Article Text

Abstract
Objectives To describe the prevalence and severity of anaemia and to examine its associations with outcome in children with bacterial meningitis (BM).
Design Secondary analysis of descriptive data from five randomised BM treatment trials.
Setting Hospitals in Finland, Latin America and Angola.
Participants Consecutive children from 2 months to 15 years of age admitted with BM and who had haemoglobin (Hb) measured on admission.
Outcome measures Prevalence and degree of anaemia using the WHO criteria, and their associations with recovery with sequelae or death.
Results The median Hb was 11.8 g/dL in Finland (N=341), 9.2 g/dL in Latin America (N=597) and 7.6 g/dL in Angola (N=1085). Of the children, 79% had anaemia, which was severe in 29%, moderate in 58% and mild in 13% of cases. Besides study area, having anaemia was independently associated with age <1 year, treatment delay >3 days, weight-for-age z-score <−3 and other than meningococcal aetiology. Irrespective of the study area, anaemia correlated with the markers of disease severity. In children with severe to moderate anaemia (vs mild or no anaemia), the risk ratio for death was 3.38 and for death or severe sequelae was 3.07.
Conclusion Anaemia, mostly moderate, was common in children with BM, especially in Angola, in underweight children, among those with treatment delay, and in pneumococcal meningitis. Poor outcome was associated with anaemia in all three continents.
Trial registration number The registration numbers of Angolan trials were ISRCTN62824827 and NCT01540838.
- anaemia
- infectious diseases
- paediatric infectious disease & immunisation
- paediatric neurology
Data availability statement
Data are available upon reasonable request. Data are available from the corresponding author upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
We report a secondary analysis of prospective, descriptive data from 2061 children who were consecutive patients of five bacterial meningitis (BM) treatment trials on three continents.
The prevalence of anaemia and its degree on admission were determined according to the WHO criteria and compared with other patient characteristics and indicators of BM severity at each study site and overall.
The risk ratios for recovery with neurological or audiological sequelae (as defined by predetermined criteria) or death in children with moderate to severe anaemia versus mild or no anaemia were calculated at discharge at each study site and overall.
Because the data were collected over 34 years, their present-day external validity and direct comparability between study sites may be limited.
The specific aetiology of anaemia could not be determined.
Introduction
The global burden of anaemia is high, especially in preschool children and in sub-Saharan Africa.1 In 2019, the prevalence of anaemia among 6 to 59-month-old children was 13% in high-income countries, 40% in middle-income countries and 59% in low-income countries.2 Besides iron deficiency, the most common cause of anaemia, other nutritional deficiencies, acute and chronic inflammation, parasitic infections and haemoglobinopathies are frequently found in anaemia,1 3 although the causes are often multifactorial and interrelated.4–6 Chronic and acute malaria parasitaemia and helminth infections contribute to the anaemia burden in tropical areas.1 3–5 In sub-Saharan Africa, severe anaemia is an important contributor to childhood hospital admissions and deaths.4 5 Anaemia is associated with poor immune function and several studies suggest that, in African children, severe anaemia may be a risk factor for invasive bacterial infections.7 Also in high-income countries, anaemia is common in critically ill children and among those admitted to intensive care units.8 In Israel, 21% of children with bacterial infection were anaemic despite their iron parameters being normal.9 In the Fluid Expansion as Supportive Therapy (FEAST) trial in Kenya, Uganda and Tanzania, 76% of children with severe febrile illness had anaemia, which was associated with increased mortality.10
Childhood bacterial meningitis (BM) is a severe invasive infection, which characteristically shows high mortality and frequent neurological and hearing sequelae in survivors. In Liverpool, of 186 children with BM, only 51 (27%) had haemoglobin (Hb) below the reference level and only seven (3.8%) had clinically relevant anaemia.11 In Malawi, however, 48% of children with BM had Hb <10 g/dL.12
Our group has conducted prospective studies of BM on three continents: in Finland (Europe), Latin America and Luanda, the capital of Angola (Africa). In the present study, our aim was to describe anaemia, including its prevalence, severity and possible causes, and to examine its associations with outcome in children with BM.
Methods
Study design, patients and data collection
Our study analyses data collected during five prospective, randomised treatment trials of BM on three continents: Europe, Latin America and Africa.13–17 All the studies were overseen by the same person (HP). The two trials in 12 hospitals in Finland recruited patients from 1984 to 1990.13 14 The Latin American trial was carried out between 1996 and 2003 in Argentina, Brazil, the Dominican Republic, Ecuador, Paraguay and Venezuela.15 The trials in Angola were performed in 2005–2008 (ISRCTN62824827) and 2012–2017 (NCT 01540838).16 17 The details of the studies and the approval of the studies have been published previously.13–17 The studies were performed following the principles of the Declaration of Helsinki. The children were enrolled after their guardian’s informed consent was obtained.
The first study in Finland found chloramphenicol marginally inferior to ampicillin, cefotaxime and ceftriaxone in the treatment of BM, and in the later studies, we used third-generation cephalosporins.13 When in the second Finnish study glycerol appeared to reduce sequelae in BM,14 a larger study in Latin America was realised to examine the potentials of glycerol and dexamethasone.15 In that study, glycerol prevented neurological sequelae,15 and it was given to children in Angolan studies.16 17 The Angolan studies examined continuous antibiotic infusion and oral paracetamol but found no definite benefits with the experimental treatment.16 17 Except for the study treatments, the patients were treated according the hospital policies. In Angola, blood transfusion was given to children with Hb <5 g/dL, or when an especially ill child showed Hb <6 g/dL.
The children were between 2 months and 15 years of age and presented with symptoms and signs suggestive of BM. BM was confirmed if the patient had (1) bacteria in cerebrospinal fluid (CSF), (2) positive blood culture, or (3) two supporting laboratory criteria. The details have been described before.13–17
All data were collected by the study clinicians and nurses using similar forms printed in the relevant language. The information obtained included demographic and clinical details, signs, symptoms, and laboratory test results on admission and during hospital stay, and outcome information defined prior to the studies. All data were then computerised.
The clinical course of the illness was divided into three categories: (1) ordinary: daily improvement, no seizures after day 3 of treatment and no focal neurological signs; (2) complicated: fever (axillary temperature >37.4°C) or irritability over 5 days, seizures after day 3 of treatment or focal seizures, focal neurological signs, another focus of infection or causative microorganism resistant to the administered antibiotic; (3) fatal. Severe neurological sequelae including blindness, quadriplegia/paresis, hydrocephalus requiring a shunt or severe psychomotor retardation. Hearing was tested with traditional audiometry or brain evoked response audiometry, and deafness was defined as a hearing threshold ≥80 dB and any hearing deficit as a threshold >40 dB. The outcomes were registered at discharge.15–17
The Hb was measured on the first (or in a few cases only on second) day of admission, and follow-up sample on day 4 (or 5). The diagnosis of anaemia was based on the first measurement and defined according to the WHO categorisation.3 The cut-off for children <5 years, at age 5–11 years and at age 12–14 years was 11.0 g/dL, 11.5 g/dL and 12.0 g/dL, respectively. For girls and boys ≥15 years of age, the cut-off was 12.0 g/dL and 13.0 g/dL, respectively. In those age groups, anaemia was considered mild with an Hb level of 10.0–10.9 g/dL, 11.0–11.4 g/dL, 11.0–11.9 g/dL, 11.0–11.9 g/dL and 11.0–12.9 g/dL, respectively. In children <5 years of age, anaemia was moderate when Hb was 7.0–9.9 g/dL and severe when Hb was lower than 7.0 g/dL. In older children, the levels were 8.0–10.9 g/dL and lower than 8.0 g/dL, respectively.3
Patient and public involvement
This study is a retrospective, secondary analysis of prospectively collected data. The treating clinicians were aware of the laboratory results and treated the patients according to the hospital policy. The development of the research question was informed by the large burden of meningitis-related mortality among children worldwide. Patients or their guardians were not advisers in this study, nor were they involved in the design, recruitment or conduct of the study. No participant or guardian was asked to advise on interpretation or writing up the results. Results of this study will be made publicly available through open-access publication where study participants, their guardians and health policymakers may access them.
Statistical analysis
All data were computed and analysed using JMP Pro 14.1.0 (SAS Institute, Cary, North Carolina) for Windows. Contingency analysis was used to examine relationships between categorical variables. Pearson’s Χ2 test was used to calculate p values. Associations with continuous characteristics were assessed using Kruskal-Wallis test. Spearman’s ρ correlation coefficient was calculated to measure the association of Hb with other numerical variables. We used logistic regression models to search for independent predictors of anaemia, variables with a p value <0.05 in univariate models were combined to a multivariate model. The results are presented as ORs with 95% CIs.
Results
In all, data from 2123 children were collected from the three continents: 351 from Finland (Europe), 654 from Latin America and 1118 from Angola (Africa). Hb information was not obtained from 10 patients (3%) in Finland, 38 (6%) in Latin America and 14 (1%) in Angola. The final series comprised 2061 children: 341 (16.5%) from Finland, 616 (30%) from Latin America and 1104 (53.5%) from Angola (figure 1).

Flowchart of children with bacterial meningitis (BM) included in the analysis.
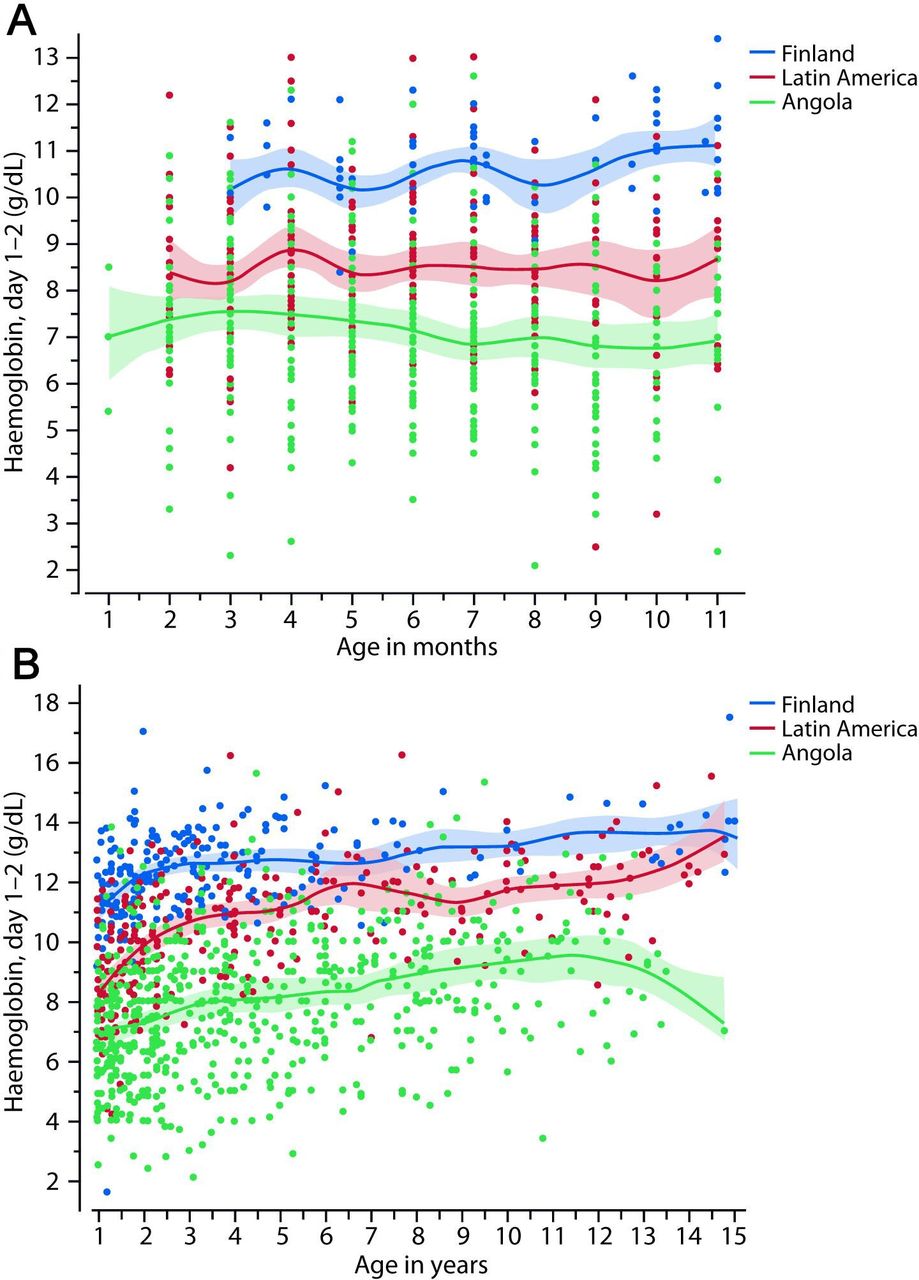
Median Hb (IQR) at admission was 8.5 (7.0–10.6) g/dL: 11.8 (10.8–12.9) g/dL in 341 children in Finland, 9.2 (8.0–10.9) g/dL in 616 children in Latin America and 7.6 (6.3–9.0) g/dL in 1104 children in Angola. Figure 2 shows the Hb levels of children at different ages in Finland, Latin America and Angola (and in all the countries separately in online supplemental figure 1). Overall, Hb correlated significantly (p<0.0001) with the following numerical variables: age of the child (ρ 0.33), duration of preadmission illness (ρ −0.42) and the findings on admission: weight-for-age z-score (ρ 0.31), CSF leucocyte count (ρ 0.21), CSF glucose concentration (ρ 0.12), blood haematocrit (ρ 0.91), erythrocyte sedimentation rate (ρ −0.23), systolic blood pressure (ρ 0.18), heart rate (ρ −0.16), respiratory rate (ρ −0.15), temperature (ρ 0.19) and Glasgow Coma Score (ρ 0.16). The correlation of Hb with blood leucocyte count differed according to the study area: ρ 0.13, p=0.02 in Finland; ρ 0.22, p<0.0001 in Latin America and ρ −0.11, p=0.02 in Angola.
Supplemental material

(A) Haemoglobin of <1 year-old children with bacterial meningitis in Finland, Latin America and Luanda, Angola. (B) Haemoglobin of ≥1 year-old children with bacterial meningitis in Finland, Latin America and Luanda, Angola.
Regarding aetiology of the disease, Hb was 10.4 (8.9–10.2) g/dL in Neisseria meningitidis meningitis, 9.0 (7.3–11.1) g/dL in BM caused by Haemophilus influenzae and 8.0 (6.5–9.5) g/dL in Streptococcus pneumoniae meningitis (online supplemental table 1 and figure 2). In all the areas, the median Hb was highest in meningococcal meningitis compared with other aetiologies being 12.0 g/dL in Finland, 10.9 g/dL in Latin America and 8.5 g/dL in Angola. The delay in seeking treatment was 2.1 (IQR 2–4) days in meningococcal meningitis, 3 (IQR 1.6–6) days in Haemophilus meningitis and 3 (2.1–7) days in pneumococcal meningitis.
In Angola, Hb was lower in 57 HIV-positive than in 671 HIV-negative children (7.0 g/dL vs 7.7 g/dL, p=0.013). In 56 Angolan children with sickle cell disease, the median Hb was 5.7 g/dL, in 141 children with a positive sickle cell screening test the median Hb was 7.2 g/dL, and in 389 children with a negative screening test, the median Hb was 7.9 g/dL. There was no difference in the Hb of children with a positive or negative malaria test or of children who did or did not receive malaria treatment (7.5 vs 7.6 g/dL in both cases). Dehydration, registered in Angola, did not explain the differences in Hb (p=0.44). In Angolan children with (n=168) or without (n=909) oedema, the median Hb (IQR) was 7.0 (5.7–8.0) g/dL vs 7.8 (6.5–9.0) g/dL, p<0.0001. Overall, Hb was significantly (p<0.0001) lower in children with markers of severe disease: Glasgow Coma Score <13, seizures at any time, focal neurological signs, other infectious focus apart from BM and dyspnoea.
Of children, 1603 (79%) had anaemia. The anaemia was classified as severe in 472 children (29%), moderate in 924 children (58%) and mild in 207 children (13%). Anaemia was detected in 95%, 78% and 30% of children in Angola, Latin America and Finland, respectively. Anaemia was mostly moderate to severe in Angola, moderate in Latin America and mild in Finland. Table 1 shows univariate analysis of the factors associated with the different degrees of anaemia.
Characteristics of children admitted with bacterial meningitis and no anaemia or anaemia of different degrees
To identify various cofactors associated with anaemia, we submitted to a multivariate model children’s baseline characteristics that showed significance in univariate analysis. The model identified the study area (Angola or Latin America vs Finland), age <1 year, duration of illness >3 days, weight-for-age z-score <−3 and other than meningococcal aetiology as independent predictors of moderate to severe anaemia (table 2). In Angola, the still breastfeeding ≥1-year-old children had moderate or severe anaemia (vs mild or none) more often than children who did not breastfeed in 93% (136/146) vs 86% of cases, respectively (430/501, p=0.019).
Results for logistic regression models comparing moderate-severe anaemia to mild-no anaemia in children with bacterial meningitis
The Hb level correlated significantly (p<0.0001) with days of abnormal consciousness (ρ −0.20), days with seizures (ρ −0.15) and length of hospital stay (ρ −0.17). Hb was significantly (p<0.0001) lower in children who died, developed severe or any neurological or hearing sequelae or had a combination of those outcomes. Table 1 shows the outcomes of children with no anaemia or anaemia of different degrees. The clinical course of the disease worsened with increasing severity of anaemia (figure 3). Table 3 shows the relative risk ratio (RR) for poor outcome in children with BM and moderate to severe anaemia versus mild or no anaemia in different areas. Severe to moderate anaemia increased the risk of death (RR 1.96, 95% CI 1.17 to 3.27) in Latin America. The small numbers of deaths in Finland and mild or no anaemia in Angola prevented getting reliable results in this analysis. However, severe to moderate anaemia increased the risk of a combined outcome of death or severe neurological sequelae in all study sites, RR being 4.55 (95% CI 1.69 to 12.24) in Finland, 2.21 (95% CI 1.46 to 3.35) in Latin America and 1.37 (95% CI 1.04 to 1.79) in Angola. The RR for death or severe neurological or hearing sequelae was 4.24 (95% 1.59–11.32), 2.05 (95% 1.44–2.91) and 1.26 (95% 1.00–1.59), respectively.

{kind=link}
{kind=link}
{kind=link}
Clinical course of bacterial meningitis in children with or without anaemia.
Relative RRs for poor outcome in children with bacterial meningitis and with severe to moderate anaemia versus mild or no anaemia in Finland, Latin America and Luanda in Angola
Hb on day 4 or 5 correlated significantly (p<0.0001) with Hb on admission (ρ 0.66). It was 11.0 (IQR 10.2–11.9) g/dL in Finland, 9.7 (IQR 8.5–11.1) g/dL in Latin America and 8.0 (IQR 7.0–9.0) g/dL in Angola.
Discussion
Anaemia, mostly of moderate degree, was detected in children with BM frequently. It was most common in Angola, among underweight children, in those with treatment delay, and in those with pneumococcal meningitis. Anaemia increased the risk for poor outcome in all our study sites.
Severe infections and bacterial infections are associated with anaemia.1 7 Anaemia can predispose children to bacterial infections,7 although on the other hand, infections also cause anaemia.1 Evidently, we here have a ‘chicken and egg problem’: does infection trigger anaemia or vice versa? Most likely these sequences take place in both directions. In our study, Hb increased during admission in Latin America and Angola but lowered during admission in Finland where delay in seeking treatment was shorter than in other areas.
Anaemia was more common in children with BM than in children living in the respective geographical areas in general. Projected against the data during the study period,2 18 the difference was 95% vs 63% in children in Angola, 78% vs 29% in Latin America and 30% vs 16% in Finland.2 Ninety-five per cent of Angolan children with BM in this study had anaemia compared with 76% of children with severe febrile illness, mostly malaria, in the FEAST trial.10 The FEAST trial used, however, a lower threshold (Hb <10 g/dL) for anaemia, which suggests that the true difference was less. In the same trial,10 33% of children were severely anaemic (Hb <5 g/dL) versus 39% in our series from Angola with a cut-off of <7–8 g/dL. In Israel, only 21% of children with acute bacterial infection presented with anaemia.9 The children with BM in Angola and Latin America were anaemic more often than those in Liverpool (27%)11 or Malawi (48%).12 In Finnish children with BM, anaemia was rarer.
The strongest factor associated with anaemia was the area where the child lived. It is well known that anaemia is most prevalent in children of low-income and middle-income countries.1 2 In this study, the children had other concurrent conditions that were associated with anaemia. Weight-for-age z-score <3 increased the odds of anaemia 3.84-fold. In general, inadequate nutritional intake increases the risk of anaemia.1 In Uganda, severe acute malnutrition and stunting were associated with anaemia in <5-year-old children.4 19 In our study, continued breast feeding in ≥1-year-old children in Angola was associated with anaemia. Another study from northern Angola showed that continued breast feeding was associated with iron-deficiency anaemia in 6-month to 36-month-old children.20 It is most likely that mothers with limited resources continue to breastfeed when they cannot afford sufficient supplementary foods.
Of our 57 HIV-positive children, only one had normal Hb. In Mozambique, 88% of HIV-infected and HIV-exposed children were anaemic, and of those, 24% were classified as having severe anaemia, in this case, Hb <7 g/dL.5 Various haemoglobinopathies are important causes of anaemia globally and in countries such as Angola.1 20 Sickle cell disease and a positive sickle cell screening test were associated with anaemia in Angola (manuscript in preparation), whereas, and contrary to most studies in Africa,5 10 20 malaria parasitaemia was not associated with anaemia in our present analysis. In Luanda, Angola, malaria is transmitted year-round. Some of the malaria parasitaemia might be chronic carriage not causing acute anaemia. Anaemia was most common in young children, the odds for <1-year-old children being 2.94. Globally, preschool children are particularly affected by anaemia,1 and in Africa, especially children <2 years of age.19 20
The longer the illness had lasted before admission, the lower was the Hb at presentation. The aetiology played a role as Hb was highest in meningococcal meningitis, possibly reflecting the acuteness of the illness onset. Anaemia of inflammation is found in patients with infections.1 7 In Ugandan children, severe anaemia was associated with elevated markers of inflammation, namely, total white blood cell count, C reactive protein (CRP) and ferritin.4 In our study, Hb correlated negatively with erythrocyte sedimentation rate, and CRP on day 4. Opposite to the children in Uganda4 and our study in Angola, the children in Latin America and Finland showed a positive correlation between the blood leucocyte counts.
Low Hb at admission and anaemia correlated with markers of severe disease at admission and during the hospital stay. Moderate to severe anaemia increased the risk of poor outcome such as death, neurological sequelae and hearing sequelae. This was found in all the study sites, except for deaths in Finland, where the deaths and severe anaemia were uncommon. However, also in Finland, moderate anaemia increased the risk of severe neurological sequelae. Combining all our study sites, severe to moderate anaemia increased the risk of death in BM 3.4-fold, the risk of death or severe neurological sequelae 3.6-fold and the risk of death or severe neurological sequelae or deafness 3.1-fold. In Malawi, only 4% of children with severe pneumonia had severe anaemia, although it increased in-hospital deaths (OR 1.41, 95% CI 1.03 to 1.92).21 In the FEAST trial, 13% of children with severe, 7% with moderate and 8% with mild anaemia died within 24 hours.10 The overall case fatality rate in children admitted for severe anaemia in the Democratic Republic of the Congo was 5.6%, being 20% in children with severe anaemia and BM.22 We hypothesise that hypoxaemia plays a major role in these deaths since Hb primarily delivers oxygen to tissues.1 Severe anaemia was associated with low cerebral oxygenation levels measured by infrared spectroscopy in a Ugandan paediatric study.23
Our study is a post hoc analysis and has some weaknesses. We did not register total blood count or measure iron indices. Some of the data were missing but we assumed the missingness to be random in our analyses. Many causes of anaemia, like parasite infections and haemoglobinopathies, other than sickle cell disease, were not screened. The time span for data collection was long. The treatment differed somewhat in different areas and with time. Third-generation cephalosporins became the treatment of choice,13 and after Finnish and Latin American studies,14 15 glycerol was given to all children in Angola. This said, we did, however, report a very large series from three continents and eight countries, and it is unlikely that these factors would have significantly distorted the results.
High health discrepancies exist between our study areas: Finland (high-income country), Latin America (upper middle-income area) and Angola (lower middle-income country). Even if in Finland, the studies were done in the 1980’s, thereafter in Latin America, and latest in Angola, the outcome was worst in Angola and best in Finland. Also, in a study from the 1980’s and 1990’s, the outcome from childhood BM was much worse in Malawi than in the UK, even with the same causative organisms.12
In summary, anaemia was very common in children with BM. It was associated with the markers of disease severity and increased the risk for poor outcome. Our results underline the need to monitor Hb levels in all children. Anaemia and low Hb levels at admission serve as a marker of severe disease and are associated with increased risk of death or sequelae. Further studies on the effect of early interventions for the correction of anaemia are needed.
Data availability statement
Data are available upon reasonable request. Data are available from the corresponding author upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and The Luanda Children’s Hospital’s Ethics Committee approved the studies in Luanda, and the relevant Ethics Committees or Hospital Boards approved the studies in six countries in Latin America and in 12 hospitals in Finland. At the time of the studies, no ID or number of the approval was given. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The authors thank the patients and their families for participating in the study, as well as all the hospital personnel for their dedicated help in the care of these patients.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors TP, IR, MK, KJ and HP conceived the study after TP had joined the data in a single database. TP and KJ did the literature searches. Analyses were performed by TP according to suggestions from IR, MK, KJ and HP. TP wrote the manuscript with important input and commentaries from IR, MK, KJ and HP. TP, IR, MK, KJ and HP approved the final manuscript and its submission. TP is responsible for the overall content as guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.