Article Text

Abstract
Introduction Shift workers are at an increased risk of developing obesity and type 2 diabetes. Eating and sleeping out of synchronisation with endogenous circadian rhythms causes weight gain, hyperglycaemia and insulin resistance. Interventions that promote weight loss and reduce the metabolic consequences of eating at night are needed for night shift workers. The aim of this study is to examine the effects of three weight loss strategies on weight loss and insulin resistance (HOMA-IR) in night shift workers.
Methods and analysis A multisite 18-month, three-arm randomised controlled trial comparing three weight loss strategies; continuous energy restriction; and two intermittent fasting strategies whereby participants will fast for 2 days per week (5:2); either during the day (5:2D) or during the night shift (5:2N). Participants will be randomised to a weight loss strategy for 24 weeks (weight loss phase) and followed up 12 months later (maintenance phase). The primary outcomes are weight loss and a change in HOMA-IR. Secondary outcomes include changes in glucose, insulin, blood lipids, body composition, waist circumference, physical activity and quality of life. Assessments will be conducted at baseline, 24 weeks (primary endpoint) and 18 months (12-month follow-up). The intervention will be delivered by research dietitians via a combination of face-to-face and telehealth consultations. Mixed-effect models will be used to identify changes in dependent outcomes (weight and HOMA-IR) with predictor variables of outcomes of group, time and group–time interaction, following an intention-to-treat approach.
Ethics and dissemination The study protocol was approved by Monash Health Human Research Ethics Committee (RES 19-0000-462A) and registered with Monash University Human Research Ethics Committee. Ethical approval has also been obtained from the University of South Australia (HREC ID: 202379) and Ambulance Victoria Research Committee (R19-037). Results from this trial will be disseminated via conference presentations, peer-reviewed journals and student theses.
Trial registration number Australian New Zealand Clinical Trials Registry (ACTRN-12619001035112).
- NUTRITION & DIETETICS
- SLEEP MEDICINE
- PUBLIC HEALTH
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
Best-practice approaches to weight loss fail to take into consideration the physiological mechanisms underlying weight gain in shift working populations.
Intermittent fasting offers a flexible approach to weight loss, where fasting days can be aligned with shift scheduling. However, the efficacy in populations that have a high incidence of obesity and unusual working schedules has not been tested.
A large variety of health outcomes will be assessed, including weight, cardiometabolic health and psychological health.
Postintervention interviews to understand the enablers and barriers to compliance.
A potential limitation of this study is the eligibility criteria of two night shifts a week restricting recruitment.
Introduction
By working at night, shift workers increase their odds of developing obesity and type 2 diabetes (T2DM) by 23% and 44%, respectively.1 2 These risks remain even after controlling for lifestyle and socioeconomic status.3 4 Shift work is typically defined as working outside of the hours of 6:00 to 18:00 and impacts approximately 20% of the employed population in industrialised countries.5 The higher risk of disease in shift working populations is likely a consequence of circadian misalignment caused by disruption to our circadian rhythms.6 This occurs when there is a mismatch between the circadian rhythms generated endogenously in the hypothalamus by the suprachiasmatic nucleus (SCN) and peripheral clocks located in the majority of body tissues. While light is the main entrainer (zeitgeber) of the SCN,7 lifestyle behaviours such as when we eat and sleep can influence peripheral clocks. As such, eating overnight and sleeping during the day can disrupt the temporal co-ordination between the SCN and peripheral clocks causing circadian misalignment.8
The metabolic consequences of eating at night are demonstrated by prolonged hyperglycaemia, insulin resistance and impaired lipid metabolism, all independent risk factors for the development of cardiovascular disease (CVD) and T2DM.9 10 Weight gain is a mediating factor in the disease progression of CVD and T2DM. Data indicate that shift workers are at greater risk of weight gain than day workers,11 and this appears to be independent of energy intake (EI)12 and may, in part, be due to the timing of food intake. Diurnal changes in energy expenditure have been observed at night compared with during the day.13–15 Morris et al reported in a simulated night shift study that the energy expenditure after eating was lower (44%) following after a meal in the evening compared with the morning.14 For night shift workers, eating at night, when energy expenditure is lower, may likely contribute to greater weight gain compared with day workers.16
While reducing total EI overnight may offset the reduced energy utilisation observed at night, other metabolic benefits may also be achieved. Postprandial hyperglycaemia is a consistent consequence of eating at night with data from a recent meta-analysis clearly showing time of day difference in postprandial glucose levels.17 Reconfiguring (or reducing) eating occasions to minimise overnight exposure to food intake will reduce the frequent and extended postprandial glycaemic excursions. In turn, this may reduce diabetes risk. In a simulated shift work study where participants underwent four nights of shift work, not eating at night was associated with reduced impairment in glucose response compared with eating at night.18 The feasibility of reducing EI at night (4-week crossover) has been successfully trialled in a pilot intervention in shift workers, with a small but significant weight loss achieved.19
There is, however, a scarcity of studies examining the effectiveness of weight loss interventions specifically for night shift workers. One short-term study (3 months) has reported successful weight loss in shift workers using a group-based workplace intervention approach targeting education to reduce EI and increase physical activity.20 The long-term effectiveness remains unknown. No studies have been undertaken to determine if prioritising a reduction in EI at night would be an effective and feasible approach to weight loss. Prioritising EI to earlier in the day, when the body is better equipped to metabolise it, has been associated with greater weight loss success in non-shift working populations. Prioritising EI to breakfast (50% of EI) was associated with greater weight loss than evening prioritisation of EI in isocaloric weight loss interventions lasting 8 and 12 weeks, respectively.21 22
Intermittent fasting (IF) may be a flexible approach to reducing EI promoting weight loss, whilst enabling a reduction of eating during night shift. A 5:2 IF dietary approach, limits energy consumption to 20%–25% of energy requirements on two ‘fast’ days per week and ad libitum eating on the remaining 5 days.23 IF also appears to prevent the compensatory reduction in resting energy expenditure observed in prolonged energy restriction by preserving lean body tissue.23–25 For night shift workers, aligning the two fast periods with night shift would reduce overnight EI that may have benefits on both weight and metabolic responses. Studies in non-shift workers have shown that weight loss with IF is similar to that achieved with continuous energy restriction (CER)26 but may promote greater improvements in insulin resistance (quantified by HOMA-IR),27 reductions in plasma triacylglycerol (TAG) and low-density lipoprotein (LDL) cholesterol concentrations.28 29
Despite the success of IF, its efficacy in populations that have a high incidence of obesity and unusual working schedules has not been tested. The flexibility in choosing ‘fasting’ days should enable shift workers to tailor their dietary intakes around shift schedules. Furthermore, designating ‘fasting’ days to align with night shift work, in order to avoid night-time eating, may further improve metabolic health outcomes over other weight loss strategies.
The aim of this study is to trial three weight loss strategies with shift workers to examine the effects on weight loss and insulin resistance (HOMA-IR). Using a three-arm parallel randomised trial, this study will compare CER with IF using a 5:2 approach with fasting when on night shift (5:2N) or fasting during the day (5:2D). We hypothesise that weight loss will be similar across the three strategies, and that the IF strategies will improve insulin resistance beyond that of CER. A mixed methods approach combining study retention with postintervention interviews will be used to understand the enablers and barriers to compliance.
Methods and analyses
Study design
The Shifting Weight using Intermittent Fasting in night shift workers (SWIFt) study is a three-arm multisite 18-month parallel randomised controlled trial with in-person assessments conducted at baseline (week 0), 24 weeks and 18 months. The weight loss component of the intervention is 24 weeks (weight loss phase with some food provided), followed by a 12-month postintervention follow-up period (maintenance phase) (figure 1).

Study design for the Shifting Weight using Intermittent Fasting in night shift workers study. CER, continuous energy restriction; 5:2N, intermittent fasting protocol whereby the two fast days coincide with night shifts; 5:2D, intermittent fasting protocol whereby the two fast days coincide with day shifts and/or days off.
The study was registered with the Australian New Zealand Clinical Trials Registry (ANZCTR) on 19 July 2019. Recruitment commenced in September 2019 and is still ongoing. The first participant was randomised to a dietary intervention on 10 October 2019. The design, conduct and reporting of this study will adhere to the Consolidated Standards of Reporting Trials guidelines.30 All participants will provide informed consent to participate and can withdraw at any time for any reason. The funding body had no role in the design, conduct or reporting of the trial. The ANZCTR and the relevant human research ethics committee (HREC) will be notified of protocol modifications.
Study settings
The target population for the SWIFt trial is night shift workers from workplaces in Victoria and South Australia who meet eligibility criteria. The clinical trial facilities are located at the Be Active Sleep Eat (BASE) facility at Monash University (Notting Hill) and the Clinical Trials Facility located at the University of South Australia (City East Campus, Adelaide).
Recruitment
The study will be advertised through social media platforms, online classified advertisement/community website, Gumtree, newspapers, television, radio and flyers. Accommodating workplaces and industry organisations may also facilitate advertising to personnel employed in night shifts through online and paper-based flyers, letters, electronic correspondence, newsletters, and internet and intranet sites. Interested participants are directed to the SWIFt study website (https://www.monash.edu/medicine/swiftstudy) to complete an initial online screening questionnaire (Research Electronic Data Capture (REDCap), Vanderbilt University, Nashville, USA), which will contain the consent form to completing the screening questionnaire and the participant explanatory statement of the overall study. Site-specific contact details will also be available (email and phone number) for participants to contact the researchers directly. Screening questionnaires will be reviewed by researchers at each study site before eligible participants are invited to attend a face-to-face screening session, details of which are outlined in the study procedure below.
Patient and public involvement
Patients and/or the public were not involved in the study design, data collection, analysis of results or dissemination of this research.
Participants
Eligibility criteria
Inclusion criteria
Study participants will be aged between 25 and 65 years and working a minimum of two nights per week in a permanent, rotating or split shift schedule for a minimum of six consecutive months. This scheduling is required to achieve the requirements of the 5:2N intervention. Participants will have a body mass index (BMI) of ≥28 kg/m2 for non-Asian men and women and ≥26 kg/m2 for Asian men and women and be able to attend either study site.
Exclusion criteria
Participants diagnosed with a medical condition (ie, type 1 diabetes or T2DM, CVD, inflammatory bowel disease) will be excluded. We will assess on a case-by-case basis medications that may affect body composition or metabolism (eg, antihypertensive, antidepressants, thyroxine, glucocorticoids). Other exclusion criteria include being pregnant, planning a pregnancy or breastfeeding, previous weight loss surgery, those with a genetic or endocrine-related disorder that impacts weight, those taking extended leave from work during the 24-week weight loss phase, and those who have dietary allergies or restrictions that prevent the consumption of provided study foods.
Study procedure
Eligible participants will be asked to attend either Monash University or the University of South Australia clinical facilities on 13 occasions over the 18-month timeframe of the trial. The number of face-to-face visits reflects a combination of primary data collection points and dietetic consults as part of the intervention procedures. After the emergence of COVID-19, dietetic consults were moved online and visits to the clinical facilities reduced as described below. A timeline of the impact of COVID-19 on the study is outlined in online supplemental A.
Supplemental material
The first visit is for the purpose of screening and obtaining written informed consent, with three subsequent visits (week 0 at baseline, week 24 at the end of the weight loss phase and month 18 at the end of the maintenance phase) for the collection of outcome data. We also ask participants to attend at 12 weeks into the weight loss phase for a midpoint weight loss phase assessment.
Screening and baseline
On completion of a screening questionnaire, participants who are deemed eligible are invited to a face-to-face screening session (visit 1) where researchers will explain the study in detail and take measurements including height and weight to verify that the BMI eligibility criterion is met. It will also be explained to participants that some food will be provided as part of the trial and they need to be willing to consume study food. In addition, participants will be required to complete seven questionnaires (see table 1 for details). During the screening session, participants will be provided with a 7-day food diary and a 14-day work and sleep diary to complete. They will also be provided with an accelerometer (GENEActiv, Active Insights, UK) to wear continuously for 14 days and a faecal collection kit (Melbourne only). An appointment is made for at least 14 days after the screening visit when participants will return to the clinical facilities for visit 2 (baseline visit).
Overview of assessment schedule and measures taken during the 18-month period
At the screening session (visit 1), participants may also consent to opt in to attend semistructured interviews at baseline, 24 weeks and 18 months to explore their experience of the weight loss intervention and perceived barriers or facilitators to following their allocated dietary strategy. All interviews will be facilitated by a researcher with knowledge of the overall SWIFt study. Interviews will take approximately 45 min, will be conducted either in person or via telephone/video conference, and recorded. The recordings will be transcribed by the researcher, a transcription app, or a professional transcription service. Interview transcripts will be entered into NVivo (qualitative research computer software) and analysed using a five-step framework analysis approach to identify key themes.31
At their baseline visit (visit 2), participants will undergo several assessments (see outcome measures in table 1) and be randomised to one of three dietary strategies after baseline assessments are completed. Each participant will meet with a dietitian and be provided with dietary guidance pertaining to their strategy. They will follow this diet for 24 weeks (ie, the weight loss phase). All participants will be provided with a Bluetooth weighing scale (Withings) and study food (see dietary intervention protocol section for details). Prior to visit 10 (end of weight loss phase) and visit 13 (end of maintenance phase) participants will either collect or be mailed a faecal sample collection kit (Melbourne only) and an accelerometer (GENEActiv), which they will wear for a 14-day period. Participants will also be asked to complete a 7-day food dairy and work and sleep diaries for 14 days. At visits 10 and 13, participants will return the diaries, faecal sample (Melbourne only) and accelerometers and repeat the assessments undertaken at the baseline visit. Participants receive a petrol voucher of AUS$100 on completion of the study to reimburse travel costs.
Randomisation
Following completion of baseline measurements, participants will be randomised to one of three dietary strategies (coded as 0, 1 or 2) by an independent body, the National Medical Health and Research Council Clinical Trials Centre (University of Sydney, Australia) interactive voice response system, to maintain allocation concealment. Treatment allocation is based on minimisation, balancing study site, age and sex between treatment groups. The research dietitians providing the dietary consultation cannot be blinded to the randomisation process as they provide the appropriate intervention guidance. Participants, once randomised, are no longer blinded to the intervention, but will be asked not to disclose their dietary allocation to other work colleagues participating in the trial. Analyses of primary outcomes will be conducted by a statistician who is not involved with the randomisation process and as such is blinded to the dietary intervention allocation.
Intervention
The interventions are all targeted weight loss dietary regimens, with no recommendations on changing physical activity provided. The behaviour change component centres around individualised dietary counselling, with participants also given Bluetooth weighing scales to self report weight at progress review visits (visits 3-6, 8-9,and 11-12). Details on the frequency of consultations are summarised in figure 1 and outlined in the section below.
Weight loss phase: 24 weeks
Participants are randomised to one of three weight loss dietary strategies that reduce EI by approximately 20%, with study foods provided to aid with compliance (see table 2). Only their allocated diet is described to participants, to avoid contamination or intervention bleed. The original protocol required participants to visit the research centre to conduct all dietetic consults in-person. The weight loss phase (24 weeks) comprises the baseline consult plus four fortnightly visits for the first 8 weeks, followed by three, four weekly visits up to 24 weeks. The maintenance phase (12 months) consists of a visit with the study dietitian at 2 months, 6 months and at 12 months post weight loss phase. A variation to the protocol was established post COVID-19 to reduce face-to-face visits.
Description of the three dietary strategies

Example of fasting days on the 5:2 diet.
5:2 fasting diets
To help participants adapt to the energy restriction (see figure 2), a list of additional ‘approved foods’ is provided, which includes low energy vegetables, drink and condiment options. Participants will also be recommended to increase their daily intake of water or kilojule-free fluids to 2 L/day. On non-fasting days, participants are asked not to overcompensate for fasting days, or over-restrict their EI to mimic fasting days.
Diet 1: 5:2 day fasting diet (5:2D)
The majority of EI will inadvertently occur during the daytime hours on these two fasting days, and overnight food intake will be limited. If a night shift starts on a day of no work, this does not count as a day off and cannot be allocated as a fasting day. However, the day at which a participant comes off night shift does count as a day off and can be allocated as a fasting day. At the baseline dietetic visit, the dietitian will work with the participant to determine the most appropriate times to consume the provided foods on fasting days. This plan will be based on the participant’s usual mealtimes, work schedules and usual sleep/wake times.
Diet 2: 5:2 night fasting diet (5:2N)
Every week, participants will fast over two 24-hour periods that include a night shift. At the baseline dietetic visit, the dietitian will work with the participant to determine the most appropriate times to consume the provided foods on fasting days. This plan will be based on the participant’s usual mealtimes, work schedules and usual sleep/wake times.
Diet 3: 20% daily CER
At the baseline dietetic consult, the dietitian will work with the participant to develop three to five dietary modification goals. Dietary modification goals are based on the Australian Dietary Guidelines. Examples include: increasing vegetable and fruit intake, reducing portion sizes or main meals, reducing intake of discretionary foods and drinks and takeaway foods. Participants will be provided with the Australian Guide to Health Eating brochure to assist with their understanding of their dietary modification goals. Participants on CER will also be provided with the list of additional ‘approved foods’.
Dietetic consults during weight loss phase
During each of the dietetic consults, the dietitian will review participant’s progress with weight loss and implementation of the dietary strategy. The dietitian will help participants identify and address any barriers. For the 5:2 fasting diets, this may include restructuring mealtimes on fasting days, managing hunger and reducing overcompensation on non-fasting days. For the CER strategy, this may include changes to and/or addition of dietary modification goals.
Compliance to weight loss intervention
Adherence to all dietary interventions will be assessed by food checklists of provided meals and 24-hour recalls during dietetic consults.
Maintenance phase:12 months
At the conclusion of the 24-week weight loss phase, the dietitian will provide dietary recommendations for the 12-month maintenance phase. During this phase, participants are asked to maintain the diet strategy they have been randomised to. At the 24-week diet consult, the participant will discuss and decide their goal (ie, continuing weight loss or weight stability) for the maintenance phase with the dietitian. No study foods will be provided during the maintenance phase.
Participants will be followed up at 2, 6 and 12 months of the maintenance phase. The purpose of these reviews is to discuss whether the participant can manage the dietary strategy with minimal dietetic and study support. Therefore, the dietitian will not provide new dietary recommendations at these reviews. However, they can revisit dietary recommendations provided at the 24-week diet consult or those provided during the weight loss phase.
5:2 fasting diets
Participants who are aiming to continue with weight loss will be advised to continue with two fasting days per week, while those who are aiming for weight maintenance will be advised to have one fasting day per week. The dietitian will advise participants on how to meet 2100–2500 kJ on fasting days.
Continuous energy restriction
For participants who are aiming to continue with weight loss, the dietitian will work with them to devise three to five new dietary modification goals. Participants who are aiming for weight maintenance will be advised to maintain the dietary modification goals that they have worked on during the weight loss phase.
Data collection
This section outlines the various outcome measures that will be collected throughout the trial. For a detailed summary of all data collection, refer to table 1.
Anthropometric measures
Height will be measured to the nearest 1 mm with a stadiometer at baseline. BMI will be calculated as weight/height squared (kg/m2). Body weight (primary outcome) will be measured two times at each visit (with the average value calculated) using calibrated electronic scales (Melbourne; SECA 515, Ecomed, Adelaide; SECA 703). Waist circumference, body composition and bone density will be measured at three timepoints: baseline (week 0), end of weight loss (24 weeks) and end of weight maintenance phase (18 months). Waist circumference will be measured to the nearest mm, according to the protocol of the International Society for Anthropometry, using a thin non-flexible metal measuring tape at the narrowest point of the abdomen or, if there is no obvious narrowing, at the midpoint between the lower costal (10th rib) border and the iliac crest.32 Body composition will be determined using dual-energy X-ray absorptiometry (Lunar ProdigyModel, GE Healthcare, Madison, Wisconsin, USA). Total body fat mass (%, kg), total body fat free mass (%, kg) and truncal fat and fat free mass (kg) will be recorded. At the Melborune site only, body composition is also measured using bioelectrical impedance analysis (SECA, 515, Ecomed). Bone mineral density (spine and hip) is also being measured (Melbourne only) and participants are asked to complete the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC). This 24-item, 3-subscale questionnaire measures pain (5 tems), stiffness (2 items) and physical function (17 items) experienced during everyday tasks, that is, walking, using stairs, light domestic duties.33
Biochemical measures
Blood parameters
Participants will have a fasting venous blood sample collected at baseline, 12 weeks, 24 weeks and 18 months.
Plasma collected will be used to assess glucose and insulin (to calculate primary outcome HOMA-IR). Serum collected will be used to assess blood lipids, including TAG, total cholesterol, LDL cholesterol and high-density lipoprotein (HDL) cholesterol. Whole blood will be collected for assessment of HbA1C and possible future assessment of genotype. All samples collected will be centrifuged (except whole blood samples) and stored at −80°C until analysis. Whole blood, HbA1C, serum lipid and plasma glucose analysis will be conducted on a Thermo Fisher Indiko (Thermo Fisher Scientific, Vantaa, Finland), using commercially available kits as per the manufacturer’s instructions. Plasma insulin will be analysed using the Millipore Human Insulin ELISA kit (EZHI-14K, Merck Millipore, Massachusetts, USA) according to the manufacturer’s instructions and read on an absorbance plate reader. HOMA-IR will be calculated using the following formula: (fasting plasma insulin (μU/mL)×fasting plasma glucose (mmol/L))÷22.5.
Faecal samples
Participants will collect faecal samples at baseline, 24 weeks and 18 months for gut microbiome analysis using 16SrRNA sequencing. Samples will be frozen in the participants’ domestic freezer on collection until being returned to the Monash University BASE Facility at Notting Hill, Melbourne, where they will be stored at −80°C. Analyses will be subject to additional funding.
Skin autofluorescence (SAF)
SAF will be measured (Melbourne site only) in triplicate on the ventral site of each participant’s forearm using an Advanced Glycation Endproduct (AGE) Reader (Diagnoptics Technologies, Groningen, The Netherlands). The AGE Reader estimates the level of long-term AGE accumulation in the skin, which are a marker of cumulative glycative and oxidative stress within body tissues. The intraindividual per cent error is <5.0% on a single day and 5.9% for seasonal changes.34 SAF measured by the AGE Reader has been validated against AGE accumulation in skin biopsies, and is recognised as a non-invasive method to predict future risk of T2DM and CVD, independent of traditional risk factors such as glucose, HbA1c and the metabolic syndrome.35
Physical measures (measures at baseline, 24 weeks and 18 months)
Blood pressure
Measurements will be taken using an automated sphygmomanometer (Melbourne Site: SureSigns VS3; Philips, North Ryde, Australia, Adelaide Site: Omron HEM-7320; Omron Health Care, Port Melbourne, Victoria), after participants have been seated at rest for at least 2 min and are in a fasted state. Three consistent measurements (systolic within range of 10 mm Hg and diastolic within range of 5 mm Hg) will be recorded and averaged.36
Physical activity and sleep will be measured using triaxial accelerometers (GENEActiv; Activinsights, Cambridgeshire, UK), which will be worn on the non-dominant wrist. Participants will be asked to wear the monitor 24 hours/day for 14 consecutive days, only removing it for activities where it may be submerged in water. Activity data will be processed by GENEActiv software (V.3.3), and periods of sleep and non-wear time will be calculated using custom filters.37 Data will be recorded continuously at 30 Hz. The signal vector magnitude of the acceleration, minus gravity, will be computed and summed over 1 min epochs.38 Non-wear will be identified using the method of Choi et al.39 A day will be valid if it includes at least 10 hours of waking wear time. Participants with fewer than four valid days will be excluded.40 The algorithm developed by van Hees et al41 will be used to analyse and calculate both physical activity and sleep patterns.
Timed up and go
The ‘timed up and go’ has been shown to be a reliable and valid assessment of dynamic balance during functional tasks.42 43 Participants will be timed in seconds as they rise from a seated position, walk 3 m, turn around, walk back and sit back down.43 Three measurements will be recorded and averaged, to provide a measure of functional mobility that correlates to balance and fall risk.44
Questionnaires
A battery of questionnaires will be collected at baseline (prior to weight loss phase), at the completion of the weight loss phase (24 weeks) and 1 week prior to the completion of the study (18 months) to examine the effect of the intervention on various aspects of physical and mental health states. For further details on validity and reliability of the questionnaires chosen, see table 3.
Use, validity, and reliability information for questionnaires and diaries
Outcome measures
Dietary, work and sleep diaries
Diet diary
A food diary recorded via paper record or the ‘Research Food Diary App’ (Xyris Software, Australia) will be completed for 7 days (in order to capture work and non-workdays) leading into their baseline, 24 weeks and 18 month visit. The data collected will be used to assess participants’ habitual food intake as well as changes in dietary patterns and/or choices.45 Data will be imported into Foodworks V.10, using the Australia Diet and Recipes Analysis (AUSFOODS 2019) database. Average total EI of macronutrients and micronutrients will be determined.
Work diary
Participants will be asked to use a paper diary to self-report the start and finish times of each of their shifts for 14 days leading into their baseline, 24-week and 18-month visit. This will be used to identify participants’ usual shift work patterns.
Sleep diary
Participants will be asked to record in a sleep diary the time they went to bed, time they woke, approximately how long they took to fall asleep and any extended periods of time they were awake during the sleep episode. This should take approximately 1 or 2 min per day to complete. The entries from the sleep diaries will be used to confirm sleep data obtained from accelerometer data, or in the case of participants not wearing the accelerometer, the data from the sleep diaries will be used to directly analyse sleeping patterns.46
Questionnaires
Depression Anxiety Stress Scale-21 (DASS-21)
The DASS-21 is a set of three self-report scales designed to measure the emotional states of depression, anxiety and stress,47 with cut-off scores calculated for conventional severity labels (normal, mild, moderate, severe and extremely severe) for the three emotional states.
Assessment of Quality of Life-8D
A multi attribute utility instrument used to identify the overall well-being of the individual and physical pain subscore. Included items (n=35) relate to happiness, pain, self-worth, coping and relationships.48 Participants are asked to tick the box that best describes their situation as it has been over the past week with options being never, rarely, sometimes, often or always.
International Physical Activity Questionnaires
A 27-question self-report questionnaire will assess physical activity levels. The duration (minutes) and frequency (days) of physical activity in the last 7 days are measured across multiple domains: transportation, recreation (including sport and leisure time), housework, job-related and time spent sitting.49 An overall score is calculated using responses to all questions to classify participants into one of three categories: (1) low/inactive (do not meet criteria for categories 2 or 3); (2) moderate or (3) high.
Survey of Shift Workers
This shortened version of the Standard Shift work Index consists of single response questions and rating scales (Likert scales) that capture participants’ shift details (sequencing, timing, duration, frequency and regularity of shifts), as well as individual difference and tolerance to shift work patterns.50 While responses to the included questions provide qualitative data, responses to each of the scales are calculated from 1 to 4 or 5.
Basic Nordic Sleep Questionnaire
This standardised 21-item questionnaire uses a combination of five-point scales and open-ended questions which measure the frequency of symptoms related to sleep apnoea and snoring, by quantifying how many nights/days per week the item happened over the past 3 months.51
Shift Work Disorder Questionnaire
A four-item questionnaire used to assess the risk of shift work disorder, including excessive sleepiness and insomnia.52 Questions, including, ‘in the past month, how likely were you to doze off at work during a shift?’ are scored on a 4-point scale, ranging from 1 (not a problem/not at all) to 4 (serious problem/highly likely).
Chronotype
Chronotype, an individual’s natural inclination regarding the times of day when they prefer to sleep or when they are most alert or energetic, will be assessed by the Morning–Eveningness Questionnaire, a 19-item numerical multiple choice questionnaire on a 4–5-point scale.53 These data will be collected once only at baseline.
Statistical analysis plan
Primary outcomes: analytic method
The aim of this study is to compare weight loss in night shift workers randomised to three diets. There is currently insufficient information to enable predictions about which diet will perform best; however, this study will rank the three diets from most successful to least successful based on absolute amount of weight loss achieved at 24 weeks.
Our primary hypothesis is that there will be weight loss in all three groups during the treatment phase. To test this hypothesis, mixed effects models will specify a dependent variable of weight (kg) with a predictor variable of time (baseline, 24 weeks), controlling for site (Melbourne, Adelaide), and a random effect of subject on the intercept, allowing participants to vary according to individual baseline levels, as well as tracking progress over time, appropriately accounting for serial correlation. We will undertake intention-to-treat and per protocol analyses. The primary effects of interest are the hypothesised change over time in each group. A priori sample size calculations were based on previous research, which found a small-medium within-subject effect for a 14-week workplace weight loss programme (f=0.1620). Using this as a minimum expected amount of weight loss in a given study group over a 6-month time period (accounting for serial correlation between baseline and 24 weeks), at the end of the treatment phase we would require 93 participants (α=0.05, 1−β=0.8), accounting for an expected 27% dropout,20 requiring randomisation of 120 participants into each diet group.
Descriptive analyses will quantify the effect size of the weight loss in each diet group. We will calculate point estimates and their variability (bootstrapping for 95% CI). These will be calculated for the active phase, and for the maintenance phase (18 months).
A secondary hypothesis is that there will be a differential effect of the diets across time on HOMA-IR (insulin resistance). Based on previous research suggesting the potential metabolic benefits of avoiding food consumption during night-time hours,18 we hypothesise that the 5:2 night-time fasting group will display an improvement in metabolism (as indicated by HOMA-IR) relative to the other diet groups. To test this hypothesis, mixed effects models will specify a dependent variable of HOMA-IR. Models will specify predictor variables of group (20% CER, 5:2D and 5:2N), time (baseline, 24 weeks) and group x time, with a random effect of subject on the intercept. The primary effect of interest is the group x time interaction effect. Sample size calculations were based on previous research, which found effect sizes for differences in night and day shift workers in HOMA-IR that ranged from small–medium (f=0.1454) to medium–large (f=0.3355). Conservatively, powering for a small–medium interaction effect, we would require 111 participants per group (α=0.05, 1−β=0.8), and accounting for an expected 27% dropout,20 we would need to recruit a total of 423 participants. Since our primary hypotheses are different, and independent, to avoid unnecessarily increasing our type 2 error rates,56 57we argue that family-wise p value adjustment for our main analyses is not appropriate.
Additional analyses will examine changes in HOMA-IR in each of the groups during the maintenance phase (18 months). Mixed effects models will specify a dependent variable of HOMA-IR and predictor variables of group (20% CER, 5:2D and 5:2N), time (24 weeks, 18 months), and group x time, with a random effect of subject on the intercept. To make sure that there is sufficient power to adequately test all of study hypotheses, we require the largest sample size estimate from the above calculations. Therefore, to detect all the effects of interest, 141 participants per group (total n=423) will be recruited over the two sites.
Exploratory analyses conducted using mixed effects models (specifying predictor variables of group, time and group x time, with a random effect of subject on the intercept), will be used to examine differences in lipids, glucose, insulin, HbA1c, body composition, waist circumference, blood pressure and QoL rating. A Kaplan-Meier survival analysis model will specify time to dropout as the dependent, and group as the independent variable (with a log-rank test for difference between curves), examining group differences in protocol dropout.
Post-COVID-19 study power estimates
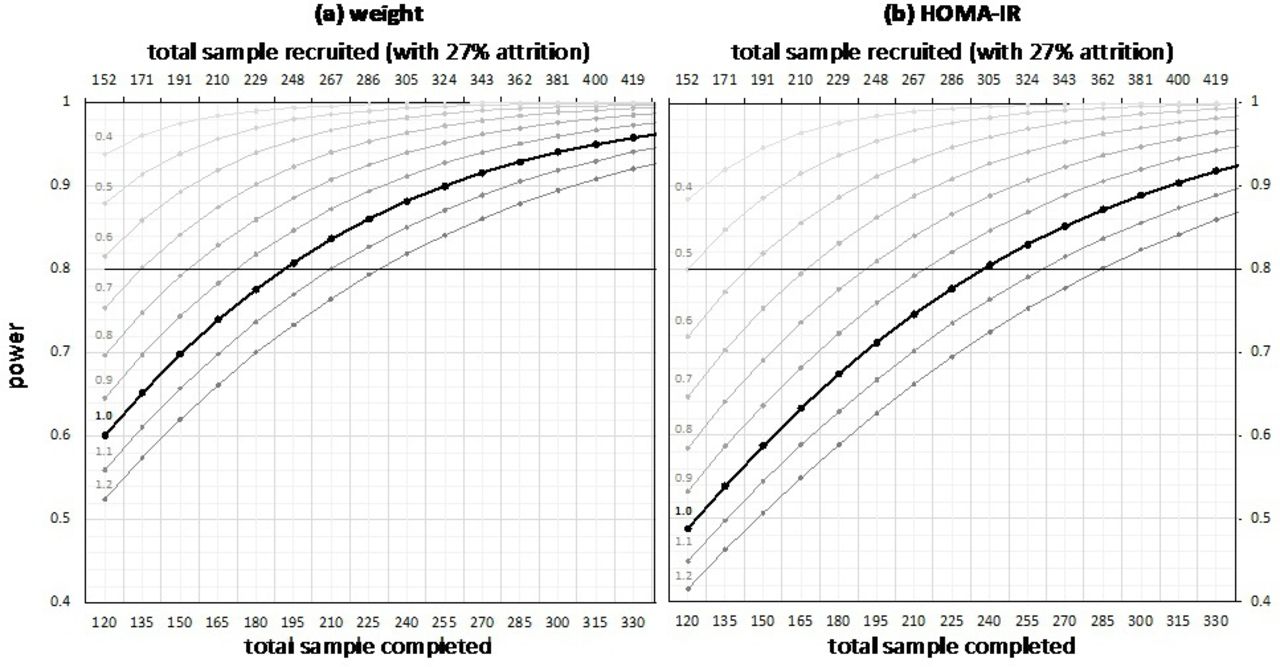
COVID-19 impacted study recruitment and data collection (online supplemental A), and as such, it is unlikely that we will reach initial sample size targets. In such cases, it is recommended that power be calculated and evaluated relative to the research aims.58 These power analyses reflect two improvements in comparison to the initial sample size calculations: (1) they have been conducted using GLIMMPSE,59 a recommended online power calculation platform for the general linear multivariate model with a fixed predictor60 and (2) they have been calculated using a more recent and relevant published estimate of the expected differences between IF and calorie restriction.61 These calculations (figure 3) suggest that, using conservative estimates for the standard deviations (for variability scale=1.0), for a 3% weight loss, 80% power would be reached at a sample size of n=64 per group (total n=192) and for HOMA-IR, this would occur a sample size of n=79 per group (total n=237). For details, see online supplemental B.
Supplemental material

{kind=link}
{kind=link}
{kind=link}
Power calculations for weight (A) and homeostatic model assessment of insulin resistance (HOMA-IR) (B). Power (y-axis) is displayed for increasing sample size (primary x-axis), with the 27% inflation applied (secondary x-axis) to account for attrition. Weight calculations represent predicted power to detect a 3% within-subject change from baseline to 24 weeks across all groups (20% continuous energy restriction, 5:2D and 5:2N). HOMA-IR calculations represent predicted power to detect a group–time interaction effect. Multiple lines represent estimated data series with scaling applied to the variability estimates (0.4–1.2) and the bold line indicating scaling equals 1.0 or no adjustment.
Data management
Study data will be collected and managed using REDCap electronic data capture tools hosted and managed by Helix (Monash University).62 63 REDCap is a secure, web-based software platform designed to support data capture for research studies, providing (1) an intuitive interface for validated data capture; (2) audit trails for tracking data manipulation and export procedures; (3) automated export procedures for seamless data downloads to common statistical packages; and (4) procedures for data integration and interoperability with external sources. All data forms will be deidentified and paper copies will be double entered and stored in the username-protected and password-protected electronic database.
Advisory committee
This project has an advisory committee comprised of researchers affiliated with the project and external to the project as well as industry representatives, a medical practitioner and consumer representation. The committee meets every 3 months to oversee progress and adherence to the protocol and monitor adverse events. Any major protocol deviations and serious adverse events that are identified during the study will be reported to the committee by the chief investigator (MPB). All expected and unexpected adverse events reported by participants are recorded into REDCap and discussed as an agenda item at monthly site team meetings, separate to the advisory committee. Those that are deemed reportable are referred to the study physician for guidance in determining continuation of the intervention. In Adelaide, all adverse events are reported to their ethics committee even if deemed not associated with the study. As per Monash Health reporting guidelines, the CI at the Monash site decides, in conjunction with the advisory committee, whether events are reportable to the ethics committee (Monash Health).
Ethics and dissemination
The study protocol was approved by Monash Health, as the primary HREC (HREC ref: RES 19-0000-462A) and registered with Monash University HREC. Ethical approval has also been obtained from the University of South Australia (HREC ID: 202379) and Ambulance Victoria Research Committee (R19-037). Results from this trial will be disseminated through national and international presentations and peer-reviewed journals.
Confidentiality
Personal information (name and contact details) will be collected by study researchers and stored in a password-protected electronic database (REDCap electronic data capture tools 62 63). Only the study’s researchers will have access to this information. Only deidentified data will be presented via publications.
Discussion
Shift workers gain weight more readily than their non-shift working counterparts and are at an increased risk of developing CVD and T2DM. The circadian misalignment experienced by these workers likely contributes to the increased risk of weight gain and consequent development of chronic diseases. However, specific guidance for this population group on how to effectively manage their weight is lacking.
While reducing EI, in the absence of decreased energy expenditure, is an effective strategy to lose weight, the mistiming of eating and sleeping behaviours experienced by these workers may limit the effectiveness of traditional weight loss strategies. At a physiological level, the mechanisms underlying this weight gain do not appear to be related solely to overall EI. Instead, the timing of food intake, or eating late into the night, has been associated with metabolic complications such as impaired glucose tolerance and lowered postprandial energy expenditure that may contribute to weight gain.13 17 18 64 65 Furthermore, from a behavioural consideration, access to (healthy) food at night may be compromised, with poor food choices widely reported in shift working populations often as a result of lack of motivation to eat well.66
In trying to encourage weight loss in shift workers, we propose that a successful strategy would need to be simple to adhere to, without reliance on food from the workplace, to minimise the energy consumed at night-time. One strategy that warrants investigation is IF, as this approach enables flexibility in the choice of fast days and can inadvertently minimise EI at times of metabolic perturbations (overnight). However, the efficacy of IF in populations with unusual working schedules has not been examined.
Strengths
There are several key strengths to this study design. To the best of our knowledge, this will be the first trial assessing multiple different weight loss strategies that consider shift schedule and meal times in shift working populations. In addition, it will assess a number of additional health outcomes including cardiometabolic and psychological. Thus, this study provides key insight into how different weight loss strategies may assist the overall health of the shift worker population. Inclusion of an active control group, using the current gold standard intervention practice of 20% CER for weight loss, helps to inform practice as it provides evidence that the treatment/intervention will be effective in usual practice. Lastly, investigations into the enablers and barriers to compliance will assist with the development of future dietary intervention study designs, given enablers and barriers will provide insight into some of the unique considerations and supportive strategies of such interventions in this cohort.
Limitations
It is anticipated that recruitment into the study will be challenging and potentially could be a rate-limiting step in study progression. Shift workers, as a result of their work schedules, can be difficult to engage. Distributing the recruitment over two research sites and two research teams who collectively have extensive experience in engaging with shift working populations will ensure successful recruitment. We also have established links with many shift work organisations and our advisory committee includes representation from both stakeholders (shift workers) and management personnel of shift working industries. Other perceived challenges are the heterogeneity in our data introduced by the many existing shift schedules and occupations that participants are likely to partake in. Our eligibility criteria require a minimum of two overnight shifts per week, but we anticipate the range of roles to be extensive in order to meet our recruitment targets. Additionally, we acknowledge that only a known diagnosis of diabetes is an exclusion criterion, and as a diagnostic HbA1c serology is not conducted at screening, individuals with undiagnosed diabetes may be included within the trial population. Furthermore, as with all behaviour change interventions, the researchers rely on participants to adhere to their allocated regimen. A high dropout rate of nearly 30% has been allowed for, based on typical dropout rates from weight loss interventions of a similar duration.
Ethics statements
Patient consent for publication
Acknowledgments
We would like to acknowledge the following individuals; A/Prof Leonie Heilbronn, Mrs Louise Massie and Dr Catherine Yandell.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors MPB, SB, CEH, AC, JD, NJK and TLS were coapplicants on the original NHMRC grant application and were involved with the original design. CLY and MI were involved in initial study set up and data collection. MPB was the lead applicant and principal investigator for the study. MPB, AC, MR, GKWL, RD, YYP, ABC and CD are involved with study co-ordination and responsible for the day-to-day running of the trial, recruitment and sample collection. JD will be responsible for analyses and statistical interpretation of results. All authors will have responsibility for preparation of manuscripts for publication poststudy completion.
Funding This trial was supported by a National Health and Medical Research Council grant, grant ID APP1159762.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.