Article Text

Abstract
Objectives To identify implicit and more profound barriers and facilitators and involving context elements to accomplish sustained physical activity (PA) in patients with a chronic disease. Understanding these barriers and facilitators may help develop future strategies to be used by healthcare professionals in primary care to support patients with a chronic disease to reach sustained PA.
Design and methods The qualitative, narrative research method storytelling was applied. Perspectives of both patients with a chronic disease (n=12) and involved healthcare professionals (n=11) were collected. Stories were audiotaped and retrieved from the transcriptions. Analysis involved a cyclic process of constant comparison. Main themes were arranged in the theoretical framework of the Capability, Opportunity, Motivation and Behaviour (COM-B) model.
Participants Patients were adults with a chronic disease or at high risk of developing a chronic disease who participated in a PA promoting programme. Eligible healthcare professionals were those involved in these PA promoting programmes in primary care, such as physiotherapists, nurse practitioners or sports consultants.
Results From 176 stories, 62 relevant and unique stories were selected for further analysis. Eleven main themes were identified and afterwards linked to the COM-B model. Trust in one’s own capabilities and in the healthcare professional were relevant themes. Also, health literacy and coping with temporary interruption were important capabilities. Important motivators were customised PA, increasing awareness, meaningful activities, exercising in a group and success experiences. Aversion to sports was seen as a barrier. Interprofessional collaboration and prerequisites can be a facilitator or a barrier.
Conclusions This study provides insight into deeper motivations, barriers and facilitators of sustained PA from both the patients’ and healthcare professionals’ perspective. Comparing these perspectives revealed different views and beliefs on some themes. Attention for temporary interruptions, aversion to sports and health literacy were identified to be important for sustained PA.
- primary care
- preventive medicine
- qualitative research
- sports medicine
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
By using storytelling implicit barriers and facilitators important for sustainable physical activity (PA) are explored among patients with a chronic disease.
Perspectives of both patients and healthcare professionals were included and compared, providing relevant clues for the improvement of support for sustainable PA.
Researchers were trained to improve their storytelling skills, which is important to ensure a narrative climate during the interviews, in order to collect real-life stories.
Intersubjectivity was reached among four researchers, increasing the quality of the study.
Patients participating in this study took part (at least once) in a PA-promoting programme, limiting the transferability of results to a population less motivated.
Introduction
The numbers of people living with a chronic disease, such as cardiovascular disease, diabetes and cancer, are substantial and increasing worldwide.1 Living with a chronic disease has considerable consequences for one’s health, quality of life and social involvement and is the cause of 71% of premature death rates worldwide.2 Integrating physical activity (PA) into one’s lifestyle decreases the risk of developing a chronic disease and reduces the severity of clinical characteristics.2–9 Guidelines recommend that everyone engages in moderate-intensity PA for at least 150 min every week, spread over several days and strength enhancing activities at least two times a week. In addition, long periods of sitting are to be avoided.10 11 Even though the positive effects of PA are evident, 30% of the world’s population does not meet PA guidelines. For over 60-year olds, this proportion is even larger; ie, 45%.12 In the Netherlands, more than 50% of people with a chronic disease are not able to meet PA guidelines.13
Sustained PA is primarily the responsibility of people themselves. However, not everyone is able to initiate and maintain sustained PA, due to insufficient health literacy—and in spite of support from primary healthcare professionals.14 Various primary healthcare professionals, such as physiotherapists and nurse-practitioners, support people with chronic diseases to improve their PA. In many cases, the therapy plan includes more PA.15
Not complying to PA guidelines is associated with: low level of health literacy, low level of education, obesity and chronic disease.16–19 Patient-reported barriers for integrating PA into one’s lifestyle are: sedentary habits, lack of social support, competing priorities, limited access to PA and apathy. In addition, physical limitations, lack of self-confidence, financial problems and lack of experiencing success have been described as barriers of PA.20 Reported facilitators for PA are: accessible facilities, tailored training programmes, attention for positive exercise experiences and beliefs, sufficient knowledge and social support.21 22 Additionally, education about the importance of PA and improving environmental and financial access appears to be helpful.20 22 23
Most of the intervention studies on barriers and facilitators for PA show short-term effects only. Sustained effects have rarely been studied nor found.24–26 Moreover, lack of details in the description of promising interventions makes it difficult to replicate treatment.27–29
Therefore, it is important to distinguish between initial behaviour change (short term) and sustained behaviour change (long term), the latter of which is harder to achieve.30 Evidence suggests that a personalised approach, including a person’s context, is needed to reach sustained PA.31 The personal context contains individual characteristics and physical, psychological and social functioning in one’s own living environment.32
To gain insight into the personal context, it is important not only to focus on explicit factors but also to gain knowledge about more implicit factors of importance to sustained PA.32–35 This study aims to identify implicit and explicit barriers and facilitators to sustained PA for people with a chronic disease, including their context, by collecting perspectives of both patients and healthcare professionals. This study, therefore, employs a narrative research method. In addition, the Behaviour Change Wheel (BCW) framework is used to order and grasp a better understanding of the identified barriers and facilitators. The BCW summarises current knowledge about behaviour change techniques. Its centre is the Capability, Opportunity and Motivation (COM-B) model, which can be used as a starting point to understand behaviour (B) in its context.32
Methods
Research design
To gain understanding of barriers and facilitators to sustained PA related to patients with a chronic disease and their context, a narrative research method—storytelling—was applied. Storytelling is an established and emerging research method in health and social science.36 37 Storytelling can be used to obtain more nuanced, contextualised and culturally reflective data than other qualitative research methods do, for example, semistructured interviews. In storytelling, the participant is asked to tell about his/her experience of interest using a sensitising question. Therewith, the participant is completely free to tell about any aspect of the experience of interest. The interviewer’s role is to create a narrative climate and only asks questions to complete the narrative elements of a story (ie, people involved, reactions, emotions). A single interview can contain multiple stories. A narrative question invites the participant to tell about a specific situation linked to an emotion around PA, either positive or negative.36 38 Storytelling focuses on the perspective of the participants, who lived the experiences as an insider and will, therefore, provide important insights and ideas, and a deeper understanding of barriers and facilitators. This presupposes a subjective truth in the social context of the participant and reveals implicit knowledge about the subject of the study.38–41 By using storytelling, health-related information specific to one’s own situation is contextualised.36 42 To ensure rich and informative data, stories of both patients and healthcare professionals about a specific situation linked to experiences and emotions were collected. The Consolidated criteria for Reporting Qualitative research guidelines (COREQ) were followed43 (see online supplemental file 1).
Supplemental material
Participants
Participants were selected by purposive sampling.44 Eligible patients were adults who participated in a PA-promoting programme focusing on supporting people with one (or more) chronic diseases or at high risk of developing a chronic disease, such as cardiovascular disease, diabetes mellites type II or being overweight (BMI >25). Eligible healthcare professionals were those involved in these PA-promoting programmes in primary care, such as physiotherapists, nurse practitioners or sports consultants. We chose to select on these criteria because patients and healthcare professionals who participated in a PA-promoting programme have experienced success and/or failure in reaching sustained PA, so could share their stories about their experiences in trying to reach sustained PA. Eligible patients were contacted by their primary healthcare professional to participate. Patients who had provided consent for participation were contacted by telephone or e-mail by a member of the research group (see below) to make an appointment for an interview.
Research group
The research group consisted of four primary researchers, experienced in conducting qualitative research (JJdB, AF, AH and PS) and eight trained students who assisted with the data collection. None of the members of the research group knew the participants before conducting the interviews. All had been trained in applying the storytelling method by an expert on storytelling, during three half-day sessions. The training included creating an interview guide, practising interview skills and analysing data.
Data collection
The interviews were conducted individually, face-to-face, at a location chosen by the participant (participant’s home, work or public place). An interview guide was used consisting of a short introduction, examples of narrative questions and a list of narrative elements38 (see online supplemental file 2). To account for the difference in perspective, the narrative questions in the interview guide for the patients slightly differed from that for the healthcare professionals. All interviews lasted approximately 1 hour, were audio taped with consent, and the interviewer made brief field notes to aid later reflection. Participants received a gift voucher (worth 25 euros for patients and 75 euros for healthcare professionals).
Supplemental material
Theoretical framework
The COM-B model was used as a framework to organise the themes found in the analysis and to help understand behaviour in its context. The model assumes that human behaviour (B) is part of a system in which three central components affect each other: Capability, Opportunity and Motivation. Capability is a person’s attribute referring to physical and psychological capability, for example, body strength, knowledge or endurance to be able to execute PA. Opportunity is an attribute of a person’s environmental system and can be physical or social. The combination of capability and opportunity makes a behaviour possible or facilitates it. Motivation is an aggregate of mental processes that energise and influence behaviour and may be reflective or automatic.32 45
Data analysis
The analysis consisted of interpreting texts in story form. Data analysis was conducted in three phases (table 1). In phase 1, the audio recordings were transcribed ad verbatim and anonymised to ensure privacy. Stories were retrieved from the transcripts using a consensus-based format (see online supplemental file 3).36 38 40 46 Member checks were done with the participants. In phase 2, the primary researchers continued open and axial analysis in a cyclic process in which constant comparison between results during each step of the analysis was done. In phase 3, main themes were arranged into the COM-B model, which was used as a theoretical framework. Conclusions on how to integrate the findings into healthcare were discussed.
Supplemental material
Analysis process
Patient and public involvement
In this study, participants were both healthcare professionals and patients. Storytelling is part of a larger project in which a method was developed in cocreation with patients and healthcare professionals that is more customised in its support to sustained PA. Before the start of the project, healthcare professionals were interviewed about their lack of competence in supporting people with chronic conditions. The research question was formulated based on their input.
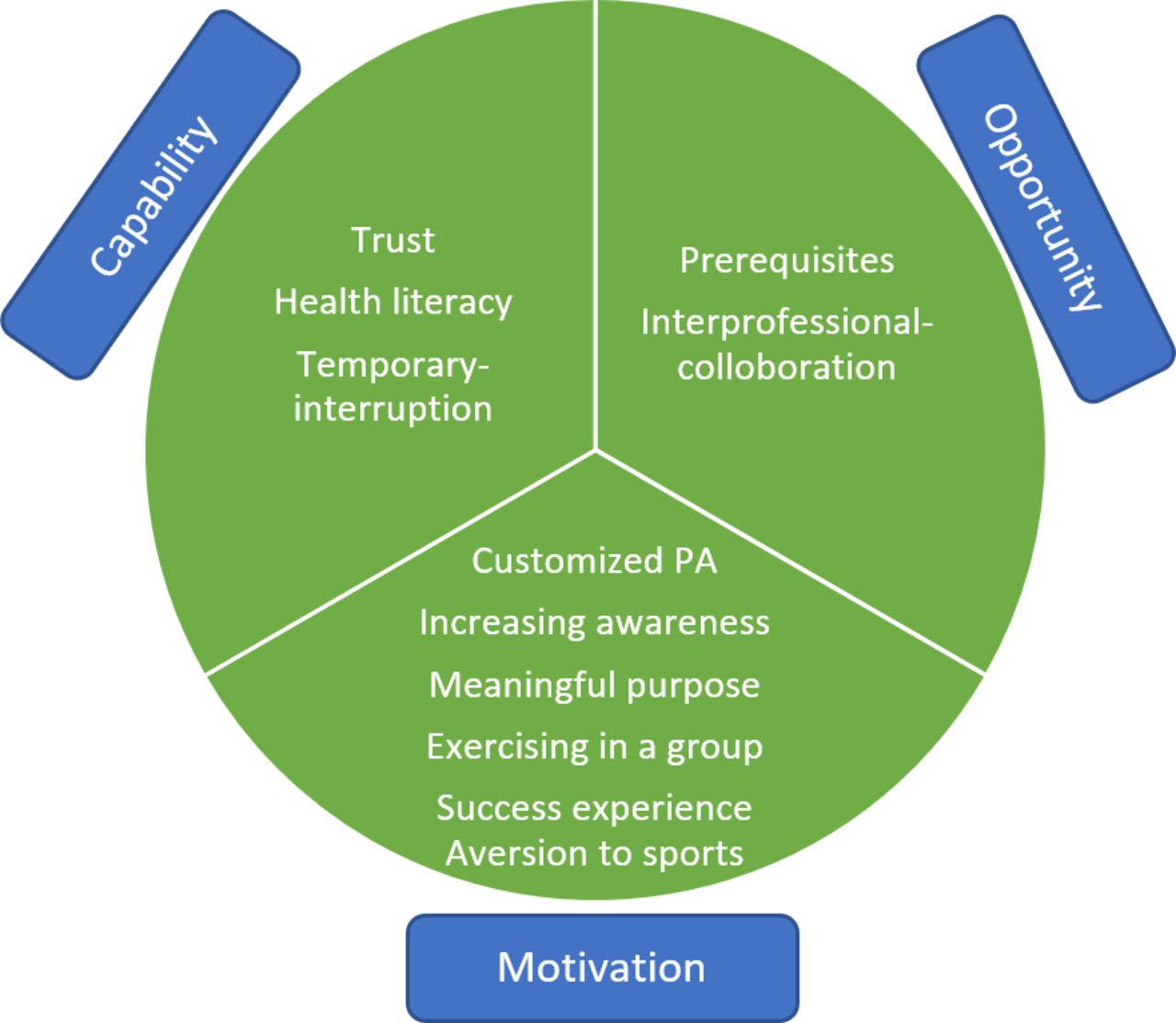
Main themes organised according to COM-B model. The main themes are linked to the C (capability), O (opportunity) or M (motivation).
Results
Twelve patients and eleven healthcare professionals participated (seven physiotherapists, three nurse practitioners and one sports consultant). Table 2 contains a summary of participants’ demographic characteristics.
Characteristics of participants
Themes
The interviews with patients and healthcare professionals resulted in 84 and 83 unique stories, respectively. The researchers selected 26 stories from the patient’s perspective, and 36 stories from the healthcare professional’s perspective (step 4, table 1+ figure 1). Rereading the stories resulted in the emergence of 23 themes in the patients’ stories and 36 themes in the healthcare professionals’ stories (step 5, table 1). After discussion, these themes were clustered into 11 common main themes (figure 1). After that, the main themes were arranged in the COM-B model (step 7, table 1+ figure 2). Exemplar stories are embedded in the text. Some stories are exemplary for multiple themes and will be addressed to in the description of several themes.

{kind=link}
{kind=link}
Results analysis process.
Capability
Three themes seemed to be connected to one’s capability to be physically active: trust, health literacy and temporary interruption.
Trust
Trust encompassed several aspects. First, patients indicated that the lack of confidence in oneself can be an obstacle to be physically active. Limitations in bodily functioning or lack of money were mentioned as reasons as well as feeling ashamed of lack of physical fitness or one’s bodily physique. These aspects sometimes made them feel anxious and inferior—and affected their self-confidence negatively. Healthcare professionals pointed out that they take a patient’s lack of confidence into consideration by approaching the patient in a positive way and proceeding step-by-step, thereby increasing the patient’s self-confidence (stories 1 and 2). Second, both perspectives indicated that trust in the treatment programme is important for successful maintenance of PA. Finally, the patients described that trust in the professional and the treatment programme strongly depends on the feeling of being understood, the social relationship and the experienced expertise of the healthcare professional. The healthcare professional is consciously engaged in gaining trust because its importance is recognised (story 3).
Story 1 ‘Do your own shopping again’
Mara, physiotherapist narrates:
A nice example of what exercise can do to you is a story of one of my patients, a single man (70–79 years). He has diabetes, his lungs are not good, he has chronic back pain and does not walk easily. In the beginning, he was very reluctant to exercise. He was unhappy in his body. Our practice is not a gym. If you approach someone in a positive way and show him that there is a potential improvement, you can achieve so much. He dares to cross the street again, walks outside with his walker and visits us every time he does his groceries to treat us and have a chat. It is nice to see that you can do something for someone in his life. That is why you try to persuade them to go and keep moving. He goes out much more often, has a totally different self-image and feels appreciated again. That is a nice side effect of being physically active.
Story 2 ‘Yes, I’ve done it again’
Mable, patient, narrates:
This summer, for the first time, I managed to swim 40 lanes again. I built it up from four lanes; each time one more lane. At one point, I was back on the 40 lanes. At the end of those 40 lanes, in the water, I was like, ‘Yes, I’ve done it again’. I also told the lifeguard, ‘I’ve got them again! Of course, he was enthusiastic. And on the way to the dressing room, I also told some people who were standing there. They also reacted: ‘Very nice!’ They knew I was working on it. They often asked, ‘Where are you now?’ ‘20 lanes’. ‘So, you only need 20 more’. ‘Where are you now?’ ‘25’. I expanded it to 70 lanes and then I was set back by my knees, so I went back to 50–60 lanes. When the pool closed, I did not swim for 2 weeks. When I started again, I felt like I had loose bones in my knee, that does not swim well… I built that up again and this week I had 40 lanes again. That went smoothly, then I thought: ‘I can do it again’.
Story 3 ‘It comes down to trust every time’
Andy, physiotherapist narrates:
I am a physiotherapist and started with a new patient last week who has a connective tissue disorder. He already had an umbilical hernia 14 times and they can’t operate anymore. If he goes beyond his limits, he is quickly exhausted. He was like: ‘well, let’s talk first because I don’t know if it’s going to work out and I don't know what I can do’. I’ve mainly been talking about that for an hour. And he went away with the outcome that he wanted to try. And that is what I like to hear. I first asked, ‘what have you done in the past’? ‘Then we’re going to build on that, we’ll start and take one step at a time. And he left with the feeling: ‘ok I'm confident I can build up here’. So, I think that is an example of what I stand for when it comes to stimulating healthy exercise behaviour. It comes down to trust every time, that is funny.
Health literacy
Healthcare professionals expressed their inability to help patients with insufficient health literacy. According to them, this inability can originate from the patient (cognitively) or from the framework of the healthcare system (story 4). Patients rarely addressed this topic themselves and may not be aware that healthcare professionals expect some degree of self-management.
Story 4 ‘We just can’t do everything’
Jake, physiotherapist narrates:
A Moroccan man with four children, who is unemployed and deals with a lot of pain, participated in two PA programmes within my practice. He speaks Dutch very well so we could talk about his functional impairments. Both programmes lasted 3 months. In between the programmes, he did not do anything, and his physical functioning deteriorated rapidly. We discussed to see what he wanted, and I even contacted some people who could help him. I said to him ‘you have to take that step yourself, I'm really not going to do that for you’. And he didn't do it. And this really has to do with health literacy. I don’t know if it has to do with Moroccan culture, but in this group I see more often that they do not dare to take the step. Maybe out of pride? We can not take this step for them either. If I want to go to a gym, I have to go there myself. We as physiotherapists do not get paid to take this step together with someone. We have discussed this extensively within the practice and I have already discussed it with the insurance company almost 20 times. We only get paid for the patients who are treated here. Nobody who is outside our profession understands that. We just can’t do everything.
Temporary interruption
Patients said that a temporary interruption of PA, for instance, for medical or social reasons, can be disastrous for sustained PA (stories 5, 6 and 9). They find it difficult to take it up again after an interruption. Healthcare professionals did not specifically mention this as an important theme.
Story 5 ‘In winter it collapses’
Rose, patient, narrates:
In summer, I manage to move around very well. I go to work cycling, it’s nice, warm and sunny. In the autumn or winter, it all collapses with me. I do not really have the inspiration or the desire to do anything. Then I would like to lie in my bed all day, watch TV or read. And you also eat differently, a bit heavier. Spring and summer are really the best time for me. When it rains, I do not feel like going to the gym. And in winter, I do not like it either because I am a person who falls easily. Somehow I can not motivate myself, it is just not easy for me in the winter. Until January, it is usually okay, and after January, it usually gets worse with motivation and energy. That is when I am the least comfortable in my skin.
Opportunity
Prerequisites and interprofessional collaboration
Two main themes linked to ‘opportunity’ were prerequisites and interprofessional collaboration, which can contribute to or have a negative effect on sustained PA. The importance of prerequisites for sustained PA is identified in both perspectives. Patients did not always experience that healthcare professionals are aware of the importance of prerequisites for PA. Suboptimal prerequisites and collaboration between healthcare professionals negatively influence their PA. They underlined the importance of communication (making and keeping appointments) and personal contact (group size, personal attention in group) (story 6). The healthcare professionals mainly mentioned financial, material and logistical prerequisites. Healthcare professionals are aware of the importance of these prerequisites (stories 4 and 7). They describe the importance of good collaboration between several healthcare disciplines for optimal support of the patient (stories 6 and 9).
Story 6 ‘Do something you like’
Fariza, patient narrates:
The nurse practitioner said: ‘you should do something you like’. And walking is something I really like. Then I approached the sports consultant again to maybe find a walking group or something but somehow I have not heard about it. That was also my mistake because I got very ill at that time and then I just could not respond to messages from the sports consultant among others. After that, it has not really been discussed anymore by the sports consultant or something like that.
Story 7 ‘Funds & foundations’
Nathan, sport consultant, narrates:
I have helped a man with a mild intellectual disability. He is in a wheelchair because of an amputation of his right leg and right arm. He had been in military service, and also had post-traumatic stress disorder (PTSD). At first, he had to go to the physiotherapist. By doing so, we have tools to eventually move on to a gym. Through some funds and foundations from the military service and rehabilitation, I was able to raise money, so he could become a member. He owes his membership to that, so it helped him.
Motivation
We found six themes linked to motivation that can function as a barrier or facilitator to reach sustained PA.
Customised PA
The importance of customised PA as a motivator was mentioned from both perspectives. Customised PA should match the capabilities of people (physically and cognitively) and their wishes and preferences. Besides, the healthcare professional should also consider that some people do not like exercising and adapt to that (stories 3, 8 and 9).
Increasing awareness
Another motivation that the healthcare professional often focuses on is increasing awareness of the patient, by using education or confrontation.
Meaningful purpose
Some patients said that having a meaningful purpose motivates them to keep moving (stories 2 and 8). Healthcare professionals also said they often use this as a strategy. They link goals to a patient’s meaningful activities and find that this motivates a patient to persevere (story 1).
Exercising in a group
According to patients and healthcare professionals, exercising in a group can be a facilitator (story 9). Some patients exercise to be among people and not primarily to achieve sustained PA. This knowledge can be used by the healthcare professional in the treatment. By contrast, several patients stated they do not want to exercise in a group.
Success experiences
The importance of success experiences, such as experiencing health benefits, as a facilitator is endorsed from both perspectives (stories 1, 2 and 8). Patients also talked about the negative effect of failure experiences (story 10).
Story 8 ‘Climbing for my granddaughter’
Wilda, patient narrates:
I try to stay as mobile as possible. I do not experience pain; I just get so stiff. When my granddaughter turned 35, I really wanted to go to her birthday. She lives alone in an old house in Amsterdam, with enormous steep stairs. To get to her apartment, I had to climb three steep stairs and I had been sick just before her birthday and had not fully recovered yet. But I did it. I went up all 50 steps and went to her birthday. She is my first grandchild and will always have a special place in my heart.
Story 9 ‘Club’
Eddy, nurse practitioner, narrates:
A woman was at an aquarobics club. She liked this very much but unfortunately she got sick and had some problems in her personal environment. Because of this, she did not go a few times and then she felt the step to go again was too big. Then she came back to me because she thought she did not exercise enough. I contacted the sports consultant and together we took the step to go back. She was very kindly received by the aquarobics club and ever since she goes back again.
Aversion to sports
Aversion to sports is related to patients not liking sports or talking about sports with the healthcare professional—it scares them and can be a barrier. They may not like this, but still want to be more physically active in daily life. The aversion to sports was sometimes described as the unpleasant experience of body signals during intensive exercise and as being related to negative exercise experiences in the past (story 10). Healthcare professionals did not address this topic.
Story 10 ‘Born without a movement-gene’
Vera, patient, narrates:
I like riding my bike, but if I do not move, I like it too. Reading a book on the couch is something I can do for hours. I do not like anything about moving, to be honest. Out of everything, I like cycling the most. As a child, it was terrible. Holidays with my parents in the mountains in Switzerland everyone liked to walk up mountains, except me and that ended in crying and tantrums. I was tired and experienced painful feet of that constant upward walking. I noticed that I do not like being out of breath at all or having soured legs. I think that is terrible, really. Getting out of breath, sweating, your heart rate going up, I find it terrible, a very uncomfortable feeling, really awful. Fun in moving is very difficult for me because I always say ‘I was born without a movement-gene’. In other words, I do not like moving at all.
Discussion
The objective of this study was to identify implicit and more profound barriers and facilitators of sustained PA in patients with a chronic disease, including the patient’s context. Additionally, perspectives of participating patients and healthcare professionals were compared and afterwards linked to the three main parts of COM-B model: capability, opportunity and motivation. In line with findings of Franco and colleagues, trusting oneself—both physically and mentally—and trusting the healthcare professional, were aspects linked to the capability to show a certain behaviour.20 Literature reports that financial, material and logistical conditions and collaboration among healthcare professionals can be both barriers or facilitators for sustained PA.20–22 Important facilitators found in this study were customised PA, awareness of the importance of PA, social aspects of PA, meaningful activities and success experiences. These facilitators are comparable to those reported in the literature.20 23
Although we found similar transcending barriers and facilitators, our study revealed more subtle and profound information about these barriers and facilitators from the patient perspective in daily life. Additionally, we were able to compare and learn from both the perspective of the healthcare professional and the patient. Comparing the perspective of patients with that of healthcare professionals revealed different views and beliefs regarding the main themes of temporary interruption, aversion to sports and health literacy. First, patients may find it difficult to pick up activities after an interruption, which obstructs sustained PA. Such interruptions included medical (eg, surgery) or social interruptions (eg, holiday). In addition, seasonal changes were brought up as possible interruptions. It seems as if patients struggle to cope with setbacks, which is an element of self-management skills (stories 5, 7 and 9).47 Raising healthcare professionals’ awareness of this struggle may provide a valuable lead for improvement of coaching and interventions.48 Second, patients’ stories often revealed an aversion to sports, originating from unpleasant bodily reactions or negative past experiences. Healthcare professionals did not describe this explicitly. Recognising that some patients do not like PA and may prefer talking about ‘moving/movement’ instead of ‘sport/exercising’ could help (story 10). Also, healthcare professionals should be more aware of a patient’s perception of unpleasant bodily reactions and explore how to accommodate for this in the choice of activity, advice or intensity of training. To increase the probability of achieving a sustained effect, healthcare professionals could focus on meaningful PA and integrating PA into the patient’s general daily life as much as possible. A theme only mentioned by healthcare professionals is health literacy. They argued that the Dutch healthcare system does not provide for the extensive support that some patients need due to low health literacy, resulting in more consultations (story 4). Perhaps, these patients were not able to reflect or verbalise the limits of their health literacy, or the healthcare professional is not able to adjust to the needs of the patients. It is important to realise that if a main theme does not emerge from the stories of either patients or healthcare professionals, this does not mean that the persons involved do not have an opinion on that theme. However, because the importance of the themes for sustained PA is indicated from one perspective, it may provide important insights into PA-promoting programmes. In future studies, these themes should be studied more explicitly.
The patients participating in this study all participated or had participated at least once in a PA-promoting programme, which goes to say they were motivated to change their PA behaviour. We specifically chose to include these patients because they could tell about attempts to reach sustained PA. However, this selection of participants limits the transferability of results to a population not participating in a PA-promoting programme. The healthcare professionals selected for this study represent the variety of healthcare professionals in the Dutch primary healthcare system that plays a role in the support of patients with chronic diseases to reach sustained PA.10 Although the sample sizes were relatively small, similar themes were found in the analysis (data saturation was reached). By conducting member checks, our interpretation of the stories was verified by the participants, which positively influences the validation of our data49
The storytelling method allows participants to talk about their own experiences in their own context, without external constraints or preconceived ideas of the interviewer.38 Because stories provide an emphasis to the relationship between experiences and emotions, action and consequences, we obtained profound and implicit knowledge about the subject of this study. In contrast to more general used qualitative study methods in health science, storytelling has the promise to potentially reveal something additive by comprising an individual’s perceived truth linked to their daily life.36 38 39 An important focus point in data used in storytelling research is to strive for a decision-trail that is transparent enough for reproducibility, which was done in this study by following the steps of the COREQ checklist.36 43 By linking the explored barriers and facilitators to theory (COM-B model), results were not only structured and compared with existing literature but were also analysed in light of the context of the participants. Additionally, it should be mentioned that not all found barriers and facilitators could be classified to only one part of the COM-B model, but could be multi-interpretable. For example, the main theme ‘customised PA’ was classified as a motivator but also could be related to opportunity. By conducting phase 3 of our analysis process with all four researchers, discussing thoroughly and rereading the underlying stories, we tried to make sure the classification represents our data as much as possible. Summarised, by using storytelling as our research method and using the COM-B model as a framework, our study revealed insights into promising themes that could assist in designing better interventions for sustained PA.31 32 36
Although most of the researchers who contributed to this study were experienced in conducting qualitative research, the storytelling training indeed assisted to develop the skills to jointly construct narrative and meaning, as suggested in the literature.38 Attention was given to creating an optimal narrative climate, by establishing a relationship prior to the interview, being interested and explaining that there was no right or wrong response. A sensitising question was asked at the start of the interview. Thereafter, narrative questions were asked. Of importance was that the interviewer focused on the storytelling, so as to facilitate appropriate follow-up questions about missing narrative elements (see online supplemental file 2).38 46
In qualitative research, important considerations are the researchers’ professional experience and reflexivity. All four primary researchers werefemale, worked as researchers and teachers at a University of Applied Sciences for physical therapy, and two had worked as physiotherapists in primary care in the past. Being aware of the importance of PA for individual health as well as having opinions and knowledge about the healthcare system might mitigate regarding the data with an open view, limiting the interpretation of the data.50 On the other hand, the interviewers being experienced healthcare professionals may have been an advantage in that the participants probably were more willing to share experiences.51 Conducting a constant comparative analysis method, in which at least two researchers were involved in each selection or analysing part, ensured that the main themes were rooted in the data52 and that intersubjectivity was reached among the four researchers, thereby increasing the quality of the analysis.
New elements found which are important to keep in mind when supporting sustained PA are attention to a possible future temporary interruption and less focus on sports participation. Furthermore, the results of our study underline the importance of taking the patient’s context into account in providing personalised support of sustained PA. While this may cost time during the treatment programme, it might be more efficient to reach sustained PA.
Conclusion
This study identified additional and more detailed information on barriers and facilitators concerning sustained PA in primary care. Building on one’s individual context and comparing the perspectives of both patients and healthcare professionals helped us draft clues for improvement of the support of sustained PA for patients with chronic diseases. Trust in one’s own capabilities and in the healthcare professional, as well as health literacy were main themes emerging from the data. Motivators for sustained PA were customised PA, increasing awareness, social aspects of PA, meaningful goals and activities, success experiences and coping with temporary interruption. Interprofessional collaboration and prerequisites such as financial or materialistic needs can be beneficial or obstructive. We found that paying attention to possible future temporary interruption and less focus on sports participation could be important elements in developing personalised guidance programmes for sustained PA in primary healthcare. Using a narrative method such as storytelling seems appropriate for studies in which context is important.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by The Medical Ethics Committee of Zuidwest Holland METC-number: 19-077. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We would like to thank all participants for their involvement in this study. For sharing their expertise in the storytelling method, we would like to thank Lausanne Mies (trainer on storytelling) and Monique Bussmann (expert on narrative research). For their contributions in collecting data, we would like to thank participating students of the University of Applied Sciences Rotterdam and colleagues of the University of Applied Sciences Leiden (Stephanie Dauphin (MSc), Noura van den Berg (MSc), Vivian Wijsman (MSc). We thank Ko Hagoort for writing assistance.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors JJdB, AF, AH, PS, JV and MS conceived and designed the study. JJdB, AF, AH and PS conducted the interviews. The data analysis was conducted by JJdB, AF, AH and PS. JB drafted the main manuscript text, which was reviewed and edited by the other authors. All authors contributed to data interpretation, and read and approved the final manuscript. JJdB is the guarantor for this manuscript.
Funding This work was supported by Taskforce for Applied Research SIA (RAAK.PUB05.029) and by Vital Delta: Medical Delta’s journey towards vitality and health, funded by Taskforce for Applied Research SIA (SPR.VG01.006) and Medical Delta.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.