Article Text

Abstract
Objective To identify critical illness survivors’ perceived barriers and facilitators to resuming performance of meaningful activities when transitioning from hospital to home.
Design Secondary content analysis of semistructured interviews about patients’ experiences of intensive care (primary analysis disseminated on the patient-facing website www.healthtalk.org). Two coders characterised patient-perceived barriers and facilitators to resuming meaningful activities. To facilitate clinical application, we mapped the codes onto the Person-Task-Environment model of performance, a patient-centred rehabilitation model that characterises complex interactions among the person, task and environment when performing activities.
Setting United Kingdom, 2005–2006.
Participants 39 adult critical illness survivors, sampled for variation among demographics and illness experiences.
Results Person-related barriers included negative mood or affect, perceived setbacks; weakness or limited endurance; pain or discomfort; inadequate nutrition or hydration; poor concentration/confusion; disordered sleep/hallucinations/nightmares; mistrust of people or information; and altered appearance. Task-related barriers included miscommunication and managing conflicting priorities. Environment-related barriers included non-supportive health services and policies; challenging social attitudes; incompatible patient–family coping (emotional trauma and physical disability); equipment problems; overstimulation; understimulation; and environmental inaccessibility. Person-related facilitators included motivation or attitude; experiencing progress; and religion or spirituality. Task-related facilitators included communication. Environment-related facilitators included support from family, friends or healthcare providers; supportive health services and policies; equipment; community resources; medications; and accessible housing. Barriers decreased and facilitators increased over time. Six barrier–facilitator domains dominated based on frequency and emphasis across all performance goals: mood/motivation, setbacks/progress, fatiguability/strength; mis/communication; lack/community support; lack/health services and policies.
Conclusions Critical illness survivors described a comprehensive inventory of 18 barriers and 11 facilitators that align with the Person-Task-Environment model of performance. Six dominant barrier–facilitator domains seem strong targets for impactful interventions. These results verify previous knowledge and offer novel opportunities for optimising patient-centred care and reducing disability after critical illness.
- quality in health care
- adult intensive & critical care
- qualitative research
- rehabilitation medicine
Data availability statement
Data are available in a public, open access repository. Data may be obtained from a third party and are not publicly available. Examples of the data are included in the article, the supplementary materials, and at the public-facing website www.healthtalk.org. Original data for this paper were obtained via a Data Use Agreement with the University of Oxford, to whom all reasonable requests for access to additional data will be referred.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
We conducted a pragmatic, cost-effective secondary content analysis that: (1) verified previously recognised barriers and facilitators to meaningful activity after critical illness; (2) provided a comprehensive inventory of them; and (3) applied the Person-Task-Environment model of performance, a common conceptual model in rehabilitation interventions, to the postintensive care unit context.
Results suggest novel opportunities for intervention, especially enhancement of system-level (environmental) facilitators.
Two qualitative methodologists including one from the original study collaborated on the analysis to ensure rigour, and four authors with clinical and research expertise in critical illness survivorship collaborated to ensure significance and relevance to current practice.
Although long-lasting functional impairment remains a major problem for critical illness survivors, data were originally collected in 2005–2006.
Introduction
Over half of critical illness survivors experience functional impairments now termed the postintensive care syndrome (PICS).1 Unfortunately, rehabilitation interventions to remediate specific functional impairments in PICS have achieved little success.2–4 Thus, PICS care strategies have begun emphasising compensation and adaption to optimise performance of everyday activities, which is a top priority for patients.5
Because performance of everyday activities is associated with independence, quality of life, mortality, healthcare utilisation and costs,6–10 interventions that enhance performance of everyday activities could substantially improve healthcare quality and outcomes.11 To be effective, interventions must address barriers and facilitators to performance. Although research has extensively characterised many important factors related to ongoing disability (eg, weakness, changes in mood and cognition and unavailability of family support),12 there is no comprehensive inventory of barriers and facilitators to activity performance of daily activities. Such an inventory could yield undercharacterised but modifiable barriers and facilitators related to environmental adaptations or goal activity modifications that could become targets for high-impact interventions. Thus, we used Sandelowski’s method of qualitative description13 to conduct a secondary content analysis of interviews with critical illness survivors, to characterise barriers and facilitators to resuming meaningful activities on the wards and after discharge from a critical illness hospitalisation.
Methods
Description of the parent study
The parent study’s overarching objective was to explore and understand critical illness survivors’ experiences of intensive care and disseminate the findings on a patient-facing website (www.healthtalk.org)14 ,15 (online supplemental material 1). Briefly, in 2005–2006, the parent study team recruited UK residents ≥20 years old who had previously received intensive care unit (ICU) care for any reason. Sampling attempted to capture a broad range of survivor perspectives by maximising variation among demographic characteristics and illness experiences.16
Supplemental material
A senior qualitative researcher (SP) conducted one-time semistructured interviews in participants’ homes; families were sometimes present, and all participants provided informed consent. Interviews had two stages: (1) in-depth narratives about participants’ experiences from critical illness onset17 18; (2) question-and-response using an interview guide informed by prior interviews, literature review and an expert advisory panel (online supplemental material 2). They were audio-recorded or video-recorded per participant choice and professionally transcribed and deidentified. Participants reviewed and corrected transcripts for accuracy (ie, member checking).19 Interviews continued until no new themes emerged related to the primary analysis (ie, thematic saturation).19
Supplemental material
Description of the current study
Despite the data’s age, we reasoned that they remained relevant for the current study because of the parent study’s high quality and the lack of significant changes in typical post-ICU pathways of care since their collection (few survivors attend dedicated post-ICU clinics). Of 40 original interviews, we excluded one with the parent of a deceased child, retaining the 39 that provided insight about barriers and facilitators to achieving performance goals after critical illness.
Coders with backgrounds in critical care medicine and geriatrics (LS) and occupational therapy (JSW) conducted a qualitative content analysis using the method of qualitative description13 20 to identify barriers and facilitators, respectively defined as factors that made it harder and easier to achieve performance goals. To facilitate clinical application, codes reflect related concepts from the International Classification of Function (the WHO’s taxonomy for function, disability and health21), when appropriate. We compared and contrasted codes to clarify underlying concepts22 and reviewed them with other clinicians to ensure clinical relevance (a form of triangulation).19 (The time elapsed since data collection precluded checking with participants.) We independently coded all transcripts, meeting after coding every five to resolve differences by consensus and discuss new patterns.23 To avoid missing important ideas, codes were not mutually exclusive.24 We required all coded statements to include at least one goal captured in the concurrent analysis (online supplemental e-Table 1).5 This study reached thematic saturation by the 14th transcript.19
To augment this data-driven, inductive analysis, we created two a priori subcodes for timing (wards and home) using Crabtree and Miller’s template method.25 They signify a broad shift in tasks and environment across the transition home. Every coded barrier or facilitator received one of these two subcodes, enabling analysis of changes over time. We used Atlas.ti V.8.2 (Berlin, Germany) for qualitative data management.
Examination of the barrier and facilitator codes suggested fit with the Person-Task-Environment model of performance (hereafter PTE model), a theoretical framework for the performance of everyday activities commonly used in occupational therapy.26 27 It posits that performance—doing a purposeful or personally meaningful activity—emerges from complex interactions between person, task and environment (online supplemental e-Figure 1). Characteristics of the person include personality and physical, cognitive and emotional regulation abilities. Task is the activity the person wants to do. Environment is the physical, social and attitudinal context. The PTE model suggests how changing the person, task and environment might impact achievement of performance goals on the hospital wards and at home after surviving critical illness. The research team reasoned that: (1) conceptually, the PTE model made sense because all coded data addressed at least one performance goal5; (2) practically, if the codes fit the PTE model, it would support their validity and clinical application; and (3) prospectively, the PTE model could expose gaps in findings for future study. In this additional analysis, all the barrier and facilitator codes are easily mapped to the PTE model.28 29
We quantised the codes by counting the total number of participants reporting each barrier or facilitator, dividing by 39 to calculate frequencies.30 Because all barriers or facilitators received timing subcodes indicating whether the participant experienced them on the wards or at home, we were able to use Atlas.ti’s co-occurrence function to report changing patterns across the transition from hospital to home both qualitatively and quantitatively. We prepared the manuscript using the SRQR reporting guidelines.31
Patient and public involvement
The Healthtalk expert advisory panel, comprising patient representatives, researchers and ICU clinicians,32 oversaw conduct of the parent study, including recruitment, sampling and interview guide development. Patient participants were recruited through health professionals and national charities. The current study sought additional analysis of patients’ experiences.
Results
Table 1 shows broad ranges of participant age (23–76 years), employment (1 student, 2 unemployed, 12 retired, 24 assorted vocations), ICU admitting diagnosis (all types) and time since hospital discharge (weeks to years).
Participant characteristics
Figure 1 summarises the 18 barriers and 11 facilitators using the PTE model, across the transition from wards to home. Tables 2 and 3 and online supplemental e-Table 2 provide frequencies and exemplars, with the a priori timing subcodes (wards or home) noted in parentheses.
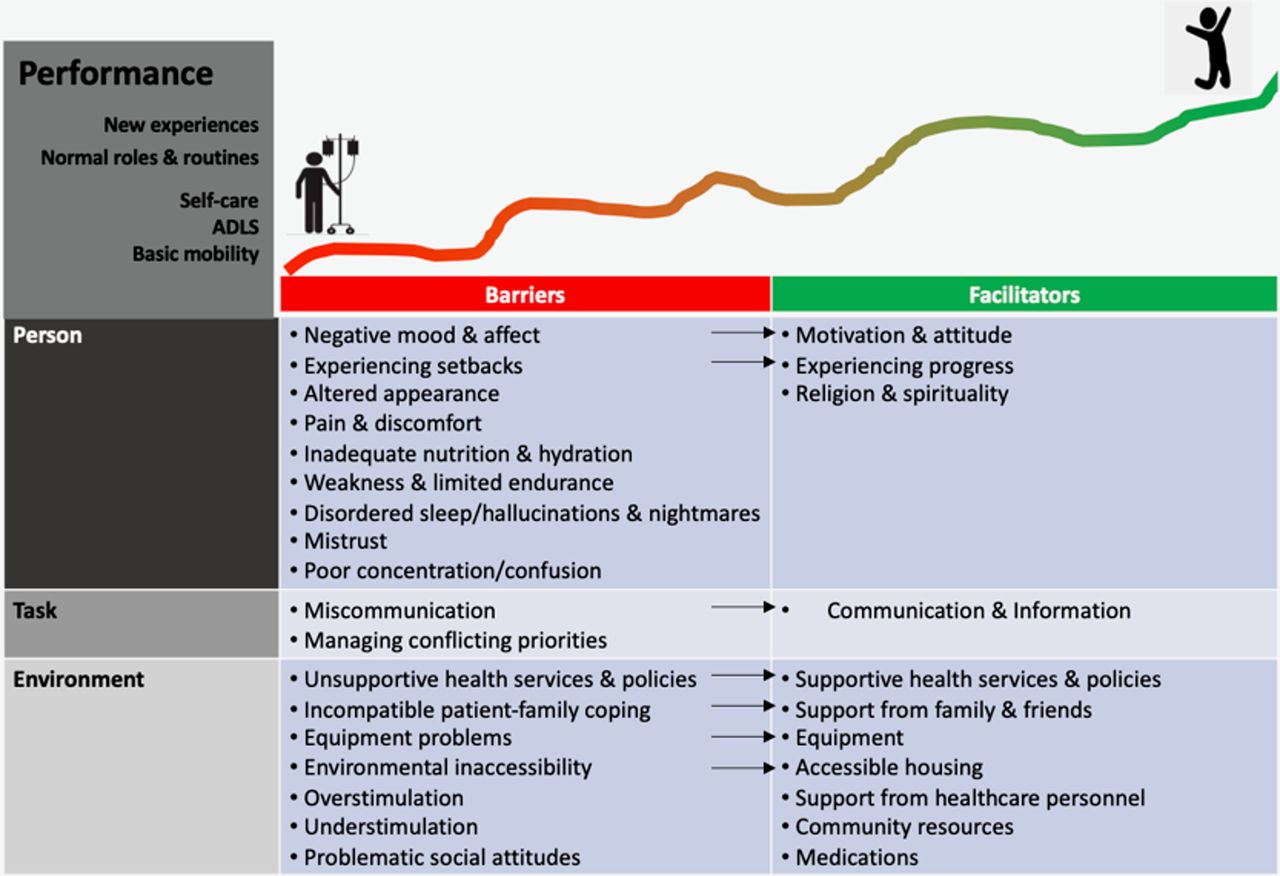
Barriers and facilitators to post-ICU recovery and discharge home using the Person-Task-Environment model of performance. ADLS, activities of daily living; ICU, intensive care unit.
Exemplars of survivors’ perceived barriers to ICU recovery
Exemplars of survivors’ perceived facilitators to ICU recovery
Person-related barriers
Negative mood or affect. Patients described fear, anxiety, panic, apathy, depression and frustration. On the wards, these feelings concerned the illness, care environment and disability. At home, negative feelings concerned inability to manage ‘normal’ tasks or to process the trauma of critical illness. Sometimes, feelings kept patients from attempting activities altogether, although they more commonly blunted patients’ efforts.
Perceived setbacks or stagnation. All patients assessed their recovery trajectory. On the wards, patients described setbacks based on clinical status: prolongation of hospital stay, mobility or self-care disability. At home, setbacks or stagnation related to slow resumption of desired activities. They caused anxiety and frustration.
Weakness or limited endurance. Initially, most discussed feeling unsafe and dependent on hospital staff; later, they expressed impatience at inability to keep up with normal activities. Fatigability was tied to perceived stagnation and thereby frustration.
Pain or discomfort. Symptoms impacted mood, sleep, and mobility. Most discussed delays in symptom recognition and treatment, with providers frequently failing to listen or express empathy about them. Patients attempted stoicism, and many experienced trade-offs between enduring symptoms or medication side effects. Symptoms typically diminished over time.
Inadequate nutrition or hydration. Patients noted weight loss, digestive problems, altered taste and reduced appetite. Initially, they worried about eating enough to heal. At home, some regained their appetites and then struggled with weight management.
Poor concentration or confusion. People described inattentiveness, impulsivity, confusion and slowed thinking. Some attributed these symptoms to medications. On the wards, symptoms contributed to inactivity. At home, patients and families were unprepared for cognitive changes and experienced high stress while developing adaptive strategies (eg, reducing multitasking, making lists and transferring financial responsibility to prevent impulse buying).
Disordered sleep, hallucinations or nightmares. These often occurred in a complex tangle. Although more prominent on the wards, they were still troubling after discharge.
Mistrust. Some mistrusted information, some mistrusted people. On the wards, mistrust occurred with unmet informational or care needs. Once home, mistrust related to poor rapport with clinicians.
Altered appearance. Alterations in physical appearance (eg, swelling, wounds, scarring and weight loss) contributed to patients’ pervasive sense of being unwell, disabled, alien or shy of social situations. This was most pronounced during hospitalisation and tended to dissipate across the transition home as the alteration became less pronounced or the patient adapted.
Task-related barriers
Miscommunication. Miscommunication was multifaceted, comprising inability to obtain desired information, getting wrong or conflicting information, feeling unheard and lacking needed anticipatory guidance. Initially, miscommunication was evident in a patient’s or family’s sense that immediate needs were unmet or clinical information was unclear. Later, it was about not knowing what to expect or how to gauge progress.
Managing conflicting priorities. Conflicting priorities were complex and idiosyncratic, occurring at the intersection between following medical recommendations, wanting to feel normal and supporting family. On the wards, conflict centred around asking staff for help versus trying themselves. At home, it was limiting activity to protect their health versus approximating normal or keeping the status quo versus trying something new.
Environment-related barriers
Non-supportive health services or policies. Problems were heterogeneous. On the wards, they concerned gaps in staffing, limited visitation policies, restrictive mobility policies and poor management of environmental stimuli. At home, they included failure to identify needs before discharge and lack of access to equipment, personal care, rehabilitation, mental health and ICU follow-up care.
Challenging social attitudes. Patients sometimes perceived a disconnect between the hardship of their experiences and the lack of compassion or understanding shown by others. When ward staff dictated that they must do for themselves, they felt infantilised and unsupported. After discharge, they felt self-conscious about disability, misunderstood by friends and family who underrecognised the lasting effects of critical illness or hurried by employers urging return to work without assessing their readiness.
Incompatible patient-family coping. Family visits interfered with rehabilitation or sleep. Some family members distanced themselves to deal with the emotional trauma of critical illness; others struggled to provide physical support; others were overprotective. Most patients and families did not communicate about these issues. On the wards, patients rarely discouraged visitors. At home, most accepted differences in family coping.
Equipment problems. Sometimes equipment discontinuation (eg, oxygen and tracheostomy) was so abrupt that patients felt unsafe. Equipment was uncomfortable, malfunctioned or interfered with activities. Sometimes patients lacked equipment or training to manage it. All these heterogeneous problems occurred on the wards; lack of equipment, inadequate training or equipment malfunction predominated at home.
Overstimulation. Tethers, noise, light, visitors and activity on the wards caused irritation and sleep disruption. After discharge, violent television was irritating, and patients felt overwhelmed in crowded public spaces or even at home with family.
Understimulation. Alongside overstimulation, patients experienced profound boredom and isolation. The physical hospital setting and social barriers to talking with other patients contributed to understimulation on the wards. At home, it was due to inadequate adaptations to support mobility or insufficiently challenging goals.
Environmental inaccessibility. Some hospital rooms made it harder for nurses or visitors to meet patients’ needs. At home, challenges related to navigating stairs and transportation.
Person-related facilitators
Motivation or attitude. Being positive and working hard were critical. Many specifically mentioned deciding that they would get better. After doing so, they strove towards their goals and did not let others hold them back. Motivation increased over time, buoyed by other facilitators.
Experiencing progress. All patients monitored progress. On the wards, it was clinical: liberation from equipment, performance of self-care. At home, it was proximity to ‘normal’. Noting progress boosted morale.
Religion or spirituality. Personal faith or spirituality helped some feel supported or make meaning of their experience, both on the wards and at home.
Task-related facilitators
Communication. Several types of communication helped. Clinicians provided diagnostic information, status updates, teaching and anticipatory guidance by which patients set expectations and gauged progress. ICU diaries and families provided details about what had happened. Clinicians, support groups and families helped patients process their experiences, set goals and work to achieve them.
Environment-related facilitators
Support from family or friends. Initially, family and friends provided food, advocacy, and social and emotional support. After discharge, they assisted with self-care, emotional support and motivation to participate.
Support from healthcare personnel. Support on the wards came from dietitians, physical and occupational therapists, nurses and physicians. At home, it came from home health, ICU follow-up care, general practitioners and mental health providers. Patients appreciated both professional expertise and humanism.
Supportive health services or policies. On the wards, patients noticed safe infection control and staffing policies, and supportive mobility, family engagement and discharge planning policies. After discharge, key policies included access to ICU follow-up, mental health and occupational rehabilitation services, and policies promoting adequate recovery time and phased return to work.
Equipment. On the wards, equipment facilitated healing (eg, catheters) or rehabilitation (eg, walkers). At home, less equipment related directly to healing (eg, stoma bags, dressings) and more supported adaptations (eg, bedside commodes). Patients needed equipment less over time.
Community resources. Participants frequently discussed resources like gyms, group therapy, networks of critical illness survivors and public transportation. On the wards, access aided discharge planning. At home, it facilitated goal attainment.
Medications. Patients discussed how medications treated symptoms or restored physical health across the recovery trajectory.
Accessible housing. Accessible housing—especially a main-floor bathroom—facilitated safe discharge planning and a staged approach to increasing mobility at home.
Patterns and evolution over time
All barriers and facilitators occurred on the wards and at home. Most performance goals had multiple barriers, multiple facilitators or both (figure 2). Barriers were more frequent initially and decreased over time, whereas facilitators were less frequent initially and increased over time (table 2). Six barrier–facilitator domains dominated based on frequency and emphasis across all performance goals: mood/motivation, setbacks/progress, fatiguability/strength; mis/communication; lack/community support; lack/health services and policies.

{kind=link}
{kind=link}
The Person-Task-Environment model of performance at home soon after critical illness discharge. A 44-year-old man who survived pneumonia said, ‘When I came home it was several weeks, a long time before I had a bath. To start with I couldn’t go nowhere. I felt like a prisoner. And then I managed to have a portable gas cylinder that I could take out with me. They said it would be good to get out. And we managed to borrow a wheelchair. And I did, the first time out was frightening, and we didn’t go very far. I felt that everybody was looking at me, which they weren’t, but I did feel everybody was looking at me. And we’d go out in the car, take the wheelchair with us, and I’d be pushed around. I slowly started building up my strength, but I found if I’d done too much then I’d have a day where I was laid out, short of breath’. Although there are performance goals about self-care in this quotation, we illustrate only the barriers and facilitators related to resuming normal roles and routines (specifically, going out).
Discussion
In this qualitative content analysis of semistructured interviews, critical illness survivors reported that critical illness is life changing, and survivors need help leveraging resources across transitions to optimise life after critical illness. Three key contributions of the study are: (1) verification of previously recognised barriers and facilitators to performing desired activities across the post-ICU trajectory; (2) a comprehensive inventory of them; and (3) application of the PTE model to the post-ICU context. Together, these contributions have three important implications for intervention studies. First, they offer an alternative to ‘bottom up’ remediation-focused rehabilitation focused on drill and practice exercises (eg, sit-to-stand, squats, list memorisation and sequence completion). In particular, the PTE model promotes ‘top down’ adaptive rehabilitation strategies focused on the performance of problematic activities (eg, preparing a meal, managing medications) that address specific physical and cognitive deficits while enhancing independent, safe execution of activities via practice.33 It also points to new potential mechanisms of recovery that expand beyond ‘fixing the person’ to focus on matching persons’ abilities to ‘meaningful tasks’ and ‘environment’. Second, areas of overlap in the PTE model suggest novel mechanisms by which barriers and facilitators may moderate one another. For example, perceived progress tends to impact productivity, engagement and well-being.34 It may explain why expectation management and validating progress are key components of ICU recovery programmes.35 36 Third and perhaps most importantly, PICS interventions have largely focused on reducing patient-level barriers,2–4 but this study’s results suggest novel and potentially high-impact strategies to enhance patient-level and system-level facilitators (online supplemental eTable 3 provides hypothetical examples).
At the patient level, we can enhance motivation, mood and agency through interventions like problem-solving therapy37 38; help patients perceive progress using active goal setting and goal attainment exercises39; and offer opportunities for spiritual practice.36 Proactive communication strategies may provide anticipatory guidance related to patients’ goals35; teach patients and families compensatory methods like pacing, energy conservation and activity scheduling40 41; and emphasise listening to address challenges. Our findings suggest that families should be included in all aspects of care, from care planning, to mobility and self-care, to emotional support.42 43 Telehealth may improve family availability.44 45
Intervening at the system level could have the greatest impact because it determines the structures, processes and culture of care. Patient, family and provider perspectives can all inform strategies.12 17 18 35 36 42 44 46 47 The observed differences on the wards and at home suggest that transitions involve shifting barriers and facilitators, so actively planning for and managing them could have an outsized impact on the rate and degree of successful adaptation. Because real-life transitions are rarely smooth,48 teams should promote patient and family engagement49 to ensure patient-and-family centred goals of care and identify needs for training, assistive devices, medication reconciliation and communication with providers. Doing so will require person-centred care policies that permit teams the time, flexibility and resources to match patients’ and families’ needs over prolonged or multiple transition periods. Developing and implementing such policies will necessitate strong partnerships between patients, families and healthcare providers on the one hand, and health systems administrators and policymakers on the other hand in order to optimise the impact on care delivery and outcomes.48
Limitations of this study warrant comment. Despite its novel results, primary data collection did not focus on barriers and facilitators. Patients may be particularly apt to underdescribe task-related barriers and facilitators when not specifically probed. Future studies should address this potential gap. The data’s age may limit generalisability. Indeed, ICU-based interventions have improved critical illness survival rates in the 16 years since these data were collected, and improved visiting policies in some parts of the UK may have enhanced environmental facilitators related to social support during critical illness hospitalizations prior to COVID-19. However, the PTE model should generalise beyond individual barriers and facilitators, providing flexibility to address a broad range of PICS-related performance limitations that remain unsolved problems.2–4 35 44 50 51 All participants resided in the UK; barriers and facilitators may differ across countries and health systems. Nevertheless, our international research team found that mismatches between our expectations and the data revealed patterns we would not otherwise have perceived. Although a strength of the study is that many participants survived long enough to reflect on the evolution of survivorship, their recollections may suffer from recall bias, recency bias and conflation with factors unrelated to post-ICU care. However, the evolution of performance goals over time reported in longitudinal qualitative studies aligns well with our data.52–54 Finally, all participants achieved sufficient function to live at home and give lengthy interviews. The most functionally impaired critical illness survivors—including the dying—likely face particular barriers and facilitators that deserve special attention.
Conclusions
This study identified 29 barriers and facilitators to achieving performance goals that easily integrate with the PTE Model. Their pervasiveness suggests novel opportunities to redesign post-ICU care at both patient-level and system-level to optimise patient-centred care and reduce disability after critical illness.
Data availability statement
Data are available in a public, open access repository. Data may be obtained from a third party and are not publicly available. Examples of the data are included in the article, the supplementary materials, and at the public-facing website www.healthtalk.org. Original data for this paper were obtained via a Data Use Agreement with the University of Oxford, to whom all reasonable requests for access to additional data will be referred.
Ethics statements
Patient consent for publication
Ethics approval
The Eastern Medical Research Ethics Committee (03/5/016), Berkshire Research Ethics Committee (09/H0505 /H0505/66) approved original data collection. The University of Pittsburgh Internal Review Board (PRO17060235) approved this analysis under a data-sharing agreement.
Acknowledgments
The authors would like to thank Drs Neil Resnick and Rama Mallampalli for supporting the data sharing agreement that made this work possible, Dr Kimberly Rak for her guidance during the early phases of analysis, and the Healthtalk expert advisory panel, consisting of patient representatives, researchers and intensive care unit (ICU) clinicians who informed all aspects of primary data collection.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @lpscheun
Contributors SP was a member of the team that conceived and designed the Healthtalk study of ICU survivors and conducted the face-to-face interviews; LS, SP, MH, CR, NL and ERS conceived and designed the current ancillary study; LS and JSW analysed the data, and all authors interpreted the results; LS drafted the manuscript, and all authors revised the manuscript for important intellectual content and approved the final version. LS is the guarantor who accepts full responsibility for the conduct of the study, had access to the data, and controlled the decision to publish.
Funding The original study was supported by the Intensive Care National Audit and Research Centre (ICNARC). LS received funding from the National Institute on Aging, grant number P30 AG024827 and the Agency for Healthcare Research and Quality, grant number K08HS027210. The authors' work was conducted independently of the funding body.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.