Article Text

Abstract
Introduction The COVID-19 pandemic and associated restrictive measures have caused important disruptions in economies and labour markets, changed the way we work and socialise, forced schools to close and healthcare and social services to reorganise. This unprecedented crisis forces individuals to make considerable efforts to adapt and will have psychological and social consequences, mainly on vulnerable individuals, that will remain once the pandemic is contained and will most likely exacerbate existing social and gender health inequalities. This crisis also puts a toll on the capacity of our healthcare and social services structures to provide timely and adequate care. The MAVIPAN (Ma vie et la pandémie/ My Life and the Pandemic) study aims to document how individuals, families, healthcare workers and health organisations are affected by the pandemic and how they adapt.
Methods and analysis MAVIPAN is a 5-year longitudinal prospective cohort study launched in April 2020 across the province of Quebec (Canada). Quantitative data will be collected through online questionnaires (4–6 times/year) according to the evolution of the pandemic. Qualitative data will be collected with individual and group interviews and will seek to deepen our understanding of coping strategies. Analysis will be conducted under a mixed-method umbrella, with both sequential and simultaneous analyses of quantitative and qualitative data.
Ethics and dissemination MAVIPAN aims to support the healthcare and social services system response by providing high-quality, real-time information needed to identify those who are most affected by the pandemic and by guiding public health authorities’ decision making regarding intervention and resource allocation to mitigate these impacts. MAVIPAN was approved by the Ethics Committees of the Primary Care and Population Health Research Sector of CIUSSS de la Capitale-Nationale (Committee of record) and of the additional participating institutions.
Trial registration number NCT04575571.
- COVID-19
- mental health
- public health
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
The use of mixed-methods associated with the longitudinal aspect of the cohort (ie, collecting information related to the same individual at multiple points) will allow for a unique understanding and insights into mechanisms at play, temporal relationships with key crisis events, and the persistent or transient nature of the psychosocial impacts throughout the evolution of the pandemic and its resolution.
The involvement of citizens, community members and other knowledge user will contribute to relevant, high-quality evidence and more coherent and integrated mitigation strategies response from health, mental health and social services workers, researchers, public health authorities, policy-makers and the healthcare system.
The use of a non-probabilistic purposive sampling approach is associated with and may induce biases and limitations leading to under or over representation of certain groups of participants.
The use of online questionnaires may induce a selection bias toward people with access to the Internet and high digital literacy, and makes it harder to reach certain vulnerable groups.
Introduction
The health crisis imposed by COVID-19 is forcing major worldwide reorganisation that will have profound consequences on our society.1 Affected countries have been attempting to contain the spread of the virus by requiring extraordinary isolation efforts from their populations.2 3 One-third of the world’s population (~3 billion individuals) has, is or will again experience some kind of isolation measures, causing an unprecedented and rapidly evolving psychosocial crisis.4–7 While biomedical research is relentlessly pursuing its efforts to understand the impact of the disease on infected individuals and to develop new treatments and vaccines, its psychosocial consequences that could affect our well-being, the state of our health system and our society cannot be ignored.5 8–10
Failure to address psychosocial and health issues will prolong the impact of the pandemic for years to come. The psychosocial consequences of this health crisis will spare no one, particularly vulnerable individuals, and will persist long after restriction measures are lifted and the pandemic is over.5 9 11 12 The combination of professional changes, the state of being ‘at risk’, the possible loss of employment, the resulting economic difficulties, changes in couple and family dynamics, school closures and the reduction of services in health and social services network may all have an impact on the adjustment and development of individuals of all ages.13–17 This impact will be significant for individuals facing unique contexts or challenges (eg, older adults, individuals living with a disability, individuals with a chronic or mental health condition, underprivileged families) and will most likely exacerbate existing social, racial and gender inequalities in health.18–25
The scale of the current COVID-19 mobilisation has destabilised several aspects of our health and social services structures. Services are being suspended, others are being maintained or intensified, and new intervention strategies are rapidly being adopted to adjust to containment measures or risk of virus transmission.26 27 Service interruptions, among others, have an impact on the physical and mental health and subsequent development of already vulnerable individuals.28 Health and social services workers are experiencing major changes in their practice during this crisis.9 29 Many of these workers bear constant witness to the human toll of the pandemic and, all too often, become part of it.9 30 31 This occurs in a context where these workers are subject to the same measures as the rest of the population, thus placing greater demands on their ability to adapt.30 32 33 It is crucial to document practice changes and adjustments of these individuals, who must remain available for their family, colleagues and the population.
Recovering from the pandemic will require a social and economic response that is just as important as the current efforts to minimise the spread of infection.1 34 There is an urgent need for information on the evolution of the psychosocial dimensions of health and coping strategies used by our population and our health and social services structures. By comprehensively documenting such information, stakeholders will be in a better position to make timely informed decisions and implement strategies to minimise the expected consequences of the crisis on our mental health and well-being.
MAVIPAN (Ma vie et la pandémie/My life and the pandemic), a mixed methods based, prospective, observational, longitudinal cohort study, was developed in response to these collective and individual needs. It was born out of an unprecedented collective effort between the four research centres of the Quebec Integrated University Health & Social Services Center and their province-wide academic, governmental, institutional and community partners.
Methods and analysis
Aims
Overall, MAVIPAN aims to accelerate the availability of high-quality, real-time evidence within health and social services structures to address, support and minimise ongoing and future, direct and indirect, psychosocial consequences of the COVID-19 pandemic. Working toward that goal, through constantly evolving research questions responsive to the pandemic evolution and knowledge users’ (KUs) needs, we will document, monitor, and evaluate the following:
Individual and family adjustment and mitigation strategies, especially for those considered vulnerable and in high-risk contexts (eg, What are the psychosocial and professional characteristics of the most vulnerable participants? What are the characteristics of those who seem to be coping well and who may have even improved during confinement? How are families coping over time?)
Healthcare, social services and front-line worker adjustment and mitigation strategies (eg, What is the role of coping and adaptive strategies on the well-being and psychological health of our workers? Are there specific sectors of activity or levels of responsibility that are more vulnerable to adjustment issues? What are the predictive factors of burnout among healthcare workers?).
The organisation of service structures (eg, What are the mental health and social service needs unrelated to COVID-19 that are not covered or poorly covered by current services? How have some services reorganised to provide appropriate levels of care and minimise barriers to care delivery?).
The social and economic response (eg, What are the economic, social and community-based initiatives that have contributed to mental health wellness? What health or social services should be prioritised on another confinement?).
We have established strategic research priorities under key themes to address our objectives. We have identified health inequities and mental health as cross-cutting themes across our objectives. Additional key themes have emerged from sources most likely to increase vulnerability during this health crisis: social environment and health, chronic diseases and disabilities, and front-line, health and social workers. Together, these strategic research priorities will be used as an evolving roadmap to assess the level and extent to which we are addressing our research objectives in a way that meets the needs of KUs and keep up with the state of current knowledge.
Conceptual underpinnings
The proposed approach draws from discussions with KUs and field experts, literature reviews on the psychosocial impacts of disasters, quarantine, and long-term inequalities resulting from crises, and considerations of the strongest study design with the least risk of bias, while considering the complexities of the current and evolving pandemic situation.35–41
MAVIPAN is grounded into the (1) Integrated Knowledge Translation (iKT) approach that actively involves KUs throughout the entire research process and its governance to enhance the relevance and uptake of results,39 and the complementary (2) Strategy for patient oriented research Patient Engagement Framework to foster a climate in which researchers and KUs understand the value of patient involvement.38 The design, measures and analyses are further informed by the (1) Model of Psychosocial Impact of Natural Disasters that specifically addresses coping mechanisms and mitigation strategies during traumatic events,41 and the (2) Dahlgren and Whitehead’s Model of the Social Determinants of Health that identifies the environmental, social, and individual spheres of influence that hinder or enhance the health of individuals and create inequities between populations.40 We will add to this model by considering structural and political determinants of health, which are emerging in the critical race literature.42–44
Patient and public involvement
Citizen-partners, community members and other KUs have been and will remain involved in the design (eg, choice of measures, recruitment strategies) of the study. Through their roles within our Governance structure (eg, members on our Executive Committee), they will remain involve throughout the conduct of the study, and the reporting and dissemination of its findings (eg, reviewing requests for collaboration, submitting research questions, co-authorship). Details about the Governance structure and terms of references are found here: mavipan.ca/about/governance.
Study design
MAVIPAN is a mixed-methods based, prospective, observational, longitudinal cohort where participants will be followed over a 5-year period.45 Data collection started on 29 April 2020. We will collect quantitative and qualitative data at time of recruitment and then according to the four expected phases of the pandemic evolution: the impact phase we are experiencing, the turning point phase when the crisis is brought under control, the recovery phase, and the post crisis following a new “normal”, accounting for additional infection waves and major events (eg, vaccines) (figure 1). The longitudinal aspect of the cohort sets itself apart. The collection of information related to the same individual at multiple points throughout the evolution of the crisis allows for a unique understanding and insights into mechanisms at play, temporal relationships with key crisis events, and the persistent or transient nature of the psychosocial impacts, and can inform when and how to intervene.46 47 The use of mixed methods is well-suited for this proposal and adds to its significance.48 Quantitative data measure indicators, determinants, and impacts (short, mid and long term). Qualitative data build a reflexive approach into the determinants, and will be central to exploring and identifying unexpected impacts and adaptation strategies experienced by participants.

Study design
Participants
MAVIPAN is open to any individual aged 14 and over who understands French or English across the Province of Quebec.49 Within this province, we have been and will continue to reach individuals in urban, suburban and rural areas where different numbers of COVID-19 cases (from no cases to hotspots) are found. We are particularly invested in recruiting vulnerable populations (eg, older adults, individuals living with a disability or a chronic/mental health condition, minorities, child protection families, individuals living in institutional settings) and populations that have become vulnerable because of the COVID-19 context (eg, healthcare and social services workers, adolescents and young adults, caregivers).
Recruitment
We continue to systematically recruit across the province, through our website,50 lead media, social media and networks (eg, Twitter, Facebook), and mass diffusion across healthcare establishments, universities and large networks. We are supported by regional Public Health Directions from healthcare establishments across the province. We have established and continue to seek collaborations with urban and rural cities (eg, City Halls) who promote MAVIPAN through their networks. We developed a recruitment plan tailored to our vulnerable populations, that includes collaborations with (1) key clinical departments and programs (eg, COVID-19 clinics) and communication offices within healthcare establishments across the province to directly reach patients and clients, (2) community-based organisations and (3) provincial thematic networks or associations.
Retention plan
We recognise the challenge of lost to follow-up in prospective cohorts.46 47 51 We have developed a retention plan that includes, but is not limited to: study branding and publicity, incentives (eg, annual gift certificates), personalised email messages, intermittent lay language summary of findings disseminated to participants, and an individualised study page to keep participants informed and engaged.52–54 We will document, when possible, reasons for attrition and work with our experts and KUs to further tailor our retention strategies accordingly.
Quantitative data collection
We collect quantitative data through online questionnaires using the REDCap electronic data acquisition platform that is maintained by Université Laval collaborative platform for large-scale and sustainable data collection named PULSAR.55 Registration, consent and questionnaires can be completed on different digital devices, in French or English. We provide support to participants with limited access to technology or participants having difficulties filling the online questionnaires such as manual-gestural language support, a telephone line and web support where research assistants can help with the registration process or the online completion of the questionnaires.
Participants can register at any point over the course of the study and complete a thorough baseline questionnaire (30–45 min). Additional questionnaires, between 4 and 6 per year, will be tailored to key events in the crisis evolution (eg, second wave) and change in restrictive measures (eg, closing of schools). These include a brief (15 min), standardised follow-up questionnaire which we intend to administer at least twice a year and ad hoc questionnaires (<30 min) aligned with key events (eg, vaccine). A notice and then one reminder is sent to participants when a new questionnaire becomes available. Participants are given a week to complete questionnaires (ie, they can start filling a questionnaire, stop at any time and come back to their saved questionnaire). Questionnaires have been and will continue to be developed and pilot tested with key experts and KUs, using brief (instead of exhaustive) validated measures when available.
Measures
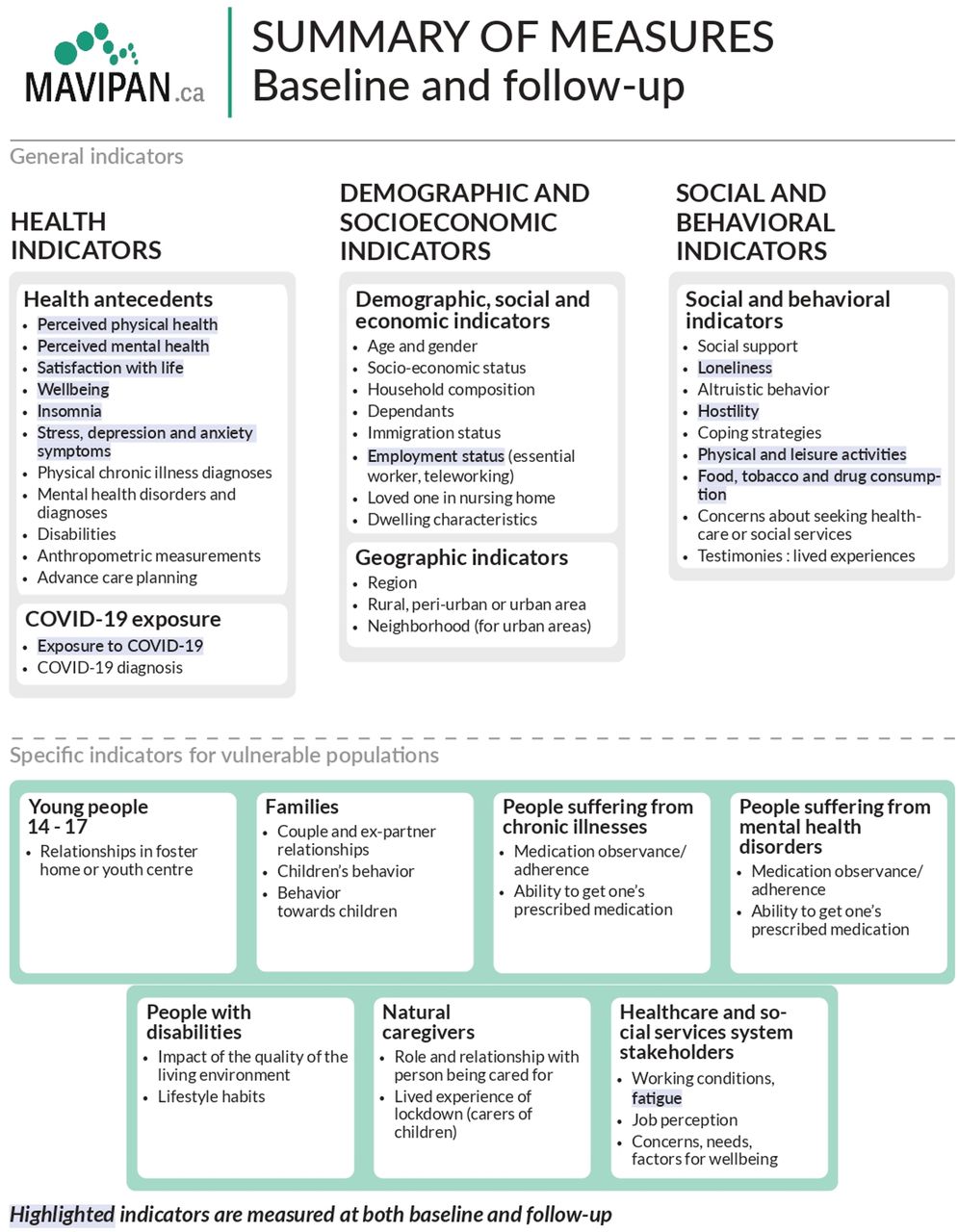
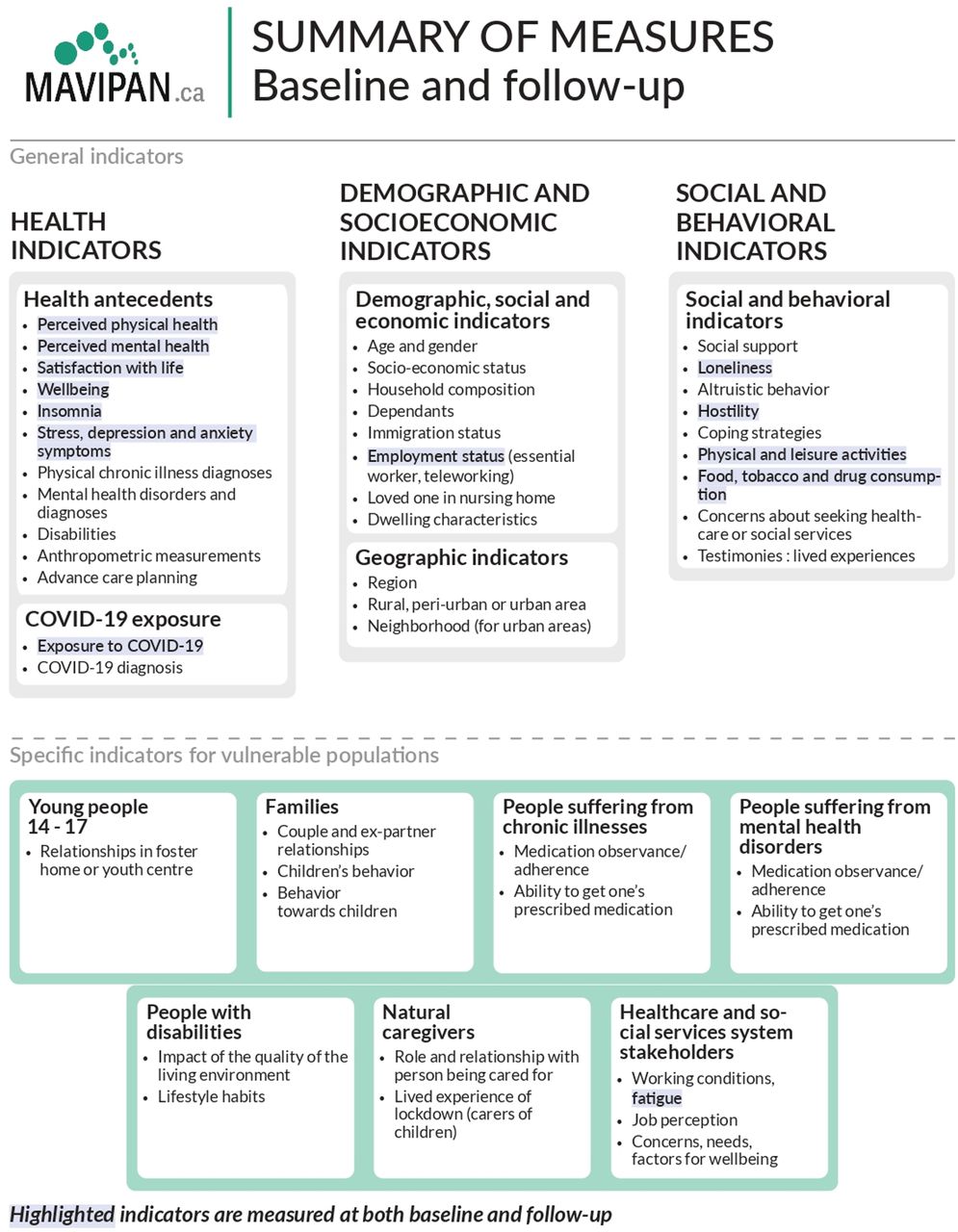
We selected well-validated measures based on our theoretical models, Public Health recommendations, expert consensus, and KUs’ inputs.39 41 56 We document health, social, behavioural and individual determinants and psychosocial impacts of the pandemic for baseline and follow-up questionnaires (figure 2; see online supplemental material 1 for a list of measures).57–73 We further added specific measures and indicators for vulnerable populations, such as disease management, changes in life circumstances attributable to the pandemic or caregiver burden. Participants have the opportunity to fill in open-ended questions addressing current or expected challenges, helpful innovations, hopeful moments and additional topics they would want to see addressed in future questionnaires. These open-ended questions are developed by the research team in close collaboration with the different committees, KU’s and citizen partners.
Supplemental material
{kind=link}
{kind=link}
Summary of measures. MAVIPAN, Ma vie et la pandémie/My Life and the Pandemic.
Linkage
At registration, we ask participants if they agree to be contacted for additional research opportunities. This allows us to add ancillary protocols (eg, interviews with subsets of participants) in response to the pandemic evolution, our findings, and the needs of KUs, thus substantially improving the quality and relevance of the information that is gathered. Furthermore, this allows for opportunities to link MAVIPAN with provincial, national and international COVID-19 related initiatives, thus fostering dynamic, multidisciplinary collaborations leading to increased impact.
Qualitative data collection
Each ancillary qualitative protocol will be unique yet (1) will share common elements of their interview guide (eg, mitigation strategies, impact of the pandemic) and (2) rely on best practices for the conduct of its activities.36 74 Qualitative components of the study will be informed by the quantitative results and the needs that our research team and our collaborators (KU’s and citizen partners) identify throughout the evolution of the pandemic. As such, there is no predetermined number of, or moment for qualitative data collection. We will conduct semistructured interviews and focus groups with specific groups of participants mainly through secured online medium (eg, Zoom, Microsoft Teams) for the time being and will adapt as the restrictive measures are lifted. Length and number of participants will be tailored to each research question. Additional approaches (eg, observations) could be added if relevant.
Data management
We recognise that longitudinal studies require an appropriate data infrastructure that is sufficiently robust to withstand the test of time.46 47 51 MAVIPAN operates using the REDCap system, a secure data entry system, housed within Université Laval’s PULSAR infrastructure. Data management is under the shared responsibility of the research team and PULSAR’s highly qualified personal. This setting ensures the highest of standards (ie, standardised data collection procedure, secured data storage, quality control, daily back-up system) in a sustainable infrastructure that guaranties housing of the data for years to come.
Sample size
We propose a cost-effective, time sensitive, non-probabilistic purposive sampling paired with online sampling and a snowballing technique without size restriction. We expect to recruit 3500 participants by the end of 2021. We recognise bias and limitations associated with this approach (eg, sampling error, self-selection, lack of representation of population).52 We have included key sociodemographic questions that will enable us to compare and weight data to provincial and national standards. We have used similar validated questions as key institutions such as Statistics Canada to further ensure comparability of our findings.
Analysis
We will pursue analysis under a mixed-method umbrella, with both sequential and simultaneous analysis of quantitative and qualitative data, to strengthen the breadth and depth in our capacity to answer our research questions.36 Findings from the quantitative analysis will inform phases of qualitative data collection and hypotheses derived from qualitative analysis will inform subsequent quantitative component. Triangulation will be used to corroborate our findings and help explain paradoxes or inconsistencies emerging within the qualitative or the quantitative analysis.
Statistical analyses will involve both cross-sectional and longitudinal methods and will be of two-folds. First, in a cross-sectional fashion, we provide constant, descriptive information for KUs, enabling them to understand the characteristics of those individuals who are faring well and not so well during the present crisis.75 In doing so, we help KUs identify high-risk individuals and families as a function of different sociodemographic characteristics (eg, sociodemographic, occupational) as they relate to mental health problems, social and health behaviours, identified needs and the use of health and social services (ie, health inequalities). These analyses will help identify populations that may be easily targeted for immediate health services or intervention to improve the state of our service structures.
Then, we will conduct analyses that will help us identify empirically-derived groups in adjustment as a function of time or other variables (ie, identify individual differences in risk with the added benefits of multiple measures of adjustment). We will conduct generalised linear mixed models that will allow us to make associations between events that unfold and characterise the current crisis and individual adjustment across time, informing resilience trajectories, coping and adaptation mechanisms as well as cumulative burden experienced by subgroups of the population.76 In-depth analyses of the factors contributing to the health and well-being (or lack of) of these subgroups will further inform on the mechanism underlying the aggravation of health inequalities.
Lastly, we will develop analytical strategies tailored to each research question. These strategies will likely include a range of methods appropriate for cross-sectional, longitudinal, linked data and causal modelling when relevant, adjusting for missing data where necessary. We will account for sex and gender-based analysis and use an intersectionality approach to explain potential comparisons with emerging key factors (sex, age, and race) in outcomes of COVID-19. Key characteristics of dropouts will be documented and analyses corrected accordingly, if needed. We perform analysis using SAS (V.9.2) or R (V.4.0.1) software package.
Our overall qualitative approach will rely on thematic analysis (although other approaches, such as a narrative approach to qualitative inquiry whereby accounts of experience are explored from the life perspective, could be added if relevant).36 77 Audio or video recorded interviews will be transcribed in verbatim, de-identified, and verified against actual recordings by team members. We will audio or video record focus groups, which will be complemented by moderator and observer notes. We will follow best practices for data management and organisation, coding, and analysis, using the most relevant software (NVivo, QDA Miner or Noldus Observer).36 77
Furthermore, throughout the study, we will conduct cross-comparisons between the ancillary protocols (including a meta-analysis of all qualitative results), which will contribute to a conceptual framework on the health impact and adaptation strategies during a world-wide pandemic.
Governance
Large longitudinal cohort studies are demanding and require sound and sustainable infrastructure and governance. We have set in place an equitable, inclusive and sustainable Governance Plan that fully includes citizens, community members, other KUs, experts and representatives from participating research centres, health establishments, and organisations across the province (https://mavipan.ca/about/governance/).
We have established (1) a Steering Committee (quarterly meetings) that provides strategic leadership, including research question priorities, milestones and national and international collaborations, facilitate research and knowledge translation activities, (2) an Executive Committee (monthly meetings) that reviews requests for collaboration and submission of research questions (ie, alignment with research priorities and feasibility), progress and challenges of ongoing work, approval of publications to be submitted, and scholarship processes for graduate students, and (3) a Lead Research Team (bi-weekly meetings) that will handle the day-to-day operations of MAVIPAN.
Study status
MAVIPAN was developed and launched within 6 weeks of the province’s first confinement in March 2020. It was designed with the aim to be flexible and adapt according to the pandemic evolution and resolution and its associated restrictive measures in the upcoming 5 years. The study is currently opened for enrollment.
Anticipated impacts
The COVID-19 health crisis has caused an unprecedented scientific collaboration. Worldwide, scientists of different countries and backgrounds have come together, rapidly sharing the most recent and relevant information about the pandemic. MAVIPAN takes part in this international scientific collaboration. As the epicentre of the pandemic in Canada, the province of Quebec is now a unique living laboratory to measure, understand and act on the impact of public health measures on population’s health and well-being. Results produced with MAVIPAN add new, unique and relevant information to other governments and populations in Canada, North America and worldwide to adjust the public health response in the next months and years. As other important waves of virus outbreaks are expected to take place, the MAVIPAN experience is central to improve the public health response.
MAVIPAN has the potential to be a critical component of the response to COVID-19 as it can initiate new rapid responses to unmet needs. It can support institutions in the mental health and social services network and inform the evidence base underpinning the deployment and organisation of services in times of crisis and in the recovery period. MAVIPAN’s unique infrastructure will increase the potential for data collection to be harmonised, shared and integrated across COVID-19 related initiatives. It will promote an agile, multidisciplinary and collaborative approach to research and address challenging and important COVID-19 research questions in a concerted and high-impact manner. Findings from MAVIPAN will improve our understanding of the psychosocial impacts, the coping mechanisms and adaptive strategies that have emerged from the restrictive measures of this unprecedented pandemic.
Limitations and strengths
We acknowledge limitations of our study. Our non-probabilistic purposive sampling approach may lead to some bias such as sampling error, self-selection and the lack of or over representation of groups of population. The use of online questionnaire may induce a selection bias toward people with access to the Internet and high digital literacy and limit the reach to more vulnerable populations that are important for this study. We do not have a prepandemic measure with the same sample, which makes it harder to infer a causal role to the pandemic and to contextualise our baseline data with regard to prepandemic levels.
However, the use of mixed methods combined with the longitudinal nature of our study will allow for a unique understanding and insights into mechanisms at play, temporal relationships with key crisis events and the persistent or transient nature of the psychosocial impacts throughout the evolution of the pandemic and its resolution. It will further allow for a reflexive approach into the determinants, and will be central to exploring and identifying unexpected impacts and adaptation strategies experienced by participants. The involvement of citizens, community members and other KUs will contribute to relevant, high quality evidence and more coherent and integrated mitigation strategies response from health, mental health and social services workers, researchers, public health authorities, policy-makers and the healthcare system.
Ethics and dissemination
Ethics and participant consent
This study was approved by the Ethics Committees of the Primary Care and Population Health Research Sector of CIUSSS de la Capitale-Nationale (Committee of record) and of the additional participating institutions. We have worked and continue to work in close collaboration with our Committee of record, who has been instrumental in designing this ‘living’ cohort. We have set templates and procedures in place allowing for an agile process and rapid response (eg, within days) to new questionnaires and ancillary protocols being submitted.
Electronic informed consent, which includes authorisation to be contacted for additional contributions, is provided by each participant and recorded within the PULSAR platform.
Each additional qualitative sub-study first has to be approved by the Ethics Committees of the institutions involved. Then, participants who have agreed to be contacted and who meet the inclusion criteria for that specific sub-study receive an email invitation. Follow-up from that invitation is specific to the characteristics and activities of that sub-study (eg, meet in person or by phone to go over details and informed consent).
We then contact those who manifested their interest in order to give them further explanation as to what participation entails. Before the interview, we send a copy of the information and consent form through email to those who agreed to participate. Official consent is given verbally before the interview.
Transparency of research and data sharing
Transparency of MAVIPAN will be evident in the clarity and completeness of datasets, codebooks and supporting documentation.50 The substantial investments necessary to build these large studies and the unprecedented nature of this health crisis argue for optimal utilisation of MAVIPAN. Data produced as a result of this study will be shared in line with the Canadian Institute of Health Research joint statement on sharing research data and findings relevant to this coronavirus outbreak. Resulting publications will be open access.
Researchers and collaborators will be able to submit research questions and obtain access to data sets. Questions being investigated will be posted on our website to avoid redundancy and promote collaborations within the research community, healthcare institutions, public health agencies, government officials and community organisations.
Knowledge translation plans
We have a well-defined iKT approach where KUs are involved throughout the research process and contribute to just-in-time diffusion and dissemination of research progress and outputs. We are providing, on an as-needed basis, following the crisis evolution, personalised (ie, as a function of region or clientele) updates to KUs. Our KUs and collaborators are helping build community partnerships and assisting us with translation and dissemination of findings. Our bilingual website50 and those of our collaborators will be an important tool for communicating our findings to other populations, stakeholders and research groups in Quebec, Canada and internationally. We will have plain language summaries posted on the website. We will further disseminate findings through news media and social networks. Furthermore, each of the research centres and healthcare institutions involved engages actively in KT towards practitioners and professionals, stakeholders and administrators, service users and other sectors of the population. Each of these platforms will be leveraged to ensure that relevant information is constantly transmitted.
Ethics statements
Patient consent for publication
Acknowledgments
MAVIPAN Research Collaborative would like to acknowledge the following research team members for their time and implication in this research: Léa Langlois, Frédéric Cantin, Josiane Lettre and Geneviève Picher. We would also like to acknowledge the ongoing support and collaboration of the PULSAR team, including Laurence Dionne-Bibaud, Audrey St-Laurent, Marie-Andrée Lévesque and Carole Artault, the Research Ethics Committee of record, the CIUSSS de la Capitale-Nationale, the CISSS Chaudière-Appalaches, CISSS Bas-Saint-Laurent, CISSS Côte-Nord, and all our partners in this initiative. For the complete list, please go to wwwmapivanca. Finally, we would like to give special thanks to all citizens and participants who give us feedback and support.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Collaborators MAVIPAN Research Collaborative: Research Centre on Sustainable Health/ Université Laval: Annie LeBlanc Ph.D., MB Ph.D., PB M.A., J-PD Ph.D., Nancy Côté Ph.D., ÉD Ph.D., MM Ph.D., M-PD B.A., M-PG Ph.D., HW Ph.D., EGGR Ph.D; University Centre for Research on Youth and Families (CRUJeF)/ Université Laval: GT Ph.D., M-HG Ph.D., M-CS-J Ph.D., DN Ph.D., JT M.A., M-CSGD M.Sc; CERVO Brain Research Centre/ Université Laval: MH Ph.D., YDK Ph.D., CC Ph.D, MI Ph.D., CM Ph.D., M-AR M.D., M.Sc., CS Ph.D., MP Ph.D., AV Ph.D., M-FD, M.Sc., PM M.D., Ph.D.; Centre for Interdisciplinary Research in Rehabilitation and Social Integration (CIRRIS)/ Université Laval: FR Ph.D., CM Ph.D., M-CO Ph.D., SB-BM-EL Ph.D, NB Ph.D.; Integrated Research Centre for a Learning System in Healthcare and Social Services (SASSS)/ Université du Québec à Rimouski: LL Ph.D.; Integrated Research Centre for a Learning System in Healthcare and Social Services (SASSS)/ Université Laval: RF M.D. Ph.D., PA, M.D., M.Sc.; McGill University: DC-V Ph.D.; Quebec Health Alliance/ Université Laval: AG M.D., M.Sc.; Integrated Centre for Health and Social Services Chaudière-Appalaches: Édith St-Hilaire M.Ps. Université du Québec à Rimouski: Marie-Hélène Morin, Ph.D.; Université du Québec en Outaouais: AB Ph.D. Centre national d’excellence en santé mentale: MG B.Éd.; Université de Montréal: DL Ph.D.; PP: LV, GP.
Contributors The following authors conceived the study, co-wrote the first draft, and made critical revisions to the manuscript: (AL, MB, PB, GT, FR, CaM, J-PD, MH andYDK). The following authors participated to the design of the study and made critical revisions to the manuscript: (CC, DC-V, NC, ED, RF, M-HG, MI, LL, MM, ChM, M-CO, M-AR, M-CS-J and CS). All authors approved the final version of this manuscript.
Funding Funding comes from discretionary funds from the four Research Centres of the Quebec Integrated University Health and Social Services Centre (CIUSSS de la Capitale-Nationale): VITAM Research Centre on Sustainable Health, University Centre for Research on Youth and Families (CRUJeF), Centre for Interdisciplinary Research in Rehabilitation and Social Integration (CIRRIS), CERVO Brain Research Centre.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.