Article Text

Abstract
Objective In medical education, biochemistry topics are usually knowledge based, and students often are unaware of their clinical relevance. To improve students’ awareness of the relevance, we integrated communication skills training into biochemistry education. No studies before have examined the difference between peer and standardised patient (SP) role plays where students explain the biochemical background of a disease in patient-centred language. Therefore, we evaluated whether students’ self-perceived competency in Canadian Medical Education Directives for Specialists (CanMEDS) roles and their opinion of the quality of role play differ if the layperson is played by peers or SPs.
Methods We randomly assigned medical students in a preclinical semester to one of the two groups. The groups used predefined scripts to role play a physician–parent consultation with either a peer (peer group) or an SP (SP group) in the parent role. Students then assessed the activity’s effects on their competency in CanMEDS roles and motivation and the relevance of the role play. To determine whether students achieved biochemistry learning goals, we evaluated results of a biochemistry exam.
Results Students’ self-perceived competency improved in both groups. The SP group rated their competency in the roles ‘Scholar’ and ‘Professional’ significantly higher than the peer group did. The peer group rated their competency in the role of ‘Medical Expert’ significantly higher if they played the role of the parent rather than physician or observer. The SP group agreed more that they were motivated by the role play and wanted to receive more role play-based teaching. The SP group perceived the role play as being realistic and rated the feedback discussion as more beneficial. The examination results were the same in both groups.
Conclusion We showed that role plays in a biochemistry seminar improve students’ self-perceived competency. The use of SPs has some advantages, such as being more realistic.
- Biochemistry
- EDUCATION & TRAINING (see Medical Education & Training)
- MOLECULAR BIOLOGY
Data availability statement
Data are available upon reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information. The datasets generated and analysed during the current study are not publicly available due to large amount but are available from the corresponding author on reasonable request. All data relevant to the study are included in the article.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
Implementation of role play early in medical education to strengthen communication skills.
First comparison of the use of standardised patients or peers in a preclinical biochemistry seminar role play activity.
Explores CanMEDS roles as a basis for a self-rating instrument about competencies.
Effects of the role play on the acquisition of factual knowledge (examination scores) were examined.
Data were mostly generated by self-ratings, and communication skills were not objectively assessed.
Introduction
Competency-based learning goals play a central role in medical education.1 2 However, biochemistry learning objectives in undergraduate or preclinical medical education are usually knowledge based, and students often are not aware of their medical and clinical relevance.3 Therefore, to stimulate student learning behaviour, universities have launched the first initiatives to combine learning content in biochemistry with relevant clinical topics. In a previous study, we started integrating communication training embedded in a clinically relevant scenario into biochemistry seminars.3 4 The seminars were held in an inverted classroom setting in which students acquired learning material in an initial self-learning phase before applying and discussing it with the lecturer in subsequent on-site sessions.3–6 In comparison with the traditional teaching method, the inverted classroom method enables students to reach a higher learning level according to Bloom’s taxonomy (eg, ‘understand’ or ‘apply’).7 Specifically, in peer role plays we trained the students in communicating (eg, ‘explain’ or ‘illustrate’ according to Bloom’s taxonomy) as physicians (experts) with patients (laypersons) to prepare them for their later professional lives.
Our approach was in accordance with international (eg, Canadian Medical Education Directives for Specialists (CanMEDS))1 2 8 and national frameworks (eg, the German Masterplan Medizinstudium 20209), which represent matrices that aim to integrate clinical topics into the early phase of medical studies and to place a stronger emphasis on competency-based training. The competencies that need to be acquired during medical training include self-regulation and self-reflection (CanMEDS role of the professional); shared research and evidence-based proceeding (CanMEDS role of the scholar); mentoring (CanMEDS role of the health advocate); economy and sustainability (CanMEDS role of the manager/leader); partnership, trust, and equity (CanMEDS role of the collaborator); and transparency and respect (CanMEDS role of the Communicator).1 2 One should note that these competencies are interdependent.
Communication skills are central for future physicians. During their preclinical studies, medical students mainly learn complex facts and processes required for understanding physiological processes and disease development. To pass their examinations, they also learn to use technical terms to explain difficult content and to communicate precisely with colleagues. However, patients are usually not medical experts, so physicians have to be able to explain complex medical information on diseases in a patient-centred manner that uses easily understandable sentences to explain technical terms. Competent communication skills require deep subject matter knowledge and are required to ensure patient understanding and compliance10 11: If a patient does not understand the purpose of the treatment, adherence to it will likely be low. Furthermore, communication training in medical students has been shown to improve their later effectiveness as physicians on different levels, that is, transfer and understanding, empathy and compliance. Thus, training of communication skills is highly important and should start during the first phase of medical education (German Masterplan Medizinstudium 2020). However, education interventions that combine basic knowledge and clinical content and competencies are rare in the field of preclinical biochemistry education.
Recent studies compared the effects of medical communication training with role plays performed with either peers or standardised patients (SP), that is, trained actors, and most showed that peer and SP role plays are comparably effective, supporting their inclusion in medical curricula.12–15 Both peer and SP approaches also led to the same levels of skills attainment in undergraduates and health professionals. However, studies of objective performance analysed only one specific task that focused on one specific aspect of communication, for example, behavioural change management.13–15 Therefore, these studies do not allow us to draw clear conclusions about the general value of role plays with peers and SPs in a broader medical context.
When students perform role plays for communication training, they have to both elaborate on the taught subject matter by using their prior knowledge and rephrase the information in their own words in a patient-centred way. The role play may also include explanations and discussions. These activities are very likely to promote learning and a deeper understanding of the subject matter.16 17
A previous study revealed that both peer and SP role plays were well accepted by students and rated as realistic and valuable tools for training communication between physicians and parents in the field of paediatrics.12 However, students considered training with SPs to be more useful than training with peers and to better represent future real physician–parent contacts. Also, SP-based training enabled the teacher to give formative feedback and assessments, which facilitated the learning process. Whether role plays with peers or SPs improve specific CanMEDS roles is still unknown. Therefore, we performed the current study to analyse whether role plays can be successfully integrated into a preclinical biochemistry seminar and whether they are accepted by students. Our study focused on the following questions:
Do role plays improve medical students’ self-perceived competency in CanMEDS roles?
Is there a difference in medical students’ self-perceived improvement in CanMEDS roles between role plays with peers and those with SPs?
Is there a difference in students’ evaluation of role plays with peers and those with SPs?
Does medical students’ knowledge of biochemistry in a written multiple choice test differ depending on whether role plays are performed with peers or SPs?
Materials and methods
Course and study description
The study was performed in the biochemistry seminar ‘From Gene to Protein’, a mandatory seminar for second semester medical students at Ulm University, Germany.4 The seminar was taught by one lecturer (SJK or MK) to 16 classes of about 20 students each and was held in an inverted classroom setting in which students studied online on their own before attending on-site learning. The seminar in the current study comprised two on-site sessions of 4 hours each (figure 1), with 1 week in between; each on-site session was preceded by a self-study phase. Each of the 16 classes performed the role play exercise to train communication skills during the second on-site session; the classes attended the seminar consecutively, so the total study duration was 2 months. The role play consisted of a physician–parent consultation in which the role of the parent was played by either peers (peer group) or SPs (ie, trained actors (see below); SP group).
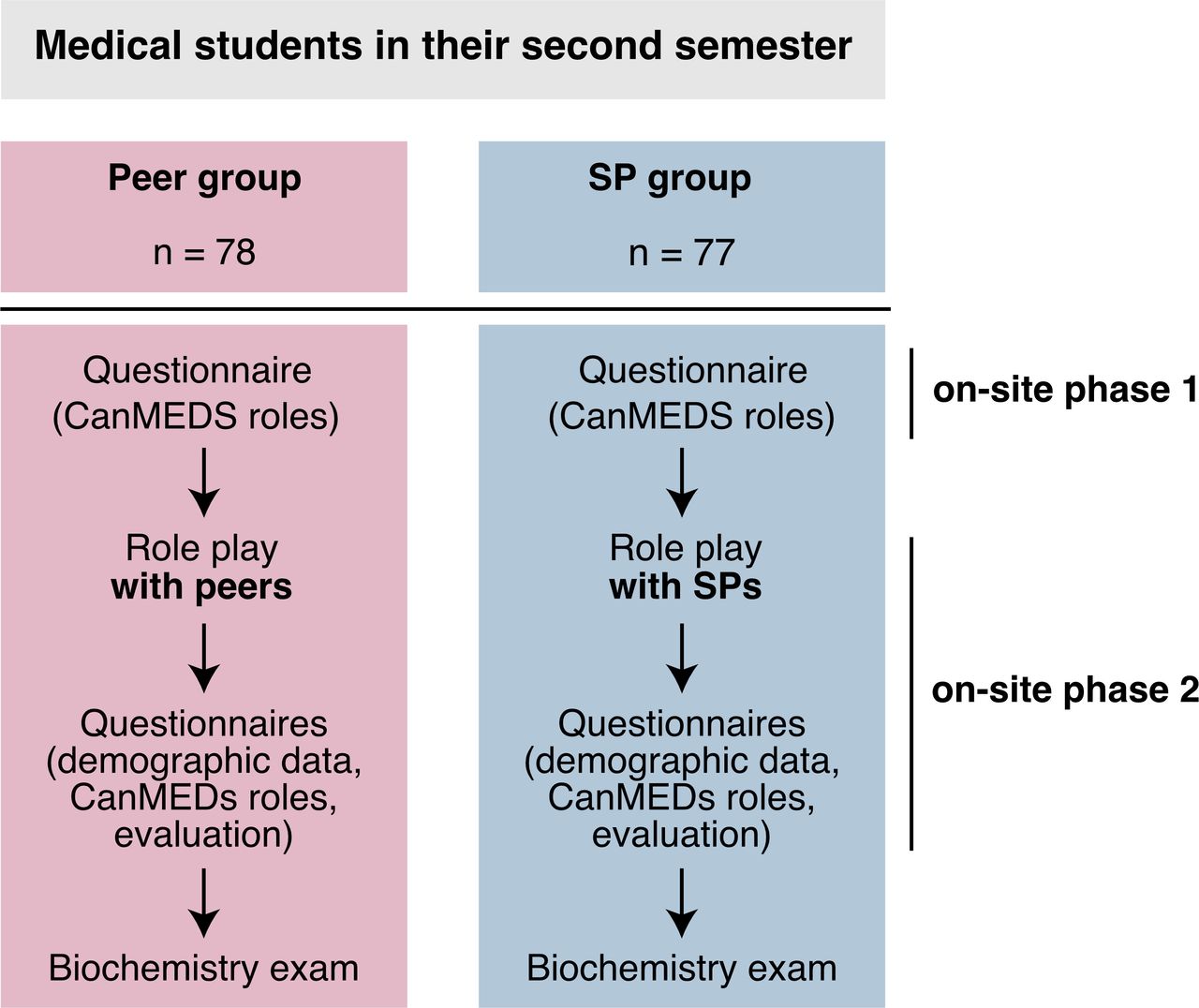
Study design. Role plays have been performed with peers (peer group) and SPs (SP group). CanMEDs, Canadian Medical Education Directives for Specialists; SP, standardised patient.
Participants in the study and group allocation
A total of 155 second semester medical students participated in this study (8 of 16 classes). At Ulm University, medical students are randomly assigned to classes by the Office of Student Affairs at the Medical Faculty. We randomly allocated students to the peer group or SP group without any influence from the lecturers.
Selection and preparation of standardised patients
The two SPs in the study were well-trained, experienced members of the Ulm Medical Faculty Standardised Patients Programme. All participants in this programme are actors and are trained by the head of the Ulm SP programme (VK), a trained drama educator. Before the study, the SPs attended a meeting to become acquainted with the contents, purpose and general framework of the planned lesson. After agreeing to prepare for the role of a parent in our study, each actor was given extensive role-specific training in which the intended scientific and communicative learning goals were identified and details of the SP response repertoire were finalised. Furthermore, both SPs attended general role play and feedback workshops, which are a routine element of the Ulm SP training programme. Thus, the SPs were well prepared to perform the required role of parent, to record and to evaluate subjective impressions during the student encounters and to subsequently reflect on their experience in a professional manner.
Role scripts
Scripts have been shown to positively support simulation-based learning.18 Therefore, for all roles, that is, physician, observer and parent, we created scripts for a consultation with the parent of a child with osteogenesis imperfecta. The physician was also given X-ray images of broken bones of the child to show the parent during the consultation. Students in the role of the physician were asked to use simple, patient-oriented words when talking to the parent. The parent was given an article from the German digital newspaper ‘Spiegel Online’ about a child with frequent bone fractures.19 The article claimed that this child’s disease was caused by gluten intolerance, and during the consultation with the physician in our study, the parent had to ask whether gluten intolerance could be the reason for their child’s broken bones. As a second possible cause, the parent was instructed to ask about osteoporosis. If the physician used the term ‘collagen’, the parent was told to ask about collagen-containing ointment as a treatment option. Feedback questions were integrated into all scripts for the feedback discussion (the guiding questions for the feedback discussion are provided in the online supplemental file 1).
Supplemental material
Role play with peers (peer group)
Peer group classes were divided into three teams. Team 1 consisted of students representing a physician in which one student was prepared for playing the role of the physician with the script explained above and was supported by his or her teammates. Team 2 consisted of students (peers) representing a parent (mother or father); again, one student was prepared for playing the role of the parent with the script described above and was supported by his or her teammates. Team 3 comprised student observers, who were guided by predefined feedback questions. These students were given a role script similar to that of the parent role script but were not given the additional information about the questions on gluten intolerance, osteoporosis, and collagen-containing ointment.
Unlike the SPs, students were not trained in how to competently play specific roles because both teachers and students lacked the resources for such training. Furthermore, communication skills were not formally assessed to allow the students to obtain first experiences with patient encounters without feeling pressured and because these skills are formatively assessed in the fourth and fifth year of medical training.
Role play with standardised patients (SP group)
Students in SP classes were divided into two teams, that is, a physician and an observer team; one of the two SPs played the role of the parent. The role scripts were the same as those used in the peer group.
Procedure of the role play session
After 20 min preparation, the consultation started between the physician and the parent, and the student playing the role of physician had to explain the biochemical background of osteogenesis imperfecta to the parent in patient-centred language. During the consultation, the peer or SP playing the role of the parent asked questions (see above) and the physician replied. After the consultation, students, teachers and peers (peer group) or SPs (SP group) held a feedback discussion because feedback is typically considered as a core part of communication skills training.20 21 To standardise the feedback sessions, students were familiarised with the general feedback rules,22 and the discussion and feedback discussion was subsequently conducted in a way that adhered closely to the guiding questions (which are provided in the online supplemental file 1).
Questionnaire on competency development
Students’ self-rating about the seven CanMEDS roles (Scholar, Communicator, Collaborator, Health Advocate, Manager (changed to ‘Leader’ in the new nomenclature), Professional, Medical Expert)1 2 was surveyed during the on-site sessions 1 (before the role play) and 2 (after the role play) (figure 1). Because the CanMEDS roles reflect continuous professional development, questions on these roles were taken as surrogates for the impact of the role plays on students’ self-perception of these items. To assess their self-perceived competency, in a paper-based questionnaire, students were asked to rank their competency in each CanMEDS role on a nine-point Likert-type scale ranging from 1 (beginner) to 9 (professional), whereby the scale was subdivided into three levels: beginner (rating of 1 to 3), intermediate (rating of 4 to 6) and professional (rating of 7 to 9). The CanMEDS concept2 was introduced in Germany in 2015 by the National Competency-based Learning Objectives Catalogue in Medicine (NKLM23), but it is not compulsory in the German medical curriculum (as based on the German Medical Licensure Act). In the study, we briefly discussed the CanMEDS concept with the students before the role plays, and in the questionnaire each role was accompanied by a brief description (3 to 4 sentences). To link the data in the questionnaires completed at on-site sessions 1 and 2, students were asked to label the questionnaires with a standardised, five-digit pseudo-anonymous code (the questionnaire ‘after the role play’ is provided in the online supplemental file 1).
Questionnaires about demographic data and the quality of the role play
We asked students to specify their age, sex, previous relevant medical education lasting at least 1 year (eg, nursing, emergency technician), and any university degree obtained before they started studying medicine. Students who participated in the role play with a peer (peer group) also had to state which role they took (observer, physician or parent). To analyse the quality of the role play, we handed out questionnaires that asked students to evaluate the role play on a six-point Likert-type scale ranging from 1 (strongly disagree) to 6 (strongly agree). The overall assessment of the role play was rated by students on a six-point Likert-type scale ranging from 1 (insufficient) to 6 (very good).
Written biochemistry multiple choice exam
To assess their attainment of the biochemistry learning goals, all students took a written biochemistry examination 2 weeks after the last class had completed the seminar. The summative test consisted of 20 multiple choice (MC) questions of the type Apos and Aneg (single best choice) and mainly tested knowledge on competency level 1 of Bloom’s taxonomy (eg, ‘remember’).7 Data were used to examine research question 4, namely whether students’ knowledge of biochemistry in a written multiple choice test was different depending on whether the role play of the parent was played by a peer or SP.
Data analyses and statistics
Before the analyses, we checked the plausibility of the data. Because not all students responded to all statements, the sample sizes varied slightly. As a measurement of learning gain in the seven CanMEDS roles, we calculated changes in self-appraisals as the difference between the student’s score before and after the role play. Nominal data (sex, relevant medical education, previous degree) were analysed with χ2 tests. Because the metric data (age, self-appraisals, evaluations and learning gain) were not normally distributed (significant Kolmogorov-Smirnov tests), we used Mann-Whitney U tests for two-group comparisons and Kruskal-Wallis H tests to compare more than two groups, that is, for data on students’ assumed roles during the role play (observer, physician, parent); we also used Mann-Whitney U tests for post hoc comparisons. Repeated measurements on questions regarding the seven CanMEDS roles were tested with Wilcoxon signed-rank tests. Analyses were two tailed, and p values <0.05 were considered to be significant. We also calculated Cohen’s d to evaluate effect size.24
Patient and public involvement
Patients and/or the public were not involved in the design, conduct, reporting or dissemination plans of this research.
Results
Participants
Not all study participants (N=155) filled out or handed in all the questionnaires. This was particularly true for the questionnaire on competency development, which was used for repeated measurements. As a result, paired data of 141 participants (91% response rate; SP group, n=70; peer group, n=71) were available for the respective analyses. In addition, not all students responded to all questions (eg, some students missed some questions), so the sample sizes vary slightly.
Data of N=154 students were available for the analyses of demographic data. Subsample sizes and the demographic data of the participants in the various subsamples are shown in table 1. The mean age was significantly lower in the peer group than in the SP group (p=0.018), but we found no other statistically significant differences between the demographic data in the two groups. We did find some variation in former education, which is discussed in the limitations section.
Demographic data of students participating in communication training in a biochemistry seminar
Students’ self-appraisal of their competency development: CanMEDS roles
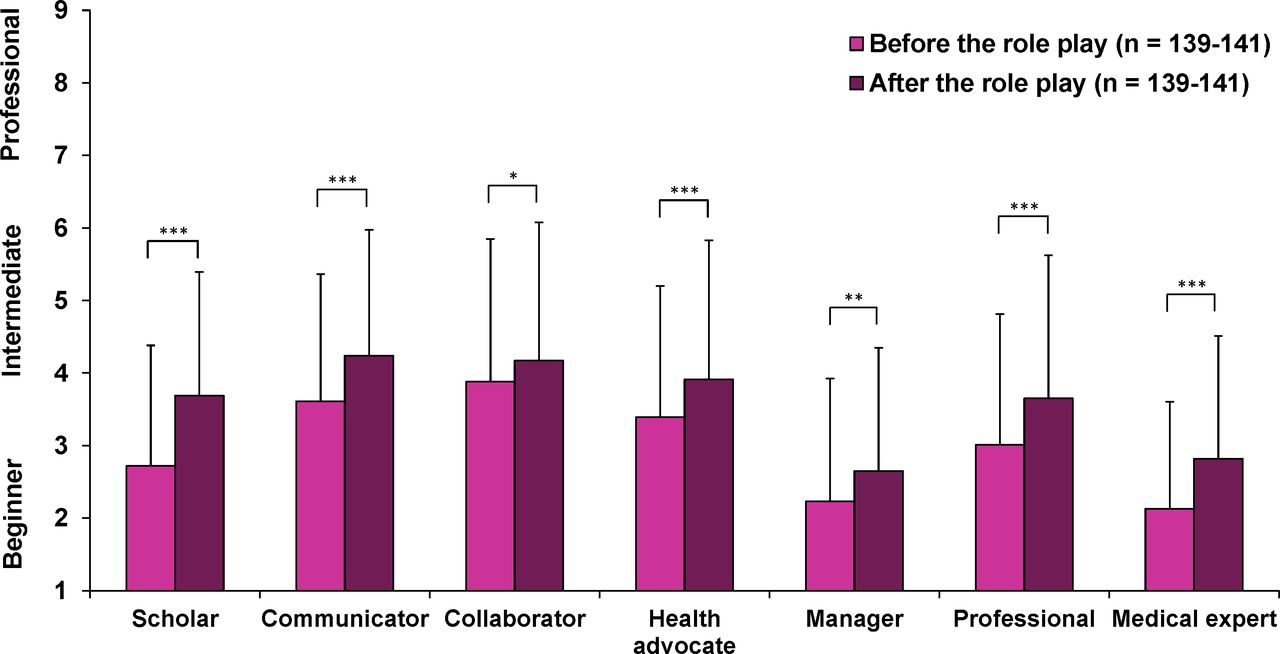
As a surrogate for the impact of the role play in general and to compare the use of SPs and peers in detail, we asked the students to rate their CanMEDS roles during on-site sessions 1 and 2 (ie, before and after the role play, figure 1). When both the peer groups and SP groups were analysed together, students’ self-appraisals about all CanMEDS roles increased significantly after the role play (figure 2, online supplemental table 1).

Mean (SD) values of self-appraisals of all students (independent f group) for the seven Canadian Medical Education Directives for Specialists (CanMEDS) roles. Students self-rated their competency on a nine-point Likert-type scale before and after a role play to train communication skills. A score of 1 to 3 was classified as beginner, 4 to 6 as intermediate, and 7 to 9 as professional. * p<0.05, ** p<0.01, *** p<0.001.
Before the role play (baseline), we found no statistically significant difference between the peer groups and SP groups in the self-appraisals of any of the CanMEDS roles (all p>0.132; data not shown). After the role play, when considering the measurement of learning gain (difference in self-appraisals before and after the role play) we found significant differences between the peer groups and SP groups in their self-appraised competencies in the CanMEDS roles ‘Scholar’ (p=0.027, d=0.46) and ‘Professional’ (p=0.043, d=0.28) (figure 3).

Mean (SD) differences in students’ self-appraisals of competency in the seven Canadian Medical Education Directives for Specialists (CanMEDS) roles as a measurement of learning gain. Students self-rated their competency in the various roles on a nine-point Likert-type scale ranging from 1 (beginner) to 9 (professional) before and after a role play to train communication skills. Differences were calculated by subtracting individual scores before the role play from those after the role play. Abbreviation: SP = standardised patient; * p<0.05.
When comparing student learning gains in the peer group according to the students’ role (observer, physician or parent), we found no differences before the role play (baseline; p=0.492; data not shown). After the role play, we found significant differences in the role medical expert: Students in the role of the parent showed a higher learning gain on their self-appraised competency than both those who assumed the role of the physician (p=0.039, d=0.69) and those who assumed the role of an observer (p=0.005, d=0.90) (figure 4). For the other CanMEDS roles, we observed no differences between students in the role of observers, physicians or parents.

Mean (SD) differences in students’ self-appraisals of the Canadian Medical Education Directives for Specialists (CanMEDS) role Medical Expert before and after a role play exercise on physician-parent communication in which peers played the role of physician (team 1), parent (team 2), or observer (team 3). The difference was calculated as a measurement of learning gain by subtracting individual self-appraisals before the role play from self-appraisals after the role play. Students self-rated their competency on a nine-point Likert-type scale ranging from 1 (beginner) to 9 (professional). Abbreviations: SP = standardized patient; * p < 0.05, ** p < 0.01.
Student evaluations of peer and SP role play
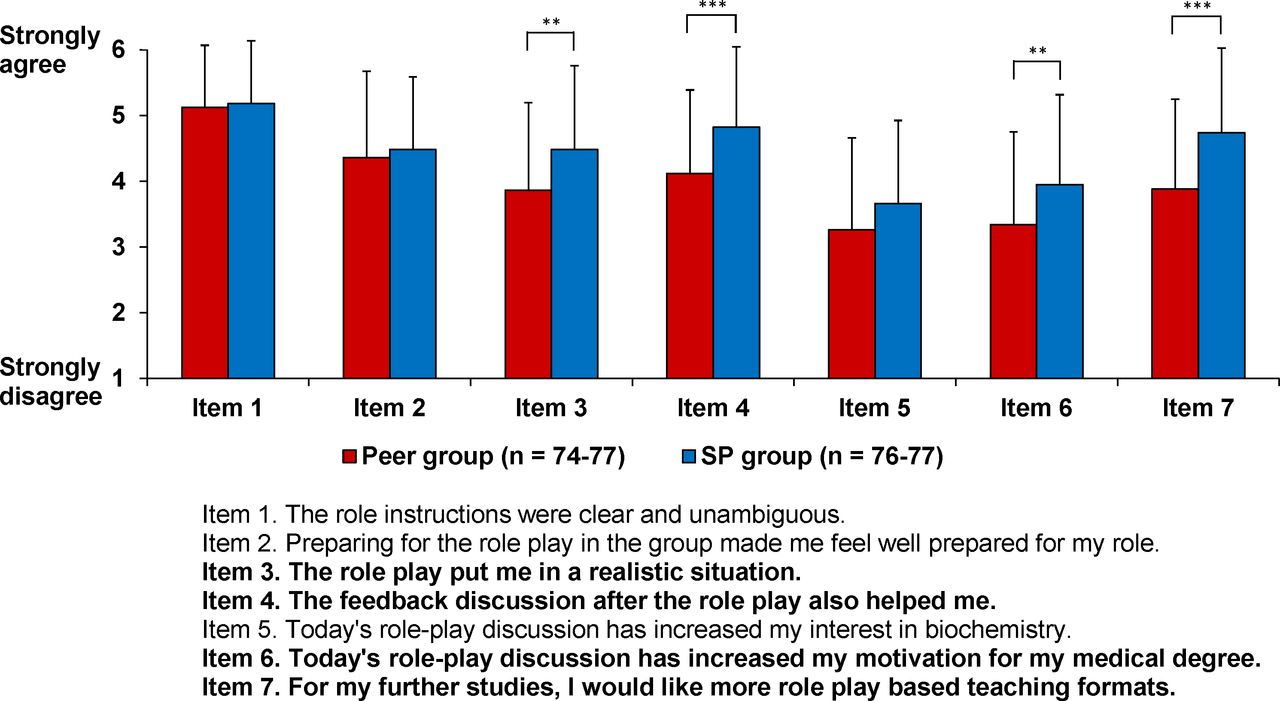
Students in the two groups differed in their evaluation of the role play. The SP group agreed significantly more strongly than the peer group with the statements that the role play represented a realistic situation (item 3, p=0.002, d=0.48), the feedback discussion was helpful (item 4, p<0.001, d=0.56), the role play motivated them in their medical degree (item 6, p=0.008, d=0.44), and they would like to have more role play-based teaching formats in their further studies (item 7, p<0.001, d=0.65) (see figure 5).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Mean (SD) values of the self-evaluation by medical students of a role play exercise on physician-parent communication. Comparison between students in the role play with a peer in the role of the parent (peer group) and those in the role play with a standardized patient, i.e. a trained actor, in the role of the parent (SP group).Students rated the seven items on a six-point Likert-type scale ranging from 1 (strongly disagree) to 6 (strongly agree). Abbreviations: SP = standardised patient; ** p<0.01, *** p<0.001.
In the overall assessment of the role play, students in the SP group rated the role play significantly better (mean (SD)=5.16 (0.83)) than the peer group did (mean (SD) 4.75 (0.80); p=0.001, d=0.50).
Learning success in biochemistry MC exam
To determine whether the acquisition of biochemistry knowledge differed between the students who had worked with a peer in the role of the parent and those who had worked with an SP in that role, we evaluated the results of a summative biochemistry examination held at the end of the semester. Students in both groups achieved a mean of 16.0 from 20 possible points (peer group: n=78, SD=2.86; SP group: n=72, SD=2.96).
Discussion
Our study showed that preclinical students benefit from and value communication training within a competency-based inverted biochemistry classroom, regardless of whether the role play uses peers or SPs. However, both forms hold specific benefits.
Students’ self-appraisal of their competency development: CanMEDS roles
Like other researchers showed before with other measurements,25 our communication training, whether performed with a peer or an SP, had a significant effect on students’ self-appraisals of their competencies in the CanMEDS roles (figure 2, online supplemental file 1). We observed the greatest gain in the roles ‘Scholar’, ‘Medical Expert’, ‘Professional’, and ‘Communicator’, all of which were most closely associated with the focus of the role play, that is, explaining the complex biochemical background of a disease in a way that a medical layperson can understand. These results indicate that our competency-based inverted biochemistry classroom approach was successful.
Differences between groups’ self-appraisals
Although role plays with peers or SPs are valuable tools for communication training, each has its own specific advantages. To make the role plays more realistic, we used actors as SPs in the role of the parent, which has been done elsewhere.21 26 In the SP group, we found a greater increase in student self-appraisals of competency in the CanMEDS roles ‘Scholar’ and ‘Professional’ (figure 3). One possible explanation could be that having an amateur actor (an SP) as the counterpart adds more seriousness to the situation/role play. Some studies showed disadvantages in this respect when using peers to play the role of patients,27 28 and in our study students rated the role plays with SPs as being more realistic (figure 5). When faced with SPs, students may try harder to phrase the complex biochemistry background in an understandable way and therefore better understand the crucial aspects of the role play exercise. Another explanation might be seen in the professional feedback provided by the SPs, which might help students to identify the importance of how they explain issues.29 The SPs in our study contributed to the feedback discussion because feedback is typically considered as a core part of communication skills training.20 21
Positive aspects of role plays with Peers
Role plays with peers have their advantages.15 25 30 First, they are more cost efficient than using SPs.12 Lim and colleagues found that when students assumed the layperson’s role, it helped them to understand how the patient would think and react.30 Lane et al15 supported this finding when they showed that role play with peers is as effective for training communication skills as role play with SPs, as assessed by a behaviour change counselling index. Bosse and colleagues25 reported that their peer role play group scored higher in the domain ‘understanding the parent’s perspective’. Our results are in line with these observations: students who took the role of a parent showed a greater increase in their self-appraisal of the role ‘medical expert’ than students who took the role of physician or observer (figure 4). On the descriptive level, other roles (except ‘scholar’ and ‘manager’) showed the same pattern, although the differences were not significant. Nevertheless, using SPs usually means that students cannot take on the role of patient (or, in our case, the parent), which might reduce the potential for additional learning. Moreover, other instruction formats also allow students to take the patient’s perspective, for example, student exercises in which they perform physical examinations on each other. On the basis of our results, we are considering asking students in future biochemistry seminars to discuss the clinical case with their friends and relatives during the self-learning phase, that is, before the role play, to give them greater insight into a patient’s perspective in medical consultations.
Students’ evaluations of the peer and SP role play
In our sample, students in the SP group agreed significantly more strongly than those in the peer group with the statement that the role play put them in a realistic situation (figure 5). This finding might indicate that students in the SP group took the role play more seriously or became more involved in the role play. Earlier studies found that students lacked seriousness in peer role plays.27 28 More seriousness in role plays with SPs could also explain why students in the SP group showed a larger increase in their self-appraisals of the roles ‘scholar’ and ‘professional’ (figure 3), as mentioned above. Further research is needed to clarify this hypothesis. The SP group also agreed to a greater extent that the feedback helped them (figure 5). The feedback from the SPs might have been more elaborate than that from the peers because our SP training programme trains SPs to give feedback. Studies have demonstrated the crucial role of feedback.29 31 32 Furthermore, the external perspective of an independent person without a medical background helps students to learn about the necessary depth and details of a medical consultation.
Another advantage of using SPs in role plays can be seen in students’ statements about their motivation, which increased more in the SP group (figure 5). Also, students’ desire for the future use of role plays in their further studies indicates the benefit of these activities. The overall assessment of the role play was good in both groups, but the SP group rated their role play significantly higher than the peer group did.
Learning success in written MC exam
We found no difference between the peer groups and SP groups in their grades on the MC examination. The summative examination asked about factual knowledge, and unfortunately we did not assess communication skills with objective measurements (eg, structured oral examinations); doing so may have identified specific advantages for the communication training with peers or SPs. Previous research found some advantages for the peer role play,25 30 and we are working on an assessment tool for future studies.
Limitations and strengths
We found some differences in sociodemographic data between the two role play groups, in that students in the peer group were significantly younger than those in the SP group. Also, we found non-significant differences between the two groups in former education, which was probably related to the difference in age. The fact that baseline self-appraisal scores were similar in the two groups indicates that the students in the SP group did not have more experience, relevant knowledge or skills. Self-appraisals can be prone to diverse biases and are not a substitute for objective measurements.33 34 Nevertheless, our results are in line with other research in communication training (eg, Bosse et al25). We think that, although our findings on the absolute levels of skills and learning gains may not be generalisable, the relative increases can be considered to be more accurate. To address this issue, we advise using objective measurements whenever possible (eg, objective structured clinical examinations), even though they can be costly. In this context, it is noteworthy that the current standard biochemistry examination based on MC questions did not directly assess the communication skill development targeted by the role play activities and that results might be more attributable to individual learning than to the teaching intervention.35 Another limitation can be seen in our use of the CanMEDS role framework in general and for communication skills in detail. The CanMEDS roles were primarily designed to depict the professional development of physicians throughout their professional lives and therefore can only be partially transferred to our seminar. The concept of the CanMEDS roles was also new to the students. Moreover, further research is needed to determine whether and, if so, how the students benefited from their self-perceived improvement in communication competencies. Another limitation of the study is that groups using trained SPs had higher self-rating regarding the CanMEDS roles (figure 4) and general points (figure 5) due to a potential stronger emersion in the role play, for example, by perceiving a greater challenge.
Despite these limitations, our data are supported by the face validity of our findings. For example, the students reported a large increase in the roles ‘scholar’ and ‘medical expert’, which were explicitly trained in the role playing exercise. Although the absolute values of the self-ratings should be interpreted with caution, the CanMEDS might be a valuable tool to identify beneficial effects of learning interventions in general. In this context, the results of the self-ratings support the hypothesis that training communication skills at an early stage of a medical curriculum benefits from the involvement of SPs because the SP group of students reported a significant increase in learning gain for the roles ‘scholar’ and ‘rofessional’.
Conclusions
We showed that using both peers and SPs, that is, trained actors, in role playing exercises is suitable for improving students’ self-perceived competency in CanMEDS roles in a preclinical biochemistry seminar. Nevertheless, the use of SPs has some advantages, such as representing a more perceived realistic training scenario. Further studies need to validate our results, for example, by implementing an objective structured clinical examination or a 360° perspective on the training by adding standardised encounter cards.36
Data availability statement
Data are available upon reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information. The datasets generated and analysed during the current study are not publicly available due to large amount but are available from the corresponding author on reasonable request. All data relevant to the study are included in the article.
Ethics statements
Patient consent for publication
Ethics approval
The ethics committee of Ulm University confirmed that no approval was required for this study. We confirm that we obtained written informed consent from all study participants. Our teaching approach was in accordance with international (eg, Canadian Medical Education Directives for Specialists (CanMEDS)) and national frameworks (eg, the German Masterplan Medizinstudium 2020). The participants were asked to give written informed consent prior to participation. All students and SPs in the images consented to publication of the images. Participants gave informed consent to participate in the study before taking part.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
AS and DACM are joint first authors.
Contributors SJK, AS, AH and DM designed the study and prepared and evaluated questionnaires. SJK, MK, VK and AH wrote the role scripts for the SPs. VK, SJK and AH trained the SPs. SJK taught during the on-site phases of the study. AS and DM performed the statistical analyses with diagrams. SJK, AS, DM, CN, MK, AH and TJB discussed and interpreted the results. SJK and AS wrote the first draft of the manuscript. All authors commented on the first draft and subsequent versions of the manuscript and approved the final manuscript. SJK is responsible for the overall content as the guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.