Article Text

Abstract
Purpose The purpose of the Loma Linda University Health (LLUH) BREATHE cohort is to test the efficacy of a novel method of continuously incentivising participation in workplace smoking cessation on participation, long-term abstinence, health outcomes, healthcare costs and healthcare utilisation.
Participants In 2014, LLUH—a US academic medical centre and university—incentivised participation in a workplace smoking cessation programme (LLUH BREATHE) by lowering health plan costs. Specifically, LLUH introduced a Wholeness Health Plan (WHP) option that, for the smokers, continuously incentivises participation in nicotine screening and the LLUH BREATHE smoking cessation programme by offering an ‘opt-in wellness discount’ that consisted of 50%–53% lower out of pocket health plan costs (ie, monthly employee premiums, copayments). This novel ‘continuously incentivised’ model lowers annual health plan costs for smokers who, on an annual basis, attempt or maintain cessation from tobacco use. The annual WHP cost savings for smokers far exceed the value of short-term incentives that have been tested in workplace cessation trials to date. This ongoing health plan option offered to over 16 000 employees has created an open, dynamic LLUH BREATHE cohort of current and former smokers (n=1092).
Findings to date Our profile of the LLUH BREATHE cohort indicates that after 5 years of follow-up in a prospective cohort study (2014–2019), continuously incentivised smoking cessation produced a 74% participation (95% CI (71% to 77%)) in employer-sponsored smoking cessation attempts that were occurring less than a year after the incentive was offered. The cohort can be purposed to examine the effect of continuously incentivised cessation on cessation outcomes, health plan utilisation/costs, use of electronic nicotine delivery systems, and COVID-19 outcomes.
- EPIDEMIOLOGY
- PUBLIC HEALTH
- COVID-19
Data availability statement
Data are available upon reasonable request. De-identified data are available upon reasonable requests for pooling projects and meta-analyses.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of the study
An open employee cohort of over 16 000 that is continuously incentivised through health plan discounts to maintain abstinence or attempt cessation from tobacco.
Linkages to a wide range of employee cohort data on health outcomes, health plan utilisation costs and cessation outcomes.
Findings are based on a cohort of university and medical centre employees and the effects of incentives need investigation in other employee groups.
Introduction
Loma Linda University Health (LLUH) is an academic medical centre with over 16 000 employees working in eight health science schools, six hospitals and a physician practice corporation. In 2014, LLUH introduced an option within the employee health plan—The Wholeness Health Plan (WHP)—that provided employees with an ‘opt-in wellness discount’ that consisted of 50%–53% lower out of pocket health plan costs (ie, monthly employee premiums, copayments for prescriptions).1 The rationale for the WHP ‘opt-in wellness discount’ was to address the burdens caused by social determinants of employee health by investing health plan resources in an incentivised prevention model.
To qualify for the WHP ‘opt-in wellness discount’, employee smokers (identified through self-report, health claims data, organisationwide health risk assessments (HRAs) and biometric screening) were required to participate in LLUH BREATHE—the WHP’s smoking cessation programme.1
A particularly innovative feature of the LLUH BREATHE smoking cessation model was that the ‘opt-in wellness discount’ through the WHP was available to all employee smokers as long as they met the requirement of annual participation in smoking cessation for current employee smokers. Thus, employee smokers on the WHP were continuously incentivised into smoking cessation through two mechanisms: (1) WHP members who had participated in the LLUH BREATHE smoking cessation programme and did not relapse, maintained their ‘opt-in wellness discount’ through the WHP and (2) WHP members who had participated in the LLUH BREATHE smoking cessation programme but later relapsed were required to enrol in the annual LLUH BREATHE smoking cessation programme in order to maintain their ‘opt-in wellness discount’ through the WHP. Additional features of the ‘continuous incentive’ model include: (1) WHP members who were non-smokers or never-smokers since hiring retain their ‘opt-in wellness discount’ by either maintaining abstinence or enroling in the annual LLUH BREATHE smoking cessation programme and (2) employee smokers who did not enrol in the WHP could, during an annual buy-in period, revisit that choice and ‘opt-in’ to WHP and the requirement to participate in smoking cessation.
This organisational model of continuously incentivised employee smoking cessation implemented at LLUH provides a ‘natural experiment’ to prospectively study the LLUH BREATHE cohort—a dynamic, open employee cohort of current smokers (non-participants in LLUH BREATHE), former smokers (cessation through LLUH BREATHE) and relapsed smokers (relapse after cessation through LLUH BREATHE) who are, on a continuous basis, offered an ‘opt in’ incentive (ie, discounted WHP coverage) by their employer to attempt, achieve or maintain abstinence from tobacco smoking.
The overall aim of this report is to provide a cohort profile of the first 5 years of follow-up (2014–2019) of the LLUH BREATHE cohort that enables the development of a research framework for a longitudinal study of the effects of a continuously incentivised employee smoking cessation model on a wide range of population health outcomes. The cohort profile will include the most current 5-year estimate of participation rate, temporal trends during 5 years of enrolment and future plans of analysis of high impact outcomes of incentivised smoking cessation model (ie, early and long-term abstinence, relapse patterns, healthcare utilisation, health economics, COVID-19 outcomes).
The secondary analysis of these health plan data received IRB approval (IRB #5170126) from the Institutional Review Board of Loma Linda University.
Cohort description
How did we develop the Wholeness Health Plan that produced the LLUH BREATHE cohort?
Background of the WHP
LLUH is an innovator in Wellness and Population Health
LLUH is a Seventh-day Adventist institution that as part of its mission to ‘Keep Man Whole’ promotes specific faith-based principles of healthy lifestyle and disease prevention in its healthcare, academic teaching, administration and campus and hospital environment.2 3 These include avoidance of tobacco and alcohol, and adherence to a plant-based diet pattern that encourages consumption of specific plant foods (ie, legumes, nuts) in place of animal products.2 Academic entities of LLUH (Schools of Medicine, Public Health) have completed more than 60 years of landmark prospective cohort studies of healthy lifestyle behaviors (1960 Adventist Mortality Study, 1976 Adventist Health Study-1, 2002 Adventist Health Study-2)4 5 that have been funded by the US National Institute of Health. These studies have documented how healthy lifestyle behaviours (avoidance of tobacco and alcohol, plant-based diet patterns) practised by Seventh-day Adventists are associated with lower risk of cancer, coronary heart disease, stroke, diabetes and a longer life expectancy.2 6
Living Whole Employee Wellness Programme at LLUH
The Department of Risk Management at LLUH administers a health plan that is offered to all benefit-eligible employees and their families. The health plan is employer-sponsored and designed to reimburse a broad range of medical expenses for benefit-eligible employees. To align the health plan with LLUH mission-focused principles on wellness, the Department of Risk Management implemented the Living Whole Employee Wellness programme to provide a comprehensive range of wellness and disease management services to support employee health. Employees could participate in this programme voluntarily. The programme included but was not limited to programmes on weight management, diabetes management through lifestyle interventions, smoking cessation and cooking classes.
Development of the WHP at LLUH
In 2014, the Department of Risk Management expanded on the success of the Living Whole Employee Wellness Programme by incorporating incentivised wellness options into a new employer-provided health plan option (WHP) that was based on an ‘opt-in wellness discount’. The wellness discount consisted of a 50%–53% reduction in out of pocket health plan costs (monthly costs, copays for prescriptions) in the existing health plan options from LLUH Risk Management. The rationale for WHP was as follows: (1) participation in a biometric screening, a HRA, and distribution of wellness and prevention information at enrolment empowered each health plan member and their families to be actively involved in managing personal health and wellness and (2) the biometric screening and HRA data obtained at enrolment allowed the health plan to assess member health to enhance the precision of health/wellness resources and population health interventions that are offered. Employees received the wellness discount through WHP enrolment if they completed a biometric screening, a HRA, created an account in the hospital’s patient/doctor portal and agreed to participate in a care management programme based on results obtained from the screening and risk assessments. The care management programme included (1) biometric result review appointments with a primary care physician, (2) appointments with a nurse care manager for health plan members classified as high risk and/or multiple chronic diseases and (3) smoking cessation for those identified as tobacco users based on either self-reported HRA or biometric screening.
LLUH Breathe cohort: a natural experiment to study employee smoking cessation that is continuously incentivised by the employer-provided WHP
The LLUH Breathe cohort can be used to study the effects of an innovative model to continuously incentivise employees who are current or former smokers to continue quit attempts or maintain abstinence from smoking tobacco. To provide a context for our methods of studying the effects of LLUH BREATHE, we describe and compare the efficacy of incentive-based smoking cessation models used by other organisations. Incentive-based programmes fall into the categories of reward-based incentives, cash-based incentives, deposit-based incentives, lottery-based or completion-based incentives and mixed models using a combination of these approaches.7
Reward-based incentives
Programmes at CVS Pharmacy8 9 and Blue Cross/Blue Shield10 have used a reward-based mechanism (US$100 to US$800 in value), whereby at key smoking cessation milestones (quit date set, quit date, 14-day/30-day/6-month point prevalence abstinence) reward points are earned towards (1) subsidised copayments and costs for prescription and over the counter cessation aids and (2) redemption as cash credits for groceries and personal items in selected stores.
Cash-based incentives
Direct cash-based incentives include models that provide cash payments for attending a health assessment for smoking cessation (ie, US$50 for a first appointment and setting a quit date) and then provide payments on achieving abstinence goals (amounts summing from US$120 to in excess of US$800 for long-term abstinence).7
Deposit-based incentives
Under deposit-based incentives, subjects deposit money into a health savings account and are refunded on achieving abstinence goals.8
Competition and lottery-based incentives
This incentive model included designs, where groups of employees compete against each other for cash prizes given to the highest cessation rate.11 Also, in lottery-based incentive programmes (‘Quit and Win’), an individual employee in the cessation group is eligible to win a cash prize.11
Mixed models
Under the mixed models,8 combinations of reward, cash, deposit-based and/or competition/lottery-based incentives are used. For example, reward points for cessation behaviours can be redeemed as cash. Also, deposits are often combined with cash incentives in excess of the amount deposited by a smoker who quits.
Comparison of incentive models with LLUH BREATHE
Several large-scale meta-analyses of the incentive models have consistently shown that cash/reward-based incentives have higher participation and efficacy than deposit or competition/lottery-based incentives.7 11 Moreover, in direct comparison of these models in CVS/Caremark employees, Halpern et al specifically demonstrated the efficacy of cash/reward programmes that used higher value (up to US$800) incentives.8 9
Relative to previous incentivised models, LLUH BREATHE provides a novel approach to incentivised intervention that consists of: (1) a mixed model of cash-based (a lower paycheck deduction for health plan coverage equates to more cash per pay period; paycheck indicates a higher amount due to a discounted health coverage deduction printed on the paycheck) and reward-based incentives (lower copays for prescriptions), (2) a socioecologic framework, whereby participants are choosing smoking cessation as part of a personal and familial/spousal choice to ‘opt-in’ to the WHP directed choices of health and wellness programmes and (3) a continuous incentive as a WHP member to continue quit attempts or maintain abstinence from tobacco use.
How did we enrol the LLUH BREATHE cohort?
Organisation-wide biometric screening for WHP enrols the LLU BREATHE cohort
Overview
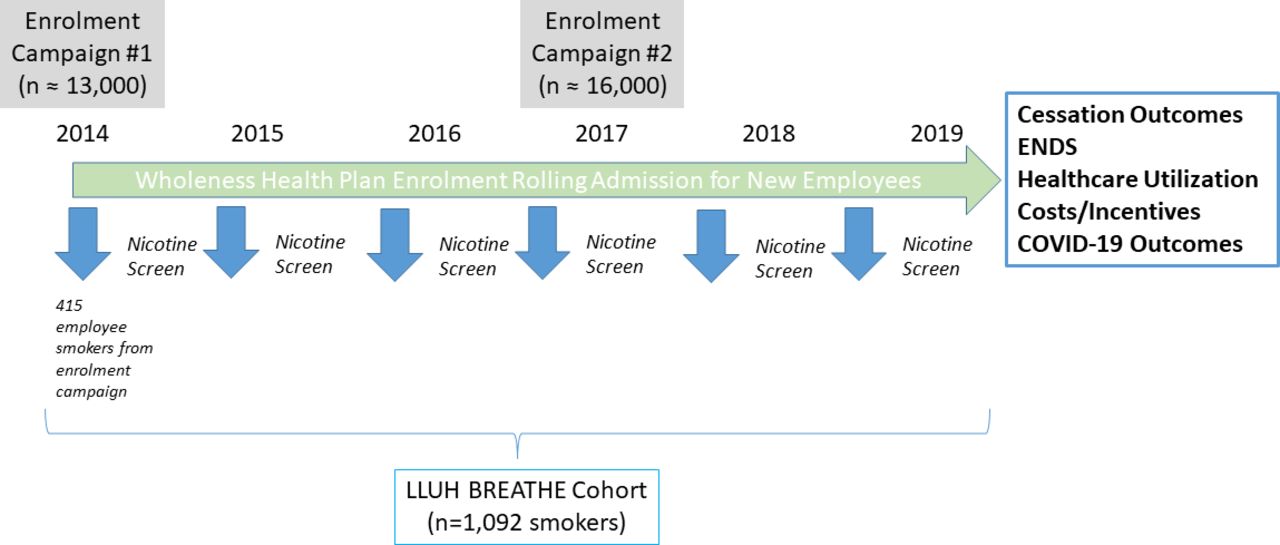
At the inception of the WHP as a health plan option in 2014, WHP enrollees underwent a series of biometric screenings and HRAs to provide employee health profile data. The biometric screening and HRAs were done as an organisationwide enrolment campaign during specific open-enrolment periods in November of 2014 and 2017. New hires were enrolled into the WHP on a rolling enrolment basis. Benefit-eligible employees have the opportunity to enrol in the WHP and qualify for the wellness discount every year. The biometric screenings and HRAs during 2014–2019 identified a cohort of employee smokers who were offered participation in employer-sponsored smoking cessation as part of the WHP wellness activities. This cohort became the LLUH BREATHE cohort (n=1092) described in this report and is depicted in figure 1 and table 1.

Enrolment of LLUH BREATHE employee smoker cohort (2014–2019). ENDS, electronic nicotine delivery systems; LLUH, Loma Linda University Health.
Demographics and health among LLUH employees who tested positive for nicotine and were offered participation in an incentivised health plan model for smoking cessation
WHP screening and risk assessment
During organisationwide health plan enrolment campaigns in 2014 and 2017, advertising for the WHP’s wellness discount activities began with a formal letter sent by mail to each benefit-eligible employee’s home. Subsequent communications were via postcard, email, mass telephone communications, fliers sent to each department, announcements posted in the organisation’s internal home webpage and articles in the employee newsletter. All communications invited employees to biometric screening and HRA appointments
Biometric screenings were made available at the workplace to all employees through a third-party vendor and included anthropometric assessment, a metabolic panel and screening for nicotine exposure (by self-report and health plan claims data during 2014–2017; by salivary cotinine test from 2017 to 2019). Rolling admissions into the health plan outside these periods in 2014 and 2017 used a similar methodology. A HRA questionnaire included sections on health behaviours, psychological stress and personal safety.
Nicotine screening during health plan enrolment
Nicotine screening results from self-report, health plan claims data or salivary cotinine testing were used to offer all employee smokers’ smoking cessation through their ‘opt in’ for the WHP. Health Plan members were given a chance to appeal ‘nicotine-positive’ results and, if approved, allowed to enrol in the WHP without the requirement for smoking cessation as habitual tobacco user.
Smoking cessation interventions for WHP members
The intervention has been described elsewhere.1
Briefly, Cohort members who participated in the intervention were asked to complete two electronic survey forms (intake/preintervention and postintervention), two physician visits and either an online or in-person group version of the American Lung Association ‘Freedom from Smoking’ course. This was an 8-week course that educated participants on the benefits of smoking cessation and assisted individuals in setting a ‘quit date’. This programme consisted of 8 weekly sessions that took approximately 1 hour to complete.
Relapse in WHP members
Relapses were detected through voluntary self-report to provider, health plan claims data or salivary cotinine testing during opt-in enrolment periods. It is noteworthy, however, that a relapsed WHP smoker who continues annual quit attempts on the LLUH BREATHE programme remains a WHP member.
Statistical analysis
To achieve our overall aim of providing a cohort profile, we conducted analyses to give the latest participation rate in the cohort and to provide temporal trends in screening, enrolment and completion of smoking cessation of the employee smokers. Participation rates and 95% CIs were computed with a continuity correction.12 Participants and non-participants were compared in χ2 and t tests.12 A non-parametric kernel smoother13 was used to examine the trends in count-based data on smoking cessation attempts, invites and screens for tobacco use.
Patient and public involvement
The data for this cohort study are from the employee health plan of a private non-profit organisation. It was not appropriate or possible to involve patients or the public in the design, or conduct, or reporting or dissemination plans of our research.
Findings to date
LLUH BREATHE cohort profile at 5 years of follow-up (2014–2019)
Our group has reported that, during the first year of follow-up, there was a 73% participation rate among in the continuously incentivised model of employee smoking cessation in LLUH BREATHE.1 The first year cessation rate of LLUH BREATHE participants was also notably high (48% achieved a 4-month point prevalence abstinence).1 Pilot qualitative data provide preliminary clues that the WHP cohort members and their providers are receptive to the incentivised intervention model.14
During the first 5 years of follow-up, the cohort grew to 1092 current and former (quit through screening and incentivised cessation sponsored by health plan) employee smokers identified among more than 16 000 employees (figure 1). The continuously incentivised model produced a 74% (95% CI (71% to 77%)) participation in an at least one employer sponsored, annual smoking cessation attempt during the follow-up. In table 1, we compare the biometric profiles of participants and non-participants in smoking cessation among LLUH BREATHE cohort members and found no significant differences. Total cholesterol was, however, higher in non-participants. We note that the unique design of LLUH BREATHE is such that non-participants can become participants during annual ‘opt in’ periods.
In figure 2 (panel 1), we show that the enrolment campaigns produced two peaks (1/2014, 8/2017) of screening positive for tobacco use during the 5 years of follow-up (panel 1). Less than a year after incentives were offered to those screening positive, we observed two peaks of smoking cessation attempts (figure 2, panels 2 and 3).

Rate of tobacco screening, incentivised health plan invites, and smoking cessation attempts among LLUH employees (2014–2019). LLUH, Loma Linda University Health.
Plan of analysis for the cohort profile
Participation, point prevalence abstinence and time to cessation
We will conduct further quantitative and qualitative analyses to measure the effect of successive enrolment campaigns on enhancing (1) participation rate, (2) point prevalence abstinence, (3) cessation attempts and (4) time to cessation in a survival analysis. These outcomes can be related to demographic, behavioural, health plan services used, nicotine screening methods (self-report, bio-specimen testing, retesting appeals) and costs incurred. We are beginning to publish exploratory qualitative analyses of WHP and LLUH BREATHE cohort member programme experiences to identify programmatic areas for improvement.14
Modelling dynamic relapse in LLUH BREATHE
Traditional statistical models often cannot fully capture the dynamic relapse process in a nicotine cessation process, where smokers often transition from one stage (current nicotine users) to another (early abstinence) and experience multiple quit attempts prior to quitting. Some smokers who are able to quit may even move onto a stage of long-term cessation (long-term abstinence), while many smokers often relapse back into their initial stage (current nicotine users). Dynamic modelling of nicotine cessation requires novel methods such as Markov models to capture the transient nature of the relapse stages.15 Figure 3 and equation 1 show a potential three-stage Markov model, where cessation moves the participants through stages left to right with probabilities, λ or θ, and relapsing moves the participants from right to left with probabilities, γ or δ. In Markov models, transition probabilities (ie, λ, θ, δ,γ; probability matrix of transitioning to next or previous stage; figure 4) are usually prespecified based on a priori data but can also be estimated. The Markov model can be expanded to include more stages to depict the natural behavioural process in nicotine cessation.

A three-stage Markov model of the smoking cessation relapse process with Latin symbols indicating the transition probabilities. Cessation moves the participants through stages left to right with lapses from long-term abstinence to early abstinence with probability, γ, and lapses from early abstinence to current nicotine users with probability, δ.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Transition probability matrix of current stages of nicotine cessation. Current nicotine users who continue to use can remain in the ‘Current Nicotine Users’ stage with a probability of 1−λ or go into the next stage, ‘Early Abstinence’, with probability of λ. Participants in the ‘Early Abstinence’ stage may relapse with a probability of δ, stay in the current ‘Early Abstinence’ stage with a probability of 1-δ-θ, or move to the next phase.
Discussion
Our profile of the LLUH BREATHE cohort reveals that our model of continuously incentivising employee smoking cessation produced a 74% participation rate in an employer-sponsored quit attempt less than a year after being offered the incentive. This participation rate among employee smokers is much higher than the norms (median of 28%) for employee participation in more than 20 studies of employee smoking cessation in affluent nations.7 16
One potential reason why the overall participation rate of employee smokers in LLUH BREATHE is higher than national norms is that the cash/reward model is of particularly high cash value.1 Specifically, the LLUH BREATHE model1 of decreasing out of pocket health plan costs by 50%–53% provides a financial incentive (US$600 to US$1200 in lower health plan costs per year) that far exceeds other incentivised cash/reward employee smoking cessation models (up to US$800 is annual cash/rewards) that have been reported in the peer-reviewed scientific literature.7–9 For the LLUH BREATHE cohort, further study is needed to measure the relationship between the cash value of the incentive on long-term abstinence. We note that incentives can be a component of long-term smoking cessation but are not a ‘stand-alone’ cessation method for employees or in other contexts.
Another potential reason for the higher participation rate is that the incentivised model under LLUH BREATHE is not a surcharge model that is punitive to smokers. This is because, under the LLUH BREATHE Plan, the ‘opt-in’ discount on premiums and copays is maintained even in the case of relapse and only stipulates that the relapsed smoker participates in an annual smoking cessation attempt through LLUH BREATHE. Analyses of the Affordable Care Act model of adding a surcharge to the premiums of all smokers do not indicate efficacy in promoting smoking cessation.17
What questions are we going to ask (moving forward)?
LLUH BREATHE is a dynamic cohort that derives from a parent cohort of over 16 000 benefit-eligible employees. A number of recent developments in tobacco use and cessation in the US impact outcomes in this ongoing follow-up study and need measurement. First, the rapid proliferation of electronic nicotine delivery systems (ie, e-cigarettes, e-pipes, and vaping pens) and heated tobacco devices needs more complete measurement in the employee smoking cessation programme. Sensitivity analysis that considers electronic nicotine delivery systems, heated tobacco use and poly-tobacco use in the cohort outcome variables is needed. The emergence of COVID-19 pandemic conditions among employees impacts smoking behaviours.18 The relationship between smoking cessation and pertinent outcomes such as SARS-CoV-2 antibodies, infection and progression needs examination as population health measures become available.
Conclusions
The LLUH BREATHE cohort profiled in this report is an open, dynamic cohort of current and former smokers who are continuously incentivised to maintain or attempt tobacco cessation through an ‘opt-in wellness discount’ on the out of pocket cost of their health plan. The initial findings from LLUH BREATHE indicated (1) high rates of participation and 4-month abstinence rates1 and (2) preliminary findings of acceptability of the incentivised health plan model to members and providers.14 Our profile of the cohort after more than 5 years of follow-up identifies a rich data set for inquiry into workplace and health plan-based incentives for achieving long -term abstinence from tobacco among employed adults.
Collaboration statement
The authors encourage collaborative work with other investigators and will make the de-identified data on abstinence and relapse available in response to reasonable requests from collaborators performing pooling projects and meta-analyses.
Data availability statement
Data are available upon reasonable request. De-identified data are available upon reasonable requests for pooling projects and meta-analyses.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Loma Linda University Institutional Review Board (IRB number 5170126). Secondary analysis of de-identified data.
References
Footnotes
Contributors PNS wrote the final version of the paper, analysed the data, obtained the funding, and is responsible for the overall content as guarantor; OM conceived the study, edited the paper; WS analysed the data and wrote sections of the paper; MH edited the paper.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.