Article Text

Abstract
Background Patients with multiple, persistent symptoms and health anxiety often report poor health outcomes. Patients who are difficult to reassure are challenging for family physicians. The therapeutic alliance between a physician and a patient can influence the prognosis of these patients. Optimising the quality of the physician–patient alliance may depend on a better understanding of the interpersonal processes that influence this relationship.
Objective The purpose of this study is to understand the experiences of patients who experience multiple persistent symptoms or high health anxiety and their physicians when they interact.
Design, participants and setting A qualitative study was conducted using grounded theory of 18 patients, purposively sampled to select patients who reported high physical symptom severity, high health anxiety or both, and 7 family physicians in the same clinic. This study was conducted at a family medicine clinic in a teaching hospital.
Results A model of interpersonal tension and collaboration for patients and physicians in primary care was developed. Helpful attitudes and actions as well as troublesome topics influence crucial dilemmas between patients and physicians. These dilemmas include if patients feel heard and validated and the alignment of goals and mutual respect of expertise and experience between patients and physicians. These experiences contribute to a constructive collaboration and in turn positive outcomes.
Conclusions This model of patient–physician interaction may facilitate providers to turn their attention away from the contentious topics and towards actions and attitudes that promote beneficial outcomes.
- family medicine
- health anxiety
- symptoms
Data availability statement
No data are available Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
It was a strength that semi-structured interviews allowed in-depth exploration of experiences.Finally, physicians were c
It is a strength that both clinician and patient perspectives were elicited.
It is a strength that the analysis supported development of model that may inform clinical care.
Not interviewing patients and physicians in matched pairs was a limitation.
Conducting the study in one clinic in a teaching hospital was a limitation.
Introduction
Primary care office visits by adults are, most often, for chronic conditions or new problems, which typically involve symptoms.1 Persistent symptoms are associated with poorer outcomes as the number of symptoms increases2 and when they are accompanied by health anxiety,3 which refers to preoccupation about disease and difficulty being reassured.4 There is a substantial literature about the challenges of managing medically unexplained physical symptoms in primary care,5–7 but the emphasis on whether or not symptoms are adequately explained may be unnecessary, since multiple symptoms of any type (whether or not they are considered to be adequately explained) and high health anxiety are associated with more medical consultations, poorer physical functioning, higher psychiatric morbidity and higher rates of outpatient visits and hospitalisation.8 9 Furthermore, specifying symptoms as physical or psychological is also complicated because many symptoms, such as pain, fatigue and insomnia, have both physical and psychological aspects. Thus, we focus on multiplicity of persistent symptoms and health anxiety, rather than on unexplained physical symptoms, but will also refer to prior studies of medically unexplained symptoms, which are studying a related phenomenon.
Although health anxiety and multiplicity of symptoms are related to one another, they are independently associated with poor outcomes.10 Since each of these presentations is associated with outcomes that indicate high utilisation and high burden, and because they often but not always co-occur, it is useful to consider them together as a challenging phenomenon in primary care. Correlates and antecedents of multiple and severe symptoms and health anxiety include being female, having experienced childhood adversity, anxiety disorders, depression, personal or family chronic illnesses, lower socioeconomic status and other social stressors.3 11–14
When symptoms are not readily diagnosed, treated and relieved, interactions been patients and physicians may become difficult.15 They may disagree about the cause of symptoms and particularly about the relative contribution of physiological and psychological factors. Clinicians may refer to persistent, difficult to manage symptoms as resulting from somatisation, which implies psychological pathology,8 and can result in the patient feeling invalidated or stigmatised. Kirmayer and colleagues7 suggest that these symptoms are ‘a social and clinical predicament, not a specific disorder’ because they represent ‘a situation in which the meaning of distress is contested.
Importantly, the therapeutic alliance between a physician and a patient can influence the treatment and prognosis of patients in this situation.6 A positive alliance can be challenging to achieve; patients report dissatisfaction with their care16–18 and physicians often describe patients with unexplained symptoms as difficult and dissatisfying.17 19 There is often a discrepancy between what patients expect and what they receive from their family physician.20 In one study, patients described their physician’s explanations of the symptoms as rejecting the reality of their symptoms.21 Patients also describe being caught in a power struggle with physicians and health systems.22 From the physicians’ perspective, they feel that they lack psychological training or skills to deal with these challenges.23 They experience frustration, a sense of inadequacy and powerlessness, and these responses influence clinical decision-making and the physician–patient relationship.24 25
Although several of the factors that contribute to the phenomena of persistent symptoms and high health anxiety being frustrating for both patients and physicians are understood, the solution to these challenges is much less clear. Specifically, paths to optimising the quality of physician–patient alliance may depend on a better understanding of the interpersonal processes that influence this relationship from the perspective of both patients and physicians. The purpose of this study is to understand the experiences of patients with high physical symptom burden or health anxiety and their family physicians when they interact with each other in a primary care setting. Our eventual goal is that understanding the overt and nuanced features of this relationship will support future efforts to improve this alliance.
Methods
We conducted a qualitative study using grounded theory to explore how interpersonal relationships between patients and family physicians influence the experience of care in the setting of multiple persistent symptoms and health anxiety. The research was conducted at the Granovsky Gluskin Family Medical Centre at Mount Sinai Hospital in Toronto, Canada, a single clinic which has about 45 000 patient visits annually. The family health team, which includes 12 staff physicians as well as residents, provides a full range of primary care services including general, preventive and acute care for all ages. Our research team provided diverse perspectives on the meaning of the data. The team included a family physician, who is also a clinical teacher and a developer of curriculum (EB); a child psychiatrist with extensive experience with medically unexplained symptoms (RG); an adult psychiatrist of patients with high symptom burden and health anxiety, who also researches the impact of interpersonal relationships on healthcare (RM); and research scientists specialising in the impact of interpersonal relationships on health behaviour (TL) and in how health professionals develop and maintain expertise (MM).
Participants and sampling
Participants were purposefully selected to explore how patient–physician interactions influence the experience of care for patients with multiple burdensome symptoms (without regard to whether or not these symptoms are explained by organic pathology) or health anxiety. Purposeful sampling deliberately selects participants who provide specific, information-rich perspectives on a phenomenon.26 The optimal diversity of a purposeful sample is a function of the research question. In this case, the research question required the perspectives of primary care patients with multiple persistent symptoms, high health anxiety or both, and of primary care physicians who treat such patients.
We recruited patients who had previously participated in a survey of childhood adversity, attachment insecurity, symptom severity and health anxiety.27 Briefly, 712 patients were approached consecutively in the waiting room after checking in for an appointment. Of 647 meeting inclusion criteria (age ≥18 years and sufficient English skills to complete the survey), 234 declined to participate, 413 consented and 351 returned a completed survey. The majority of the participants were white (66%) and had completed post-secondary education (68%). Multiplicity of burdensome symptoms was measured with the Patient Health Questionnaire–Physical Symptoms instrument (PHQ-15), in which patients score the degree they are bothered by 15 common symptoms (eg, stomach pain, dizziness) for on a three-point scale (0=not bothered at all; 1=bothered a little; 2=bothered a lot) during the past 7 days. A score of >9 was used to indicate multiple burdensome symptoms.28 Health anxiety was measured by the Short Health Anxiety Inventory, which is comprised of 14 questions for which the participant chooses a statement (scored 1 to 4) that best describes their feelings over the past 6 months.29 A score of >17 was used to indicate high health anxiety.30
We identified patients to participate in the current study from the pool of survey patients who had high physical symptom severity only (10% of survey participants), high health anxiety only (13%) or both (21%). Interview participants were not selected for age, gender or other demographic characteristics. Thirty-four patient participants were invited to participate by email. Patients were recruited until thematic saturation was achieved in the concurrent analysis of interviews (N=18, 53% participation rate).
Physician participants were recruited from the 12 staff physicians via self-referral after notification of the study via email and team meetings. Every physician who volunteered (N=7) was interviewed. Physicians were interviewed without respect to whether or not they provided care to the specific patients who were interviewed.
Patient and public involvement
Key informants, including the authors, physicians and nurse primary care providers from a non-teaching community hospital, and a team at that hospital who were developing a curriculum for continuing primary care education, informed the research question. Patients and the public were not involved in the design, recruitment or conduct of the study. A lay summary will be prepared for patient participants of the study and a grand rounds presentation was prepared for physician participants.
Data collection
Eighteen patients and seven physicians participated in individual, semi-structured interviews by one researcher (TLL) from July to December 2019. Interviews were 30 to 45 min long. The interview guide was developed with input from key informants and the consensus of the research group. Questions in the patient interview guide addressed the patient’s experience of bothersome symptoms, their impression of their relationship with their physician, examples of good appointments and challenging ones, health goals and thoughts about how their physician could help them achieve their goals. The physician interview began with a description of a prototypic patient who is difficult to reassure about persistent symptoms and asked them to reflect on interactions with similar patients. They were asked to describe their experiences in these interactions, their concerns, example of good and challenging appointments, their goals for the patient and their impression of the patients’ goals. Both interview guides were iteratively revised over the course of interviews to include themes developed through the analysis. In addition to responses to the interview guide questions, participants were invited to share any experience they thought was relevant. Data collection continued until we achieved theoretical saturation.31 Interviews were anonymized, transcribed and analysed concurrently with data collection.
Analysis
Interview data was coded and categorised using NVivo V.12.5 (QSR International, Burlington, Massachusetts, USA). An iterative, constant comparative approach of grounded theory was used to identify, analyse and report themes within the data32 and to revise the interview guide as new themes were identified and explored. To provide a diversity of perspectives on the meaning of the data and how to label and define emerging themes, a key feature of thematic analysis is for several individuals to read and interpret the transcripts from the interviews. Two team members (TLL, RM) reviewed the anonymised transcripts to organise data into themes. They coded the transcripts separately to identify concepts, key words and reflections, and then compared their results with the other members. After the first four patient interviews, the research team (RM, TLL, MM, EB, RG) met to discuss coding themes. Member checking with key informants was used to revise the interview guide to include themes developed through the analysis. Researchers (TLL, MM, RB) met during the further data collection to discuss and refine the coding framework and themes. The research team met again to review and refine the conceptual framework that evolved through the data analysis.
Results
The patients interviewed included 3 men and 15 women. They ranged in age from 22 to 70 years, with a median of 41 years. Four had high physical symptoms only, four had high health anxiety only and ten had both. The physicians included three men and four women. Their years of practice ranged from 2 to more than 40 years, with a median of 36 years.
Overall, both patient and physician participants found that their interactions could be very frustrating. We identified three main themes about these interactions. First, the participants agreed on certain topics that commonly caused conflict. Second, they described interpersonal processes that were challenging, especially feeling heard or not, feeling validated or invalidated, and agreeing or disagreeing on goals. Managing these challenging interactions seemed important to the outcome. Finally, patients identified attitudes and actions that can be adopted by physicians to promote a positive resolution of tensions. Patients and physicians agreed that positive interactions support good outcomes.
Patients and physicians experienced mutually frustrating interactions
Both patients and physician spoke of how frustrating their interactions could be.
At times I kind of secretly wish that maybe she would find another doctor because I do find our relationship so difficult … (Physician 2)
They identified strong negative emotions and sometimes a lack of trust.
I was really annoyed with (physician) about the MRI. That scared me, and I was so mad at her that I told her that if it turned out that it was a problem, I was going to sue her. I was so mad, because I did not trust her. (Patient 2)
Physicians described their frustration in terms of power struggles and no-win interactions.
I feel pushed into doing more tests than I would normally do which is frustrating but also worries me because you can always find some sort of suspicious finding in the tests… It’s kind of a nightmare. (Physician 1)
Often these frustrating interactions were about certain common topics.
There were clearly identified ‘troublesome topics’ for patients and physicians
A small number of troublesome topics often led to conflict. The first of these was whether or not a patient needs tests or a referral. Several patients expressed a desire for investigations and referrals that was resisted by healthcare professionals.
One thing I'm trying to convince (the physician) to do… I want to get a full body MRI done… I haven’t sold him on that yet. (Patient 3)
Physicians were aware that overinvestigation can be harmful. Some felt that giving in pressure to investigate symptoms amplified tension in the clinical interaction.
Don’t give in to all the tests and stuff they want… the more tests I ordered the more they were coming back and it didn’t ease anything and make anything better. (Physician5)
Others felt that sometimes doing a test that is not strictly indicated was valuable for the purpose of reassurance.
The over-testing and over-referral… like we don’t want to necessarily do that. But I recognize… helping them to live with that anxiety… sometimes may necessitate doing a test. (Physician 4)
Some patients reported that the results of tests did not provide clarity.
I had every test done under the sun… Everything came back negative… Basically, I was left with, ‘we can’t figure out what’s wrong with you.’ (Patient 4)
Another troublesome topic was the possibility of missing a serious disease because of attributing symptoms to anxiety. Both patients and physicians worried about this.
When patients present frequently with… symptoms that don’t really fit a specific diagnosis… that can lead me to wonder if maybe I’ve missed something. (Physician 2)
One physician acknowledged that the concern over missing something serious and the patient’s inability to be reassured were mutually reinforcing.
I find the patients who cannot be reassured very challenging because they tie into my own anxiety about missing things, and I feel that at the end of the visit often neither of us is satisfied. (Physician 1)
Another troublesome topic was the possible role of psychological factors and stress contributing to symptoms. Some patients resist their physician making a connection between current and past life stressors and their current symptoms.
I usually know that there are psychosocial roots for their ongoing health anxiety. I try to explore those areas and often I’m met with resistance. (Physician 1)
Other patients saw clear links.
I think that mine is a chronic trauma from childhood, which for me… manifests bodily. I did have a very sensitive body, and I feel everything highly so I get stomach upset and heart palpitations at the slightest thing… (Patient 1)
Some physicians expressed a belief that a successful outcome depends on patients accepting the psychological roots of their current difficulties.
I do think it’s helping them try to get inside into their own symptoms… the primary goal which might be helping them make that connection between what’s going on in their life and their symptoms. (Physician 2)
Finally, prescription medication was often contentious. One common source of conflict was whether or not a patient would take psychiatric medication.
Well, since I staunchly do not want to take (psychiatric) medication, it’s a little bit difficult for her to talk to me about it, because the area that she could help me with… I don’t want anything to do with. (Patient 8)
Conflict also often arose over whether or not a physician would prescribe medication to reduce symptoms, often pain.
Sometimes I'll go in and there’s a med that I've used before… and I know it helps for a certain thing and they're like, no, we’re not going to give it to you. (Patient 3)
While these troublesome topics provided the content for difficult interactions, it was the interpersonal process in these discussions that appeared to be crucial. In other words, troublesome topics provoked tensions or conflicts that challenged how patients and physician interacted with each other.
Troublesome topics often led to interpersonal challenges in the patient–physician relationship
Certain interpersonal challenges were identified: being heard or not, agreeing on goals, respecting each other’s expertise and feeling validated or not.
Patients consistently endorsed the importance of ‘feeling heard’. When they did not feel heard, little else could be accomplished.
(The physician) was very one-way… And I honestly walked out, because she wasn’t listening to what I was saying. (Patient 10)
When asked what it meant to be heard, patients spoke both of their physician actually listening and also of the shared understanding that resulted.
I feel he heard me… he really listens, understands, and knows you have a medical problem. (Patient 9)
Sometimes the evidence of being heard was that a physician remembers what has been said from one appointment to another.
She’ll basically recap the last time that I saw her, and even saying little things that aren’t necessarily things that she may have written down. (Patient 4)
Disagreeing on short-term goals was often related to the troublesome topics of medication or tests.
(I asked for an MRI) and she said, so, what’s the reason for it? What’s the point that you want to do this?… everything is a fight today. Anyway, I kind of just felt myself slump when she said that. (Patient 12)
One physician described wanting to help a patient shift her goal from cure to optimal function.
She’s like once we get this cured I’m going to be back to normal. And I think… I hope that you do go back to your normal but you know, you’ve been this way for five years and unfortunately you haven’t been able to go back full time yet… You want to be able to provide information that allows them to function as well as they can. (Physician 6)
Patients and physicians discussed appreciating each other’s goals and negotiating. For the patients, this was often explicitly linked to physicians listening.
(A Physician can provide the best possible care by) listening and taking in all the information, and then, I think, suggesting a plan. But then, also, asking what the patient feels the next step should be. (Patient 5)
Both patients and physicians wanted the other to respect their expertise. Patients want to be recognised as the experts of their own experience.
(What I want is) respecting me as a human being, respecting me as somebody who is an equal and knows my problems better than you do… (Patient 13)
Physician do not want to compromise their medical expertise.
I think there is always that tension of wanting to preserve the Physician-patient relationship but not being prepared to do things or behave in ways that compromise your own sense of professional self. (Physician 1)
Finally, physicians were challenged to help a patient feel validated: acknowledging the patient’s perspective, reassuring them that their experiences are understandable, acknowledging progress and keeping the patient ‘in mind’.
I think the fact that she validates my challenges and doesn’t tell me that I’m dreaming them up is extremely important… (but) if I’m over-thinking a situation, she’ll tell me. She’ll say, this is something that you don’t need to be worried about. (Patient 13)
Invalidating experiences often result from dismissing a patient’s concerns or perspective.
I couldn’t walk very far because [I couldn’t control my bowels]… And she said, oh, that’s just ridiculous… So, I was really upset about it. (Patient 2)
A validating experience can be challenging to accomplish when patients are reluctant to speak about their needs or their fears.
I’d be too embarrassed to go make the appointment with the Physician, to say, I’m frightened of this medication or the impact that this mental illness is having on me, and I need reassurance… it would be humiliating. (Patient 7)
Fortunately, since the successful resolution of these interpersonal challenges is important, patients identified things that physicians can do to foster successful listening, validation, agreement on goals and respect of each other’s expertise.
Specific physician attitudes and actions promote successful resolution of interpersonal challenges
Patients identified a number of ways that physicians can influence interactions positively, including listening actively, communicating clearly, spending time, collaborating and providing advocacy.
She definitely heard and she knew why I wanted (a test). I knew why she didn’t want to do it. Yes, I think we both heard each other… She’s very easy to talk to. (Patient 12)
Physicians spoke about the benefits of managing expectations, and of collaborative negotiation.
Half of what we do is trying to understand… the patient’s real concerns… what they expect… and then negotiating something sensible. (Physician 3)
Patients also described positive experiences of negotiating goals.
I was like, I want to completely stop my medication. And he, kind of, said, maybe you shouldn’t do that. It seems like they’re working… But we’ve kind of worked on that, so lowered the dosage… (Patient 16)
Patients also appreciated physicians keeping an open mind, providing expertise, and allowing time.
When I went to see (physician) last, I wanted to ask him about (antidepressants)… He didn’t try to push anything on me… I was grateful that… I didn’t get the sense of an ultimatum, or you have to do this. (Patient 7)
Constructive interactions demonstrated compassion and fostered trust.
She told me she trusts me… I think when they care about you, you care about yourself more too. (Patient 15)
Physicians and patients identified collaboration emerging out of good interactions and trust.
At some point I think we created a bond enough that I felt comfortable enough to say ‘Look. I know you’re feeling these physical symptoms but… there is an underlying issue that’s going on. Like how are you doing outside of here?… And then like the visit after that he just kind of brought up… his issues with his ex-partner…. And he’s like you know what, after that relationship broke down that’s when I started feeling all these things. (Physician 5)
Discussion
Summary
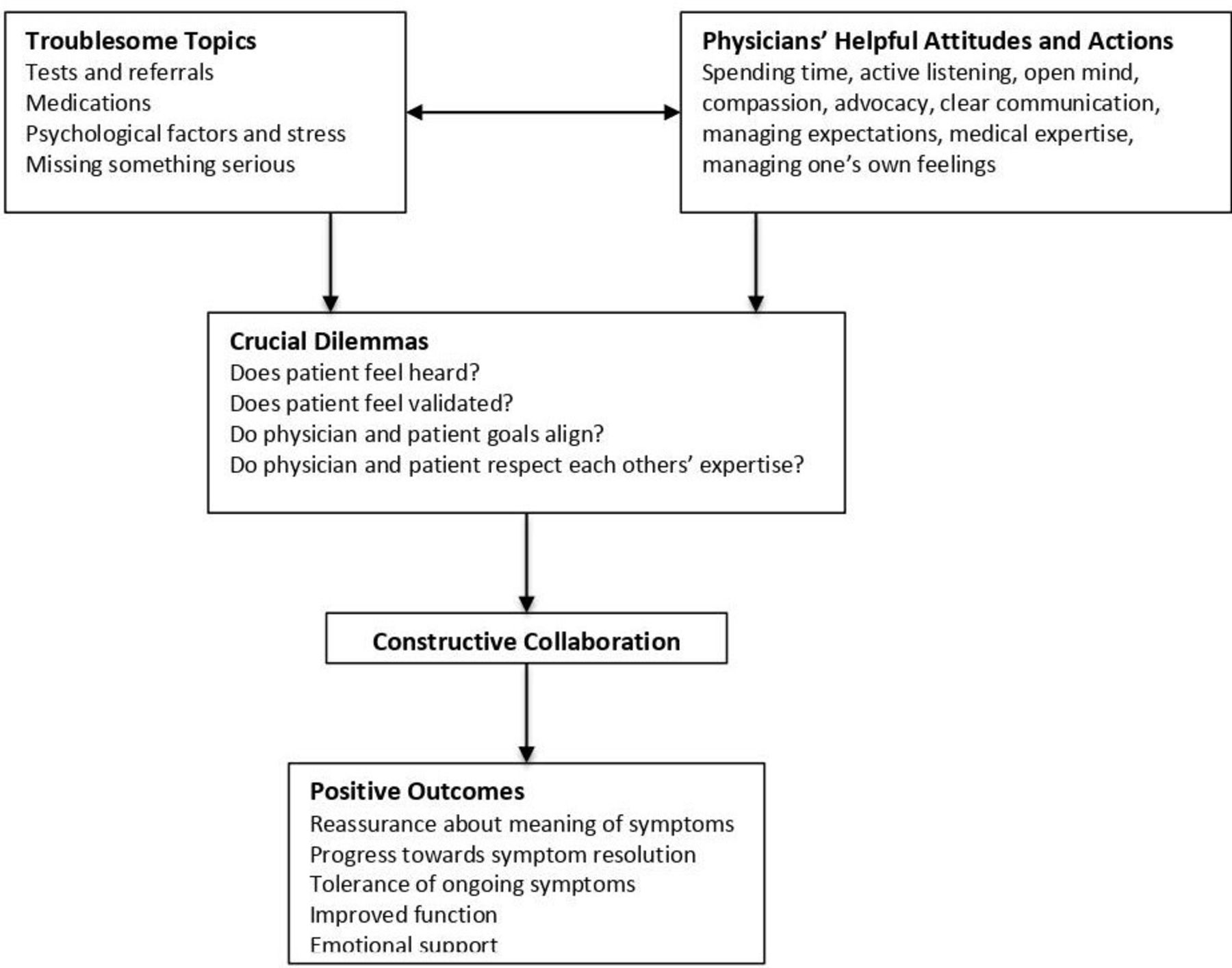
The reports of these patients with high physical symptom burden and/or health anxiety and their family physicians suggest that both may find their interactions quite frustrating, often because of conflicts that arise from troublesome topics and which lead to challenging interpersonal interactions. They navigate interpersonal dilemmas in which patients experience themselves as well heard and validated or not, and physicians and patients find their goals align and their individual expertise is respected or not. Successful resolution of these dilemmas may represent progress from conflict over contentious topics to attention to the quality of interpersonal interactions and is facilitated by physician attitudes and actions, including spending time, active listening, keeping an open mind, showing compassion, providing advocacy, communicating clearly and managing expectations, in addition to providing medical expertise. Success in dealing with these dilemmas is marked by collaborative interactions in which conflicts are negotiated and differences of opinion are tolerated. We have mapped this sequence in a model (figure 1).

{kind=link}
A model of interpersonal tension and collaboration for patients with high physical symptom burden or health anxiety in primary care. Physicians’ helpful attitudes and actions can facilitate discussion of troublesome topics and both identify and resolve crucial dilemmas. Resolution of these dilemmas leads to collaborative interactions between patients and physicians and, in turn, to positive outcomes for patients.
Comparison with existing literature
Our results converge with previous research showing that contentious topics include disagreement over the necessity of medications, patients with unrealistic expectations of care or vague complaints, or patients who do not follow advice, provide expected respect or are time-consuming.15 33 These difficulties are associated with physician burnout, stress and intent to leave one’s practice.33 On the patient’s side of the interaction, tensions have previously been attributed to a professional having limited time, medications prescribed without discussion, poor continuity of care and a focus on disease instead of the whole person.34 Our study advances this understanding by suggesting that while these topics lead to conflict, they need not doom the interaction to a mutually frustrating stalemate. Attention to interpersonal process rather than just the content of disagreement is helpful. Furthermore, attitudes and actions that are familiar to primary care physicians and core aspects of training in communication skills35 foster collaboration and constructive interpersonal relationships in these challenging interactions.
The literature reviewed above suggests that each participant attributes the cause of difficulty to the other. One possible benefit of the model developed here is that it directs attention away from individual contributions to frustrating interactions and towards interactive or relational aspects of these challenges. This observation aligns with patient-centred primary care that involves attention to the quality of the physician–patient relationship, including attention to communication skills, empathy and compassion.36 37 The model is also consistent with approaches to care that emphasise the value of validating patients’ perspectives in patient-centred37 and trauma-informed care.38 Validation of patient experiences and reports is also a key aspect of several psychotherapies that improve interpersonal functioning, especially dialectic behavioural therapy.39 Indeed, the formative benefits of parent–child interactions that are validating and the harms of early experiences that are invalidating may be a relevant antecedent, given the association between early life adversity and both unexplained symptoms and difficult medical encounters.11 13 14 40 These associations suggest that invalidating clinical encounters for patients with high physical symptom burden and health anxiety may represent an ‘echo’ of earlier developmental difficulties and present a risk of re-injury for patients with such past experiences.
Strengths and limitations
The grounded theory method used in this study is able to describe the experiences of patients and physicians, including areas of conflict and contradiction (eg, divergent views about the value of negative tests for reassurance), as they occur within the setting in which the study was conducted. Purposive sampling of patients with high physical health burden and health anxiety may increase the salience of participants’ observations to others with similar concerns. In studies using grounded theory, transferability of the knowledge generated to other settings requires an appeal to sources of validation that are beyond the evidence provided in the study itself, such as the consistency of the model the study generated with other theoretical models. A strength of the model developed in this study is that it reflects other frameworks that prioritise patient experience and attend to the quality of therapeutic relationships.
Limitations of this study include interviewing physicians and patients who were not matched as provider–patient pairs, which could provide a more nuanced understanding of diverse perspectives on the same interactions. Our operational definition of multiple symptoms and/or high health anxiety is novel and evidence-based and could be considered as strength. However, it limits comparability of the current study with prior studies of medically unexplained symptoms. Setting the study in a single clinic at teaching hospital and drawing participants from a sample with little racial diversity and a bias towards high education may limit the transferability of knowledge generated to other types of primary care settings. While the model that this study generated could guide future efforts in training and clinical practice, this study has not tested its utility.
Implications for research and/or practice
The model suggests that focusing on the content of conflictual topics leads to clinical deadlock, while prioritising interpersonal process may provide opportunities for positive change. In the primary care setting, attention to interpersonal process requires a mix of patient-centred communication skills, especially asking about patients’ concerns, priorities and values and listening actively to their responses, responding to patients’ emotions, with genuine personal engagement and emotional involvement and engaging in shared decision making. These skills are well established in primary care41 and so the model may promote a reminder to apply familiar skills at a time of interpersonal challenge rather than a new intervention. Continuing education to refresh these skills using methods such as observed interviews or interactions with standardised patients42 could be useful. That both patients and physicians find these interactions frustrating indicates that testing if such educational approaches could improve care is warranted.
In summary, our data suggest that physicians’ attitudes and actions, such as those that promote feelings of validation, may help overcome troublesome topics and lead to positive interactions and constructive collaboration between patients and physicians. One potential value of this model is that it may encourage clinicians to shift their focus away from those troublesome topics (content) and towards building trusting relationships with their patients (process). This study provides experiential observations of patients and physicians in family medicine that support that value of interpersonal skills and strategies in managing very common and challenging presentations of burdensome symptoms and high health anxiety.
Data availability statement
No data are available Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Mount Sinai Hospital Research Ethics Board, #18-0329-E. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
TLL is a Fellow of the Medical Psychiatry Alliance, a collaborative health partnership of the University of Toronto, Centre for Addiction and Mental Health, Hospital for Sick Children, Trillium Health Partners, Ontario Ministry of Health and Long-Term Care, and an anonymous donor. RM’s work is supported in part by the Chair in Health and Behaviour at Sinai Health System, funded by Sinai Health System and the University of Toronto, and by the Medical Psychiatry Alliance. We thank the key informants for their contributions.
References
Footnotes
Twitter @erinbearss
Contributors TLL, RM and MM designed the study. TLL, MM, EB, RG and RM performed the analyses. TLL conducted the literature search and wrote the first draft of the manuscript. All authors contributed to and have approved the final manuscript. RM is the guarantor for this work.
Funding This work was supported by the Medical Psychiatry Alliance (no award number) at the University of Toronto and by the Chair in Health and Behaviour at Sinai Health System, funded by Sinai Health System and the University of Toronto.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.