Article Text

Abstract
Objectives The aim was to understand how participants engage with Brown Buttabean Motivation (BBM) a grassroots, Pacific-led holistic health programme and the meaning it has in their lives. The objectives were to explore the impact BBM had on all aspects of their health and well-being, what attracted them, why they stayed, identify possible enablers and barriers to engagement, and understand impact of COVID-19 restrictions.
Design Qualitative study with thematic analysis of semi-structured interviews of BBM participants, followed by theoretical deductive analysis of coded data guided by Pacific Fonofale and Māori Te Whare Tapa Whā health models. In this meeting-house metaphor, floor is family, roof is culture, house-posts represent physical, mental, spiritual and sociodemographic health and well-being, with surroundings of environment, time and context.
Setting Interviews of BBM members conducted in South Auckland, New Zealand, 2020.
Participants 22 interviewees (50% female) aged 24–60 years of mixed Pacific and Māori ethnicities with a mixture of regular members, attendees of the programme for those morbidly obese and trainers.
Results Two researchers independently coded data with adjudication and kappa=0.61 between coders. Participants identified the interactive holistic nature of health and well-being. As well as physical, mental and spiritual benefits, BBM helped many reconnect with both their family and their culture.
Conclusions BBM’s primary aim is weight-loss motivation. Many weight loss studies provide programmes to improve physical exercise and nutrition, but seldom address sustainability and other core factors such as mental health. Programmes are often designed by researchers or authorities. BBM is a community-embedded intervention, with no reliance external authorities for its ongoing implementation. It addresses many factors impacting participants’ lives and social determinants of health as well as its core business of exercise and diet change. Our results indicate that BBM’s holistic approach and responsiveness to perceived community needs may contribute to its sustained success.
- PUBLIC HEALTH
- QUALITATIVE RESEARCH
- MENTAL HEALTH
- General endocrinology
Data availability statement
No data are available. The rich contextual data in this study is derived from interview transcripts and for ethical reasons it is not appropriate for these data to be shared for secondary analyses.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
A strength is the rich dataset from a diverse range of participants.
Analysis was guided using Pacific theoretical framework.
A further strength is independent coding of data with adjudication between researchers and calculation of inter-rater reliability.
Although some participants’ involvement had lapsed for a time, all were still engaged with Brown Buttabean Motivation, and interviews with people who had discontinued their involvement might have given different insights.
Introduction
Despite 40 years of evidence and advocacy to address rapid weight gain in New Zealand (NZ), statistics consistently illustrate epidemic proportions of obesity.1 Recent data indicate about 31% of adults are reported to experience obesity.2 Of major concern is the unequal burden of obesity, impacting nearly two-thirds Pacific (63%) and almost half of all Māori (48%) adults.
The origins of obesity are complex, but a key factor is the ‘obesogenic environment’ with high availability of cheap, energy-dense food, poverty, food insecurity and racism. The impact of the obesogenic environment is particularly evident in indigenous (Māori in NZ) and marginalised peoples.3 These systemic issues, along with a lack of physical activity and inappropriate nutrition,4 contribute to disproportionate obesity in Māori and Pasifika people (Pacific people living in NZ). Pasifika are 40% more likely to have sedentary lifestyles than the total NZ population, and more likely to dwell in neighbourhoods with fewer economic resources, where obesity is more prevalent.5 Evidence indicates that the fundamental causes of ethnic disparities in health are social and economic inequalities, which are underpinned by racism.6 Obesity is associated with premature mortality and several health conditions including type 2 diabetes, cardiovascular disease, cancer and obstructive sleep apnoea, as well as psychological and social problems. Given the high prevalence of overweight and obesity in the Pacific population, programmes should target the whole community and the environment in which they live, rather than targeting individuals.7
Internationally, robust randomised trials have been conducted on lifestyle interventions, which have assessed weight loss as an outcome. Several large studies have demonstrated significant weight losses,8–10 but these changes may not be sustained long-term. Programmes that engage Pacific communities over time to maintain weight loss face considerable challenges. Sociocultural factors play a significant role in diet and physical activity, and tailored interventions are needed to provide culturally appropriate community-based approaches.11 A number of such programmes have been assessed in Pacific and Māori populations, although these are generally small and low quality studies, and some have reported small reductions in weight. Key enabling factors identified include rewards such as money or enjoyment, social connection and making lifestyle changes that are achievable and sustainable over time.
Brown Buttabean Motivation (BBM) is a Pacific and Māori-led health programme established in 2014. With an overarching vision to prevent and reduce obesity and associated conditions such as diabetes, its programmes are aimed at helping people lose weight in a healthy sustainable way while achieving health, fitness and motivational goals.12 The core activities are a number of bootcamp trainer-led exercise classes where people participate collectively and encourage and support each other. Exercises can be modified according to ability, and in the ‘From the Couch’ classes people with morbid obesity exercise in a sitting position. All classes are free, a variety are run between 5:30 am and 20.30 hour to accommodate people’s different working and domestic lives, and pre-COVID-19, no registration nor class-size restrictions were required. Some bring their children with whole families exercising together. Trainers have all come through the programme and are unpaid. With the onset of the pandemic, many classes moved online and BBM also ran a growing foodbank, distributing healthy donated food boxes to Pacific people suffering food insecurity, and running vaccination drives.
Testimonials from members report large and sustained weight loss, but they say that it is much more than just a weight reduction or an exercise programme. It has inspired them to change the way they live their lives. BBM differs from interventions designed for research projects, because it is a self-referral and holistic service run by a grassroots, organic organisation adapting to the needs of the community it serves.
Objectives
The aim of this study was to understand participants’ engagement with BBM, and the meaning it has had in their lives. The objectives were to explore how participants have engaged with BBM, the impact it has had on all aspects of their health and well-being, what has attracted them and why they have stayed, and to identify possible enablers and barriers to people engaging with BBM.
Methods
Study design
This qualitative study of participants’ engagement with BBM uses an initial deductive thematic approach, combined with a subsequent theoretical inductive analysis of coded data.13
Patient and public involvement
This is a codesign project of University researchers and the public organisation BBM. BBM has been integrally involved in the study design, recruitment to the study and will assist in dissemination. Throughout the process the University of Auckland researchers have been led by the priorities, experiences and preferences of BBM.
Participants
Sampling was purposive from a range of BBM programmes with an emphasis on diversity including age, gender and number of years of involvement, including volunteer trainers who have been through the programme. Given that BBM is predominantly a Pasifika and Māori programme, the focus was on these ethnicities.
Recruitment
Adult participants (18 years and older) were recruited through the BBM network, using a snowballing technique. Members of the BBM operational team approached potential participants, as well as posting invitations on their social media platforms and displaying posters in the physical headquarters. Participants were asked if they would like to be involved in the research, given a Participant Information Sheet if they were interested, and asked to contact the research assistant to arrange an interview time.
Interviews and setting
In-depth interviews were conducted by three trained research assistants of Tongan, Samoan/Māori and Fijian ethnicities using a semi-structured interview schedule (see online supplemental information). During the interviews, BBM participants were invited to talk about their engagement with BBM, with prompts as required. Interviews ranged from 18 to 53 min, with an average of 36 min. They were audiorecorded with informed consent, and conducted face-to-face in a South Auckland office (n=13) or remotely via Zoom (n=9), depending on the COVID-19 alert levels in place. Interview transcripts were transcribed either by the interviewer or via a commercial transcribing service. All participants self-identified ethnicity, including multiple ethnicities, and were identified by a pseudonym. One researcher intermittently reviewed the participant demographics and the interview transcripts. Because it was proving difficult to recruit Pasifika males, an older male interviewer was added to complement the two young female ones. Participant recruitment ceased when there was data saturation across a diverse range of participants.
Supplemental material
Analyses
An initial inductive thematic analysis approach was used. After reading and re-reading the responses, the authors devised a coding framework through a process of consensus. All participants were assigned Pacific pseudonyms to ensure anonymity. The interviews were loaded into NVivo V.13 and data were coded separately for each participant. The key overarching themes were barriers to BBM engagement, the culture of BBM, not just an exercise programme, personal benefits gained and the impact of COVID-19, with underlying subthemes in each. The process was iterative, with codes and their descriptions further adapted following joint discussions between four researchers. Two researchers coded independently and resolved discrepancies through adjudication. Cohen’s Kappa for each code were exported from NVivo and an average calculated to measure inter-rater reliability.
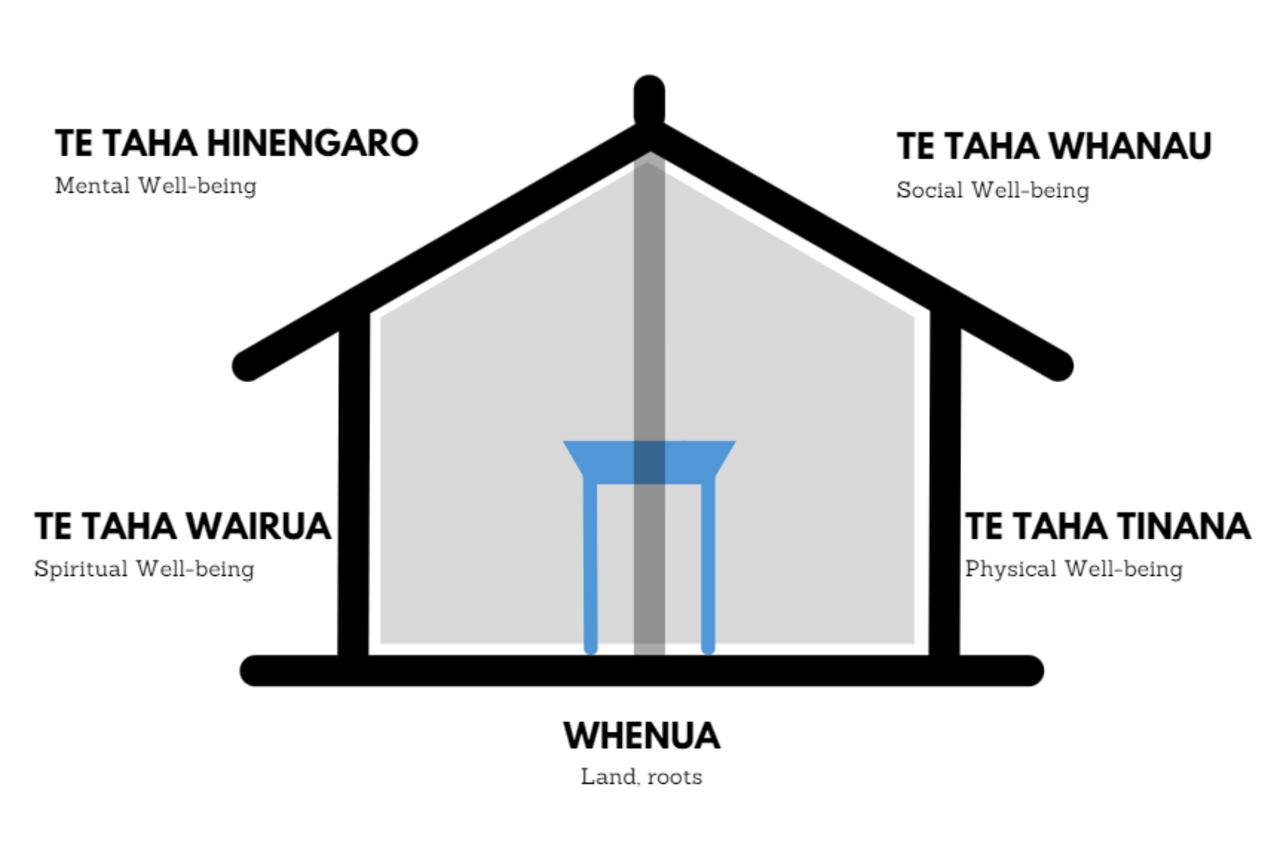
Once the data were coded, a deductive analysis was guided by the Pacific health Fonofale framework14 (figure 1), and the similar Māori health Te Whare Tapa Whā model15 (figure 2), which use the dimensions of a Samoan or Māori meeting-house as a metaphor. In Fonofale, the floor/foundation is the family and community, defined broadly as extended family and other community member relationships connected by shared values (taha whānau for Māori).16 In the Māori model, the foundation of the whare is the land and place of belonging (whenua), and family is represented by the fourth pillar (taha whānau).

Fonofale model of Pasifika health and well-being.15
{kind=link}
{kind=link}
Te Whare Tapa Whā model of Māori health and well-being.16
The four posts (pou) of Fonofale are the physical, mental, spiritual and other components of health and well-being. Physical well-being (taha tinana in Māori) involves taking care of one’s body with healthy lifestyle behaviours and managing disease. Mental well-being (taha hinengaro) involves emotions, cognition, communication and motivation to achieve goals, not just addressing mental illness or distress. Spiritual well-being (taha wairua) may relate to faith or religious beliefs, or a connection with the sacred. It may be expressed through beliefs and practices that support a sense of self-awareness, identity and purpose. The fourth pou identifies other components such as sexuality, age, gender and socioeconomic status that might influence well-being.
In the Fonofale model, the roof represents cultural practices, beliefs and values that shelter people. Surrounding the fale is the physical environment, the sociopolitical context and the point in time. This is a dynamic model promoting the holistic nature of health and well-being, and the interactive relationship of components. Themes and specific codes were mapped to the elements of Fonofale (table 1), and the results are presented using this theoretical model.
Fonofale framework mapped to themes and codes
Results
There were 22 participants, 11 male and 11 female, aged between 24 and 60 years, of Pacific (Samoan, Tongan, Niuean, Cook Island Māori), Māori or mixed Pacific/Māori ethnicities, with the exception of one South American (table 2). Thirteen were members of BBM programmes, three were attending ‘From the Couch’ for those with morbid obesity, and six were involved in training and coaching. The majority of participants self-reported weight loss since attending BBM, ranging between 3 and 135 kilograms. Their involvement with BBM spanned from 3 months to 5 years, with an average of 2 years 4 months.
Description of participants
Cohen’s kappa was 0.61 between two coders, indicating moderate inter-rater reliability. Coded results are presented using the structure of the meeting house (Fonofale) theoretical framework.
Family foundation
Family and community as the foundation or base of BBM is demonstrated in the codes of collective support, social enabler and social support. ‘I’m more accountable in a group than doing it on my own’ [Mele]; ‘everybody’s helping everybody’ [Pita]; ‘felt like it was a big family straight away’ [Lima]; and ‘recognising that for our Polynesian people … health and wellbeing lies in our hands …, but it’s something that we need to do sort of collectively’ [Mahina]. Hine says ‘the movement and the culture that we have at BBM is all whānau and family-orientated …we like to serve and help our people’.
For some, BBM has helped them to re-connect with their families. Afi says ‘Two years ago, I never attended family functions—I always say to my wife, you go, I’ll stay home because I do night shift, so I always make excuse not to go… Now, I’m like confident, I always turn up to the family functions and I always put my hand up, it’s been awesome aye, it’s been a big life changing for me and my family’. Similarly, Lima explains that before attending BBM, ‘I used to lock myself in the room at home… make up excuses, not even go to family events, because I just didn’t want to be seen in public’.
BBM also helped some participants better look after their own families. ‘Family, whānau is the core… Knowing your purpose in terms of what you're doing and how that impacts your family. If you can’t look after yourself, you obviously can't look after your family [Filipo] and ‘my wife’s doing it as well with me so we kind of train together and I guess that because I’ve got four kids and they look at us and they go, oh mum and dad’s training. So, we’re trying to instil that into them’ [Sefulu]. Ane has seven children and says ‘how can we look after our children if we’re not looking after ourselves? I nearly lost my kids at one point but my own journey, now that is what we are showing our kids’. For Iva, BBM has had ‘a massive impact in terms of getting us involved as a family… our family getting stronger together, working out together, having things to talk about together, and having discussions about the pros and cons of what we’re doing’.
Physical well-being pou
The code of improved physical health mapped directly to the physical health house-post (pou). Examples include ‘[the doctor] said I don't know what you've done but you’re no longer diabetic and you need to stop taking your pills’ [Pita]; ‘my doctor said to me ‘I can’t believe this but, you don’t need the [sleep] machine anymore… your breathing is fine, your heart rate is so good. I did an overnight there, they watch you with cameras all night, and they said that I was like not even making all these weird noises.’ [Tipene]; and ‘I’m taking all these drugs because I have a heart condition and yeah my doctor’s going what are you doing different? I said I’m at BBM. He says keep going, because your blood pressure’s nice, it’s at a good level’ (Ioane).
Help with daily activities also fits with this pou. Mana describes how reducing her size through being with BBM means she can now do things others take for granted: ‘walking up and down the stairs, fitting in a car, washing myself, tying my own shoelaces… BBM has given me all those things ten-fold’. For Lima it means now ‘being able to fit in a chair’ and Pita ‘walking upstairs carrying stuff’. Many describe engaging in healthier behaviours. Mana says ‘outings that I used to do back in the day would be to the pub, to a karaoke bar or whatever… now my outings are to the beach or to the pools, or to walk up a mountain’. For Pita ‘since I came here, I trained every day, doing the right food, drinking a lot of ice water and stuff’, and Mona ‘We don't eat very many takeaways anymore, no fizzy. Before I was real bad, oh man, I would sit in my bed at night with my bottle of drink and chips and chocolate and biscuits, yeah’.
Mental well-being pou
This was the strongest theme. Many participants responded that BBM has helped them with their mental health. Examples include ‘helped me a lot mentally I'm not stressed. I can handle difficult situations at work because we do get really busy. Yeah, I just take it in stride. BBM has been a great help in my life’ [Mele]; ‘having a clearer mind, being a lot more focused, able to set goals for myself that I know that I can achieve’ [Mahina]; ‘it made me feel better and more confident’ [Leilani]; ‘when I started with BBM, I was suffering from quite a bit of anxiety and having panic attacks… I was on counselling, and medication… my mental health was in quite a bad state. Now I can address 100 people in a room for a session. I can run a session alone and not have any issues, I’m quite the extrovert now. I have seen a big shift in me being more sociable and in my mental health’ [Teuila] and ‘mental wellbeing, that’s the bit that’s helped me the most’ [Tane]. Fetu explains that ‘I went through depression four and a half years ago where everything went downhill from there. It’s been an uphill battle from there… I’m off the anti-depressants… just everything is positive. I’m happy to wake up, I’m happy to train, do the 6am classes to get it out of the way and then straight into work after that. In the beginning it was hard, but now it’s just a part of my life and so the mental aspect, that’s helped me phenomenally. I’m a natural pessimist but now my wife’s just like, man you must be on crack or something. Because it’s just always positive’.
Motivation was also a big theme, including no shame if they lapsed. ‘If you fall off the wagon you just reset and carry on again. No-one says, oh you fell off, dopey fool eh, you don’t get that. All you get is well, stand up, let’s go again. You’re not the dopey fool that fell off. You’re the guy that stands up and carries on again’ [Ioane]; ‘you can come off the wagon, but you're always welcomed back and I suppose that helps with someone like me that’s got self-esteem issues’ [Huhana], and ‘I learnt that hey, don’t worry about it. Stop. Reset. Which is a big thing at BBM. Once you’ve recognised your failure, you reset, you start again’ [Ioane]. Similarly, Ane says he relates to the BBM message that ‘people don’t know that it’s okay to be vulnerable, it’s okay to be weak—just be able to stand back up. You can fall so many times—who cares, it’s how you get back up’.
Spiritual well-being pou
The third pou represents spiritual health. For Mana ‘for ages I was kind of just disconnected from a spiritual side’ but since BBM she has learnt that ‘if you give to God, he'll give to you as well’. For Iva ‘It’s not necessarily God but … when I relax and my mind is clear and I’m just thinking about bettering myself, just positive thoughts. Spirituality is more of a meditating state’. Mona says that ‘God is good and, it’s God’s blessings that things happen when they happen. My partner and I have a saying that, we're in the right place at the right time, or we are where we need to be’. From Tane’s point of view ‘I go to church when I can, but it’s just made me more positive. Like I’m not all hocusy pocusy, I know there’s issues I still need to work on. I’ll always have my faith. Basically, through Dave and BBM it’s just increased my faith’.
Mahina identifies her spiritual health with ‘tino rangatiratanga or self-determination… being part of something bigger, re-educating our people about who we actually are, and not in a Western sense, as people of the Pacific… and the beautiful things that we have to offer the world when we're in the right body, mind, spirit’. It engenders a sense of self-control and leadership ‘helping me to recognise that, you know, I have the ability to do whatever it is I set my mind to’ [Mahina], and Iva ‘BBM has given me the opportunity to lead from the front as opposed to leading from the back.’
Other well-being pou
Some participants identified other social benefits from BBM such as financial ‘I’ve saved a lot of money—stop spending money on junk food’ [Pita]; providing a safe tolerant environment ‘We all grew up in the hood, in state houses, we all have been around alcoholism, gang affiliations. We’re able to go into the safe space that he’s given us, because I’ve been to the gym—I don’t feel comfortable there’ [Ane] and ‘it’s just like a safe space, the community and knowing that you're not alone’ [Mana]; impact on their children ‘my kids are confident in their schoolwork, when they go to school they’re always putting their hands up… I know my kids were shy before—now they’re confident and doing stuff because they’ve seen what it’s like to work hard for your stuff or set a goal’ [Afi); addressing food insecurity ‘putting food on our table so we were able to pay our rent’ [Ane], and employment ‘I was unemployed. I was on the benefit. I had just gotten out of jail… she talked to Dave to help me find a job, and that’s how I ended up with the food bank job…Such a blessing’ [Hine].
Cultural roof
Culture serves as the roof in the Fonofale model. In the context of this study, this is both Pacific cultural values and the culture of BBM, with its own qualities and values. Participants indicated that BBM has helped them connect with their own and other Pacific and Māori cultures - ‘a connection to your culture which is actually really really strong’ [Huhana]; ‘get to respect other people’s cultures’ [Pita]; and ‘I’ve learnt a whole lot being surrounded by people of my culture than I would have, if I had not joined BBM… the island culture isn’t individual like the western culture’ (Tane). Mahina says ‘recognising our Polynesian people is that our health and wellbeing lies in our hands, but it’s something that we need to do sort of collectively’.
Collective support is one of the valued qualities of BBM – ‘everybody encourages each other, which whatever fitness level you are’ [Mele] and ‘always encourage you to cheer each other, to give high fives is part of the culture at BBM and making some fun and doing some exercise like games’ [Lucia]. Ioane explains how helping each other is a core Pacific value: ‘We’d go back to Samoa, and there’d be things that people just did. If you need help, people just came and helped. If you were cutting the grass, the next-door neighbour with his machete and two of you will be cutting the grass. So it’d be done. This is what BBM’s like’.
Other cultural components are the sense of belonging and inclusive welcoming: ‘positivity, the vibe is good. When you go there it’s very inviting’ [Iva] and ‘As soon as you step through that door you immediately belong to the BBM family, especially it doesn’t matter where you’re from, doesn’t matter what culture, doesn’t matter what size—you can walk through those doors, straight away everyone’s encouraging you’ [Lima]. BBM has the by-line of no excuses: ‘A saying that BBM has is no excuses. And I say that to myself every day when I get up. Gotta get up no excuses. You know, and to any little thing. Put the rubbish out, no excuses’ [Pita]; ‘I used to have all these excuses… now I always believe that there’s always a way, just don’t give up and just find something that works for you’ [Lima]. BBM also has the motto of no judgements: ‘being an addict,… I’m Māori and I've got tattoos, I’m not you know that educated, I didn't finish school and just being taken in by BBM with open arms. No judgments’ [Hine] and ‘BBM I can walk in anytime. I don’t feel embarrassed. I don’t feel shy. When I'm in public I still struggle on my own’ [Huhana]. Mina sums up the sense of inclusiveness with ‘we're all on this journey together’.
Surroundings
Environmental factors include access to classes—for some people, location of classes is a barrier ‘some people can make it and some people it’s too far’ [Iva], or they may be over-crowded ‘all sessions always be packed’ [Mele]. For others ‘classes are free which is a bonus’ [Mele] and they value the flexibility provided by online options ‘even if you didn't go to the boot camps you've got the online as well’ [Huhana]. Timing of classes is an issue for some, for example Pita would like ‘more classes at different times because of my work’. Several also identified that they need to make time to fit BBM into their lives, especially if they are leading classes—‘we run classes at 5.45 in the morning… you’ve got to give up time so that is the sacrifice, and I accept it’ [Iva] and ‘personal cost is time‘ [Ioane].
One of the biggest contextual factors has been the COVID-19 pandemic. The interviews mostly took place after NZ’s first hard (Level 4) lockdown requiring people to stay at home: ‘I was pretty scared to go outside to be honest, you know when they were saying, don't go up street, don’t walk around. We tried some online but it just didn't feel this thing’ [Pita]. Some regained lost weight ‘I’ve put it all back on. That’s why I’m doing the reset’ [Leilani]. The social connection was also missed ‘Not having that social interaction, that was tough’ [Ioane] and ‘I missed the people’ [Lucia].
Others, however, found that BBM moved live online and still supported them: ‘stuff that we learnt from BBM we trained at home, like we knew what to do and that. And he was also giving programmes on Facebook, there was still no excuses not to train. He put down programmes for us on our Facebook page - here’s a programme for you guys to do today and just carry on’ [Sefulu] and ‘luckily I have a very good training partner, so we did zoom workouts and that kept me going. Even if I wasn’t able to be with my BBM family, I still found a means to train’ [Teuila]. Not all gained weight—‘I lost 10 kgs during the lockdown’ [Tipene]. Mina says ‘it was more online because it was lock down. There was just trying to find things to do. It was hard, but after listening to Dave and going through his life story that was just an inspiration. So since lockdown I was able to drop 30 kilos right till today’.
For many, BBM is seen as not just an exercise programme but their own and their family’s new way of life: ‘I’ve changed my lifestyle. I don’t do what I used to do before’ [Afi] and ‘I could never imagine leaving BBM’ [Huhana]; ‘it’s a journey for me personally’ [Mele], and ‘it’s not a short journey, it’s a long-term journey’ [Afi]. Ane, ‘this is my lifestyle … now I can’t wake up without doing a workout … I’m getting my kids done, and going to work’. Sefulu says ‘when the kids look at you and it rubs off on them and I guess once that’s installed in them and they just carry on with their family later on in their life.’
While the different health benefits were recognised, participants identified the interactive holistic nature of health and well-being. As Mahina says ‘I've just come to realise that it actually has benefits, mentally, spiritually, it’s amazing just how life changing… having a healthy mind and body can do for a person’. Hine connects her spiritual health with the other aspects of her life. ‘My spiritual health…, it’s all like a ripple effect, I feel good because I've exercised. I've lost weight so that it makes me feel good, and mentally my mind is clear. So my body, my tinana, feels good, and then my mind feels good, my hinengaro and then my wairua feels good. It all goes together pretty much… It’s really awesome. It’s really food for the soul having good people like that encouraging and uplifting you like every day’.
Discussion
This study firmly asserts profound insights of why this holistic lifestyle change programme for Māori and Pasifika peoples appears to be intrinsically meaningful and therefore effective for participants. BBM’s difference is its grassroot origins as a Pasifika and Māori-led intervention, embedded in the community it serves, with no reliance on researchers nor external authorities for ongoing implementation. Most participants (18/22, 82%) self-reported a weight loss ranging from 3 to 135 kg since joining BBM. Moreover, all respondents identified benefits from BBM across various aspects of their lives beyond improvements in weight and physical fitness. Our coded data fitted well into the Pacific15 and the Māori16 models of health, which comprise individual elements of overall well-being. Participants identified positive effects on their physical, mental, emotional and spiritual health and well-being, which were often woven together so that they augmented each other. Many identified BBM as both their family and their culture.
The 1946 Constitution of the WHO declared that ‘health is a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity’.17 This concept was reaffirmed in the WHO Alma-Ata (1978)18 and Astana (2018)19 Declarations which identified the need for primary healthcare to address the economic, sociocultural and political determinants of health for individuals, communities and families, as well as providing first-contact comprehensive, continuous and equitable care across their lifespan. Primary care should look after the whole person in the context of their life and their family. However, too often care is fragmented and focused on single conditions or diseases.
Many weight loss studies provide programmes to improve physical exercise and nutrition, but seldom address sustainability and other core factors such as mental health and motivation. There are some exceptions. A holistic wellness programme named Spirited Life was implemented with a cohort of US clergy. This intervention included stress management, motivational interviewing, social interactions as well as a weight loss programme.20 It resulted in sustained weight loss after 3.5 years in participants with obesity.21 Another programme entitled ‘Health at Every Size’ is a weight-neutral approach focused on intuitive eating, self-acceptance and healthy behaviours rather than dieting and losing weight for women with different body sizes, and has been evaluated in a number of different countries and settings.22 Canadian researchers promote its use with Indigenous women, because labelling them obese implies that they are failing to improve their own health, and ‘Health at Every Size’ helps their ‘(re)connecting to cultural health’.23 Participants have been shown to have physical and mental health and quality of life improvements, but generally do not lose weight.24 Most studies of weight reduction programmes involving dietary changes and/or increased exercise show initial weight loss but this is not maintained, and by 5 years weight reduction is modest, or participants have regained their preprogramme weight.25 26 Connectedness, relationships, sharing and collaboration are fundamental Pacific and Māori cultural principles in which BBM is grounded.27 The value of an ethnic-led intervention that is characterised by ‘no excuses’, ‘no judgements’ and everyone helping each other, appear to contribute to the long-term sustainability of the programme.
Strengths of this project include the rich dataset from a diverse range of participants, independent coding with adjudication, and use of a Pacific theoretical framework for analysis. During the adjudication process there was generally consensus as to the codes assigned to each text, but coders chose different start and end points of quotes to illustrate a code, as well as the assigning of text under more than one code, due to overlapping and interdependent themes, which reduced the kappa value. Although some participants’ involvement had lapsed for a time, all participants were still engaged with BBM, and interviews with people who have discontinued their involvement might have given different insights.
We are now undertaking a quasi-experimental longitudinal quantitative cohort study with measured or self-reported weight at various time intervals for both general and the FTC members to evaluate the effectiveness of BBM for sustained weight loss and general health and well-being. Secondary outcomes for the From the Couch group will include clinical and biometric data for comorbidities including diabetes.
In summary, this qualitative study demonstrates that participants’ engagement in BBM, a grassroots, Pacific-led and Māori-led, voluntary organisation, addresses many components of their health and well-being beyond the core business of weight and diet management. For many, their involvement has been life-changing. The BBM model might be tailored to other communities, with the key being a ground-roots initiative embedded in, and embraced by, the people it serves.
Data availability statement
No data are available. The rich contextual data in this study is derived from interview transcripts and for ethical reasons it is not appropriate for these data to be shared for secondary analyses.
Ethics statements
Patient consent for publication
Ethics approval
The study was approved by the University of Auckland Human Participants Ethics Committee on 15 June 2020 for 3 years (Reference 24676).
Acknowledgments
We would like to acknowledge our three interviewers, Perpetua (Pepe) ‘Akau’ola, David Qaranivalu, Mia Loheni and our colleague from BBM, Fuatino Laban. Many thanks also to all our BBM interviewees who contributed their stories for this study. Ngā mihi nui, vinaka, fa’afetai lava, malo ‘aupito.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Correction notice This article has been corrected since it first published. In 'To cite' information author name has been updated to Savila F.
Contributors FS, FG-S, WB, MH, BS, DL, AB and FG-S were involved in conceptualisation and study design. FS, PL, FG-S and MH conducted the analyses. FG-S drafted the initial paper for publication. All authors contributed to the writing of the paper, and all have read and approved the final manuscript. FG acts as guarantor for this statement.
Funding This work was supported by a Health Research Council of New Zealand Activation Grant, Project number 20/1335. The funding body plays no role in the design of the study and collection, analysis, and interpretation of data nor in writing the manuscript.
Competing interests DL is the Founder and AB is the Marketing Communications Associate of BBM Motivation, and both are integral members of the research team. WB’s wife is a Pilates instructor at BBM. No other authors have any conflict of interest to declare.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.