Article Text

Abstract
Objectives It has been hypothesised that smoking intensity may be related to occupational stress. This study aimed to investigate whether stress, including problems with superiors or co-workers, is a driver of smoking.
Design Cross-sectional study.
Setting and participants 59 355 employees (34 865 men and 24 490 women) across multiple occupations who completed a self-reported questionnaire-based occupational stress survey between April 2016 and March 2017 in Niigata Prefecture.
Main outcome measures Stress scores for the Brief Job Stress Questionnaire subscales summed up after assigning high points for high stress and converted to Z-scores based on the mean of all participants. Heavy smokers (HS) smoked ≥15 cigarettes/day and light smokers (LS) smoked <15 cigarettes/day and were compared with non-smokers (NS) by gender.
Results The main subscale items that were significantly associated with smoking status in both genders included ‘physical burden’, ‘irritation’ and ‘physical symptoms’. In the analysis that included smoking intensity, the stress score for ‘co-workers’ support’ was significantly lower for LS men than NS men (NS 0.091±0.98, LS −0.027±1.00, HS 0.033±0.99), and was significantly higher for HS women than NS women (NS −0.091±1.00, LS −0.080±1.05, HS 0.079±1.03). However, the stress score for ‘co-workers’ support’ was low among LS women aged ≤39 years in the manufacturing industry.
Conclusions It was speculated that LS men and some LS women gained ‘co-workers’ support’ using smoking as a communication tool while reducing the degree of smoking. The existence of such ‘social smokers’ suggested that to promote smoking cessation, measures are essential to improve the communication between workers in addition to implementing smoking restrictions in the workplace.
- mental health
- occupational & industrial medicine
- public health
- preventive medicine
Data availability statement
No data are available. Individual participant data for this article, including study protocols, are not available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
The strength of this study is that it is one of the largest comprehensive surveys of more than 50 000 employed individuals in East Asia and describes a wide range of components of occupational stress, including support by superiors or co-workers.
In addition to a simple comparison of smokers and non-smokers, we compared heavy smokers and light smokers separately to clarify stress factors characteristic of women who are heavy smokers and men who are light smokers, which has not been well studied.
We have included industry-specific surveys to clarify conditions of support by co-workers according to smoking rates in workplaces.
A limitation of this study is that it was a cross-sectional study and therefore causal relationships could not be identified.
Introduction
Smoking is a personal health problem that presents a significant risk for conditions such as malignancies and cardiovascular and respiratory diseases and is a serious public health challenge, such as workplace secondhand smoke and work productivity issues.1–4 Most studies that include smoking and occupational stress consider both as risk factors for non-communicable diseases and unfavourable habits such as those related to alcohol drinking, overeating and exercise. Only a few studies have focused directly on the relationship between smoking and occupational stress.5–9 Since the serious health hazards of smoking have become recognised, the smoking rate among Japanese men has decreased year by year, although it is still high worldwide and the smoking rate among women remains flat.10 11 Under these circumstances, the revised Health Promotion Law was fully enforced in Japan in 2020. This law stipulates that ‘premises of public facilities such as hospitals and schools are non-smoking, commercial and industrial facilities such as offices and restaurants are non-smoking in principle, and in case of violations, a penalty of 500,000 yen or less’ will be enforced. However, in existing small-scale restaurants or bars, smoking bans are not enforced, and exceptions are allowed as a transitional measure, which makes this a slightly loose regulation.12
Research on the backgrounds of smokers in Japan has been reported in recent years, mainly on educational disparities13 14 and industry differences.15 Although there are few academic studies published in English addressing why Japanese workers continue to smoke or why they are unable to quit, in general, many smokers cite ‘stress’ as a reason.16 17 Although it was not a study of reasons for smoking, a recent Japanese survey of the general public that included those who were not working reported an association between smoking intensity and ‘serious psychological distress’ in women.18 In addition, a market research company (Cross Marketing, Tokyo, Japan)19 conducted a survey on reasons for smoking and found that ‘stress’ was cited by 40.4% of smokers as the main reason for smoking in Japan.
There are multiple aspects to occupational stress, and various stress models have been developed to elucidate causal associations with occupational stress. Among them, workload (job demand) and work discretion (job control) are widely accepted as representative causes.20 21 In addition, workplace relationships are important as a buffer against stress. The demand-control-support (DCS) model, which adds support from co-workers and supervisors to demand and control, is mainly used to investigate the association between cardiovascular disease and work stress in research.22 23 In recent years, the DCS model and indicators such as workplace social capital or organisational justice have been used to investigate workplace support, but the relationship between smoking and these stress indicators is still controversial.
For example, Kouvonen and colleagues reported that lower ‘job control’ was associated with increased smoking intensity among civil servant women in Finland while no such association was found in men.7 In a study of Japanese men in a single workplace, Kawakami and colleagues suggested that the intensity of smoking increased in Japanese men in a group with low job control and low social support.8 Fukuoka et al tracked the outcome of smoking cessation for 2 years and reported no association between stressors and continued smoking cessation in a similar group of male Japanese workers.24 Studies using other indicators also found that ‘low confidence in workplace organizations’ was associated with smoking,9 and ‘poor trust relationship with superiors’ was associated with smoking in women managers.5 On the other hand, the opposite result was reported where ‘good workplace support’ was associated with smoking among women in the nursing profession.25 Although it has been reported that ‘social connections’ are involved in both smoking and smoking cessation,26 other conditions, such as related to workplace environment or duties, might be required for social support to help control smoking.
Because of the very limited number of large-scale comprehensive studies on a variety of industries in the East Asian region, where smoking rates are known to be high, no consistent conclusions can be drawn on the association between various occupational stresses, such as lack of workplace support, and smoking. Therefore, we administered a detailed occupational stress survey, including smoking intensity and workplace support, to approximately 60 000 employees from industries of different sizes and categories to determine the relationship between smoking intensity and occupational stress and differences in the relationship by gender, age and industry.
We hypothesised that smokers experience more occupational stressors than non-smokers (NS), and that the greater the stress, the higher the intensity of smoking. We also hypothesised that better workplace support would buffer stress and suppress smoking. To test these hypotheses, we compared the stress scale of NS, light smokers (LS) and heavy smokers (HS) by gender. Since supportive environments in the workplace vary according to the age of workers and industry, we added comparisons by age group and industry group. Therefore, through our results we could identify measures to promote smoking cessation by reducing working smokers’ stress and improving the work environment.
Methods
Survey participants
Among 64 279 employees who underwent an occupational health examination and stress check based on the Occupational Safety and Health Act between April 2016 and March 2017 in Niigata Prefecture, 34 865 men (mean age 41.8 years old) and 24 490 women (mean age 41.9 years old) participated in this study. Excluded were employees whose gender was unknown, had incomplete examination data, an incomplete stress check response or were ≤19 or ≥70 years old. The industry type was classified according to a large number of persons working at seven occupations and a smaller number of workers in an eighth category designated as ‘other’.
Also, in this survey participants were limited to workers at establishments in and around Niigata Prefecture; thus, participants were not representative of workers nationwide.
Patient and public involvement
Patients were not involved in this study.
Stress check
The 57-item ‘Brief Job Stress Questionnaire’ (BJSQ) developed and validated by Shimomitsu and colleagues was used to assess occupational stress.27 It has been used in previous studies as well as in workplaces across the country by the Ministry of Health, Labour and Welfare in guiding the Stress Check Program.28 The purpose of this programme was to assess stress in individual workers and in the work environment, and its results were reported to be associated with long-term leave and turnover of workers.29 30 Participants were required to answer questions on the BJSQ using a Likert scale of 1–4 points. The BJSQ contains several related questions, and the scores of the individual questions are added together to produce a result for each category. The total score for each category resulted in high points for high stress (simple total score). Question content was broadly divided into three components: ‘Job Stressors’, ‘Mental and Psychological Stress Reactions (‘Stress Reaction’)’ and ‘Social Support’. ‘Job Stressors’ has nine subscales (job demands, job control, meaningfulness of work, work environment, suitability for work, physical burden, skill utilisation, required job quality, interpersonal relationships), and ‘Stress Reaction’ has six subscales (vigour, irritation, fatigue, anxiety, depression, physical symptoms). Originally, ‘Social Support’ included four subscales (superiors, co-workers, family and/or friends (family), life satisfaction), but ‘life satisfaction’ was excluded because it was not related to support resources. Its elimination left three subscales. Scores were tabulated for each of these three components and 18 subscales.
These simple total scores were compared and examined using Z-score values (Z-scores) standardised from the average score of participants for each component or each subscale. Results with reference to the simple total scores are presented in online supplemental table 1.
Supplemental material
Smoking status and intensity
Information on smoking status (smokers or NS) and the number of cigarettes smoked per day was obtained from the medical check-up questionnaire. Based on the median number of cigarettes smoked in the all smokers (AS) group, we defined those who smoked <15 cigarettes/day as LS and those who smoked ≥15 as HS. In the LS, HS and NS groups, the distribution of chronological age was calculated in 10-year increments and the stress check scores (Z-scores) were compared among the three groups.
Analysis of ‘Co-workers’ support’ by industry type and workers’ age
To investigate the differences by industry and age, we divided the participants into two age groups (≥40 or ≤39 years old) and compared the ‘co-workers’ support’ subscale by industry categories.
Statistical analysis
Smoking was compared between the AS and NS groups using unpaired t-tests for all 18 subscales, and additionally compared using nominal logistic analysis adjusted for age, body mass index (BMI), amount of alcohol consumption and drinking frequency. Based on the results obtained from the basic statistics, the average age and BMI differed significantly according to smoking intensity. Therefore, age and BMI were selected as items for adjustment. In addition, since a prior publication31 showed that many workers smoke when drinking, drinking behaviour was also an adjustment item. To clarify the synergy of stress indicators that are strongly related to smoking status, logistic regression analysis was conducted for smoking status to 18 subscales. Three models were tried: model 0 (without adjustment), model 1 (adjusted for age and BMI) and model 2 (model 1 with additional adjustment for amount and frequency of alcohol consumption), and the three subscales with the highest ORs were selected in every trial. Participants with positive or zero Z-scores on the selected subscales were classified as stressed (+) and those with negative Z-scores were classified as stressed (−) to form two groups. Nominal logistic regression analysis was performed on eight combinations of three subscale stresses (+) or (−).
Regarding smoking intensity, the Z-scores of the three components of the BJSQ and the 18 subscales were compared for the NS, LS and HS groups by the Dunnett’s test with NS as the control. Z-scores were examined by multivariate analysis adjusted for age and BMI, amount of alcohol consumption and drinking frequency. Additionally, an examination of ‘co-workers’ support’ by industry and age group compared the NS, LS and HS groups by multivariate analyses adjusted for BMI, amount of alcohol consumption and drinking frequency.
JMP for Macintosh (V.14.0.0) was used for statistics.
Results
The smoking rate for the entire study population was 13.6% for women and 41.4% for men. For both genders, the smoking rate by age group was highest in the 40s and the lowest in the 20s. There were more LS and fewer HS among women in all age groups. In men, the number of LS was greatest among those in their 20s. The industry category with the lowest smoking rate was civil servants of both genders (table 1).
Demographics of study participants (n=59 355)
Mean age of women smokers was significantly older than for NS; in addition, both LS and HS women were significantly older than NS women. Among men, LS were significantly younger than NS, and HS were significantly older than NS. In women, BMI was significantly lower in LS and higher in HS than in NS, but no significant difference was observed between NS and AS. In men, BMI was significantly lower in AS and LS than in NS, but there was no significant difference in BMI between HS and NS (table 1).
As shown in table 2, many of the stress subscales were independently and significantly associated with smoking. The ORs for each subscale were almost the same in the three models, and even after taking into account the amount and frequency of alcohol consumption, the three highest ORs for both genders were for ‘physical burden’, ‘irritation’ and ‘physical symptoms’. Conversely, ‘co-workers’ support’ had the lowest OR of all subscales, especially for men. The risk increased with the combination of the three factors of ‘physical burden’, ‘irritation’ and ‘physical symptoms’ for both genders (table 3).
ORs of smokers to non-smokers for a 1 SD increase in the BJSQ stress Z-score of men and women (by subscales)
ORs of smoking to not smoking for the BJSQ subscale combinations highly associated with smoking
Compared with NS, the BJSQ simple total score for AS women had significantly higher stress values than for NS in all components (online supplemental table 1). When compared with NS by smoking intensity (figure 1), Z-scores for almost all subscales for HS women were significantly higher, with only ‘job demands’, ‘suitability for work’ and ‘required job quality’ being not significantly different between NS and HS. Results of the multivariate analysis for all ‘Social Support’ subscales also showed that HS women had significantly higher Z-score values than NS women.

Z-scores of components and subscales on the Brief Job Stress Questionnaire (BJSQ) by participants grouped according to smoking intensity. †P<0.05 versus non-smokers (Dunnett’s test only). #P<0.05 versus non-smokers (Dunnett’s test and multivariate analysis adjusted for age, body mass index, amount of alcohol consumption and frequency of alcohol consumption).
In men, the AS group had slightly but significantly lower scores for ‘Social Support’ than the NS group (online supplemental table 1). According to smoking intensity, the ‘Social Support’ score compared with NS was significantly lower in LS by multivariate analysis, but no statistical difference was observed between NS and HS (figure 1). Significantly higher stress scores were shown for ‘job demands’ and ‘required job quality’ in LS than in NS.
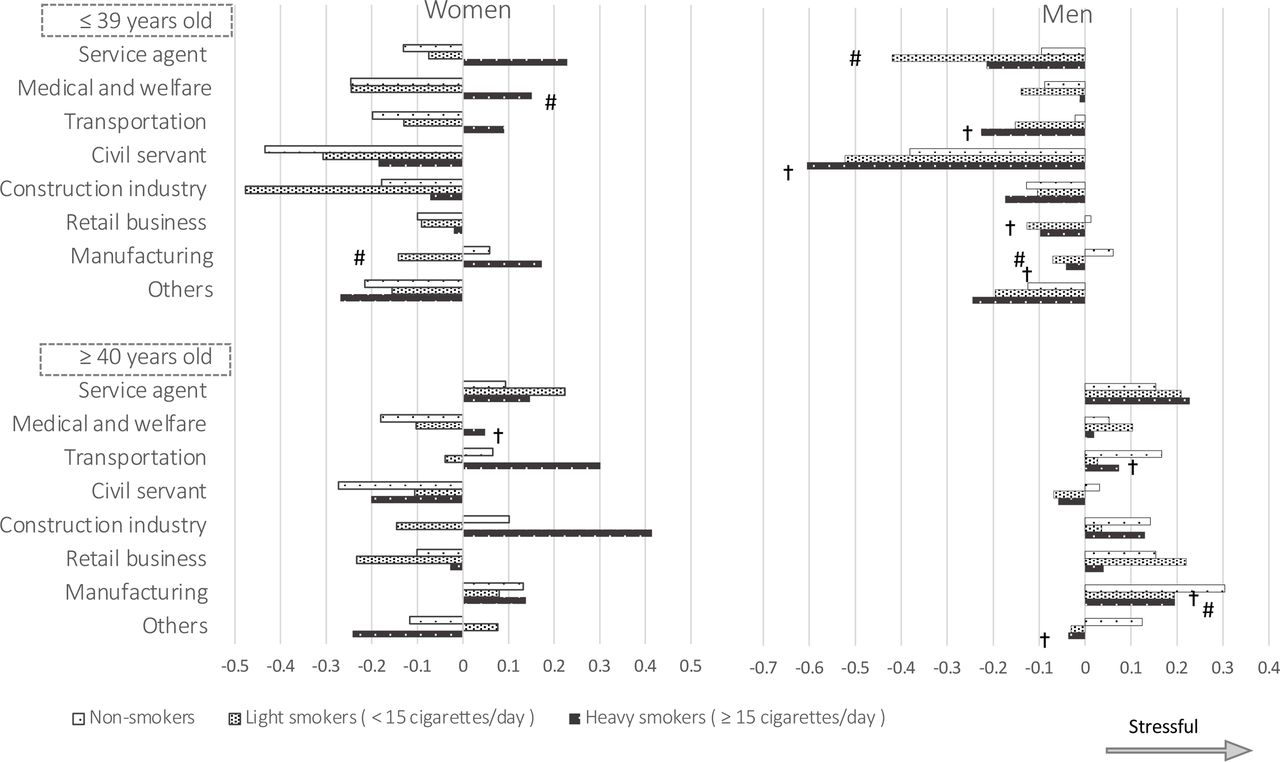
Since ‘co-workers’ support’ differed from the other subscales in that smokers were less stressed than NS, we added an analysis that included industry type and chronological age (≤39 years old vs ≥40 years old) (figure 2). By industry, in women, HS in the medical and welfare industry had the highest stress scores for ‘co-workers’ support’ compared with NS in the same industry. Exceptionally, LS in the manufacturing industry were characterised by lower stress scores for ‘co-workers’ support’ than NS. In men, LS in the service industry, LS and HS in the manufacturing industry and HS in ‘other’ industries had significantly lower stress scores for ‘co-workers’ support’ than NS in their respective industries (online supplemental figure 1). By age group, in women, both HS ≥40 years old and HS ≤39 years old had the highest stress scores for ‘co-workers’ support’ compared with NS in their respective age group. In men, HS ≥40 years old, HS ≤39 years old and LS ≤39 years old were characterised by lower stress scores for ‘co-workers’ support’ than NS in their respective age group (online supplemental figure 2). By age group and industry, in women ≤39 years old, HS in the medical and welfare industry had the highest stress scores for ‘co-workers’ support’ compared with NS in the same industry. LS in the manufacturing industry had lower stress scores for ‘co-workers’ support’ than NS in the same industry. In men ≤39 years old, LS in the service industry and LS in the manufacturing industry had significantly lower stress scores for ‘co-workers’ support’ than NS in their respective industries. Also, in men ≥40 years old, HS in the manufacturing industry had significantly lower stress scores for ‘co-workers’ support’ than NS in that industry (figure 2).
Supplemental material
Supplemental material

{kind=link}
{kind=link}
Z-scores of ‘co-workers’ support’ subscale on the Brief Job Stress Questionnaire (BJSQ) by participants grouped according to smoking intensity, age group (≥40 and ≤39 years) and main industries. †P<0.05 versus non-smokers (Dunnett’s test only). #P<0.05 versus non-smokers (Dunnett’s test and multivariate analysis adjusted for body mass index, amount of alcohol consumption and frequency of alcohol consumption).
Discussion
This is the first large-scale study to investigate a wide range of components of occupational stress and smoking intensity using the BJSQ. We have clarified occupational stress specific to smokers on the following three points. (1) Subscales independently associated with smoking in both genders were ‘physical burden’, ‘irritation’ and ‘physical symptoms’. However, since there was no synergistic effect of these three major stress subscales, we felt it was not important to prioritise addressing this stressor or stress response in the workplace. (2) HS women were generally highly stressed. (3) LS men obtained more ‘co-workers’ support’ even though they had higher stressors such as ‘job demands’. As hypothesised, the larger the amount of smoking in women, the greater the stress in all three components of ‘Job Stressors’, ‘Stress Reactions’ and ‘Social Support’. But in men, smoking intensity and social support did not support the hypothesis. The reason why smoking status was strongly associated with ‘physical burden’ rather than ‘job demands’ is that ‘small breaks to rest the body’ may be strongly linked to smoking and become a habit in the manufacturing, transport and construction industries in men. The high rate of smoking in these occupations has already been shown in a survey of medium-sized and small-sized companies in Japan.15 ‘Job demands’ primarily identifies the degree of psychological burden whereas ‘physical burden’ was evaluated by only one question asking whether the work involved physical labour. In an earlier occupation-specific survey, Strickland and colleagues reported nearly twice the rate of smoking among white construction workers compared with whites in general in Missouri, USA.32 Chau and colleagues examined the work content in assessing ‘physical job demands’ and reported that workers with a higher total amount of physical work, such as ‘working under bad weather’ and ‘using vibration tools’, smoked greater numbers of cigarettes in the Lorene region of France.33 This is probably because such workers often work on the same team and recognise smoking as a ‘means of dealing with work difficulties’. Furthermore, smokers recognise that smoking can relieve the ‘irritation’ that they feel as occupational stress, but this ‘irritation’ can also occur as symptom of nicotine withdrawal due to a temporary interruption of smoking during work.34 In addition, nicotine withdrawal can be manifested by dizziness and palpitations. In a review, Parrott stated that smokers tended to report high ‘daily’ stress and that stress symptoms such as irritation increase when they cannot smoke frequently, and that successful quitters experience reduced ‘stress’.35 Strictly speaking, these complaints by smokers may not be ‘physical symptoms’ of occupational stress.
The reasons why HS women were highly stressed are complex. HS women generally have high scores for ‘Job Stressors’ such as ‘job control’, ‘work environment’ and ‘interpersonal relationships’, and they may be engaged in low discretionary tasks in the first place. In addition, it was shown that women smokers not only workers in general were more likely than men to express negative emotions, such as anxiety, regarding the stress response36; biological and socioenvironmental ‘sex differences’ are being explored.37 Tomioka et al18 suggested the necessity of coping with psychological distress as a smoking cessation measure for Japanese women, including the non-regularly employed and unemployed. Our results suggest that coping with stress symptoms may also be useful for smoking cessation among regularly employed women who are more financially stable. Similarly, the results of ‘Social Support’ suggested that HS women engaged in tasks with less support than NS. Conversely, the stress caused by lack of social support may have led women to smoke. Creswell and colleagues reported that, in general, ‘social support’ aided in the success of smoking cessation.38
In men, there might be a kind of ‘social smoking’ because smokers reported better ‘Social Support’ than NS. Earlier reports captured the phenomenon that college student smokers smoked only when with friends and acquaintances,39 40 and the presence of youth who habitually smoked only on social occasions, such as at parties, became recognised. They were reported to display positive actions in preventing secondhand smoking by NS.41 Even in Japan, smokers who ‘do not smoke at home’ exist, and their restrained smoking style was reported.42 This type of smoking, which is highly related to peers, has been defined as ‘peer smoking’.33 43 The results for ‘co-worker’s support’ suggest that LS are more likely to be social smokers, especially in the service and manufacturing industries. LS men and women in the manufacturing industry had significantly better coworkers’ support than NS. This means that LS in these industries may feel closer to their co-workers when they smoke.
Research on social support and smoking in the workplace suggested that smoking functioned as a communication tool. In China, where the smoking rate is as high as 38%, it is highly speculated that supervisors and coworkers are smokers, so smokers are more likely to obtain support by supervisors.44 A study in North America reported (smoking rate: 26%) that supervisors’ support inhibited smoking, but coworkers’ support did not.45 In addition, a study of civil servant Brazilian men (smoking rate: 17%) reported that social support suppressed smoking.46 Thus, the association between ‘social support’ and smoking may be explained by differences in the workplace smoking rate, with better relationships between NS in environments with a low smoking rate and better communication between smokers in workplaces with high smoking rates. LS men probably have sufficient knowledge about the health hazards of smoking to suppress their smoking intensity. However, they may be psychologically unable or fail to initiate smoking cessation because they may be afraid of losing social support in a workplace with a high smoking rate. Indeed, interventional surveys of smoking cessation guidance have reported that workplaces with a higher percentage of smokers have a stronger impact on peer smoking behaviour and lower rates of long-term smoking cessation.43
Smoking rates may also be a factor in ‘co-workers’ support’ scores. Among women, ‘co-workers’ support’ was better for LS than NS in the manufacturing industry. The smoking rate among women in the manufacturing industry was relatively high at 15.8%, and it is estimated that women obtain ‘co-workers’ support’ through smoking in such workplaces. These findings seemed to mean that good communication through smoking in a workplace could occur if the smoking rate was relatively high. In addition, the relationship between coworker support and smoking intensity within industries may differ depending on work duties. In health and social work, smoking is perceived as undesirable, and HS who take frequent smoking breaks are imagined to have reduced communication with colleagues. Promoting smoking cessation among youth is desirable for their health, and smoking regulations may be acceptable especially for young social smokers due to their behavioural characteristics. Common social smoking measures in workplaces include bans on smoking on workplace premises and during working hours.47 Simultaneously, it is necessary to promote communication among workers in the workplace, even under a non-smoking environment. Alternatives to smoking that promote informal communication include taking short breaks, increasing opportunities for face-to-face conversations and increasing opportunities for interaction with workers in other departments based on the benefits that smokers have received.48
Significance and limitations of this study
The strength of this study is that it was a large comprehensive occupational stress survey of employed individuals in East Asia. Therefore, this study could investigate the association between a wide range of occupational stresses and smoking intensity across multiple occupations, suggesting for the first time that workplace stressors and supportive conditions may differ according to smoking rates in workplaces and by gender.
A limitation of this study is that it was cross-sectional and therefore causal relationships could not be identified. Factors such as working hours, job position and company size, which could not be surveyed at this time, may have contributed to the association between smoking and physical burden. Also, because the number of cigarettes smoked was provided by self-report in a health check-up questionnaire, responses may be inaccurate, such as inputting less than the actual dose. Reports by users of electronic cigarettes and heated tobacco product users may not have been accurate because it is difficult to translate these products into the number of cigarettes smoked or because users are not aware of them as tobacco products.
Conclusions
The occupational stress of smokers of both genders may be related to the subjective ‘physical burden’, ‘irritation’ and ‘physical symptoms’. In analyses of smoking intensity and gender, both strong psychosomatic stress symptoms such as ‘irritation’ and ‘physical symptoms’ and lack of social support at work were observed in HS women; however, in contrast, over AS, ‘co-workers’ support’ was good in men. In addition, in young LS women in the manufacturing industries, where the smoking rate is relatively high, we observed significantly better ‘co-workers’ support’ compared with that in NS, suggesting the presence of ‘social smokers’ who continue to smoke small amounts as a communication tool in these workplaces.
These results suggest that improvement of the communication environment among workers may be essential for the promotion of smoking cessation at the same time as smoking bans in worksites and public facilities.
Data availability statement
No data are available. Individual participant data for this article, including study protocols, are not available.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the Ethics Committee of Niigata University (2017-0401), and we have obtained consent for the use of personal information from all participants on the health check-up. After confirming the concordance of the data, personal information such as the participant’s name, personal identification code for health check-up orders and the name of the company or office to which the worker belonged was removed before using the data for analysis. This study does not involve animal subjects. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We would like to thank the staff of the division in charge of information processing of the Niigata Association of Occupational Health for their great cooperation.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors ST, KK and HS planned and designed the study. MT, KM, MO and KS did the project administration, funding acquisition and data collection. HS is responsible for the overall content as the guarantor. ST and KK calculated the data for the statistical analyses, did the literature review and wrote the first draft of the manuscript following the discussion with all the authors. MK, SK, KF and HS contributed to the editing of the manuscript. All authors participated in data interpretation, commented on subsequent drafts, approved the final manuscript and agreed to submit the manuscript for publication.
Funding This study was supported in part by the Japan Society for the Promotion of Science and Ministry of Health, Labour and Welfare. Grants-in-Aid for Scientific Research (19139518) of Japan Society for the Promotion of Science (JSPS).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.