Article Text

Abstract
Objective To describe the clinical outcomes of COVID-19 in a racially diverse sample from the US Southeast and examine the association of renin–angiotensin–aldosterone system (RAAS) inhibitor use with COVID-19 outcome.
Design, Setting, Participants This study is a retrospective cohort of 1024 patients with reverse-transcriptase PCR-confirmed COVID-19 infection, admitted to a 1242-bed teaching hospital in Alabama. Data on RAAS inhibitors use, demographics and comorbidities were extracted from hospital medical records.
Primary outcomes In-hospital mortality, a need of intensive care unit, respiratory failure, defined as invasive mechanical ventilation (iMV) and 90-day same-hospital readmissions.
Results Among 1024 patients (mean (SD) age, 57 (18.8) years), 532 (52.0%) were African Americans, 514 (50.2%) male, 493 (48.1%) had hypertension, 365 (36%) were taking RAAS inhibitors. During index hospitalisation (median length of stay of 7 (IQR (4–15) days) 137 (13.4%) patients died; 170 (19.2%) of survivors were readmitted. RAAS inhibitor use was associated with lower in-hospital mortality (adjusted HR, 95% CI (0.56, (0.36 to 0.88), p=0.01) and no effect modification by race was observed (p for interaction=0.81). Among patients with hypertension, baseline RAAS use was associated with reduced risk of iMV, adjusted OR, 95% CI (aOR 0.58, 95% CI 0.36 to 0.95, p=0.03). Patients with heart failure were twice as likely to die from COVID-19, compared with patients without heart failure.
Conclusions In a retrospespective study of racially diverse patients, hospitalised with COVID-19, prehospitalisation use of RAAS inhibitors was associated with 40% reduction in mortality irrespective of race.
- COVID-19
- GENERAL MEDICINE (see Internal Medicine)
- EPIDEMIOLOGY
Data availability statement
Data are available on reasonable request. All data relevant to the study are available from the corresponding author on request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This study background was based on multiple questions regarding the safety of RAAS inhibitors raised by the community of the primary care physicians and patients in the beginning of the COVID-19 pandemic.
Other strengths of the study include a large racially diverse sample of patients with COVID-19 from the US Southeast and a robust approach to extraction of data from electronic health records.
Observational retrospective nature of this study does not allow drawing causal inferences.
Residual unmeasured confounding, such as socioecomonic status, may influence study results.
The study included patients from a limited geographical area and a single hospital site.
The data on out-of-hospital mortality and same-hospital readmissions may be incomplete as some COVID-19 patients may have been readmitted to other area hospitals.
Introduction
The USA has experienced an unprecedented public health crisis with the COVID-19 pandemic.1 Persons with cardiovascular and metabolic disease are at increased risk for mortality and morbidity from COVID-19.2–5 Cardiovascular disease and diabetes mellitus are highly prevalent among US adults, with 45% of adults having HTN, 13%—diabetes mellitus, 6.7%—coronary artery disease and 2.4%—heart failure.6 These chronic conditions disproportionally affect adults in the Southeast compared with other parts of the USA.6 Patients with hypertension, heart failure, diabetes and chronic kidney disease are often prescribed renin–angiotensin–aldosterone system (RAAS) inhibitors, that is, ACE inhibitors (ACEi) or angiotensin receptor blockers (ARBs). In animal studies, performed prior to the emergence of COVID-19, ACEi were found to increase the expression of ACE2 receptors.7 The SARS-CoV-2 binds to ACE2 receptors in lungs,8 leading to concerns about potential risks of using RAAS inhibitors in the setting of COVID-19. While subsequent studies have demonstrated the safety of RAAS inhibitor use among persons with COVID-19 and indication for RAAS use,9–11 the association of RAAS inhibitor use with hospital readmission after the index COVID-19 admission is not well described.
Most of reports12 describing the associations of pre-existing use of RAAS inhibitors with COVID-19 outcomes were obtained in White or Asian, not African American populations. Compared with Whites, African Americans have a high incidence of adverse effects of RAAS inhibitors.13 Disproportionally affected by multiple health disparities, African Americans have also been shown to have an increased risk of severe COVID-19, requiring hospitalisation.14 Persons of African descent were also at higher risk of contracting COVID-19 in the largest to date cohort study of the COVID-19 susceptibility in England.15
To better understand the association of baseline RAAS inhibitor use with outcomes of COVID-19 hospitalisation, we assembled an observational retrospective cohort of racially diverse hospitalised patients with laboratory-confirmed COVID-19 in Alabama. We examined whether baseline RAAS inhibitor use was associated with COVID-19 health outcomes, including (1) in-hospital mortality, (2) need for intensive care unit (ICU) admission (3) acute respiratory failure requiring invasive mechanical ventilation (iMV) and (4) same-hospital readmission for any cause among survivors of the COVID-19 index hospitalisation. We also assessed whether the association between RAAS inhibitor use and mortality differed by race.
Methods
Study participants and procedures
This observational retrospective cohort study included 1024 adult (age 18 and above) patients hospitalised with confirmed COVID-19 between 1 March 2016 and 16 September 2020 at the University of Alabama at Birmingham (UAB) teaching hospital in Birmingham, Alabama. The first cases of the COVID-19 were detected in Birmingham beginning on 1 March 2020. The cases increased very slowly over the spring of 2020, with a sharp surge 10–14 days after 4 July 2020. After the initial surge, COVID-19 cases declined slightly in August 2020, but then started to rise, achieving an spike in December–January 2021 (data not included in this report). The UAB ICU neared but did not exceed capacity. During the first surge of COVID-19 cases in July 2020, UAB Hospital implemented a delayed intubation strategy, favouring treating COVID-19 respiratory failure with supplemental oxygen, delivered via high flow nasal cannula. Therefore, all analyses of respiratory failure were adjusted for the time of the index admission for COVID-19 (before vs after 15 July 2020).
COVID-19 cases were confirmed by reverse-transcriptase PCR (rt-PCR). We extracted patient data electronically from our institution’s Electronic Health Record (EHR; Cerner) data warehouse (i2B2) supplemented by manual chart review. Data were prepared for analyses by the COVID-19 Core data Extraction/Transformation team using Oracle SQL developer (V.11.2). For each of the patients with laboratory-confirmed COVID-19, encounter data for the index admission were obtained, including admission date, date of the earliest positive rt-PCR for COVID-19 and death or discharge date. The admission/discharge dates for all subsequent outpatient and inpatient encounters and dates of death after the index hospitalisation were also electronically extracted. For each of the hospital readmissions (n=172) a manual chart review was conducted to confirm admission/discharge dates. For each of the deaths (n=16) that occurred after index hospitalisation we conducted manual chart review for confirmation. From the initial sample of 1029 patients, we excluded 5 patients with missing index admission dates or missing dates of birth.
Patient and public involvement
No patients involved.
Outcomes and main exposure
Study outcomes included in-hospital COVID-19-related mortality, need for the ICU admission, respiratory failure defined by a need for iMV, and same-hospital readmission for any cause after the index hospitalisation. Data on RAAS inhibitors included use of ACEis and ARBs prior to the index COVID-19 hospitalisation, and were derived from the index admission medication reconciliation data in the EHR. If patients were taking a combination medicine that included an ACEi or ARB as one of the components, they were classified as having been prescribed ACEi/ARB in the analysis.
Covariates
Covariates were selected on the basis of the risk factors for severe COVID-19 infection identified by the Centers for Disease Control and Prevention and previous reports on COVID-19 morbidity and mortality.16–19 Patient sociodemographic characteristics included age at the index admission (calculated, using birth and admission dates) and self-reported race, sex, marital status and cigarette smoking status. We created age categories as follows: 18–40, 41–64, 65–74 and 75 years and older. Body mass index (BMI) was calculated using height and weight obtained most recently prior to the index COVID-19 admission. BMI categories included: ‘underweight’ is less than 18.5 kg/m2, ‘normal weight’ 18.5–24.9 kg/m2, ‘overweight’ 25–29.9 kg/m2 and ‘obese’ 30 kg/m2,and above. We obtained data on comorbidities, including hypertension, coronary artery disease, diabetes, chronic obstructive pulmonary disease, heart failure, chronic kidney disease, HIV, sickle cell disease and history of solid organ transplant using corresponding, Intenational Classification of Diseases, The Tenth Revision (ICD-10) codes.
Statistical analysis
Patients with COVID-19 who were prescribed RAAS inhibitors at baseline were compared with those who were not prescribed RAAS inhibitors using two-sided t-tests for continuous variables and χ2 tests for categorical variables. We examined the association of RAAS inhibitor use with study outcomes in three different samples: (1) overall sample, (2) patients with any indication for RAAS inhibitor use, such as hypertension, diabetes, chronic kidney disease, coronary artery disease or heart failure and (3) patients with hypertension. Outcomes were assessed with unadjusted and multivariable models. To examine the association of in-hospital mortality from COVID-19 with baseline RAAS inhibitor use we constructed Cox proportional hazards regression models adjusted for age, sex, race, marital status, smoking, BMI and medical conditions. We created an interaction term between RAAS use and race to test for effect modification by race in the fully adjusted models of COVID-19 in-hospital mortality. The need for ICU and the presence of respiratory failure were examined separately in logistic regression models, with adjustment for the same patient characteristics and for the time of admission (before vs after 15 July 2020).
We examined the charts of the survivors of the index COVID-19 admission postdischarge for a same-hospital readmission for any cause using medical records. The EHR data were abstracted for any subsequent in-hospital and outpatient encounter after the index hospitalisation and UAB hospital readmission dates were extracted. The time to readmission was calculated using index discharge data and readmission date. To examine the association between baseline RAAS use and readmissions, we used the Fine and Gray model to account for competing risk of death in the post-discharge period that was adjusted for the same patient characteristics. The proportionality assumption was tested and satisfied in the Cox proportion hazards models. All statistical analyses were performed in SAS software (SAS Institute) V.9.4,
Results
Among 1024 patients, admitted to UAB hospital with COVID-19 (mean (SD) age, 57 (18.8) years), 532 (52%) were African American, 514 (50 %) were male, 493 (48 %) had hypertension, 323 (32 %) had heart failure, 487 (48 %) were obese, 210 (20.5%) had diabetes and 98 (11 %) were current smokers (table 1). There were 365 (36%) patients taking RAAS inhibitors at baseline. Patients with baseline RAAS use were older, more likely to be African American, and had more comorbidities.
Characteristics of patients, admitted to UAB hospital with COVID-19, between 1 March 2020 and 16 September 2020
The median length of stay (LOS) for the index COVID-19 hospitalisation was 7 days, (IQR 4–15 days). Maximum LOS was 175 days. Sixty per cent of included COVID-19 cases were admitted after the initial surge in Birmingham, between 15 July 2020 and 16 September 2020. During the index hospitalisation, 137 (13.4%) patients died. Additionally, 16 (1.8%) patients died from any cause postdischarge, either during a hospital readmission or out of the hospital. Cumulative all-cause mortality included 153 (14.9%) deaths. At the time of the cohort assembly on 16 September 2020, 23 patients remained in the hospital. During the index hospitalisation 466 (45.5%) patients required ICU care, and 276 (27%) persons required iMV. The proportion of patients who were intubated was higher in the early period, before 15 July, compared with the period of after 15 July 2020, when placing the patient with respiratory failure on high flow nasal canula became a preferred treatment strategy: 201 (32.4%) vs 75 (18.6), p<0.001.
In-hospital COVID-19 mortality and RAAS use
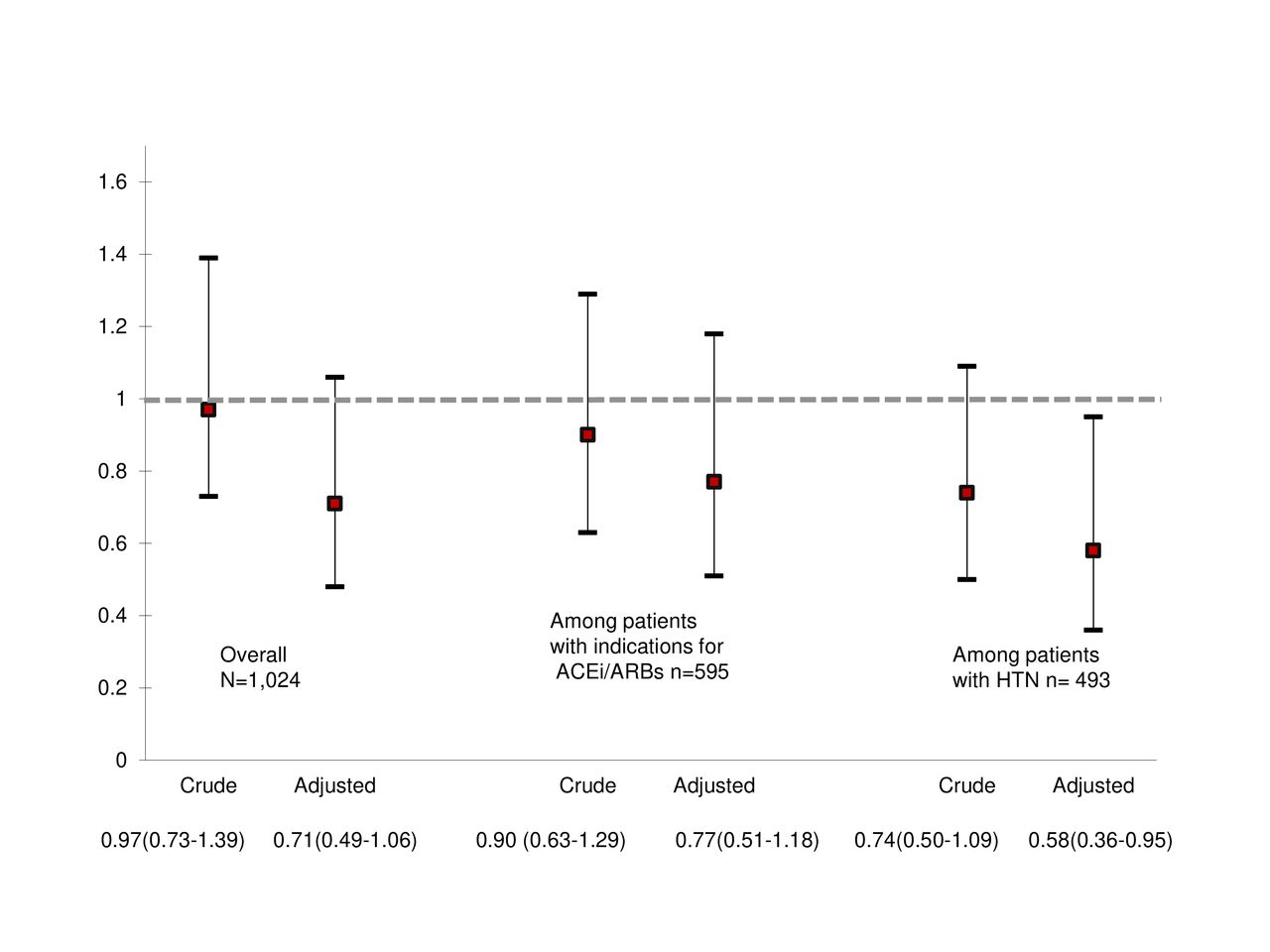
The median time to death was 13 days (IQR 6–20 days). In the overall study sample, baseline RAAS inhibitor use was associated with significantly reduced risk of in-hospital mortality (adjusted HR (aHR) 0.56, 95% CI 0.36 to 0.88), p=0.01, after adjustment for all covariates) (figure 1). A similar protective effect of RAAS inhibitor use on mortality was observed among patients with any indication for RAAS inhibitor use (aHR (95% CI) for RAAS inhibitor use 0.59, 95% CI 0.37 to 0.94, p=0.03) and among patients with hypertension (aHR for RAAS use 0.54, 95% CI 0.33 to 0.90, p=0.02). We did not observe effect modification by race in the overall sample. The RAAS inhibitor use*race interaction term had associated p=0.81. Compared with Whites, African American race was not associated with in-hospital mortality from COVID-19 in the adjusted model (aHR 0.88, 95% CI 0.60 to 1.29, p for trend 0.55) (table 2). Other factors associated with increased cumulative mortality in our sample included age 65–74 years (aHR 3.67 (95% CI 1.85 to 7.31)), age 75 years and older (aHR 4.89 (95% CI 2.36 to 10.14)), obesity (aHR 2.10 (95% CI 1.34 to 3.29)) and pre-existing heart failure (aHR 1.88 (95% CI 1.20 to 2.94)) (table 2).

COVID-19 in-hospital mortality, HR, 95% CIs for ACE inhibitors/angiotensin receptor blocker (ACEi/ARB) use. Figure 1 presents crude and adjusted HRs and 95% CIs for in-hospital COVID-19 mortality. Indications for ACEi/ARB use included HTN, chronic kidney disease, coronary artery disease, diabetes and heart failure. Overall model adjusts for age, race, sex, marital status, smoking, BMI categories and medical conditions: HTN, chronic kidney disease, coronary artery disease, diabetes, heart failure, HIV, COPD, history of solid organ transplant. among those with indication for RAAS inhibitor, model adjusts for age, race, sex, marital status, smoking, BMI categories, and medical conditions: HIV, COPD, history of solid organ transplant. Among those with HTN, model adjusts for age, race, sex, marital status, smoking, BMI categories and medical conditions: chronic kidney disease, coronary artery disease, diabetes, heart failure, HIV, COPD, history of solid organ transplant.Abbreviations: BMI, body mass index; COPD, chronic obstructive pulmonary disease; HTN, hypertension, RAAS, renin–angiotensin–aldosterone system.
Factors, associated with in-hospital mortality among patients with COVID-19, admitted to UAB Hospital, between 1 March 2020 and 16 September 2020
COVID-19 in-hospital events and RAAS inhibitor use
RAAS inhibitor use was not associated with the need for ICU in all analyses (figure 2.) In the overall patient sample, RAAS use was not associated with iMV, aOR 0.71 (95% CI 0.48 to 1.06) (figure 3). In contrast, among patients with hypertension, baseline RAAS inhibitor use was significantly associated with reduced odds of iMV after adjustment for covariates (aOR 0.58 (95% CI 0.36 to 0.95), p=0.03). African Americans admitted with COVID-19 were more likely to have respiratory failure, requiring iMV: aOR 1.58 (95% CI 1.01 to 2.31), p=0.02. Other factors associated with the increased risk of iMV for the COVID-19-related respiratory failure included current cigarette smoking (aOR 1.80 (95% CI 1.08 to 3.02), p=0.03), pre-existing heart failure (aOR 2.32 (95% CI 1.45 to 3.71), p<0.001) and being admitted to UAB before 15 July 2020 (aOR 1.97 (95% CI 1.39 to 2.79), p<0.0010.

Intensive care use, OR, 95% CI for ACE inhibitor/angiotensin receptor blocker (ACEi/ARB) use. Figure 2 presents crude and adjusted ORs and 95% CIs for in-hospital COVID-19 mortality. Indications for ACEi/ARB use included HTN, chronic kidney disease, coronary artery disease, diabetes and heart failure. Overall model adjusts for age, race, sex, marital status, smoking, BMI categories, and medical conditions: HTN, chronic kidney disease, coronary artery disease, diabetes, heart failure, HIV, COPD, history of solid organ transplant. Among those with indication for RAAS inhibitor, model adjusts for age, race, sex, marital status, smoking, BMI categories and medical conditions: HIV, COPD, history of solid organ transplant. Among those with HTN, model adjusts for age, race, sex, marital status, smoking, BMI categories and medical conditions: chronic kidney disease, coronary artery disease, diabetes, heart failure, HIV, COPD, history of solid-organ transplant. BMI, body mass index; COPD, chronic obstructive pulmonary disease;Abbreviations: ICU, intensive care unit; BMI, body mass index; COPD, chronic obstructive pulmonary disease; HTN, hypertension, RAAS, renin–angiotensin–aldosterone system.

{kind=link}
{kind=link}
{kind=link}
Respiratory failure, requiring invasive mechanical ventilation, OR, 95% CIs, for ACE inhibitor/angiotensin receptor blocker (ACEi/ARB) use. Indications for ACEi/ARB use include HTN, chronic kidney disease, coronary artery disease, diabetes and heart failure. Overall model adjusts for age, race, sex, marital status, smoking, BMI categories, and medical conditions: HTN, chronic kidney disease, coronary artery disease, diabetes, heart failure, HIV, COPD, history of solid organ transplant, time of admission (before vs after 15 July 2020). Among those with indication for RAAS inhibitor, model adjusts for age, race, sex, marital status, smoking, BMI categories and medical conditions: HIV, COPD, history of solid-organ transplant, time of admission (before vs after 15 July 2020). Among those with HTN, model adjusts for age, race, sex, marital status, smoking, BMI categories and medical conditions: chronic kidney disease, coronary artery disease, diabetes, heart failure, HIV, COPD, history of solid organ transplant, time of admission (before vs after 15 July 2020).Abbreviations: BMI, body mass index; COPD, chronic obstructive pulmonary disease; HTN, hypertension; RAAS, renin–angiotensin–aldosterone system.
Same-hospital 90-day readmissions among COVID-19 survivors
Over a median follow-up of 51 (IQR 28–82) days, 170 (19.2%) of 887 discharged patients were readmitted to the same hospital for any cause (table 1). Among those who were rehospitalised, the median time to readmission following the index discharge was 10 days (IQR 4–29 days). The proportion of persons with same-hospital readmission among those with baseline RAAS inhibitor use was 23.5%, compared with 16.7% among those who were not prescribed RAAS inhibitors (p=0.01) (table 1). In the fully adjusted Cox proportional models, accounting for death as a competing risk, baseline RAAS agent use was not associated with readmissions (table 3). Compared with white patients, patients of the Hispanic/Latino/Asian or other race/ethnicity were less likely to be readmitted (aHR 0.42, 95% CI 0.20 to 0.90). African American race was not statistically significantly associated with hospital readmission (aHR 1.11, 95% CI 0.78 to 1.60). Among the chronic medical conditions only diabetes was significantly associated with higher risk for same-hospital readmission after the index COVID-19 admission (aHR 1.56, 95% CI 1.02 to 2.94).
Factors associated with same-hospital readmission among patients with COVID-19, between 1 March 20201 and 16 September 2020
Discussion
This study presents data from 1024 patients with COVID-19 admitted to a teaching hospital in Alabama. Results of this study support the safety of maintaining patients with chronic conditions on ACEis and ARBs during the COVID-19 pandemic and expands previous reports by demonstrating the protective effect of the ACEis/ARBs from mortality in a racially diverse sample of patients with COVID-19. Among patients with hypertension, the use of ACEis/ARsB prior to contracting COVID-19 was associated with a reduction in the likelihood of endotracheal intubation by nearly 40%. Further, ACEi/ARB use was not associated with greater need for ICU-level care or with an increase in the same-hospital readmissions.
Baseline use of ACEi/ARB was associated with 40% lower in-hospital mortality in patients with COVID-19, after controlling for potential confounders such as age, sex, race, obesity, smoking and chronic medical conditions. These results were similar in the sample of patients who had any indication for RAAS inhibitors, and in patients with hypertension. Previous research has shown no association between the use of RAAS inhibitors and susceptibility to COVID-19,20 and has demonstrated the safety of continuing these medications during the pandemic.10 11 21 Similary to our results, in 1.4 million patients with hypertension, heart failure, diabetes, kidney disease or ischaemic heart disease registered in the Swedish National Patient Registry, ACEi/ARB use was associated with a reduced mortality in COVID-19 cases (aHR 0.89, 95% CI (0.82 to 0.96)).22 Our study expands on previous findings by demonstrating both safety and reduction in COVID-19-related mortality associated with RAAS inhibitor use in a racially diverse sample where 50% of patients were African American. Potential mechanisms of protective effects of ACEi/ARB in COVID-19 are not well understood. One of the potential explanations of the decreased mortality among patients on ACEi/ARB medications prior to COVID-19 is that patients’ chronic conditions were better controlled before the infection, which, in turn, reduced complications of COVID-19. Another body of research suggests that prolonged RAAS use may, in fact, downregulate ACE2 receptor expression, limit inflammation and reduce lung injury in COVID-19.23–25 Unfortunately, the design of our study does not allow us to prove or disapprove this hypothesis.
Half of the patients hospitalised with the COVID-19 infection in our sample were African American, whereas the proportion of African Americans in Alabama is only 26.7%. This finding highlights the racial disparity in the COVID-19 pandemic, in which a higher proportion of African Americans developed severe COVID-19 infection, requiring hospitalisation,26 compared with Whites. African Americans were also more likely to require iMV in our study. However, similar to other studies of COVID-19 outcomes in the US,27 race was not an independent predictor of death or hospital readmission in our study.
Our findings confirm previous observations that advanced age, obesity, and comorbidities are associated with death from COVID-19.16 28 Importantly, more than 30% of our patient sample admitted with severe COVID-19 had pre-existing heart failure, a rate almost 10 times higher than the prevalence of heart failure in the general population. Heart failure was the only chronic condition, in addition to age and obesity in our sample, that was independently associated with increased in-hospital mortality from complications related to COVID-19. Patients with heart failure were also at increased risk of developing respiratory failure, requiring iMV. These represent a particularly vulnerable group requiring special attention from healthcare to reduce mortality and morbidity from the COVID-19.29 30
The rate of same-hospital readmissions among COVID-19 survivors was 19%, similar to that in a recent study of the patients with COVID-19, treated in the Veterans Affairs hospital system31 but higher, than in other reports estimating that only 3%–10% of patients were rehospitalised after the index COVID-19 admission.32 33 The high rates of hospital readmission in our study sample may be explained by the high level of chronic disease prevalence and worse general health in the general population of Alabama. Importantly, diabetes was significantly associated with increased re-admission risk among COVID-19 survivors. Alabama has the third highest prevalence of diabetes among adults (14%) in the USA, according to the National Diabetes Statistics Report-2020 by the Centers of Disease Control. Our findings are likely to extend to states with a similar high prevalence of diabetes mellitus and underscore the importance of close outpatient follow-up of this at-risk population.
Study limitations include limited geographical area and single hospital site. The data on out-of-hospital mortality and same-hospital readmissions may be incomplete, as some COVID-19 patients may have been readmitted to other area hospitals. On average 30% of patients originally admitted to the UAB hospital are readmitted to other hospitals. The observational retrospective nature of this study does not allow drawing causal inferences. Additionally, residual unmeasured confounding, such as socioecomonic status, may influence study results. EHR data regarding pre-existing medical conditions and smoking may be incomplete. Strengths of the study include a large racially diverse sample from the US Southeast, a region disproportionally affected by COVID-19 and high prevalence of multiple comorbidities. Further, we were able to develop a robust approach to extraction of data from EHR and assemble a cohort of the patients with COVID-19.
In conclusion, in this retrospective study, the use of RAAS inhibitors was associated with decreased in-hospital mortality from COVID-19 in a racially diverse sample. RAAS inhibitor use was not associated with ICU-level care or hospital readmissions in the cohort of patients with COVID-19, while patients with diabetes were at a high risk for same-hospital readmission. Among patients with hypertension, baseline RAAS inhibitor use was associated with a reduced risk of iMV. This retrospective study may support the continuation of RAAS inhibitors during the COVID-19 pandemic unless there are contraindications for these pharmacological agents.
Data availability statement
Data are available on reasonable request. All data relevant to the study are available from the corresponding author on request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants but University of Alabama in Birmingham. Protocol number is IRB-300005431 exempted this study. This study includes data from medical records. No patient contact.
Acknowledgments
The authors would like to thank Ryan Wong, Jackson Hoelsey, UAB Informatics Institute’s Data Extraction Team (Matt White and Dale Dickinson), Data Transformation Team (Suneetha Thogaripally, Mohit Varshney, Greer Bukholder, MD, and Alfredo Guzman) and UAB Center for Outcomes Effectiveness Research and Education (especially Alia Tunagur) for all the help in coordinating the dataset assembly.
References
Footnotes
Twitter @ParagGoyalMD
Contributors YK and JW responsible for the overall content as the guarantors. YK delineated project idea and design, conducted data analysis and drafted the manuscript. YK and GM conducted data management and analysis. YK, GM and JW had full access to data and ensured the accuracy or integrity of data. SC, RF, MMS, PG, SO, ALC and EAJ edited and revised the manuscript. All authors provided substantial contributions to the conception or design of the work; interpretation of data; revising the draft critically for important intellectual content and final approval of the version to be published.
Funding The National Center for Advancing Translational Sciences of the National Institutes of Health supported this research in part under award number UL1TR001417. YK is supported by the UAB School of Medicine Special Covid-19 funding mechanism and NHLBI T32 HL007457 'Mechanisms of Hypertension and Cardiovascular Diseases'.
Disclaimer The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Competing interests ALC reports serving as a consultant for Bayer. EAJ reports research funding from NIH, and Amgen; editorial board membership: Circulation: Cardiovascular Quality and Outcomes; consulting: American College of Cardiology and McKesson; Expert witness for DeBlase Brown Everly.; and royalties for UpToDate. MMS reports research funding from Amgen. SO reports research funding from Bayer, CinCor Pharma, George Medicine and Idorsia Pharmaceuticals. Other authors report no conflict of interest
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.