Article Text

Abstract
Importance No proven treatment is available for severely ill COVID-19. Therapeutic use of COVID-19 convalescent plasma (COPLA) is under investigation.
Objective To compare the efficacy of COPLA with standard medical therapy (SMT) alone in severe COVID-19 patients.
Design, setting and participants A multicentric, open-labelled, phase-III randomised controlled trial conducted at two treatment centres with COPLA collected at the third dedicated centre in North-India, the coordinating centre during trial from June 2020 to December 2020. The study population comprised 400 participants in the ratio of 1:1 in each treatment group.
Intervention One group received COPLA with SMT (n=200), and another group received SMT only (n=200).
Main outcome measures Primary outcome was time to clinical improvement measured by a two-point reduction in the ordinal scale. Secondary outcomes included duration of O2 therapy, the proportion of patients on mechanical ventilation at day-7, mortality, SARS-CoV-2 antibody levels, cytokine levels and incidence of adverse events.
Results The median time to a two-point reduction in the ordinal scale in both groups was 9 days (IQR=7–13) (p=0.328). The median duration of O2 therapy was 8 days (IQR=6–12) in COPLA and 10 days (IQR=6–12) in SMT group (p=0.64). The PaO2/FiO2 ratio showed significant improvement at 7 days in COPLA group(p=0.036). There was no difference in mortality till 28 days in both groups (p=0.62). However, if COPLA was given within 3 days of hospital admission, a significant reduction in ordinal scale was observed (p=0.04). Neutralising antibody titres in COPLA group (80 (IQR 80–80)) were higher than SMT group (0 (IQR 0–80)) at 48 hours (p=0.001). COPLA therapy led to a significant reduction in TNF-α levels at 48 hours (p=0.048) and D-dimer at 7 days (p=0.02). Mild allergic reactions were observed in 3 (1.5%) patients in COPLA group.
Conclusion and relevance Convalescent plasma with adequate antibody titres should be transfused in COVID-19 patients along with SMT in the initial 3 days of hospitalisation for better clinical outcomes.
Trial registration number NCT04425915.
- COVID-19
- blood bank & transfusion medicine
- blood bank & transfusion medicine
Data availability statement
Data are available on reasonable request. Data (unpublished data in its row form in Microsoft excel sheet) will be available with principal investigator of the study and it will be available for researcher in unidentified data form on reasonable request to principal investigator till 5 years from date of publication. Rest all data relevant to the study are included in the article or uploaded as online supplemental information
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
Study highlights the role of testing of antibody titres in convalescent plasma.
Patient baseline titre levels are unrelated with outcomes.
Study emphasises that the timing of transfusion of high titre convalescent plasma is critical.
Delayed transfusion of convalescent plasma is rather harmful and should be discouraged.
Duration from admission to transfusion could not be regulated as most patients did not fulfil inclusion criteria on the day of admission.
Introduction
Since the emergence of SARS-CoV-2 infection in late 2019, no proven treatment options are available forCOVID-19. Researchers are working relentlessly to develop therapies to combat this life-threatening problem. COVID-19 convalescent plasma (COPLA) use in COVID-19 has been approved for off-label emergency use and under phase III trials by many national and international bodies. Convalescent plasma from recovered COVID-19 patients contains neutralising antibodies against the spike protein of SARS CoV-2, which may benefit severely sick COVID-19 patients by neutralising the virus and halting its replication in the host. Convalescent plasma was found effective in the treatment against the Middle East respiratory syndrome, influenza A (H1N1), Avian influenza (H5N1) and Ebola in the past.1–3 One recent observational study conducted by the Mayo Clinic on 20 000 patients transfused convalescent plasma has shown a good safety profile.4A study done by Cheng et al on 80 patients of SARS virus who received convalescent plasma had a lower mortality rate than the overall mortality rate. They reported encouraging outcomes in patients treated with convalescent plasma in the 2003 SARS pandemic. They further found that out of 80 patients, 33 patients transfused convalescent plasma within the 2 weeks of symptom onset showed better outcomes than those transfused later.1 During the current pandemic (SARS CoV-2), many studies have proven that convalescent plasma can limit viral replication by providing passive neutralising antibodies to SARS CoV-2in the initial viraemia phase and thus mitigate the disease in the absence of definitive therapy.5 In recovered patients, who are prospective COPLA donors, there are variations in antibody titres and specificities against components of the virus.6In this trial, we assessed the safety and efficacy of convalescent plasma transfusion in severe COVID-19 patients using an ordinal scale until 28 days for clinical outcomes.
Methodology
Study settings and trial design
The COPLA-II trial was a multicentric, open-labelled randomised controlled trial conducted at two treatment centres with convalescent plasma being collected at the third dedicated centre in India, which was also the coordinating centre during the trial. The study population comprised 400 patients with severe COVID-19, and stratified block randomisation (each block of 10) was done in the ratio of 1:1 with 200 patients in each of the treatment groups (ie, CP with standard medical therapy (SMT) as the intervention arm vs SMT only as control arm). Allocation concealment was done using the ‘Sequentially Numbered Opaque Sealed Envelopes’ method. Written informed consent from all the study participants was taken before their enrolment in the study. The trial protocol is available in online supplemental material 1 as study protocol and online supplemental material 2 as statistical analysis plan. The conduct of the trial was as per the Declaration of Helsinki principles.
Supplemental material
Supplemental material
The sample size was calculated by assuming median survival in SMT as 24 days, and convalescent plasma with 18 days giving a reduction of 25% of the median time; then with α=5% and β=20%, A sample size of 190 participants was needed to be enrolled in each treatment arm by survival analysis method. (Z1-α/2+zβ)2/((ln(θ))2 where Z1-α/2=1.96 and zβ= 0.84, θ= λ1=log2/24 λ0=log2/18. Hence, we enrolled 400 cases equally and randomly allocated into two arms, as shown in figure 1. The study was started on 14 June 2020, and the last follow-up was conducted on 15 December 2020. All the authors are fully responsible for the trial design and conduct and assure the data’s authenticity. The overall study was monitored regularly by an independent data and safety monitoring board.
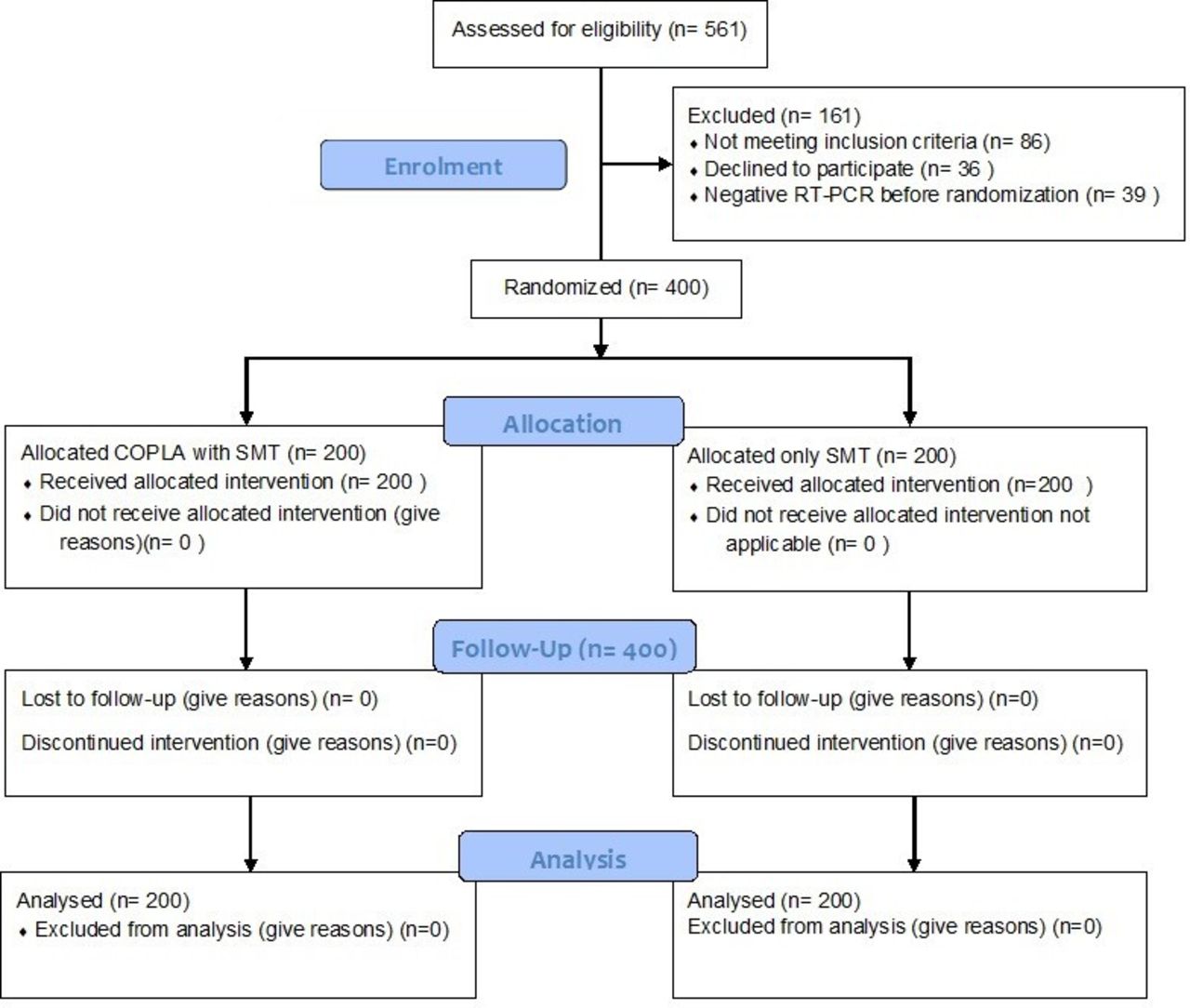
Consort flow diagram. COPLA, COVID-19 convalescent plasma; SMT, standard medical therapy.
Inclusion and exclusion criteria
Study participants with severe COVID-19 of age 18 or above were considered for randomisation in the study after obtaining informed consent at both the COVID-19 treatment centres. The WHO Interim Guidance defined severe COVID-19 as following any of the two criteria out of five including ventilated patient within 24 hours, respiratory rate ≥30 beats/min, oxygen saturation in the resting state level less than 90% in resting state, Partial pressure of oxygen/ Fractional inspired oxygen ratio (PaO2)/(FiO2) ≤300 mm Hg, and lung infiltrates ≥50% within 24–48 hours. Patients with a history of allergy to plasma, pregnancy, multiorgan failure, HIV, viral hepatitis, cirrhosis, renal impairment on dialysis and Renal replacement therapy (RRT), cancer, uncontrolled hypertension and diabetes, arrhythmias, unstable angina and haemodynamically unstable patients requiring vasopressors and expected life expectancy less than 24 hours were excluded.
Intervention
Patients in the intervention arm were given two doses of 250 mL of convalescent plasma on consecutive days along with the standard of care, while in the control arm, only standard of care was given. The standard of care was based on the detailed guidelines for COVID-19 management laid down by the Ministry of Health and Family Welfare, India.7 All institutional protocols for supportive management were implemented but not restricted. It included other investigational drugs like remdesivir and dexamethasone approved by the government authorities for COVID-19 patients irrespective of the treatment group. Guidelines issued by the ARDSNet for ARDS and the Surviving Sepsis campaign for sepsis were followed.8 All the patients were monitored daily until clinical improvement or up to 28 days as per the ordinal scale. At the plasma collection centre, up to 500 mL of convalescent plasma was collected from recovered COVID-19 patients as per the Drugs and Cosmetics Act 1940 and Rules 1945, amended on 11 March 2020.9 Collected plasma was labelled appropriately and frozen below −30°C for 1 year.
Laboratory evaluation
We tested the presence of IgG antibodies and neutralising antibodies to SARS CoV-2 in the serum of study subjects. The spike protein S1 receptor-binding domain (RBD) IgG antibody titres were done by ELISA method (SARS-CoV-2 Spike S1-RBD IgG Detection Kit, Genscript, USA), directed against the SARS-CoV-2 RBD proteins. The titre was determined by the ELISA method with sample dilutions 1:80, 1:160 and 1:640 as per the manufacture’s instruction. All the samples were tested in duplicate. ELISA titres were determined by the endpoint dilution. The S1 RBD IgG antibody titres were determined in recipient samples before transfusion at baselines 24, 48, 72 hours than day 7, day 10 and day 14. A fourfold rise in titres was considered useful for protection.
The determination of serum neutralisation antibodies in donors was done by the SARS-CoV-2 surrogate virus neutralisation test Kit (Genscript, USA). The minimum acceptable neutralising antibody titre of transfused convalescent plasma was 80. The test is used to detect circulating neutralising antibodies against the SARS-CoV-2 virus that can block the interaction between the RBD of the viral spike glycoprotein with the ACE2 cell surface receptor. The neutralisation antibody titres at 1:80 dilutions were tested as per the manufacturer’s instruction at similar time points as S1 RBD IgG antibody titres.
Cycle threshold value
We amplified two SARS CoV-2 E-genes (for sensitivity) and RdRP genes (for specificity) by 45 cycles run by RT-PCR (real-time, reverse transcriptase-PCR, Q-Line-ER nCoV-19 RT-PCR Detecon kit, POCT services, India) method. Any amplification ≤40 cycle threshold (Ct) value for both the genes was considered as positive, and the cycle number (Ct value) was noted. Any amplification >40 Ct was considered as negative .
Other lab parameters
Patient’s samples were tested for complete blood count (CBC), D-dimer, International normalized ratio (INR), Activated partial thromboplastin time (APTT), Liver function test (LFT), kidney function test (KFT), Lactate dehydrogenase (LDH), C reactive protein (CRP), serum ferritin and cytokines (IL-1, IL-6, TNF-α) (equipment/kit details are in online supplemental material 1).
Clinical outcomes
The primary outcome measure was time to clinical improvement, defined as a reduction in ordinal scale by two points or live discharge, whichever was earlier up to 28 days. Secondary outcome measures included the proportion of patients in each treatment group based on the ordinal scale at 48 hours, 7 days, 14 days and 28 days, duration of O2 therapy, Intensive Care Unit (ICU) stay, hospital stay, the proportion of patients on mechanical ventilation at day 7, mortality in both groups at 7 days, 28 days. Incidence of adverse effect in both the groups during 28 days, presence of antibodies to SARS-CoV-2 in serum after plasma administration on the baseline, after 48 hours, day 7 and day 14 and their correlation with disease parameters, changes in cytokine levels and acute phase reactant till 28 days.
Statistical analysis
Data collected and entered into Microsoft excel sheet 2010. The Statistical analysis was conducted using SPSS software V.22 (IBM). Descriptive analysis was mean±SD or in median (IQR) as appropriate for a continuous variable. The categorical data is shown as n (%), and continuous data were analysed either by Student’s t-test or Mann-Whitney test depending on the normality assumption. The categorical data is analysed by χ2 or Fisher’s exact test. Besides this Kaplan-Meier method, along with Cox regression analysis, was also used for survival analysis. Repeated measure analysis was carried out to see change over the period, followed by post hoc comparison by the least square deviation method. The significance was seen at a 5% level of significance.
Patient and public involvement
Patients and the public were not involved in the design, conduct, reporting or dissemination plans of this trial.
Results
Patients
A total of 561 patients were assessed for eligibility, out of which 86 did not meet the inclusion criteria, 36 declined to participate and 39 were RT-PCR negative; finally, a total of 400 patients were randomised equally into the COPLA group (COPLA with SMT) and SMT group (SMT only). All the patients included in the COPLA group received at least one dose of 250 mL of convalescent plasma.
Baseline patient profile: both the patient groups were comparable for mean age, gender and body mass index
The patients in both the COPLA and SMT groups had a comparable ordinal scale, O2 saturation, respiratory rate, PaO2/FiO2 ratios, and other laboratory parameters, as shown in table 1.In the COPLA group, 500 mL of convalescent plasma was transfused in two divided doses of 250 mL each 24 hours apart in addition to the standard medical treatment in both the groups. The median S1 RBD IgG antibody titre of all patients at baseline was 0 (0, 40). In COPLA group, it was 0 (0, 40) while in SMT group 0 (0, 80), with no significant difference between COPLA and SMT group at inclusion in the study (p=0.275). The median neutralising antibody titre of all patients at baseline was 0 (0, 40). In COPLA group it was 0 (0, 40) while in SMT group 0 (0, 80) with no significant difference between both treatment groups at inclusion in the study (p=0.322). We found that overall, 136 (34%) patients had S1 RBD IgG antibodies at baseline due to the natural course of infection, among which 65 (32.5%) were in COPLA group while 71 (35.5%) were in SMT group and were comparable statistically (p=0.526). Similarly, overall, 130 (32.5%) had neutralising antibodies at baseline, among which 62 (31%) were in COPLA group while 68 (34%) were in SMT group and were comparable statistically (p=0.522).
Baseline characteristics of study participants
Primary outcome
The median time for a two-point reduction in ordinal scale in both groups was 9 days with an IQR betweent0.328), as shown in table 2. On subgroup analysis after adjusting for days to randomisation and transfusion of convalescent plasma before (n=115, ≤3 days) or after (n=85, ≥4) 3 days from admission, significant improvement in ordinal scale was observed in the COPLA group patients who were transfused within 3 days of admission (n=115 vs n=85; p=0.04), as shown in figure 2. Further, patients transfused convalescent plasma after 3 days of admission showed less improvement in the ordinal scale than SMT therapy (p=0.08).

Comparison of ordinal scale in both treatment groups. SMT, standard medical therapy.
Changes in clinical parameters during treatment
Secondary outcome
The proportion of patients in each treatment group based on the ordinal scale at 48 hours, 7 days, 14 days and 28 days were comparable with no statistically significant difference as shown in table 3. Maximum patient mortality was observed within 7 days of randomisation in both the treatment groups, and the majority were discharged within 14 days of randomisation.
Proportion of the patients with ordinal scale at different timelines
The median duration of O2 therapy was 8 days (IQR=6–12) in COPLA group as compared with 10 days (IQR=6–12) in SMT group, but the difference between both the groups was not significant (p=0.644). Improvement was observed in oxygen saturation and respiration (reduction in the respiratory rate) at 48 hours and 7 days with no significant differences in both the treatment groups, and on further subgroup analysis it was not significantly different with transfusion timings. (online supplemental material 3 as oxygen saturation with time of transfusion). Improvement in PaO2/FiO2 ratio was observed at 48 hours and 7 days in both the treatment groups, and it showed a clinically significant improvement at 7 days in the COPLA group as compared with SMT group (p=0.036). Total 51 patients needed mechanical ventilation till 7 days, out of which 27 (52.9%) were in COPLA group while 24 (47.1%) were in the SMT group, and on day 7, 2 patients were on active mechanical ventilation in COPLA group while three patients were in SMT group and rest in both the groups were succumbed. No significant difference in requirement of mechanical ventilation was observed between both the groups till day 7 (p=0.61). The median SOFA scores were comparable at 48 hours and day 7, with no significant difference between the groups, as shown in table 2.
Supplemental material
Antibody levels
There was a significant increase in S1 RBD IgG antibody titres and neutralising antibody titres in the COPLA group compared with SMT group at 48 hours, 7 days and 14 days post-transfusion, as shown in figure 3 and table 4. On subgroup analysis in COPLA group to see mortality at 7 days and 28 days and change in ordinal scale, we did not find any differences with baseline titres in patients at the time of randomisation and transfusion. On repeated measure analysis, when we considered both initial zero titres and transfusion less than 3 days, we observed a significant reduction in the ordinal scale (p=0.016) related to the timing of transfusion irrespective of baseline titre value as shown in figure 4.

Progression of antibody titres in both groups in patients with no baseline titres. RBD, receptor-binding domain.
Changes in viral load and SARS CoV-2 antibody titre

Impact of titres and transfusion timings on ordinal scale.
In both the study arms, baseline cytokine levels were comparable. On convalescent plasma transfusion, median post-transfusion IL-1β, IL-6, were reduced at 48 hours and 7 days, and in SMT group, only IL-1β level was reduced at 48 hours and 7 days while IL-6 was increased at 48 hours and then decreased on day 7. The TNF-α level was increased in both the COPLA and SMT groups at 48 hours and 7 days. The cytokine differences did not attain statistical significance in both the groups except the 48 hours TNF-α level, which was higher in the SMT group (p=0.048). Acute-phase reactants, including Serum ferritin, CRP and D-dimer, were assessed at baseline, 48 hours and 7 days. Serum ferritin levels were raised at 48 hours and then decreased below the baseline at 7 days in both groups with no significant difference. The CRP showed a decline at 48 hours and 7 days from the baseline level in both groups, which was not statistically significant. The median D-dimer levels were near the baseline value in the COPLA group while rising in the SMT group after 48 hours and 7 days. The median D-dimer levels were significantly higher in the SMT group at 7 days than in the COPLA group (p=0.02). Levels of cytokine and acute-phase reactants are as shown in table 5. We found a significant increase in D-dimer, IL-6, serum ferritin and CRP levels in the non-survivors compared with the survivors at day 28, as shown in table 6.
Post-transfusion cytokine and acute phase reactants level
Factors affecting mortality in COVID-19 patients
Mortality
Total mortality was 19.75% (79/400) at 28 days.25 (54.3%) died till 7 days, and 42 (53.2%) till 28 days in the COPLA group, while 21 (45.7%) died till 7 days, and 37 (46.8%) till 28 days in the SMT group. No statistically significant difference in mortality was observed between the groups at 7 days (p=0.64) or 28 days (p=0.62). Mortality prediction by Kaplan-Meier survival analysis revealed no significant difference in mortality at day 28 (p=0.537) in both the treatment groups. In COPLA group, subgroup analysis revealed no significant difference in mortality at day 7 (p=0.32) or day 28 (p=0.2) when convalescent plasma was transfused within 3 days of hospital admission, while significantly high mortality was observed at day 7 (p=0.03) and day 28 (p=0.01) when the convalescent plasma was transfused beyond 3 days of admission (figure 5).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Comparison of mortality in both treatment groups. SMT, standard medical therapy.
The median duration of ICU stay was 9 days (IQR=6–14) and hospital stay was 12 days (IQR=9–16) in the COPLA group while the median duration of ICU stay was 9 days (IQR=6–15), and hospital stay was 13 days (IQR=9–18) in the SMT group. However, the difference was not significant (p=0.983). During plasma transfusion, mild allergic reactions (urticarial) were observed in three patients, managed by an antihistaminic with symptomatic relief. No other transfusion reactions, including transfusion-related acute lung injury, were observed in the COPLA group.
Discussion
In this randomised controlled trial, we identified the antiviral effects of convalescent plasma transfusions as add-on therapy to the standard medical treatment in the initial days of SARS COV-2 infection. COVID-19 has affected more than 170 million people, and the tally of death has reached 3.5 million patients and counting in different waves worldwide.10
Different treatment modalities
Recently, the initiation of vaccination against COVID-19 in different parts of the world has been encouraging, although these vaccines are of varying efficacy and there is limited access due to high demand. Because of limited access to vaccine and mutant variants of SARS CoV-2, most of the world population is still vulnerable to infection. Even after more than 1 year, no specific treatment has evolved to curtail SARS CoV-2 infection. Dexamethasone has shown some effectiveness in the management of severe cases in the RECOVERY trial by reducing the mortality from COVID-19.11Summary recommendation of National Institutes of Health has suggested convalescent plasma therapy and SARS-CoV-2immunoglobulin for COVID-19 as under investigational drugs due to insufficient data available on its effects, timing and doses of transfusion on the survival of COVID-19 patients.12
Role of convalescent plasma therapy in COVID-19
Convalescent plasma therapy can be given to the SARS-CoV-2 patients in view of expected possible clinical efficiency, immediate availability of a large pool of the donors, relative ease of procuring, storage and transfusion. Convalescent plasma therapy is based on the principle of providing neutralising antibodies against the SARS-CoV-2spike protein to patients with active infection.6 COPLA transfusion was done in two divided aliquots on consecutive days since patients are already in respiratory distress, and a large single dose of 500 mL might be an aggravating risk factor for the development of transfusion-associated cardiac overload. Further aliquoting of 250 mL was done at the time of collection, so the quality of COPLA was maintained. Due to this approach, we did not encounter any reaction related to cardiac overload or respiratory distress. In our study, both the treatment groups were comparable at baseline in terms of the presence of S1 RBD IgG antibodies and neutralising antibodies. Almost 30% of patients in both groups had antibodies due to the natural course of infection, suggesting the need to determine the baseline antibody titres in recipients before transfusion to use resources judiciously and for favourable outcomes. We found a significant rising trend in antibodies post-transfusion of convalescent plasma compared with SMT, which might be useful to expedite the immune response against the virus. Additionally, we found that patients with no previous antibody titres in COPLA group have shown a reduced proinflammatory cytokine response and acute phase reactants which are strong predictors of mortality in such patients. On the assessment of laboratory parameters, we found elevated baseline levels of D-dimers; IL-6, serum ferritin and CRP as predictors of mortality, similar to the findings reported in a meta-analysis done by Huang et al, and Kermali et al13 14
Further Zhang et al and Yao et al found that D-dimer levels were elevated in COVID-19 patients correlating with disease severity and an important predictor of in-hospital mortality in severe COVID-19 patients.15 16 In the current study, we observed no significant difference between both the treatment groups in terms of the time of two-point reduction in the ordinal scale similar to the study done by Salazar et al.17 Similar to the other studies, we did not find any significant difference in the duration of O2 therapy, ICU stay and hospital stay between both the groups. Even the overall mortality in both the groups till 28 days was comparable, indicating no survival benefits with convalescent plasma transfusion.18–21
Impact of timing of COPLA transfusion
When we considered the timing of transfusion from admission to randomisation within 3 days, on repeated measure analysis, we found significant improvement in ordinal scale in the COPLA group patients who were transfused convalescent plasma within 3 days of admission as compared with SMT group. Similarly, Arnold Egloff et al, conducted a retrospective study on patients hospitalised with COVID-19 and found that mortality risk was lower with quicker recovery in patients who received convalescent plasma within 3 days of admission as compared with patients who received in more than 3 days.22 Furthermore, our study highlighted that if convalescent plasma was transfused after 3 days of admission, it significantly worsened the improvement on an ordinal scale. Generally, most of the patients seek a hospital facility after 3–5 days of infection; the window of transfusion of convalescent plasma remains very small, and justifies its use up to 3 days from admission. Our findings justified transfusion of convalescent plasma within 3–7 days from the onset of symptoms or infection of COVID-19 while condemning its use beyond 7 days. It further emphasises that the early transfusion of convalescent plasma can be beneficial, while delayed transfusion can have detrimental effects, strongly supporting the Indian Council of Medical Research (ICMR) guidelines.23 Further, Libster et al reiterated that early transfusion of high-titre convalescent plasma in COVID-19 infection could reduce the disease’s progression in elderly patients favouring the findings of our study.24Although overall mortality was similar in both the treatment groups, we found a reduction in the mortality on the transfusion of convalescent plasma within 3 days. In this study, we also found that if plasma transfusion after 3 days had no beneficial effect of reducing significantly high mortality, similar to the PLACID trial.18
Comparison with other studies
This study analysed all the critical parameters related to treatment with convalescent plasma, which included timing of transfusion, the dose of transfusion, and all clinical and laboratory parameters required for assessing COVID-19 infections. On review of various studies, we found few studies documented improvement in clinical and laboratory parameters. In contrast, other studies had shown neither improvement in the clinical status nor reduced mortality compared with the SMT alone or with the placebo treatment.4 18–21 25–28The noteworthy common short-coming observed was that most previous studies included severely affected COVID-19 patients who already had organ involvement or required mechanical ventilation. Further, baseline neutralising antibody titre was not performed in these studies, and the timing of transfusion was not mentioned, which is crucial to the expected outcome of convalescent plasma therapy. Donor neutralising antibody titre was not performed in many of these studies.18–24 However, Körper et al performed CAPSID trial on severe COVID-19 patients and found that after 21 days, success rate was higher in patients receiving convalescent plasma as compared with standard treatment alone. They performed a subgroup analysis of high titre versus low titre convalescent plasma and concluded that high titre convalescent plasma significantly reduces time to clinical improvement, significant reduction in time to discharge from hospital and better overall survival.29 Joyner et al further categorised convalescent plasma as high, medium and low titre, and found that patients not receiving mechanical ventilation had lower risk of death with transfusion of high titre plasma as compared with transfusion of low titre plasma.30 Kunze et al studied the effect of geographic distribution of donors and found death within 30 days was lower in group receiving near-sourced plasma than in group receiving distant- sourced plasma.31 This trial showed promising safety with transfusion of convalescent plasma which makes it a considerable treatment option.4
In this study, we strictly followed for the duration from screening to randomisation and transfusion within 3 days (primarily within 24 hours), but the duration from admission to transfusion could not be regulated as most of the patients were not fulfilling inclusion criteria on the day of admission. As a result of this, we could find that participants whose admission to randomisation (plasma transfusion) duration was less than 3 days had a better outcome. Although timely use of convalescent plasma has better outcomes, mortality was similar in both the study group, suggesting multifactorial pathophysiology of the disease. One of the reasons postulated was that the precise duration of onset of illness was unknown to most patients and their attendants. Additionally, in this study, we could find that the baseline titre of the patient had no role in patient outcomes in terms of mortality and reduction in ordinal scale with COPLA transfusion. Further applying this concept will reduce the delay in transfusion waiting for baseline titre results and unnecessary costs incurred by patients or the government based on the Indian council of medical research guidelines.23Among the benefits is that the collected plasma can be stored in the lyophilised form to overcome avoidable delay in the transfusion and make it readily available for COVID-19 patients for timely transfusion. In addition, it will further avoid delays due to the logistics and availability issues, even in remote areas.
Conclusion
Convalescent plasma with adequate antibody titres should be transfused in COVID-19 patients along with standard medical treatment in the initial 3 days of hospitalisation to SARS CoV-2 for better clinical outcomes.
Data availability statement
Data are available on reasonable request. Data (unpublished data in its row form in Microsoft excel sheet) will be available with principal investigator of the study and it will be available for researcher in unidentified data form on reasonable request to principal investigator till 5 years from date of publication. Rest all data relevant to the study are included in the article or uploaded as online supplemental information
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Institute of Liver and Biliary Sciences, New Delhi, Reference number or ID for ethics: IEC/2020/77/MA05. Participants gave informed consent to participate in the study before taking part.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @Nirupma
Contributors SKS, MB, SK, VD, PB, AM, PK, EG, NT, VS, CB and SST made the study concept and design; acquisition of data done by KC, AG, AN, RA, SA, JH, SJ, BKY, PS, GK and AB did statistical analysis;Drafting of the manuscript was done by PB, AM, PK, EG, NT, VS, CB, SST, VS, CB, SST, KC, AG, AN, RA, SA, JH, SJ, BKY, PS, GK and AB; critical revision of manuscript done for important intellectual content done by SKS, MB, VD, and SK. Administrative and technical support by SKS, MB and AM. Lead/guaranter of the study: SKS. Author responsible for the overall content as the guarantor: SKS and MB
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.