Article Text

Abstract
Objectives To examine factors associated with declaration of disability by medical students and doctors, and the association of declared disability with academic performance.
Design Observational study using record-linked data collected between 2002 and 2018.
Setting UK Medical Education Database is a repository of data relating to training of medical students and doctors. Disability and other data are record-linked.
Participants All students starting at a UK medical school between 2002 and 2018 (n=135 930).
Main outcome measures Declared disability was categorised by the Higher Education Statistics Authority. Outcomes related to undergraduate academic performance included scores in the educational performance measure (EPM), prescribing safety assessment and situational judgement test. Performance in postgraduate examinations was studied, as well as prior attainment in school examinations and aptitude tests.
Results Specific learning disability (SLD) was the most commonly declared disability (3.5% compared with the next most commonly declared disability at 1.0% of n=129 345 all cases in the study), and during the period covered by the data, SLD declarations increased from 1.4% (n=6440 for students starting in 2002) to 4.6% (n=8625 for students starting in 2018). In a logistic regression, the following factors predicted recording of SLD on entry to medical school ((exp(B)±95% CI), p<0.0001 unless otherwise stated): attendance at a fee-paying school (2.306±0.178), graduate status (1.806±0.205), participation of local areas quintile (1.089±0.030), age (1.034±0.012). First year medical students were less likely to declare SLD if they were from a non-white ethnic background (Asian/Asian British 0.324±0.034, black/black British 0.571±0.102, mixed 0.731±0.108, other ethnic groups 0.566±0.120), female (0.913±0.059; p=0.007) or from a low index of multiple deprivation quintile (0.963±0.029); p=0.017. In univariate analysis with Bonferroni corrections applied for multiple tests, no significant difference was observed in the recording of SLD according to socioeconomic class (χ2=5.637, p=1), whether or not a student’s parents had a higher education (χ2=0.140, p=1), or whether or not a student had received a United Kingdom Clinical Aptitude Test (UKCAT) bursary (χ2=7.661, p=0.068). Students who declared SLD at some point in medical school (n=4830) had lower EPM normalised deviate values (−0.390) than those who did not (−0.119) (F=189.872, p<0.001). Those for whom SLD was recorded were as likely to complete the course successfully as those who did not declare disability (93.0% successful completion by those for whom SLD declared from year 1 (n=2480), 92.2% by those for whom SLD declared after year 1 (n=2350), 91.6% by those for whom SD not declared at any point (n=85 180)) (χ2=6.905, p=0.032). Of 3580 first year students who declared SLD, 43.1% had not sat the UKCAT Special Educational Needs aptitude test (which gives extra time for those with special educational needs), while 28% of 2400 registrants for whom SLD was recorded as medical students did not declare it at General Medical Council registration.
Conclusions Substantial increases in declaration of SLD may reflect changes in the social and legal environment during the period of the study. Those who declare SLD are just as likely to gain a primary medical qualification as those who do not. For some individuals, disability declaration appears to depend on context, based on differences in numbers declaring SLD before, during and after medical school.
- medical education & training
- health policy
- public health
Data availability statement
Data are available upon reasonable request. The dataset used in this study was acquired from the UK Medical Education Database and is held in the Safe Haven. Interested parties can apply to re-analyse the data used in this study. Data access requests must be made to UKMED. Full information for applications can be found at https://www.ukmed.ac.uk.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
We studied 135 930 medical students and junior doctors who started medical school between 2002 and 2018; our coverage is therefore both contemporary and comprehensive.
Disability data were linked with other data, allowing more detailed investigation than has previously been possible.
Disability, as declared by medical students to Higher Education Statistics Authority, is self-reported and therefore unverified for the purposes of this analysis.
Information on disability at postgraduate level is less detailed than at undergraduate level.
Introduction
Disability in medicine is an issue to which the profession has returned repeatedly over the years, with detailed pronouncements from the British Medical Association (BMA) (two, in 2007 and 2020),1 2 and the General Medical Council (GMC) (several, most recently in 2019).3–5 This enduring focus reflects the importance of the issue, but also profound changes in the social and legal environment during the same period. The 2010 Equality Act,6 which subsumed the 1995 Disability Discrimination Act7 (except in Northern Ireland), posited disability in a much wider context, designating it as just one of nine protected characteristics, the others being age, gender reassignment, marriage and civil partnership, pregnancy and maternity, race, religion or belief, sex and sexual orientation. The conducts prohibited under the Act include discrimination, victimisation and harassment, but it is discrimination—specifically, the fear of being accused of it—which most preoccupies medical schools, postgraduate deaneries and National Health Service (NHS) trusts, the key providers in the UK of training of medical students and doctors. The GMC, like other regulatory agencies, has sought to reposition itself and the profession in relation to disability. The need to do so is not merely driven by legislation. According to Welcomed and valued,5 only 1% of junior doctors responding to the national training survey declare disability, compared with an estimated prevalence of disability in adults of working age of 19%.8
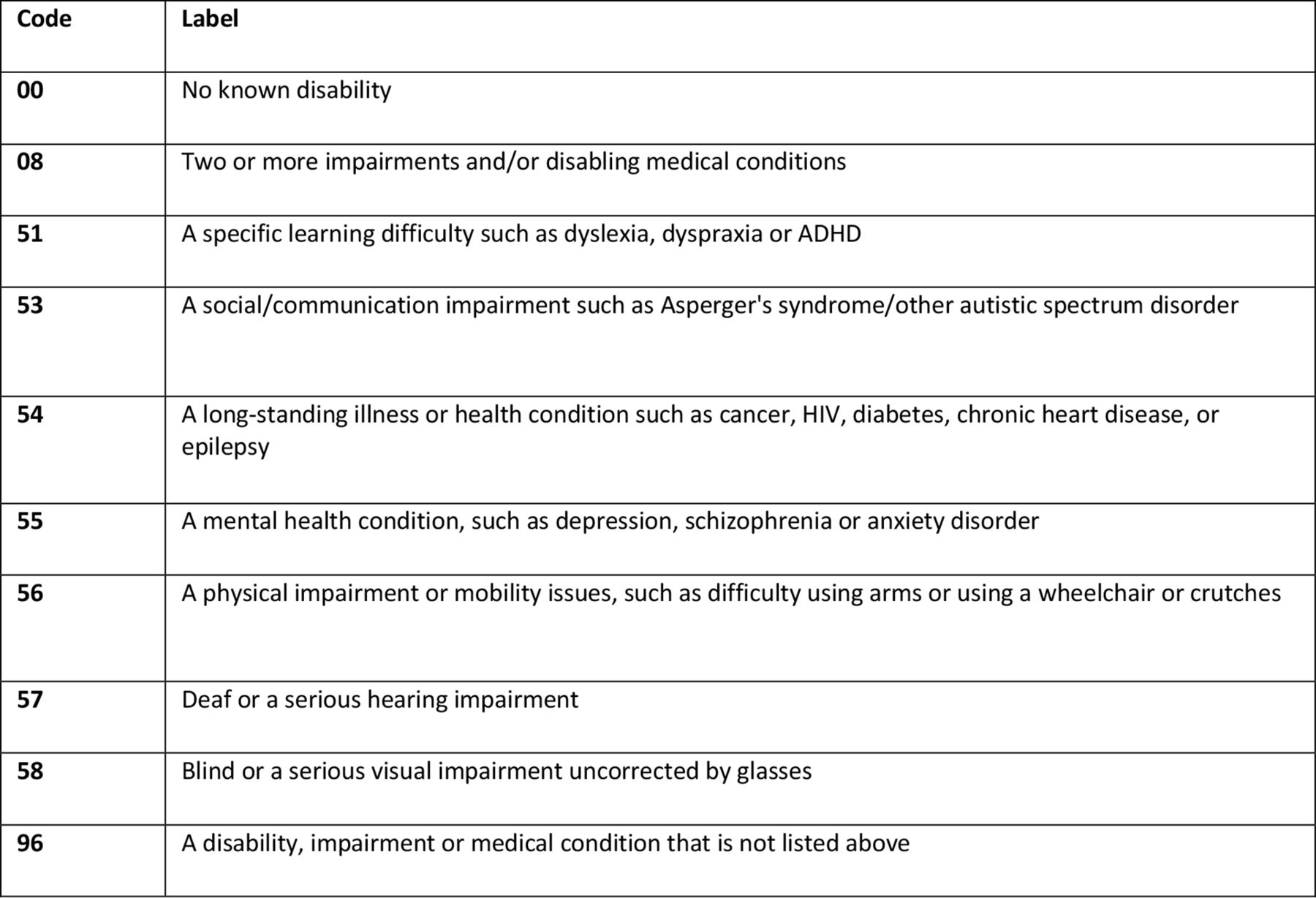
The Equality Act defines disability as a physical or mental impairment that has a substantial and long-term adverse effect on the ability to carry out normal day-to-day activities.6 The constructive ambiguity of this wording has been highlighted.9 Interpretation of the Act in practice is exclusively done at institutional level by disability services. Outcomes of disability assessments are categorical, with the individual labelled as either disabled or not; impairments are specified as per the classification of the Higher Education Statistics Authority (HESA) (figure 1). Medical students thus declare disability within a fixed framework over which they have no control. Once disability is declared, the disabled label usually ‘sticks’, at least until graduation. For example, few students who declare a specific learning disability (SLD) (the most common declared disability) ‘undeclare’ themselves subsequently before gaining their primary medical qualification. At postgraduate level, in contrast, junior doctors are able to choose a specialty that suits them, for example, individuals with visual impairments may avoid specialties that rely heavily on, say, microscopy. In doing so, they are unwittingly applying a more flexible, interactive model of disability,10 used by the World Health Organization (WHO), the interaction being between impairment(s) and activities (educational and/or clinical). This definition does not see disability per se as the problem; rather, the problem is the interaction between the impairment and the activities and/or environment.
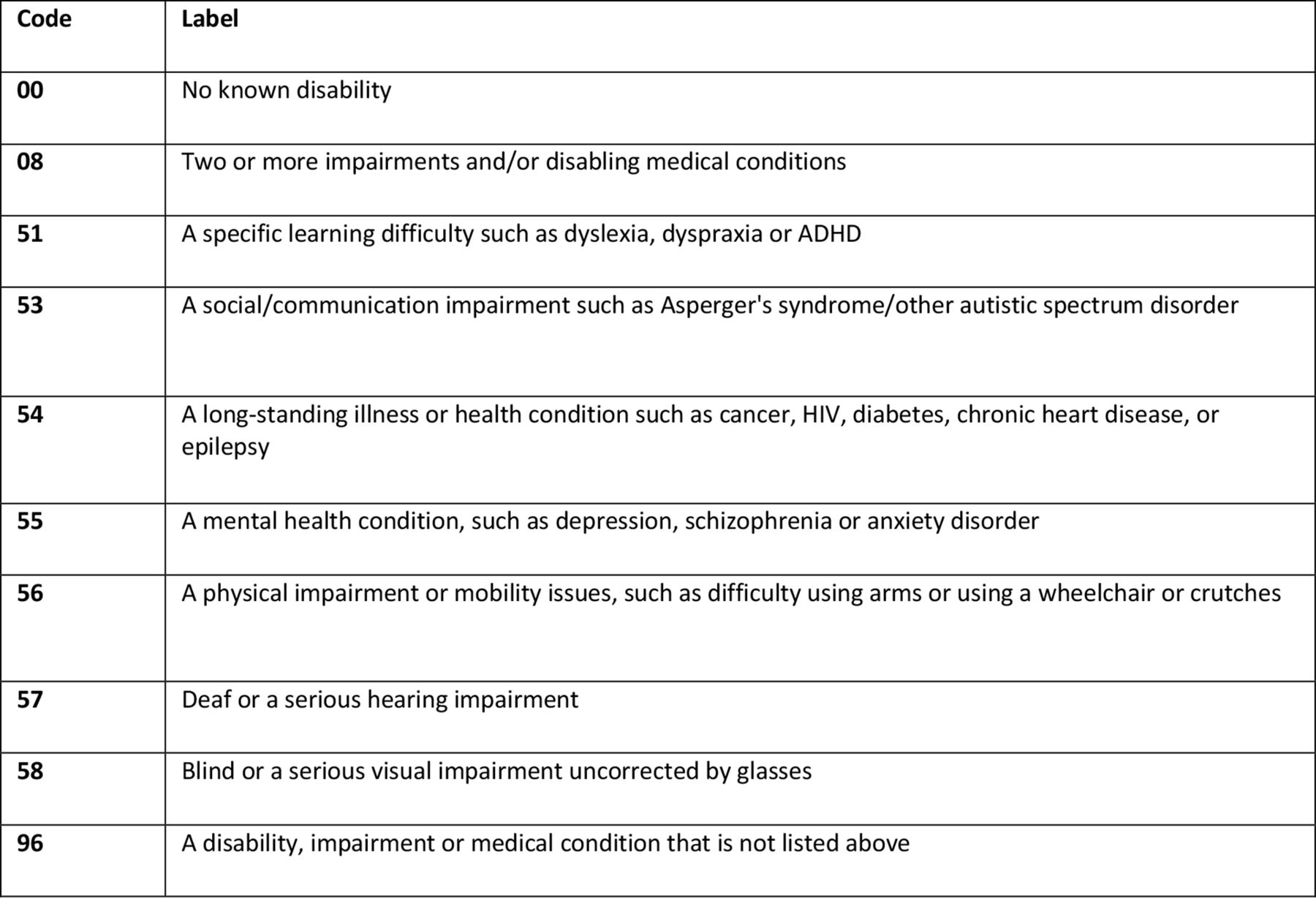
Classification of declared disability in higher education by the Higher Education Statistics Agency. ADHD, attention deficit hyperactivity disorder.
This difference in the ‘declaring environment’ between undergraduate and postgraduate spheres may help to explain why disability is much more likely to be declared by medical students, compared with doctors in training (quoting again from Welcomed and valued, 9% of medical students declare disability).5 Consistent with this interpretation, 9% of newly-registered doctors—who, like medical students, have not yet reached the stage of choosing their postgraduate specialty—declare disability.5 It may also explain how, in the past, rigid adherence to the requirement for certain physical competencies to be achieved by all medical students meant that disability could preclude the study of medicine but not its practice.11 The illogicality of this position has been recognised by the GMC. In the 2009 edition of Tomorrow’s Doctors,12 learners are required to provide cardiopulmonary resuscitation or direct other team members to carry it out (italics indicate the amendment from the previous edition). Shrewsbury provides a comprehensive examination of the curriculum outcomes in Tomorrow’s Doctors 2009 from the perspective of disability.9 In Welcomed and valued, the original position has been fully reversed: ‘no health condition or disability by virtue of its diagnosis automatically prohibits an individual from studying or practising medicine’.5
The impact of changes in curriculum outcomes on the declaration of disability by medical students is unclear. Leaving aside disabilities that ‘declare themselves’, for example, mobility impairments that require use of a wheelchair, in other cases, like specific learning difficulties or mental health conditions, declaration of disability represents a calculation of the relative advantages and disadvantages of doing so. Failure to declare may reflect a perception, justified or not, that the disadvantages outweigh the advantages. For example, applicants may worry that their chances of being admitted to medical school may be jeopardised by declaring disability. Equally in other cases, the opposite calculation may be made—that, say, getting extra time in summative assessments (the most common accommodation) may confer an increased likelihood of progressing. However, limited information is available on the factors that are associated with declaration of disability, or the association between declared disability and academic performance. The recent establishment of the UK Medical Education Database (UKMED), a repository of record-linked datasets hosted by the GMC, permits more detailed investigation than has previously been possible. In the current report, we have explored the UKMED datasets to address these and other questions.
Methods
Study population and design: student data
All data used in the analyses were obtained from UKMED and were anonymised as per the UKMED research process.13 The data definitions are given in the UKMED data dictionary,14 which categorises, defines and summarises all data held in the UKMED database. The study population consisted of all students starting at a medical school in the UK between 2002 and 2018. Cases where the first available year of programme or year of study was greater than one, and cases with no identifiable course type, were excluded. Data were available for 129 345 individuals. Flow of data is shown in figure 2.

{kind=link}
{kind=link}
The flow of data through the study. GMC, General Medical Council; HESA, Higher Education Statistics Authority; PG, postgraduate; PMQ, primary medical qualification; SLD, specific learning disability; UG, undergraduate.
Data on medical school processes
In conjunction with the Medical Schools Council (MSC), we surveyed UK medical schools on their approach to identifying and supporting students with SLDs. Data collection was interrupted by the outbreak of COVID-19; we received returns from 18 of the 38 medical schools with HESA data.
Categorisation of declared disability
Declared disability was self-reported by students to medical schools using categories defined by HESA, as shown in figure 1. Categories included two or more disabilities and/or disabling medical conditions, and a disability, impairment or medical condition that is not otherwise listed.
United Kingdom Clinical Aptitude Test and United Kingdom Clinical Aptitude Test Special Educational Needs
The United Kingdom Clinical Aptitude Test (UKCAT) (now called University Clinical Aptitude Test) is a cognitive skills test undertaken by the majority of applicants to UK medical schools. It allows extra time for applicants who are able to provide a letter from their school, college or university which confirms and provides the basis for their entitlement to this in examinations (diagnosis from, eg, medical practitioner, educational psychologist, specialist teacher). Applicants who satisfy this requirement may sit UKCAT Special Educational Needs (UKCATSEN),15 and are given 25% extra time. Scores analysed in the current report were all based on first attempt.
Academic performance and progression
The relationship between SLD and academic performance was studied by examining scores in the educational performance measure (EPM), prescribing safety assessment (PSA) and situational judgement test (SJT).
Separately, we analysed available HESA data on academic progression according to declaration of SLD in first year or subsequently. HESA records reasons why students have left their medical course (for the vast majority it is successful completion of the course and graduation).16 Code 02 (HESA RSNEND Code 2) is ‘academic failure/left in bad standing/not permitted to progress’. According to HESA, this is considered to be different from simply dropping out, which is coded separately, and which may be more closely related to personal reasons. Code 02 is applied specifically to students whose progression is limited or interrupted by failure in assessments. In the current report, Code 02 status was recorded irrespective of whether the student was subsequently readmitted to the course; medical schools submit data to HESA prior to academic appeals, and so it is possible for a student to be readmitted despite being categorised as Code 2.
Educational performance measure
Since 2013, applicants to postgraduate foundation programmes have been ranked within their year cohort into deciles of educational performance. This forms one component of the EPM. The EPM comprises two elements: medical school performance in deciles, for which 34–43 points are available, and educational achievements, which are worth up to 7 points. A maximum of 50 points can be awarded for the EPM.17 Assessments included in the EPM must meet specific criteria. Individual medical schools decide which assessments to include in the score, after consultation with students, and are required to publish these assessments on their websites. In 2012, applicants were ranked in quartiles. In order to combine data from 2012 and subsequent years in a single analysis, EPM quartiles and deciles were converted into normalised deviate values, using the method of devised by Garrud and McManus.18
Prescribing safety assessment
The PSA was developed jointly by the British Pharmacological Society and the MSC as a way for students to demonstrate competence in the safe and effective prescribing of medicines. First delivered in 2014, it was formative in 2014 and 2015. Since 2016, passing the PSA has been required for progression to the second foundation year (FY2). PSA data include a record of whether the candidate was given extra time. The analyses in the current report use z scores calculated from the mean and SD of all attempts at the PSA in the given calendar year. PSA performance data were based on first attempts only.
Foundation programme situational judgement test
The SJT is part of the selection process for entry to the Foundation and Academic Foundation programme. It is a computer-based assessment designed to assess some of the essential competences outlined in the national person specification and is based around clinical scenarios. Its purpose is to target key attributes in the person specification including patient focus, commitment to professionalism, coping with pressure, effective communication and team working. The SJT presents applicants with a series of work-related situations and asks them questions about how they would respond to these situations. These questions take multiple formats such as multiple choice and ranking. The SJT raw score was converted into a z score, based on the published mean and SD from the technical report for the applicable year. We used the final SJT score—that is, the one associated with admission to the foundation programme. The total z score was the mean of z scores from different years; this explains why it is not 0. We do not have information about whether or not candidates sitting the SJT received adjustment/extra time.
Statistical methods
HESA statistical control rounding rules are applied throughout this report.19
IBM SPSS Statistics V.27 (IBM United Kingdom) was used to perform the statistical analyses listed below.
Univariate analysis was used to evaluate HESA recording of SLD in relation to each of the following variables: gender, ethnicity, domicile, school type, graduate status, socioeconomic category, index of multiple deprivation (IMD), participation of local areas in higher education (POLAR), parental possession of a higher education qualification.
Logistic regression analysis was performed to predict HESA recording of SLD, using variables that reached significance in the univariate analysis above.
Cohen’s kappa coefficient was used to express the agreement: between (1) HESA-recorded SLD in the student’s first year and whether or not the student had sat the UKCATSEN (this coefficient was also calculated separately for each medical school); (2) HESA-recorded SLD at any time during medical school and declaration of SLD at GMC registration.
Cohen’s d coefficient was used to estimate the effect size of: (1) HESA-recorded SLD and/or extra time on PSA score; (2) HESA-recorded SLD on SJT score; (3) HESA-recorded SLD in first year and/or extra time (UKCATSEN) on UKCAT total score; (4) HESA-recorded SLD on prior school performance. The benchmarks suggested by Cohen were used to evaluate small (d=0.2), medium (d=0.5) and large (d=0.8) effect sizes.20
Pearson’s χ2 test was used to evaluate the relationship between (1) HESA-recorded SLD during or after first year, and HESA RSNEND Code 2 (see above); (2) HESA-recorded SLD at medical school and successful completion of the course resulting in a primary medical qualification.
Patient and public involvement
Neither patients nor the public were involved in the design, conduct, reporting, or dissemination plans of our research.
Results
Factors associated with declaration of disability
Recording of SLD increased significantly over the period of the study; recording of physical/hearing/visual impairments much less (table 1). In univariate analysis of factors potentially associated with declaration of SLD in first year, no significant difference was observed in the recording of disability by socioeconomic class, by whether or not a student’s parents had a higher education, or by whether or not a student had received a UKCAT bursary (online supplemental tables S1 and S2). On this basis, these variables were not included in subsequent logistic regression analysis, in which the following factors were predictive of recording of SLD in first year: chronological year of entry into medical school, age in year of admission to medical school, male sex, graduate status, attendance at a fee-paying school, high POLAR quintile. Compared with white ethnicity, students from other ethnic groups were less likely to declare disability, as were students from a lower IMD quintile. These results are summarised in online supplemental table S3, which also includes variation by medical school and course type.
Supplemental material
Higher Education Statistics Authority (HESA)-declared disability in UK medical schools by chronological year
Association of disability with academic performance at medical school
Educational performance measure
Online supplemental figure 1 summarises EPM normalised deviate scores according to declaration of SLD. Students who declared SLD at some point in medical school had lower EPM normalised deviate values than who did not: −0.390 (N=3575) versus −0.119 (N=49 590), F=189.872, p<0.001.
Supplemental material
Prescribing safety assessment
We identified four groups according to whether or not SLD was recorded and/or extra time was granted in the PSA at the end of training. Performance of these groups is compared in online supplemental table S4. The differences observed reached statistical significance but were mostly small.
Foundation programme SJT
Online supplemental table S5 summarises the SJT score by recorded SLD. SJT data were available on all those applying for foundation posts from 2013 through to 2020. Although the difference was statistically significant, the effect size was below what Cohen classifies as small.
Academic progression and completion of course
Students who had SLD recorded after starting medical school (ie, recorded in a subsequent year of study but not in first year) were more likely to have failed to progress due to academic failure than those who had no record of SLD, or those who were recorded as having SLD in their first year of study (table 2). This suggests that investigations into whether a student has a SLD are undertaken in response to academic failure. Our survey of medical schools confirmed this; 11 out of 18 respondents indicated that screening for SLD is undertaken in response to academic performance issues. Only one indicated that they proactively tried to identify students with SLDs.
Recording of HESA RSNEND Code 2 relating to failure to progress, according to declaration of specific learning disability (SLD) in year 1 or subsequently
Table 3 summarises the successful completion of the course according to declaration of SLD. Those who declared SLD were at least as likely to complete the course successfully as those who did not (differences were statistically significant, but small). We did not examine whether students declaring SLD took longer to complete their medical course. The expected length of time taken to complete the course varies by student according to, among other things, whether an intercalated degree is taken (optional in some schools and compulsory in others).
Successful completion of primary medical qualification (PMQ) according to declaration of specific learning disability (SLD) in year 1 or subsequently
Association of disability with academic performance before and after medical school
Before
Scores to measure prior educational attainment—at A-Level, Scottish Higher and General Certificate of Secondary Education (GCSE)—were derived using the method previously used by McManus et al.21 Online supplemental table S6 shows lower scores in those for whom HESA-declared SLD was recorded during medical school, but the differences were mostly small.
Those who sat UKCATSEN obtained significantly higher UKCAT total scores than those who did not, regardless of whether they declared SLD in their first year. Those who did not sit UKCATSEN and declared SLD in first year had the lowest mean score of the four groups (online supplemental table S7). The difference in UKCAT scores between highest and lowest-scoring groups corresponds to approximately two deciles of performance, based on UKCAT data.
After
Mean college membership examination marks of those with HESA-recorded SLD as medical students were compared with those with no SLD recorded. The analysis was restricted to first attempt examinations where at least 50 cases with SLD were recorded. However, examination data were left censored; collection by the GMC did not commence until 1 August 2013 and it was possible for those in the UKMED population to have taken examinations from 2008. Small or trivial differences were seen for written examinations (consistently around 0.3) and clinical examinations (Practical Assessment of Clinical Examination Skills (PACES) and Clinical Skills Assessment (CSA)) (below 0.2). The differences are not reliable for exams with fewer than 120 cases (the CI on Cohen’s d cross 0) (online supplemental table S8). UKMED does not hold data on whether the examination candidates received extra time.
Agreement in declaration of disability on entry to and exit from medical school
Entry
The agreement between recording in first year of SLD and sitting UKCATSEN was examined. Of 3580 students who declared SLD to HESA in first year, 56.9% sat UKCATSEN. Of 2615 successful applicants who sat UKCATSEN, 22.0% did not declare SLD to HESA in first year. Cohen’s kappa coefficient was 0.646 (N=87 455). We calculated the kappa for agreement between UKCATSEN and HESA separately for each medical school. The lowest was 0.337 at Leicester (N=2885) and the highest was 0.802 at Newcastle (N=3010).
Exit
Seventy-two per cent of 2400 registrants who had SLD recorded at some point during medical school declared SLD when they registered with the GMC. Nine per cent of those who did not have SLD recorded at any point during medical school (N=30 270) declared SLD on registration. Kappa for agreement: 0.791, N=32 670. By medical school, lowest kappa was 0.698 (Buckingham, N=120); highest 0.903 (Leeds, N=1135). The variation in recording across schools on exit when compared with GMC recording appears to be lower than that on entry between HESA and UCAT.
Discussion
It is over 25 years since the landmark enactment of the Disability Discrimination Act in 1995. In the intervening years, government agencies and organisations like HESA and the GMC have collected and published data relating to disability. Although these have, for example, established trends, more detailed questions require linkage of disability status and other data, and it is only recently that this has become possible on a meaningful scale with the establishment of UKMED.14 The current report is the first to apply this powerful tool to the investigation of disability in medicine. We have examined the factors associated with the declaration of disability, and the association of disability with academic performance before, during and after medical school. We provide the most detailed account to date of what is known about declared disability in medical students and junior doctors in the UK.
The HESA categorisation of disability used by all UK medical schools gives specific form to the generic definition found in the relevant legislation.6 7 It is explicitly comprehensive (its final category is ‘a disability, impairment or medical condition that is not covered above’) and embraces both physical and non-physical disabilities, including a ‘specific learning disability such as dyslexia, dyspraxia and attention deficit hyperactivity disorder (ADHD)’. SLD was the most commonly declared disability throughout the study. At the end of the study period, in 2018, 4.6% declared it, compared with 1.8% declaring the next most commonly declared disability (a mental health condition); moreover, it increased more than threefold during the study period, from 1.4% in 2002. Declaration of mental health conditions also increased, particularly in the last few years. In contrast, declaration of blindness and deafness remained unchanged during the period of the study, and although declaration of physical impairment/mobility issues increased from 0.1% to 0.3%, it too remained at a low level throughout. Thus, SLD in particular may act as a ‘bellwether’ of disability declaration, responding to changes in the social and legal environment during the period of the study.
Notwithstanding these changes, doctors and medical students still perceive their working environment to be comparatively hostile to the declaration of disability. More than three-quarters of respondents to the 2020 BMA survey2 indicated that they were worried about being treated unfavourably if they disclosed a disability or long-term health condition to their employer or place of study. In the current report, specific groups less likely to declare included those who were younger, women, from a non-white ethnic background, or school-leavers. Interestingly, socioeconomic class and parental higher education status did not predict declaration, although attendance at a fee-paying school did. The ongoing existence of real and perceived discrimination22–25 may help to explain why some groups are less likely to declare SLD than others. There is also evidence of avoidance26 and altered healthcare-seeking behaviour27 in people with disability; in this context, not declaring SLD might be viewed as analogous. Certainly, some of the same factors are associated with each for example, age and sex; young people find it challenging to disclose disability.28
Perceived hostility of the clinical environment may also help to explain why 28% of those recorded as having SLD as medical students did not declare it when registering with the GMC. The transition from medical student to junior doctor marks a critical career point, and the associated uncertainty and anxiety associated with the change in role may precipitate different declaring behaviour. The opacity of the registration process itself may not help. Indeed, respondents to the BMA 2020 survey confirm this:
‘Applicants [for GMC registration] can be asked to provide a range of detailed and potentially sensitive health information about themselves. However … it is not always clear to them why particular information is required, or how this will be used to determine their fitness to practice. This uncertainty can cause considerable anxiety for some disabled applicants. These responses suggest that greater clarity around this process may reassure disabled applicants that they will receive the support they need to successfully pursue their medical careers’.2
Altered declaring behaviour at GMC registration may be part of a wider, transition-related, phenomenon. Consistent with this, the previous critical career transition—from applicant to medical student—was also associated with altered behaviour, although in the reverse direction; just over half of students who HESA-declared SLD in first year had sat UKCATSEN as applicants, even though published UKCAT scores were higher in those who sat UKCATSEN. It may be that having matriculated, medical students are less apprehensive about declaring SLD than they were as applicants at the outset of their highly competitive selection journey to medical school.
Medical students might be less apprehensive still about declaring SLD if they knew that those who do so are just as likely to complete the course successfully as those who do not. Although scores in academic performance outcomes like EPM, PSA and SJT were lower, the observed differences were small, and academic progression was similar in students for whom SLD was recorded in first year, and in those for whom it was not declared at any point. The finding that those for whom SLD was recorded subsequently (ie, after first year) were more than twice as likely to have failed to progress due to academic failure may simply reflect the fact that academic failure is often a trigger for investigations into whether a student has SLD. Crucially, this specific group was also just as likely to complete the course and gain a primary medical qualification. (It is counterintuitive that a group more likely to fail are just as likely to complete the course successfully, but this juxtaposition does not take into account the length of time taken to complete the course.) Another recent study has documented poorer performance in students with cognitive/learning disability compared with matched controls, as well as a measurable impact of accommodation on academic performance.29
Comparative attainment before and after medical school is much harder to interpret based on available data. Although we found only small differences in performance according to recording of HESA-declared SLD during medical school, we do not have data on SLD declaration and/or granting of extra time in school examinations. In addition, only successful medical school applicants were compared—no meaningful conclusion can be drawn about the wider impact of declared SLD on performance in school examinations. Similarly, at postgraduate level, differences in performance by declaration of SLD at medical school were small, but interpretation is bedevilled by the caveats outlined previously.
Implications for stakeholders
Stakeholders in the medical training of disabled colleagues are many and varied. They include disabled individuals themselves (as applicants, medical students and doctors), organisations tasked with their training and/or its regulation (medical schools, postgraduate deaneries, NHS trusts, the GMC), as well as the wider medical and health professional workforce (including other groups experiencing discrimination) and society in general (patients, including disabled patients, policy-makers and researchers). Our key findings will be of interest to all of these. The substantial increase in the declaration of SLD during the study period, combined with its apparent dependence on context, based on differences in numbers declaring at key transition points, provides evidence that it may act as a bellwether for disability declaration. Its sensitivity to influencing factors and context confers an indicative role of importance to all, and is partly why it has been the principal focus of the current report.
While attendance at a fee-paying school predicted recording of SLD in first year, socioeconomic class, and parental higher education did not, suggesting that schools play a more important role than the stereotypical ‘pushy parents’ of yore. The discrepancy between the numbers sitting UKCATSEN and declaring SLD in first year raises the possibility of underidentification of SLD by schools, further underscoring the importance of their role. Further research is required to establish the feasibility of identifying and extrapolating good practice across the sector; in particular, if early identification has the same effect on academic performance at school as it appears to have at medical school (see next paragraph).
Our finding that those for whom SLD was recorded—at any point—were as likely to gain a primary medical qualification as those for whom it was not will be of substantial interest to medical students, medical schools and policy-makers alike, suggesting that the adjustments made, for example, extra time in examinations, may broadly achieve their aim of reducing the disadvantage incurred by the disability. The findings summarised in table 2 indicate a smoother path to graduation for those declaring SLD from first year, compared with those declaring subsequently; the latter were more than twice as likely to have failed to progress due to academic failure. This raises the intriguing possibility that early identification of SLD might ensure a less ‘bumpy ride’ to graduation. Proactive identification is likely to be resource intensive, suggesting that a pilot may be required to establish the value and impact of doing so.
There is a dearth of detail on disability at postgraduate level, compared with undergraduate recording by HESA, and a host of questions that remain unanswered. We do not know, for example, how disability declaration varies by specialty, region or phase of training, or how it relates to perceived hostility of the workplace; or what relationship there is between disability declaration and performance, including (but not exclusive to) postgraduate examinations; or indeed if those who declare disability in postgraduate examinations also declare it in their workplace. As a first step, the GMC may wish to review the registration process, given the feedback articulated earlier.2 This alone will not address these questions, and policy-makers in particular may wish to review the detail of disability data collected in the workplace.
Conclusion
A substantial increase in declaration of SLD was observed between 2002 and 2018. This period encompassed the enactment of the 2010 Equality Act, and the introduction of assessments with national reach (EPM, PSA, SJT). We found that those who declare SLD are just as likely to gain a primary medical qualification as those who do not. We also found that the transitions, from applicant to medical student, and from medical student to foundation doctor, were associated with substantial differences in SLD declaration, suggesting that for some individuals, disability declaration may depend on context.
Several factors limit the conclusions that can be drawn. First, HESA-declared disability is self-reported and therefore unverified at the point of declaration. Second, numbers declaring disabilities other than SLD were comparatively small, limiting their amenability to similar statistical treatment. Third, the lack of detail on disability at postgraduate level leaves many unanswered questions. However, this is the first study to attempt to ‘map’ disability in medicine in the UK. Our coverage is contemporary and comprehensive, and our findings will inform current and future policy, as well as guiding research in this area.
Data availability statement
Data are available upon reasonable request. The dataset used in this study was acquired from the UK Medical Education Database and is held in the Safe Haven. Interested parties can apply to re-analyse the data used in this study. Data access requests must be made to UKMED. Full information for applications can be found at https://www.ukmed.ac.uk.
Ethics statements
Patient consent for publication
Acknowledgments
Data source: UK Medical Education Database (“UKMED”) UKMEDP054 extract generated on 27 November 2020. Approved for publication on 25 June 2021. We are grateful to UKMED for the use of these data. However, UKMED bears no responsibility for their analysis or interpretation. The data includes information derived from that collected by the Higher Education Statistics Agency Limited (“HESA”) and provided to the GMC (“HESA Data”). Source: HESA Student Record 2002/2003 to 2018/2019; Copyright Higher Education Statistics Agency Limited. The Higher Education Statistics Agency Limited makes no warranty as to the accuracy of the HESA Data, cannot accept responsibility for any inferences or conclusions derived by third parties from data or other information supplied by it.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @mjmbiochem
Contributors MJM: conceptualisation, investigation, methodology, writing—original draft. JSD: conceptualisation, investigation, methodology, project administration, validation, writing—review and editing. DTS: data curation, formal analysis, investigation, methodology, project administration, software, validation, writing—review and editing. MJM is the guarantor and is responsible for the overall content.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests All authors have completed the Unified Competing Interest form (available on request from the corresponding author) and declare their competing interests as per below. Otherwise, there is: no support from any organisation for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years, no other relationships or activities that could appear to have influenced the submitted work. Michael Murphy: no competing interest declared. Jon Dowell: UKMED Advisory Board member and chair of the UKMED research group. Daniel Smith is employed by the GMC as data analyst working on the UKMED project.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.