Article Text

Abstract
Objective Adverse health effects of fine particles (particulate matter2.5) have been well documented by a series of studies. However, evidences on the impacts of black carbon (BC) or elemental carbon (EC) on health are limited. The objectives were (1) to explored the effects of BC and EC on cardiovascular and respiratory morbidity and mortality, and (2) to verified the reliability of the meta-analysis by drawing p value plots.
Design The systematic review and meta-analysis using adapted Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach and p value plots approach.
Data sources PubMed, Embase and Web of Science were searched from inception to 19 July 2021.
Eligibility criteria for selecting studies Time series, case cross-over and cohort studies that evaluated the associations between BC/EC on cardiovascular or respiratory morbidity or mortality were included.
Data extraction and synthesis Two reviewers independently selected studies, extracted data and assessed risk of bias. Outcomes were analysed via a random effects model and reported as relative risk (RR) with 95% CI. The certainty of evidences was assessed by adapted GRADE. The reliabilities of meta-analyses were analysed by p value plots.
Results Seventy studies met our inclusion criteria. (1) Short-term exposure to BC/EC was associated with 1.6% (95% CI 0.4% to 2.8%) increase in cardiovascular diseases per 1 µg/m3 in the elderly; (2) Long-term exposure to BC/EC was associated with 6.8% (95% CI 0.4% to 13.5%) increase in cardiovascular diseases and (3) The p value plot indicated that the association between BC/EC and respiratory diseases was consistent with randomness.
Conclusions Both short-term and long-term exposures to BC/EC were related with cardiovascular diseases. However, the impact of BC/EC on respiratory diseases did not present consistent evidence and further investigations are required.
PROSPERO registration number CRD42020186244.
- public health
- respiratory medicine (see thoracic medicine)
- cardiology
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
Adapted Grading of Recommendations assessment, Development and Evaluation, formulated by the WHO global air quality guidelines working group, was used to evaluate the certainty of evidence.
This study incorporated a detailed search strategy, explicit literature screening and risk of bias assessment.
The p value plots were used to evaluate the reliabilities of meta-analyses.
Limitation on searching grey literature should be noted.
Background
Black carbon (BC), a ubiquitous component of air particulate matter (PM), is usually measured through optical absorption.1 Elemental carbon (EC), another carbonaceous material with a graphitic structure, is commonly measured by thermal or thermo-optical method.1 2 Although the measurement methods are different, BC and EC are often considered interchangeable. BC is mainly emitted from traffic and combustion-related sources and is a measured component of the PM. The adverse health effects of PM, especially PM2.5, are well documented. In 2017, a total of 2.94 million deaths resulted from ambient PM worldwide.3–5 PM2.5 is composed of various constituents, in which some of them are more toxic and hypothesised as the main cause of the adverse effects of PM2.5. A growing body of studies indicates a potential role of BC among these more toxic constituents.6 7 In addition, some reviews demonstrated that BC is a better indicator of adverse effects of PM from combustion sources according to robust associations from epidemiological studies.8 9 The underlying pathological mechanisms of BC include oxidative stress, inflammation and gene mutations.10–12
Due to its association with adverse health, the number of studies exploring the effects of BC on cardiorespiratory diseases has rapidly increased in recent years. Cardiovascular and respiratory diseases are common diseases worldwide, with a heavy disease burden and major implications for clinical practice and public health. The global burden of disease study 2017 indicated that cardiovascular and respiratory-related death ranked first and third respectively among non-communicable diseases.4 Health effects of acute and chronic exposure to BC have been widely reported. Despite that there is some epidemiological evidence that BC was associated with cardiorespiratory diseases, in other studies, no statistically effects were observed.
The reliability of air quality epidemiological studies is often poor, with a serious lack of reproducibility of published findings.13
A lack of reproducibility in epidemiological studies can be attributed to many factors, but p-hacking is a common issue. If researchers run a regression with and without outliers, with and without a covariate, with one and then another dependent variable, then false positive results are much more likely to be reported. There can be a selective reporting problem (compute many tests and selectively report small p values), which is referred to p-hacking.14 When a study examines many questions, tests numerous statistical models and does not perform multiple testing statistical corrections, p hacking is referred to as multiple testing and multiple modelling.15 16 Since the uncorrected statistical estimates are likely not unbiased, the results of meta-analysis may unreliable. Therefore, it is essential to exploring the p values in a meta-analysis.
Some systematic reviews analysed the impact of BC on health. Nevertheless, quantitative associations between BC exposure and cardiovascular and respiratory diseases have not been well-characterised due to different objectives of the reviews.17 18 A series of eligible studies published recently have not been considered. In addition, the GRADE (Grading of Recommendations assessment, Development and Evaluation) framework was not adopted in previous systematic reviews. Compared with Yang et al,19 this study included recently published eligible studies. Furthermore, meta-analysis of BC effects on vulnerable populations and geographical regions were conducted. Moreover, based on a p value plot, the reliability of meta-analysis was examined. Therefore, a systematic review and meta-analysis was performed to further elucidate the health effects of BC/EC in this study. The objectives were (1) to investigate the association of short-term and long-term exposure to BC/EC with the respiratory and cardiovascular morbidity and mortality; and (2) to verify the reliability of the meta-analysis using p value plots.
Methods
Patient and public involvement
Patients or the public were not involved in this study.
Database
PubMed, Web of Science and Embase databases were systematically searched using the following terms: (black carbon* or elemental carbon*) AND (respiratory* or cardiovascular*) AND (morbidit* or hospitalization* or death* or mortalit* or outpatien*) AND (time series* or case cross* or cohort*)". We limited our search to studies from inception to 19 July 2021. In addition, the reference lists of the included studies and related reviews were manually evaluated to identify additional relevant studies. The details of the search strategy in PubMed were shown in online supplemental table S1.
Supplemental material
Inclusion and exclusion criteria
A time series study, case cross-over study or cohort study that evaluated the impact of BC/EC on cardiovascular or respiratory diseases was included in this systematic review and meta-analysis. Studies were considered eligible for inclusion if they fulfilled the inclusion criteria as follows: (1) study types restricted to time series, case cross-over or cohort studies; (2) studies considering BC/EC as air pollutants; (3) based on the International Classification of Diseases (ICD) 9th or 10th revision, diseases included respiratory diseases, wheeze, other respiratory distress insufficiency or respiratory cancer (ICD9 codes 460–519, 786.07, 786.09 or 162; ICD-10 codes J00–J99, R06.251, R06.001 or C34) or cardiovascular diseases (ICD9 codes 390–459, ICD-10 codes I00–I99); (4) studies considering morbidity or mortality as outcome; (5) estimates were OR, relative risk (RR) or HR with 95% CI or enough information for their calculation and (6) publication language was restricted to English.
The exclusion criteria were as follows: (1) studies on soot or black smoke were excluded, because the definition of such components usually lacked precision; (2) studies assessing the disease progression exposure to pollutants in individuals with cardiovascular or respiratory diseases (eg, chronic obstructive pulmonary disease (COPD) and asthma); (3) studies focusing on particular populations (eg, pregnant women and miners) or population living in specific environments with high pollution concentration (eg, residential area near industrial complexes, population exposed to sugar cane burning and neighbourhoods that expose many streets); (4) studies focusing on seasonality; (5) conference abstracts and (6) study period less than 1 year.
Selection of articles and extraction of data
To identify eligible studies, two investigators independently screened titles and abstracts. Studies whose relevance could not be determined by titles and abstracts were subjected to full text screening. Any disagreement was resolved by discussion. A third investigator was involved in the discussion when a consensus could not be reached.
Two reviewers independently extracted the following items from each included study. Study characteristics were extracted using a standardised form that included but was not limited to the following items: first author, publication year, country, study design, diagnosis standard, time period, population age, statistical models, air pollutants, outcomes and number of events. If the reported data of the included studies were unclear or missing, the first author or corresponding author was contacted by e-mail. Any conflicts were resolved by the involvement of a third investigator if the controversy was not solved after the discussion.
Data synthesis
Regarding the meta-analysis, the RR was used as an effect estimate, and the OR in case cross-over study and HR in cohort study were considered equivalent to RR. Estimates from the maximally adjusted model in the cohort study were extracted when multiple estimates were present in the original study to reduce the risk of potential unmeasured confounding.20 In addition, the estimate was converted to a standardised increment (1 µg/m3) of RR. The following formula was used to calculate standardised risk estimates:

Two studies did not show the overall risk, while stratified risk estimates by age and location were reported.21 22 In this case, the stratified estimates were pooled. One study presented the estimates of both morbidity and mortality, which were combined in the overall analysis.23 In addition, if the same cohort data were analysed in different studies and the latest study was included.24–26
Risk of bias assessment
The risk of bias was assessed for each study according to the Office of Health Assessment and Translation tool and the Navigation Guide tool.17 27 28 Risk of bias evaluation was conducted as follows: exposure assessment, outcome assessment, confounding bias, selection bias, incomplete outcome data, selective reporting, conflict of interest and other bias. Each domain was considered as ‘low’, ‘probably low’, ‘probably high’, ‘high’ or ‘not applicable’ criteria. Two investigators conducted the risk of bias evaluation. Any inconsistency between the investigators was discussed and a third researcher was involved to resolve any disagreement.
Evaluation of certainty of evidence
An adaptation of the GRADE framework, formulated by the WHO global air quality guidelines working group, was used to evaluate the certainty of evidence.29 The rating process on the certainty of evidence started at moderate. The certainty was graded into four levels: ‘high’, ‘moderate’, ‘low’ and ‘very low’. Five reasons were used to downgrade the certainty of evidence: limitations in studies, indirectness, inconsistency, imprecision, and publication bias; three reasons were used to upgrade: large magnitude of effect size, all plausible confounding shifts the RR towards the null and concentration-response gradient. To evaluate the magnitude of the effect size, the E-value was calculated using the following formula:

Statistical analysis
Statistical analysis was performed using STATA (V.12.0, Stata Corp). In this meta-analysis, the random-effects model was conducted for anticipating significant heterogeneity among studies. Heterogeneity among trials was assessed by the χ2 test and the extent of inconsistency was evaluated by the I.2 An 80% prediction interval (PI) of meta-estimate was calculated to assess the inconsistency. To assess potential sources of heterogeneity, subgroup analyses were performed on outcomes (morbidity and mortality), single lag days (0, 1 and 2 days), study areas (Europe, America and Asia) and seasons (warm and cold). The estimates from BC and EC were combined, since both of them are indicators of carbon-rich combustion sources, and are usually considered interchangeable in medical research.
Estimates were pooled separately where more than three estimates were available. Most studies presented estimates for single lags and the estimate of shortest lag was used to combine the estimates (RRs) of shortest lag in meta-analysis. However, only a few studies presented cumulative lags, and the estimates of shortest cumulative lags were used in the meta-analysis. In addition, Mostofsky et al indicated that PM2.5 is a potential confounder in assessing the health effects of PM2.5 constituents.7 For overall and outcome analysis, PM2.5-adjusted estimates and PM2.5-unadjusted estimates in the models were combined, respectively where more than three estimates were available. Regarding the subgroup analysis, PM2.5-unadjusted estimates were analysed, while PM2.5-adjusted estimates were not presented due to the limited number of included studies. Moreover, primary data of the included studies could not be obtained, hence it was impossible to evaluate whether the same patients were repeatedly included across multiple studies. Therefore, the sensitivity analysis was performed on all age populations to investigate the robustness of the aggregation results by the removal of studies with partial temporal overlap from the same geographical location. Most of the included studies analysed and presented results of cardiovascular or respiratory diseases, hence systematic diseases were analysed in the acute effect analysis, except for the chronic effect analysis. Publication bias was assessed by Egger’s regression test when the outcome included more than 10 studies. Trim and fill method was used to correct on asymmetry for the outcome with publication bias. A p<0.05 was considered statistically significant.
Non-traditional methods were used to assess the reliability of basic studies, which is different from mainstream environmental epidemiology. Studies with large analysis search spaces suggest the use of a large number of statistical models and statistical tests for an effect, thereby allowing greater flexibility of researchers to selectively search through and only report results showing positive effects. Fifteen studies included in the meta-analysis were randomly selected. The number of outcomes, predictors and covariates were counted. We computed the search spaces as follows: Space1 is outcome times predictor times lags. Space2 is 2covariate. Space3 is Space1 times Space2. Space3 is the total analysis search space. Search spaces were computed by the method introduced in Young and Kindzierski.30
The p value plot was used to inspect the distribution condition of the p values.31 Regardless of sample size, the p value is distributed uniformly between 0 to 1 under the null hypothesis. If the shape of p value plot is a straight line and follows an approximate 45° line, then the p values are consistent with a distribution of true null hypothesis; the p values are assumed to be random.31 If the shape is approximately a hockey stick, the p values on the blade are not consistent with chance, whereas those on the arm are consistent with chance, the results are ambiguous. Therefore, p value plot was used to assess the validity and reliability of included studies.
P values of included studies were computed using RR, low CI and high CI. Then, the p values were ranked from smallest to largest using 1, 2, 3… and the plots were constructed. The following formulas were used to calculate p value:



Results
A total of 1694 studies were initially identified and 129 were reviewed in depth. We excluded the studies which study period less than 1 year or same data were analysed in different studies.32 33 Of these, 70 fulfilled the inclusion criteria (figure 1).7 21–26 34–96 Of the 70 included studies, 56 estimated the short-term effects of BC/EC using a time series design or case cross-over design, while 14 studies explored the long-term effects of BC/EC using a cohort design. Thirty-seven of the 70 studies reported morbidity as the outcome variable, 25 studies reported mortality and 8 studies reported both morbidity and mortality. Thirty-five studies analysed both cardiovascular and respiratory diseases, 18 studies merely investigated cardiovascular diseases, and 17 studies assessed respiratory diseases. Thirty-seven studies were conducted in the USA, 14 in China, 4 in Canada, 2 in the UK, Sweden, Korea and Serbia, 1 in Denmark, Iran, Germany and the Netherlands. The remaining three studies collected data from two different countries: Spain and Greece, Spain and Italy, Sweden and Denmark. Twenty-seven studies classified the diseases using the ICD-9 codes, 26 used the ICD-10 codes, and 10 used both the ICD-9 and ICD-10 codes. However, the remaining seven studies did not employ the ICD standards (online supplemental table S2). In addition, the authors of 33 studies were contacted, but only 19 answered our request (response rate: 57.6%).

Flow diagram of hliterature screening process.
Short-term effect of BC/EC on cardiovascular and respiratory diseases
Overall, short-term exposure to BC/EC was associated with an increased risk of cardiovascular diseases (RR 1.007 per 1 µg/m3, 95% CI 1.002 to 1.011) (adjusted by trim and fill method) in overall analyses (table 1 and figure 2). Cardiovascular diseases (RR 1.016 per 1 µg/m3, 95% CI 1.004 to 1.028) were associated with BC/EC in the elderly (65+ years) (figure 2).

Impact of short-term exposure to BC/EC on cardiovascular diseases in the PM2.5-unadjusted model. BC/EC, black carbon/elemental carbon; PM, particulate matter.
Short-term impacts of BC/EC on cardiovascular and respiratory diseases in different models
Impact of BC/EC on cardiovascular diseases was related to the exposure lag. The estimates of the association were strongest on the day of the event (lag 0) (RR 1.011 per 1 µg/m3, 95% CI 1.006 to 1.016), and then diminished on lag 1 (RR 1.005 per 1 µg/m3, 95% CI 1.002 to 1.008) and lag 2 (RR 1.002 per 1 µg/m3, 95% CI 0.999 to 1.005) (online supplemental table S3). Subgroup analyses on geographical location was performed for morbidity and mortality, respectively. Significant association between BC/EC and cardiovascular mortality was observed in Asia (RR 1.003, 95% CI 1.001 to 1.005). However, no association was found in America (RR 1.017, 95% CI 0.998 to 1.037) and Europe (RR 0.990, 95% CI 0.979 to 1.001) (online supplemental figure S1). On the other hand, an increased risk of cardiovascular morbidity was observed in America (RR 1.022, 95% CI 1.016 to 1.029) with short-term exposure to BC/EC, while only one study performed in Europe (RR 1.026, 95% CI 1.006 to 1.047) investigated the short-term effect of BC/EC on cardiovascular morbidity.23 In addition, just one study in Asia performed the short-term effects of BC/EC on stroke morbidity (online supplemental figure S2).66
No association was observed between short-term exposure of BC/EC and respiratory morbidity (RR 1.012, 95% CI 0.993 to 1.031) and mortality (RR 1.013, 95% CI 0.997 to 1.030) (table 1).
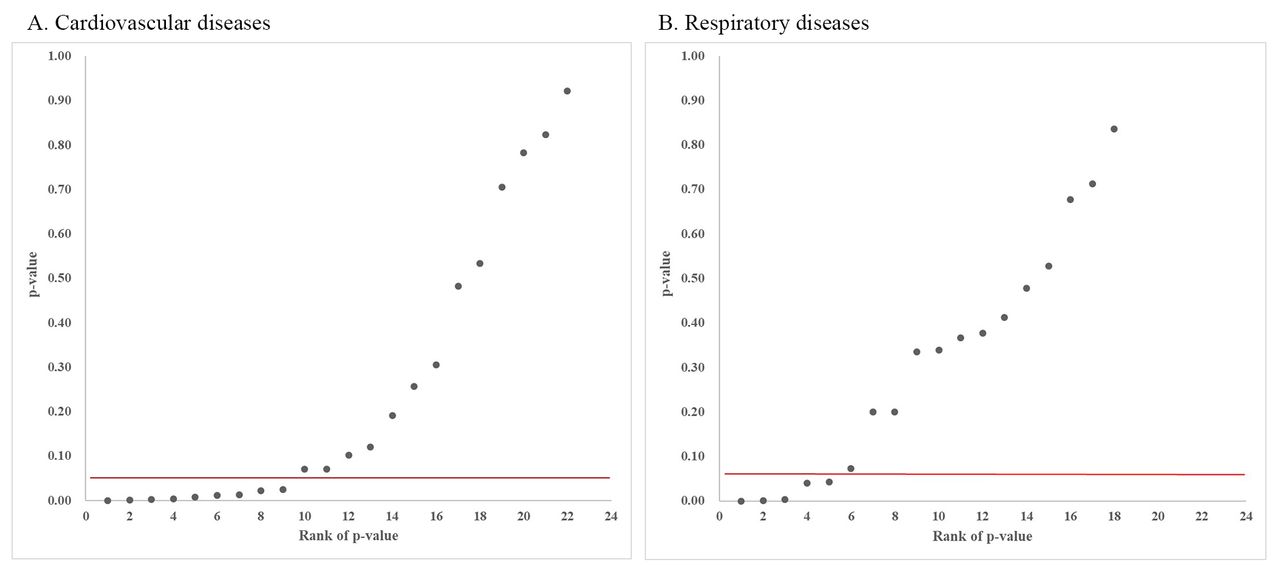
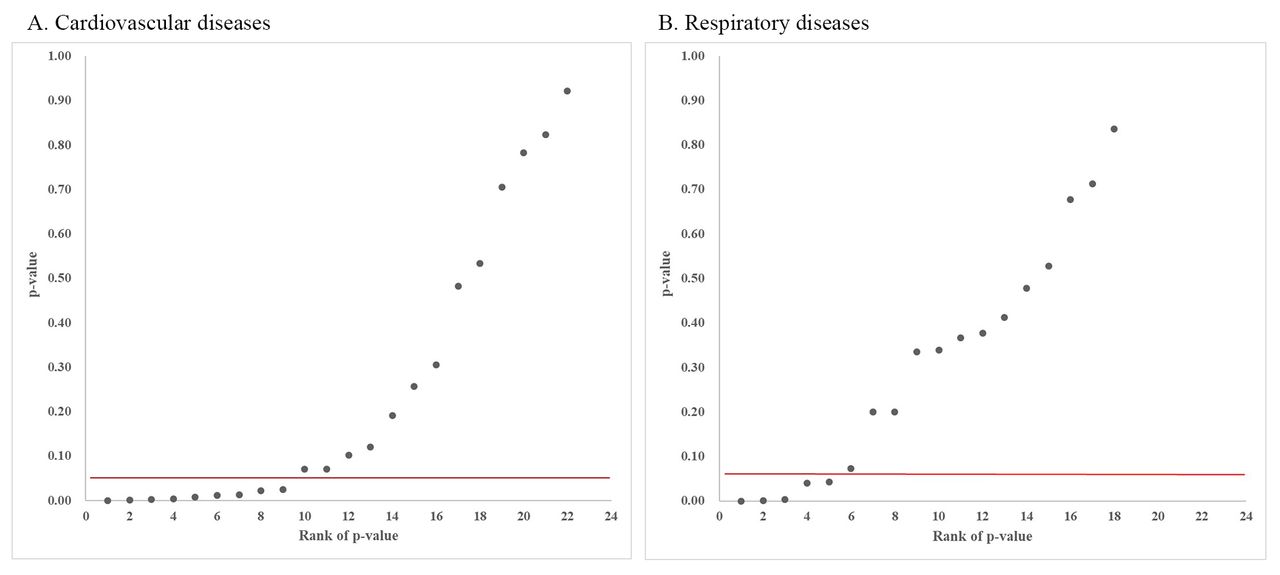
P value plots of short-term exposure to BC/EC on cardiovascular and respiratory diseases in the PM2.5-unadjusted model
We chose at random 15 studies included in the meta-analysis. Then, we extracted analysis items (outcomes, predictors, covariates, and lags) and calculated the search spaces. Table 2 lists the counts of outcomes, predictors, covariates and lags for the 15 studies. There were many thousands of possible analysis options in each of the randomly selected studies and summary statistics of the numbers of options are given in online supplemental table S4. Across the studies, the median number of possible analyses was 12 000 (IQR 2688–15 360) for Space3, which took all the factors into account.
Variable counts and analysis search spaces for the 15 studies chosen from the meta-analysis
In figure 3, the plot of cardiovascular studies showed a shape of hockey stick. There were 9 p values less than 0.05 and 13 larger than 0.05 (online supplemental table S5). The smallest p value in cardiovascular group was 0.000087 and the largest was 0.921904, which was of a wide range. The association between BC and cardiovascular diseases were consistent with a mixture based on p values and p value plot. We did not find a consistent effect so there is no proof of a causal effect. The shape of the plot on the impact of BC on respiratory diseases was close to 45° line. Four calculated p values were less than 0.05, while 14 were larger than 0.05 and fell on an approximate 45° line (online supplemental table S5). In addition, the smallest p value was 3.2036×10−45 and the largest was 0.836403. The smallest p value was so small that p hacking (or even data fabrication) may exist. As the p value plot’s shape approached a 45°, the impact of short-term exposure to BC/EC on respiratory diseases was likely to be random.
{kind=link}
{kind=link}
{kind=link}
P value plots of short-term exposure to BC/EC on cardiovascular diseases (A) and respiratory diseases (B) in the PM2.5-unadjusted model. BC/EC, black carbon/elemental carbon; PM, particulate matter.
Long-term impact of BC/EC on cardiovascular and respiratory diseases
Five studies assessed the long-term exposure to BC/EC and cardiovascular diseases, and a positive association was observed (RR 1.068, 95% CI 1.004 to 1.135) (online supplemental figure S3). Three studies assessed the long-term exposure to BC/EC and ischaemic heart disease (IHD), and a positive association was observed (RR 1.066, 95% CI 1.009 to 1.127). On the other hand, four studies assessed the long-term exposure to BC/EC and respiratory mortality. Meta-analysis was not performed due to limited included studies and no association was observed among the include studies.25 60 68 75 However, one study analysed COPD. It indicated that long-term exposure to BC/EC was associated with an increased risk of COPD morbidity (RR 1.060, 95% CI 1.020 to 1.100), while no impact was observed for COPD mortality (RR 1.070, 95% CI 1.000 to 1.140).24
Results from the PM2.5-adjusted model
In the PM2.5-adjusted model, six studies were included in the meta-analysis of short-term exposure to BC/EC and cardiovascular diseases (RR 1.014 per 1 µg/m3, 95% CI 1.001 to 1.027) (online supplemental figure S4). The meta-analysis indicated that the association was robust compared with the results of the PM2.5-unadjusted model. In addition, the impact of BC/EC on cardiovascular morbidity in the PM2.5-adjusted model (RR 1.018 per 1 µg/m3, 95% CI 1.006 to 1.031) was consistent with the results in the PM2.5-unadjusted model (RR 1.022 per 1 µg/m3, 95% CI 1.016 to 1.029). However, an increased risk was found between BC/EC and cardiovascular mortality in the PM2.5-unadjusted model (RR 1.003 per 1 µg/m3, 95% CI 1.001 to 1.006), while no association was observed in the PM2.5-adjusted model (RR 1.006 per 1 µg/m3, 95% CI 0.993 to 1.019) (table 1).
Sensitive analysis
In the sensitive analysis, similar results were observed from the overall analysis of all age populations. Increased risk of cardiovascular diseases after exposure to BC/EC was found (RR 1.006 per 1 µg/m3, 95% CI 1.002 to 1.010) by eliminating studies with partial overlap from the same geographical location.21 23 38 80 In addition, no statistical significance was observed (RR 1.008 per 1 µg/m3, 95% CI 0.992 to 1.023) between respiratory diseases and BC/EC after eliminating overlapped studies (table 1).21 23 88 94
Risk of bias and certainty of evidence
The risk of bias assessment of the included studies is shown in online supplemental table S6 and more analytically in online supplemental table S7. In general, the majority of the included studies were rated as ‘low risk’ in the items of outcome assessment, selection bias, incomplete outcome data, conflict of interest and other bias. The confounding bias and selective reporting were mostly rated as ‘probably low’. However, seven studies were rated as ‘probably high’ risk because not all critical potential confounders were adjusted in the analysis.7 24 26 46 55 74 91 In addition, the majority of the included studies on the exposure assessment were assessed as ‘probably low’ and ‘probably high’, and in some cases studies were rated as ‘high’ risk. Three studies were rated as ‘high risk’ on exposure assessment mainly because pollutants were measured with a single monitoring over a large geographical area, and not measured at least daily.53 85 92
The certainty of evidence on the acute effects of BC/EC on cardiovascular diseases in the PM2.5-adjusted model was rated as ‘moderate’ and in the PM2.5-unadjusted model was rated as ‘low’. The evidence on the chronic effects of BC/EC on cardiovascular diseases was evaluated as ‘moderate’ certainty (online supplemental table S8).
Discussion
A comprehensive search of three electronic databases was performed using a well-defined search strategy. Finally, 70 studies assessing the short-term and long-term impacts of BC/EC on cardiovascular and respiratory morbidity and mortality were included. Using a random effects model, the pooled effect estimates indicated that the short-term exposure to BC/EC was associated with an increased risk of cardiovascular diseases, but not on respiratory diseases in all populations. BC/EC was associated with cardiovascular diseases in the elderly (65+ years). In addition, association between short-term exposure to BC/EC and cardiovascular diseases differ across continents.
Short-term exposure to BC/EC was related with cardiovascular diseases in the elderly
Overall, the meta-analysis results indicated that short-term exposure to BC/EC was associated with an increased risk of cardiovascular diseases, but not on respiratory diseases in all populations. In general, the PM2.5-adjusted model and the PM2.5-unadjusted model and sensitivity analysis showed that the associations were consistent. In contrast to the meta-analysis calculations, p value plots indicated mixed results for cardiovascular. Some studies indicated an effect while others appeared to be random. For respiratory effects, the p value plot was consistent with randomness, no effect. Our counting results, table 2 and online supplemental table S4 indicates that small p values could be the result of multiple testing/multiple modelling.
However, the association between BC/EC and cardiovascular mortality should be further explored by further studies, which should pay more attention to the PM2.5-adjusted model. Subgroup analysis indicated that the effects of BC/EC on cardiovascular diseases were the most significant on the current day and the impacts were decreased with lag days. In addition, the association between BC/EC and cardiovascular mortality in the cold season was stronger than that in the warm season. A potential reason could be that the concentration of BC/EC in the cold season was higher than that in the warm season.97–99 Subgroup analysis on pollutant (BC and EC) indicated that the results from the PM2.5-unadjusted model and PM2.5-adjusted model were not consistent. Furthermore, the sensitivity analysis on omitting a single study showed that the results were not robust (data not shown). An essential reason could be that BC and EC were considered interchangeable. Three included studies simultaneously assessed the effects of BC/EC on cardiovascular diseases.22 63 93 However, in the PM2.5-adjusted model, no statistically significant difference was observed between EC (RR 1.039, 95% CI 0.993 to 1.083) and cardiovascular morbidity. In addition, Samoli et al illustrated that the impact of BC/EC on cardiovascular morbidity differed in the elderly and other age groups, while Atkinson et al indicated no statistically significant difference between BC/EC and cardiovascular mortality in both the PM2.5-adjusted model and PM2.5-unadjusted model.22 85 On the other hand, increased risk of long-term exposure to BC/EC and cardiovascular diseases was observed. However, in this meta-analysis, due to the limited number of included studies, only short-term exposure to asthma morbidity was evaluated. In addition, a subgroup analysis on the chronic effects of BC/EC on cardiovascular and respiratory diseases was not performed because of the limited number of included studies.
The overall quality of acute effects of BC/EC on cardiovascular diseases in all populations in the PM2.5-unadjusted model was evaluated as ‘moderate’. We downgraded one level for publication bias, hence the estimate was adjusted using the trim and fill method.29 In addition, inconsistency was not downgraded because 80% PI does not included unity, or it included unity but less than twice the 95% CI.
Vulnerable populations
This meta-analysis revealed that BC/EC may have acute effects on cardiovascular diseases in the elderly.100 In addition, lung function and mucociliary clearance decline with long-term exposure to pollutants and increasing age.5 101 These factors might contribute to making the elderly more vulnerable to BC. On the other hand, this meta-analysis indicated that an increased risk was observed between BC/EC and asthma morbidity in children of 0–18 years. Asthma, a chronic airway disorder, is a serious health disease and previous studies indicated that children have higher PM2.5 deposition rather than the adults, and BC is an essential constituent of PM2.5.102
Underlying pathological mechanism
In our study, the pooled effect estimate indicated that short-term and long-term exposure to BC/EC was associated with an increased risk of cardiovascular diseases. There are considerable speculative literatures on possible underlying mechanisms. An animal study conducted by Niwa et al revealed that BC accelerated atherosclerotic plaque formation.103 Furthermore, a human panel study was performed to assess whether the patients with IHD experience change in the repolarisation parameters exposure to rising concentration of pollutants.104 The results indicated that the variability of the T-wave complexity increased with increasing EC during periods of 0–5 hours, 12–17 hours and 0–2 hours before ECG measurement.104 On the other hand, a p value plot analysis did not support a consistent effect of BC/EC on cardiovascular disease. The original meta-analysis examined heart attacks and claim effects for PM10 and PM2.5, which performed by Mustafic et al.105 A critique was given in Stanley Young and Kindzierski who used p value plots to call those claims into question.30
Suggestions for further research
First, critical potential confounders (temperature, seasonality, day of the week and long-term trends) and other potential confounders (holidays and influenza epidemics) should be considered in time series and case cross-over studies, especially for influenza epidemics. Influenza epidemics are factors usually neglected in short-term studies. Second, studies should adjust PM2.5 when assessing the health effect of PM2.5 constituents. Mostofsky et al showed that PM2.5 may be associated with both health and its constituents. Constituents having closer association with PM2.5 may illustrate a stronger association with diseases. Therefore, the results of PM2.5-unadjusted model could introduce bias.7 Third, further studies are suggested to evaluate the health effects of long-term exposure to BC, especially for morbidity. An essential difficulty that needs to be acknowledged is the availability of the disease data. Emergency department visits and outpatients are more time-sensitive data than mortality, hence these indicators are more representative to some extent in investigating the health effects of environmental factors. However, the data of emergency department visits and outpatients generally from medical institutions are more difficult to obtain than data on mortality, with a large portion of mortality data arriving from departments of disease control institutions in China. Forth, the present evidence on the health effects of BC was mainly from America and Asia. Studies assessing the association in other geographical locations are suggested, which might contribute to the evaluation of the potentially different effects of BC in different continents. Fifth, more studies need to provide evidence to prove the association between BC/EC and respiratory diseases in vulnerable populations.
Strength and limitation
This systematic review and meta-analysis provided a comprehensive and current evidence for the short-term and long-term exposure to BC/EC on cardiorespiratory morbidity and mortality. Adapted GRADE framework was used to assess the certainty of the evidence. Multiple testing/multiple modelling was not considered in current GRADE theory, which should be further explored in the future. Potential limitations in our study are as follows. A significant heterogeneity for the pooled estimates was noticed in the meta-analysis, which might be due to the high variability in the study population, outcomes, and geographical locations. Therefore, subgroup analyses on age of the population (all and older than 65 years old), outcomes (morbidity and mortality), geological locations (Europe, America and Asia) and lag days (0, 1, 2 days) were conducted for a further investigation of the potential sources in conditions more than three estimates. Most of the included papers used in our study were from the USA or China, which affected the pooled estimates, although it is an inherent and inevitable selection bias. We have extracted and calculated the regional distribution of BC concentration of included studies. It showed that the mean BC concentration is highest in Asia, which maybe an essential reason of the results. In addition, consistent results of cardiovascular and respiratory diseases exposure to BC/EC were observed by eliminating studies with partial overlap from the same geographical locations.
The reliability of meta-analysis is an essential challenge for environmental epidemiology research, which should be improved in the future. The reliability of meta-analysis was analysed by combining p value plots and heterogeneity. Our findings indicated that the impact of BC on cardiovascular diseases was more reliable. However, the impact of BC on respiratory diseases was random and some reported small p values may exist p hacking. It is not appropriate to do meta-analysis blindly when researchers do not understand the limitations in the basic studies. Therefore, it is essential for authors to understand the causes of limitations and draw objective conclusions.
Conclusions
Both short-term and long-term exposures to BC/EC were related with cardiovascular diseases. However, the impacts of BC/EC on respiratory diseases did not present consistent evidence and further investigations were required.
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information.
Ethics statements
Patient consent for publication
Acknowledgments
We would like to thank the authors of the original studies for their contributions to our systematic review and meta-analysis, especially authors who provided their raw data for the analysis. We are grateful to Professor S. Stanley Young and all reviewers for their helpful comments and suggestions on this manuscript. We would like to thank MogoEdit company for helping us in the language editing of our article.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors SW, XZ and XS developed the research design. XS, YH, YM and LJ analysed the data and interpreted the results. XS, YH, YM, XW and JZ drafted manuscript. AS, YuL, YaL, JT, XL and YG did literature screening and data extraction. All of the authors contributed to drafting the manuscript. The final manuscript was approved by all authors. XS is the guarantor and accepts full responsibility for the work.
Funding The work was supported by the National Key Research and Development Program of China (No.2016YFA0602004) and Innovation Fund Project on Public Meteorological Service Center of China Meteorological Administration in 2020 (Grant numbers: K2020010).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.