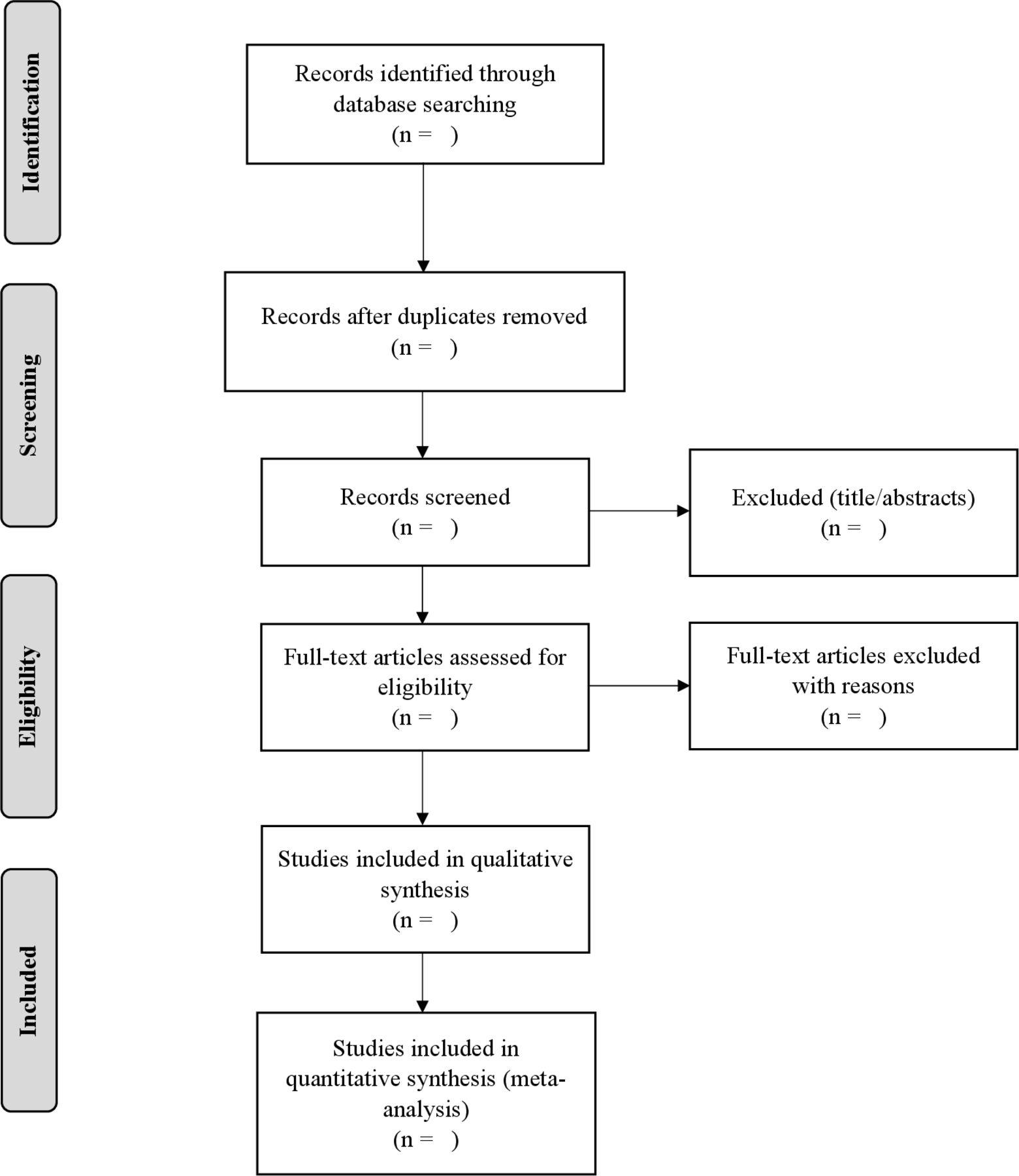
The selection process will be performed by two independent reviewers (LRS and MSB) who will screen the titles and abstracts. Once a consensus has been reached, both researchers will independently apply the inclusion and exclusion criteria after reading the selected studies in full. In the event of disagreements, consensus will be sought; however, if disagreement persists, a third reviewer (AMM) will be consulted. Should the complete article be unavailable, the reviewer (LRS) will contact the study authors. If the authors are unable to provide the full article or fail to reply to the request after three attempts, the study will be excluded. The reasons for excluding trials will be recorded. The reviewers will not be blind to the journal titles, study authors or institutions. The study selection process is shown in a PRISMA flow diagram (figure 1).26

{kind=link}
Flow chart and descriptions of study selection.
Data extraction
After the final consensus and selection of the primary studies, the two reviewers (LRS and MSB) will work independently. Disagreements will be resolved by consensus and, should they persist, a third reviewer (AMM) will be consulted. The following study characteristics will be extracted: publication details (author and year), participant characteristics (size and type of population, age, sex, pain intensity, severity of the functional disability and disease duration in months), number of individuals and men and women in each group, outcome measures and assessment tools used, treatment applied in the intervention and control groups (type of placebo, adjunctive and exercise therapies, treatment duration, number and frequency of sessions, follow-ups), adverse events and a summary of the main findings. For the meta-analysis and effect size calculation, post-treatment means and SD will be sourced from the original papers when available, or by contacting the authors via email in the event of missing data. Should the authors be unable to provide the missing data or fail to reply to the request after three attempts, the study will be excluded from further statistical analysis.27
Risk of bias and clinical relevance
The Physiotherapy Evidence Database (PEDro) scale will be used to assess the risk of bias of the studies included in this systematic review. The reliability of this tool is fair to good.28
Although the scale contains 11 items, specification of eligibility criteria will not be included in the final score, which will therefore range from 0 to 10. Each affirmative answer will receive one point and all these points will then be added to obtain the final score.29 The rating of studies indexed in the PEDro database will be maintained and the non-indexed studies will be independently evaluated by two reviewers (LRS and MSB). In case of disagreement, a third reviewer (AMM) will be consulted. Studies will be rated as low risk of bias (≥7/10), moderate risk of bias (4–6/10) and high risk of bias (≤3/10)30 based on this scale. Risk of bias will not be an inclusion criterion. The criteria recommended by Higgins and Green23 will be used to assess clinical relevance.
Quality of intervention descriptions
The Template for Intervention Description and Replication (TIDieR)31 checklist and guideline will be applied to evaluate how well the interventions are described in the RCTs. This tool was developed to improve the reporting of interventions across different study designs, such as trials, case–control and cohort studies.31 In order to adapt the instrument to the study purpose and create a score, a template similar to the PEDro scale was created,32 whereby the scores for each TIDieR item for the intervention and control groups were summed with each item assessed on a 3-point Likert scale, with the following categories: not reported (0), partially reported (1) and adequately reported (2). The summary score will be calculated by adding the score (0, 1 or 2) for the 12 items, with summary scores ranging from 0 to 24 points.32 Based on these scores, the studies included in this systematic review will be rated as having good (≥21/24), moderate (18–20/24) or poor intervention descriptions (≤17/24), based on the scores reported by Briani et al.33 It is important to note that this is a customised rating classification because there is currently no rating classification available in the literature. The TIDieR checklist will be completed and scored by two independent reviewers (LRS and MSB). Any discrepancies will be resolved during a consensus meeting, and a third reviewer (AMM) will be available to resolve any disagreements if needed.
Data synthesis and statistical analysis
Data synthesis
Pairwise meta-analysis
The Review Manager Software Package RevMan (V.5.3.) will be used for the pairwise meta-analysis.34 For data synthesis, studies will be assigned by subgroup category considering the type of adjunctive treatment applied, that is, knee braces, laser therapy, dry needling, etc. Meta-analysis will be performed only in the event of clinical and methodological homogeneity. Data will be pooled when studies are sufficiently homogeneous in terms of the population studied, intervention applied and comparisons performed (outcome measured and assessment times). The mean difference or standardised mean differences with 95% CIs will be used to calculate the continuous variables.
Network meta-analysis
Bayesian NMA will be conducted to compare the effects of different adjunctive treatments through direct and indirect comparisons. The Markov Chain Monte Carlo algorithm will be applied. All NMAs will be carried out using WinBUGS software (V.1.4, Medical Research Council, UK, and Imperial College of Science, Technology and Medicine, University of Cambridge, UK).
Measure of the pain and function outcomes will be presented as mean difference or standardised mean difference, with their 95% credible intervals. Both fixed and random effects models will be fit and model fit compared using the deviance information criterion and posterior mean residual deviance.
Assessment of heterogeneity
Two reviewers (LRS and RFCMP) will evaluate clinical, methodological and statistical heterogeneity. The I² statistic will be used to assess statistical heterogeneity, while methodological heterogeneity will be based on study biases and clinical heterogeneity on population characteristics.23
Transitivity analysis
For transitivity analysis, participant setting, symptom duration, age and baseline outcome values will be considered modifiers of treatment effects. Exercise modality and dose/intensity as well as adjunctive treatments will also be considered effect modifiers.
Exploring inconsistency in the network
Inconsistency (agreement between direct and indirect evidence) for both the pain and knee function outcomes will be evaluated globally and locally for each treatment comparison using node-splitting35 and by evaluating the statistical inconsistency of the network separately in every closed loop.36 Local inconsistency will be deemed statistically significant if loop-specific 95% CIs do not include zero.
Meta-biases
In order to determine whether reporting bias exists, the protocols of the studies included in this systematic review (when available) will be assessed to determine whether they were published before patient recruitment began. The presence of selective reporting of outcomes (outcome reporting bias) will also be evaluated.
Qualitative data synthesis
A qualitative data synthesis will be presented, even if the meta-analysis is not performed, including study characteristics such as year of publication, country of origin, sample size, type of intervention, outcomes and assessment tools used.
Certainty of the evidence (Grading of Recommendation, Assessment, Development and Evaluation (GRADE) approach)
Two reviewers (LRS and MSB) will independently evaluate the overall confidence in the evidence and strength of the recommendation using the GRADE approach, which analyses the following domains: trial design limitations due to risk of bias, inconsistency of results, indirectness in assessing the quality of a body of evidence, imprecision of results and publication bias.37 The strength of the evidence will be presented according to a rating system with four categories: high, moderate, low, or very low, in line with the GRADE approach.37
Dealing with missing data
Whenever possible, we will contact authors to request any missing data, especially for information that is needed to complete the meta-analysis. Should the authors be unable to provide the missing data or fail to reply after three attempts, the study will be excluded from further statistical analysis.27
Plans for documenting important protocol amendments
Should an event of any protocol amendments occur, the date of each amendment will be accompanied by a description of the change and rationale in this section. Changes will not be incorporated into the protocol.
Patient and public involvement
No patient involved.
Data sharing statement
Not applicable once this study is a protocol.
Perspectives
PFP is a chronic condition that significantly affects the quality of life of this population and may precede patellofemoral osteoarthritis,38 39 which results in greater functional disability and reduced quality of life. Thus, determining which treatment is most effective at improving pain and physical function in this population is highly relevant. In this respect, systematic reviews are important because they provide clinical evidence to guide clinical practice and scientific evidence for future studies, based on the gaps identified in the available literature. As such, we believe that this systematic review is important because it will make it possible to determine whether adjunctive treatment is relevant in a conventional exercise programme and, if so, which adjunctive treatment is more effective at improving pain and physical function when compared with a control group.
The results of this systematic review could contribute to justifying the need or not for costs related to the availability of material and therapist training when implementing adjunctive therapy in clinical practice.
Ethics statements
Patient consent for publication
Acknowledgments
The authors gratefully acknowledge the financial support from the Fundação de Amparo à Pesquisa do Estado de São Paulo—FAPESP (grant number 2020/03544-5) and the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior—Brasil (CAPES)—Finance Code 001.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @LarissaRSouto
Contributors LRS is the guarantor. LRS and FVS came up with the study idea. LRS, FVS, RFCMP, MSB and AMM designed the study. LRS and RFCMP designed the strategy search and the risk of bias. LRS, FVS and RFCMP designed the statistical analysis plan and drafted the manuscript. All authors provided feedback and gave important intellectual input. All authors read and consented to the content of the article.
Funding This study is supported by the Fundação de Amparo à Pesquisa do Estado de São Paulo—FAPESP (grant number 2020/03544-5) and the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior—Brasil (CAPES)—Finance Code 001. The FAPESP and CAPES did/will not have a role in the study design.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.