Article Text

Abstract
Objectives Studies have demonstrated that it is possible to prevent type 2 diabetes for individuals at high risk, but long-term results in the primary healthcare are limited and high dropout rates have been reported.
Design A longitudinal design was used to study changes in participants’ diabetes risk and anthropometrics from baseline to 60 months follow-up. A cross-sectional design was applied to investigate differences between dropouts and completers of the 60 months follow-up.
Setting Healthy Life Centres in the Norwegian primary healthcare.
Participants 189 individuals aged >18 years with a Finnish Diabetes Risk Score ≥12 and/or a body mass index (BMI) ≥25 kg/m2 were included and offered to attend Healthy Life Centre programmes for 12 months. Measurements were performed annually up to 60 months after inclusion.
Interventions Healthy Life Centres arrange behavioural programmes including physical activity offers and dietary courses as part of the primary healthcare. This study offered individuals to attend Healthy Life Centre programmes and followed them for 60 months.
Primary outcome Assess changes in participants’ diabetes risk, cardiovascular measures and anthropometrics from baseline to 60 months.
Secondary outcome Investigate characteristics of dropouts compared with completers of 60 months follow-up.
Results For participants at 60 months follow-up, diabetes risk and anthropometrics decreased (p<0.001). Out of 65 participants classified as high risk for diabetes at baseline, 27 (42%) changed to being at moderate risk at 60 months follow-up. Remission of diabetes was seen for six of nine participants. Of 189 participants enrolled in the programme, 54 (31%) dropped out at any given point before 60 months follow-up. Dropouts were younger with higher, BMI, weight and waist circumference compared with the completers (p<0.001).
Conclusions Having a long-term commitment for participants in primary healthcare interventions could be beneficial for the reduction of diabetes risk and improvement of anthropometrics as shown at the 60 months follow-up.
Trial registration number NCT01135901.
- diabetes & endocrinology
- public health
- health services administration & management
- change management
- organisation of health services
Data availability statement
Data are available on reasonable request. The data supporting the findings in this article can be found at the Centre for Obesity Research (ObeCe), St. Olavs Hospital, Trondheim, Norway and are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- diabetes & endocrinology
- public health
- health services administration & management
- change management
- organisation of health services
Strengths and limitations of this study
The 60 months follow-up constitutes the longest follow-up on Healthy Life Centre (HLC) programmes and primary healthcare programmes in Norway to prevent type 2 diabetes for people with overweight and/or obesity.
The study intervention was to offer participants to attend the existing HLC programme in the primary healthcare, to secure its validity and transferability for clinical practice.
The cross-sectional design used to compare dropouts versus completers, is limited in its ability to elucidate causal relationships, thus, the design yields information about associations and allowed us to compare the two groups.
For the longitudinal design used, there was no control group for the follow-up measures, which limits the generalisability of findings.
There was no control group due to randomising participants against their expressed will to treatment, which solely involves behavioural change, may result in very low compliance of participants, which made a randomised design unfeasible in the given setting for HLC programmes in the Norwegian primary healthcare.
Introduction
In western countries, type 2 diabetes (T2D) is highly prevalent and the most associated risk factor of the condition is increased body mass index (BMI).1 Prevention of T2D has been emphasised the last 30 years.2–4 A large amount of studies have found that the onset of T2D for individuals at high risk can be postponed with behavioural interventions including dietary changes and physical activity.5–11 Furthermore, of individuals with newly diagnosed T2D (>6 years) who attended a behavioural intervention study found remission of T2D among 50% of them12 after 1 year and the remission was sustained after 2 years for more than a third.13
Initially, studies regarding prevention of T2D were conducted with randomised controlled trials (RCTs) performed in comprehensive experimental settings.5–10 It was further emphasised as necessary to replicate the RCTs in primary healthcare settings to investigate the feasibility and effectiveness of behavioural interventions in real life.14 Consequently, studies provided promising results,15–19 showing that it was also possible to prevent T2D in primary healthcare settings.20–22 Nevertheless, there are only a few studies reporting long-term results of interventions aiming to reduce the development of T2D.15–18 23 Results from a cohort inthe National type 2 diabetes prevention programme in Finland (FIN-D2D) with 7.4-year follow-up showed long-term benefit with reduced incidence of drug-treated T2D for individuals who had achieved a moderate weight loss during a 12 months programme of lifestyle counselling in primary healthcare.23 A large amount of literature has acknowledged a lack of more research on long-term follow-up of interventions aiming to reduce the development of T2D.24–27 In interventions to prevent T2D, participants with less healthy behaviour have been more likely to drop out.28 High dropout rates have in general been a problem for interventions with dietary changes and physical activity, in essence questioning the success of the intervention strategies.29–31
In Norway, Healthy Life Centres (HLC) in primary healthcare target individuals with chronic conditions or at high risk of diseases who need support to change their lifestyle.32 The HLC offer programmes containing dietary and physical activity courses. However, there is great uncertainty to what extent interventions like HLC programmes actually contribute to improved health outcomes.33 The HLC programmes’ content, resources and setting are drawn into question in relation to achieving positive health outcomes for participants.34 The largest Norwegian study of HLC participants to date found that the initial improvement in physical activity levels immediately after the intervention was not maintained at 12 months follow-up.35 However, another study found improved diabetes risk measures and anthropometrics at 24-month follow-up.36 Furthermore, of participants at high risk for developing T2D invited to attend an HLC programme in Norway, the majority did not meet to participate and their characteristics showed that they had lower education levels and were more often unemployed than those who attended the HLC programme.36
To date, research on long-term impact (>24 months follow-up) of HLC programmes on participants’ health outcomes like diabetes risk measures and anthropometrics is lacking. Thus, the primary aim of this study was to study the development in participants’ diabetes risk measures, cardiovascular measures and anthropometrics at 12, 36 and 60 months follow-up. Based on the results of previous studies on HLCs,33–36 the question was raised who benefits of attending the HLC programmes. To determine if the HLC may appeal only to a certain section of the target population, the second aim of this study was to investigate if participants who dropped out differed from those who completed the 60 months follow-up to provide some better insights into which groups of people are more likely to drop out.
Research design and methods
Study design
A longitudinal, non-randomised, single-arm, pre-post examination was used to investigate the development in participants diabetes measures, anthropometrics and cardiometabolic changes with follow-up assessments at baseline, 12, 36 and 60 months after inclusion.
A cross-sectional design was used to investigate if participants who dropped out at any given point before 60 months differed from participants who completed the 60 months follow-up.
Patient and public involvement
When planning the study, the research group presented the study protocol for a group of appointed patients representing their conditions (overweight, obesity, T2D and cardiovascular diseases) to involve them in the planned study. They were presented for the research question, the design, intervention and the conduct of the study. Some changes were performed after their feedback regarding the intervention period. They could also comment on the outcome measures and recruitment of the study, where different options for recruitment sites were obtained from the group. They were introduced to the methods and had the possibility to give the research team feedback of their thoughts about the methodological part of the study, whereas no comments were obtained.
Thus, they had several suggestions for the dissemination of the study results, both to participants, to their own group and to the municipalities involved.
Study setting and intervention
The Regional Centre for Obesity Research and Innovation (ObeCe), St. Olav’s Hospital, Trondheim initiated the VEND-RISK study in collaboration with four municipalities (Stjørdal, Meråker, Tydal and Selbu) in Central Norway.
The VEND-RISK study purposely intended using existing local interventions in the primary healthcare. Participants were thus offered to attend the HLC programmes serving the four municipalities. The practical organisation of HLC services is largely shaped at the community level depending on local framework conditions and priorities. It is based on local resources and executive work in each municipality.32 The HLCs serve as a low-threshold health service and Norway’s public health insurance covers the cost of participation.30 HLCs are defined as individual and group-oriented programmes to promote health and to enhance social communities.32
The personnel in the HLC serving the four municipalities was two nurses, whereas one was a study nurse, two contracted physiotherapists and a part-time clinical nutritionist.
The participants attended the HLC programme for 12 months, that is, three periods with 12 weeks offers. In the beginning and at the end of every three periods during the 12 months of the programme, the study nurse performed individual health conversation. The conversation in the beginning was meant to clarify the participants’ resources, motivation as well as to set goals. The conversation at the end was meant to evaluate the process and make plans for how to maintain healthy habits. The health conversations were based on principles from Motivational Interviewing. The Norwegian Directorate of Health arranges certification courses for the HLC personnel for the use of Motivational Interviewing.
The HLC offered one group-based nutrition course once every period of 12 weeks; ‘good food for better health’, developed by the Norwegian Directorate of Health.32 The course went over 4 weeks with 2 hours sessions (a total of 10 hours), both theoretical and practical with different themes for each session. The course aimed to inspire to have healthy food choices and good dietary habits with the intention to have a good start to achieve sustainable changes in nutrition habits. All participants received a cook book produced for the course. The nutrition course was based on the national dietary advice.37 Individual conversations were used to address eating habits including diet and nutrition, and participants who wanted could get more counselling and individual follow-up with the HLC clinical nutritionist.
Various physical activities, which were optional indoor and outdoor activity classes were offered continuously over the 12 months, two to four times a week with a duration of 1–2 hours each. The classes were both individual and group-based, and included cardio and resistance training. The intention was to get participants to be more physically active and to follow the national recommendations for physical activity. Participants’ feedback about what they preferred and found feasible regarding their physical condition was continuously considered. In addition, the HLC personnel provided information about activities in the local municipality such as hiking possibilities, fitness clubs, swimming, exercise classes and walking groups that participants could attend.
Inclusion criteria and recruitment
Individuals aged >18 years living in the municipalities: Stjørdal, Meråker, Tydal and Selbu were included in the study with the following inclusion criteria: they had a Finnish Diabetes Risk Score (FINDRISC) ≥12 and a BMI ≥25 kg/m2. Also, some individuals (n=10) without FINDRISC >12, but with a BMI ≥25 kg/m2 were included. The inclusion criteria for participants having a BMI ≥25 kg/m2 was based on the Norwegian national guideline for the primary healthcare regarding prevention, screening and treatment of overweight and obesity.38
Participants for the VEND-RISK study were recruited at four different time-points: 2010, 2011, 2012 and 2013. From 2010 to 2012, eligible participants were recruited through an advertisement in a local newspaper and by referrals from general practitioners (GPs). The recruitment in 2013 was conducted in collaboration with the North-Trøndelag Health Survey 3 (HUNT3), where participants who were identified with a high risk for developing T2D got an information letter and an invitation to attend the VEND-RISK study.36
Participants
Altogether, 194 participants met the inclusion criteria, 5 were excluded (BMI <25 kg/m2) resulting in 189 participants enrolled in the HLC programme. During the follow-up period, 15 were excluded and 54 dropped out at any given point before 60 months (figure 1). Participants were excluded when having had bariatric surgery (n=3) or conservative treatment for obesity in specialised healthcare (n=7), or if their levels of physical function were reduced due to pregnancy (n=2) or serious illness that required treatment (n=3).
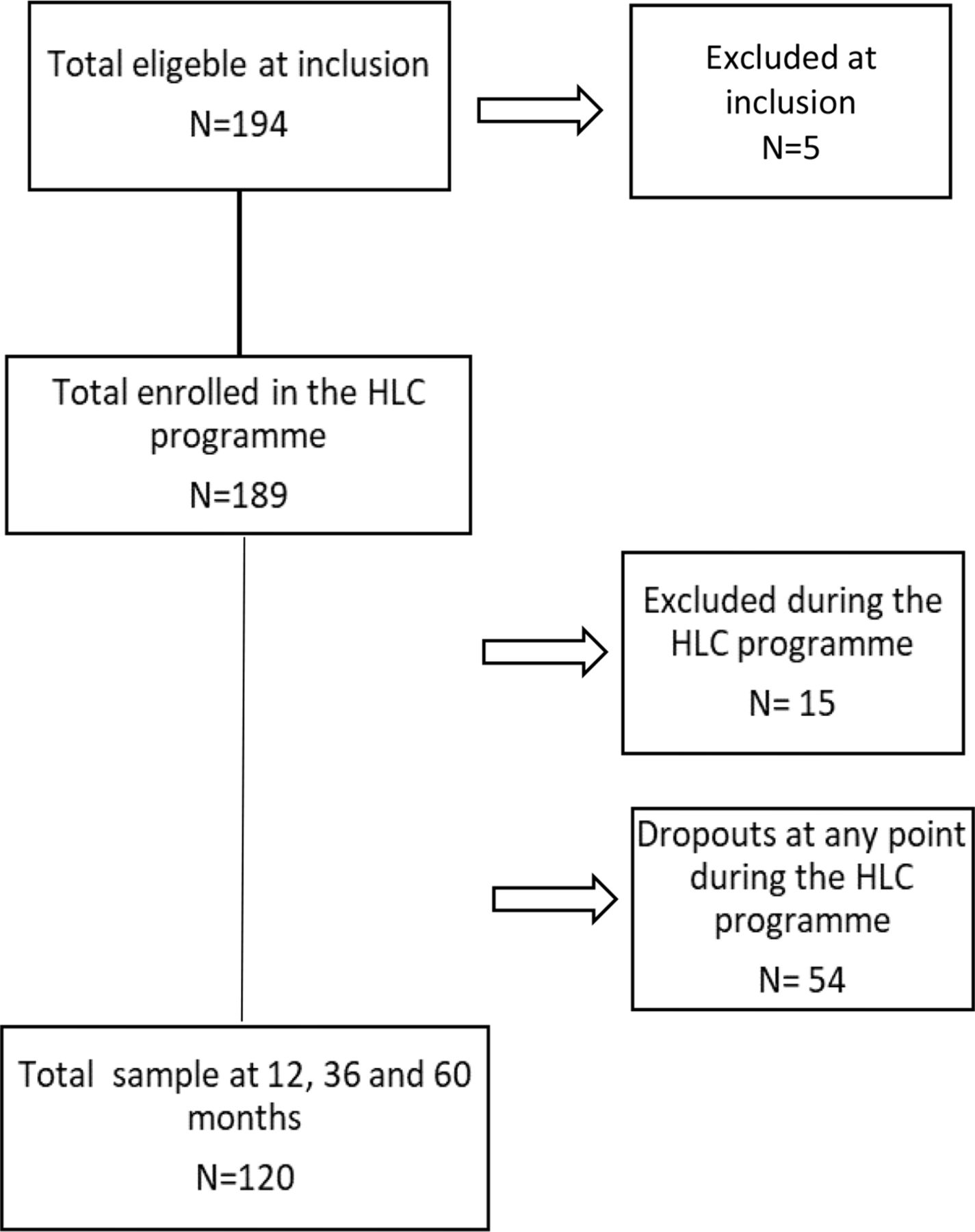
Sample size at inclusion, number excluded, total number of participants enrolled in the Healthy Life Centre (HLC) programme, number excluded during the time of the programme and total sample at 12, 36 and 60 months.
The final sample consisted of 120 participants.
Measurements and procedures
The participants had annual follow-up tests for 60 months prospectively. Because of different time-points for inclusion, measurements were collected at different times: baseline measures were assessed from 2010 to 2013, 12 months follow-up measures from 2011 to 2014, 36 months follow-up measures from 2013 to 2016 and 60 months follow-up measures from 2015 to 2018.
The sociodemographic characteristics collected were age, gender, civil status, occupational status and voluntary work. Civil status was categorised as married/co-living or being single/widowed. Occupational status was categorised as working, sick leave/disability benefits and retired. Voluntary work could be attendance in local groups such as Norwegian Women’s Public Health Association, The Cancer Association and The Heart-Lung Association. The answer to the category was either yes or no.
To measure diabetes risk, haemoglobin A1c (HbA1c in %/mmol/mol) and the FINDRISC questionnaire (range: 0–26) were used.
The anthropometric measures included were height and weight (for BMI) and waist circumference (WC). The measurement of height and weight followed a standardised procedure where participants wore light clothes and no shoes. BMI was calculated as weight divided by height squared (kg/m2). WC was measured at the iliac crest at end expiration with measuring tape.39
To assess cardiovascular risk factors, triglycerides, total cholesterol, high-density lipoprotein cholesterol and low-density lipoprotein cholesterol were measured with blood samples.
VO2-max test were presented as mL/kg/min (mL of oxygen per kilogram of body weight per minute). The test was performed with oxygen and carbon dioxide analysers, heart rate monitor and a stopwatch. A treadmill was used, except for two participants where a training cycle was used. The treadmill and cycle were checked and calibrated. The test procedure was explained to the participants, and a screening of health risks was conducted. Appropriate warm-up was performed. Oxygen uptake was calculated from measures of ventilation, as well as oxygen and carbon dioxide levels in the expired air. The maximum level was determined at or near test completion. The test was performed according to an individually adapted protocol with constant speed where the incline of the treadmill increased by 2% every minute until the participant reached VO2-max. Expired air was collected and volume measured via MetaMax II (Cortex MetaMax II, Cortex, Leipzig, Germany) and Douglas bags (Hans Rudolph, Kansas City, USA). Heart rate was measured with a heart rate belt and heart rate monitor (Polar RS400, Polar Electro Oy, Kempele, Finland). VO2-max was reached if the following occurred: a plateau or ‘peaking over’ in oxygen uptake, maximum heart rate was reached, attainment of a respiratory exchange ratio of 1.05 or greater, if uptake did not increase by >2 mL/kg/min at maximum working load, and volitional exhaustion.
The HLC personnel collected the sociodemographic characteristics, FINDRISC and performed the measurements of height, weight and WC. Blood samples were taken at the local GP office requisitioned by the medical doctor responsible for the VEND-RISK study (BK). The VO2-max test was performed by an exercise physiologist from the Department of Circulation and Imaging (ISB), Norwegian University of Science and Technology (NTNU) and one of the contract physiotherapists at the HLC.
Analyses
All analyses were conducted using the IBM Statistical Package for Social Sciences V.26. Two different analysis steps were implemented.
First, to study the development of the diabetes risk measures, anthropometrics and cardiovascular risk measures from baseline to 12, 36 and 60 months, repeated measurement analysis of variance F-tests have been adjusted for violation of the sphericity assumption using the Huynh-Feldt correction formulas. Missing values within these analysed indicators were imputed following the procedure recommended by Schafer and Graham.40 Weight, WC and VO2-max measures were stratified by gender. The VO2-max test was conducted for too few participants at 12 months to be included; missing values was imputed with a maximum likelihood estimation using all available information.
To further illustrate the changes in the participants’ diabetes risk measures, the HbA1c levels at baseline, 12, 36 and 60 months were categorised into three groups: moderate risk (HbA1c <6.0%, 42 mmol/mol), high-risk (HbA1c 6.0%–6.5%, 42–48 mmol/mol) and possible diabetes (HbA1c >6.5%, 48 mmol/mol).
Second, baseline characteristics of those who dropped out during the study, that is, dropouts, and those who met the follow-up measures, that is, completers, were described with means and SD. Independent sample t-tests with bias-corrected bootstrapped CIs were applied to see if there were any differences between dropouts and completers.
Results
Table 1 and figure 2 display the developments in anthropometrics, T2D risk cardiovascular risk measures and VO2-max tests from baseline to 12, 36 and 60 months follow-up. The results at 12 months follow-up show significant reduction in participants measures with mean differences of −0.2 mml/L in HbA1c, −1.0 points in the FINDRISC, −3.4 kg (men)/−1.6 kg (women) body weight, −0.7 kg/m2 BMI and −3.9 cm (men)/−1.7 cm (women) in WC. The improvements in measurements are maintained at 36 months follow-up and HbA1c further improved at 60 months follow-up. The VO2-max test scores improved significantly, that is, +0.3 (men) and +5.3 (women) mL/kg/min at 60 months follow-up. The effect size for all effects was small, with the exception of reduction of VO2-max test where the effect size was medium. Of the 189 participants enrolled in the VEND-RISK study, 54 (31%) dropped out at any given point before 60 months follow-up. Table 2 provides the results of the comparison between dropouts and completers who finished the 60 months follow-up. Dropouts were at the point of inclusion significantly younger with a lower FINDRISC, they had significant higher body weight, BMI and WC. Those who dropped out were also less engaged in voluntary activities.

Development of body weight (A), body mass index (BMI) (B) waist circumference (C), haemoglobin A1c (HbA1c) (D), Finnish Diabetes Risk Score (FINDRISC) (E), cholesterol (F), high-density lipoprotein cholesterol (HDL) (G), low-density lipoprotein cholesterol (LDL) (H), triglycerides (I), and VO2-max (J) at baseline, 12, 36 and 60 months measurements among participants (n=120). Missing values are imputed with a maximum likelihood estimation using all available information.
Repeated measure ANOVA results for the blood tests with Huynh-Feldt correction for violation of the sphericity assumption (n=120)
Comparison of dropouts (n=54) and completers who fulfilled 60 months (n=120)
Figure 3 shows that the number of 65 (54%) participants with high risk for T2D (HbA1c 6.0%–6.5%, 42–48 mmol/mol) at baseline decreased to 40 (33%) participants (HbA1c <6%, 42 mmol/mol) at 36 months into the VEND-RISK study, which improved further to 38 (32%) participants at 60 months. Nine participants were categorised as having possible diabetes at baseline, whereas only three had possible diabetes at the 60 months follow-up. Of the nine participants in the possible diabetes group at the baseline, six changed into a lower risk group. These six had a mean weight reduction in this time of 10.1 kg (SD 14.5), whereas the three participants who remained in the possible diabetes group had a mean weight reduction of 2.6 kg (SD 4.1). From 36 to 60 months, five of six participants went from being in the possible diabetes group to lower risk categories. These five had an average weight reduction of 3.7 kg (SD 4.3), whereas the one participant who remained in the possible diabetes category had no change in weight. Due to the small numbers, no meaningful statistical tests could be calculated for these comparisons.

{kind=link}
{kind=link}
{kind=link}
Number of participants categorised with haemoglobin A1c (HbA1c) levels as moderate risk (HbA1c <6%, 42 mmol/mol), high risk (HbA1c 6.0%–6.4%, 42–48 mmol/mol) and possible diabetes (HbA1c >6.5%, 48 mmol/mol) at baseline, 36 and 60 months and their changes (coloured trajectories) between categories from baseline to 36 and 60 months. The green columns (moderate risk) trajectories from baseline to 36 months show that four participants went to high risk (yellow line) and two to possible diabetes (red line). From 36 to 60 months, 11 participants went to high risk (yellow line) and none to possible diabetes. The yellow columns (high risk) trajectories from baseline to 36 months show that 34 participants went to moderate risk (green line) and 1 to possible diabetes (red line). From 36 to 60 months, 15 participants went to moderate risk (green line) and 2 to possible diabetes (red line). The red columns (possible diabetes) trajectories from baseline to 36 months show that six participants went to high risk (yellow line). From 36 to 60 months, four participants went to high risk (yellow line) and one to moderate risk (green line).
Conclusions
Our results demonstrated that it was possible to reduce T2D risk measures for participants at high risk, as shown previous studies,5–11 14–18 thus not in a Norwegian HLC setting. Furthermore, our findings of improvements in participants’ physical activity level by VO2-max after the intervention (12 months) was maintained at 36 and 60 months follow-up. Participants at high risk for T2D in this study slightly decreased their body weight from baseline to 60 months follow-up. Previous studies have found modest weight losses of 5% to <10% associated with significant improvements in cardiovascular risk factors at 12 months.41 Although differences in body weight and lipids did not reach statistical significance in our study, the T2D risk measures was reduced, which implicates that small changes could protect against developing T2D. The results at 60 months should be interpreted as positive, especially since anthropometrics, diabetes risk and cardiovascular measures indicate a long-term maintenance of change in health behaviour of the participants. The maintenance of changes is often discussed as one of the greatest challenges in lifestyle interventions. The ‘Hawthorne effect’ could partly explain the maintenance of diabetes risk measures, VO2-max and anthropometrics in our study as it makes participants especially motivated to comply as they know they are part of a study and are being observed.42 However, previous findings on HLC participants’ maintenance of physical activity level that increased during the HLC programme was found to be decreased from the measures right after intervention, that is, 3 months, to the measures at follow-up, that is, 12 months.35 However, our study intervention was longer, that is, 12 months, and with longer follow-up, that is, 60 months. Shorter interventions, <12 months have shown limited evidence on clinically meaningful benefit for outcomes on body weight.43 Hence, our findings of reduction in anthropometrics and maintenance at follow-up measures add to other studies on lifestyle interventions with clinical meaningful reduction in body weight, saying that programmes over 12 months or more can help to achieve clinically meaningful weight loss and lower mortality during long-term follow-up.44 The presence suggests that participants at high risk for T2D and/or with overweight or obesity in HLC programmes should have a 12-month intervention period to help for behavioural change that could result in the improvement and maintenance of improvement in VO2-max and the reduction and maintenance of reduction in diabetes risk measures and anthropometrics. In addition, previous research has suggested that commitment and maintaining regular contact with participants in behavioural interventions is recommended for achieving long-term change.45 Participants in our study had regular health conversations with the study nurse during the first 12 months, and further in the annual measurements, which may be of importance for participants’ behavioural change.
As our findings showed a substantial dropout (31%), it could seem like HLC programmes do not appeal to a certain part of the target population. Based on our findings of dropout characteristics and previous studies from HLC programmes,33–36 it looks like differences in the dropouts and completers’ characteristics could indicate a different need for support in the HLC programmes. As discussed above, the present findings indicate that the HLC programme was adequate for completers to reduce their diabetes risk measures and anthropometrics. Basically, the dropouts in our findings had higher BMI and WC compared with the completers, consistent with results from another study that also found that dropouts had higher BMI.46 Furthermore, our study dropouts were younger compared with the completers, as previous studies investigating dropout of lifestyle interventions also have found.47 Thus, dropouts in our study had a lower FINDRISC that could be explained by the lower age, as age <45 years gives more score on the FINDRISC scheme. Previous findings showed that younger age of participants at high risk for T2D was associated with higher expectations and clarity regarding lifestyle changes.48 Unfortunately, that those being younger with higher BMI and WC dropped out suggests that they may need an intervention the most, and this has also been suggested by previous findings.47 Hence, to improve the effectiveness of HLC programmes and reducing the dropout rate it would be an idea to identify those at high risk of dropping out early on and provide them with the necessary support, like a more individualised treatment. Another possibility is to limit the access to HLC programmes to those expected to complete and thus provide other treatment or interventions for those likely to dropout. Either, the ideal had to be that HLC programmes were more individualised and with different intervention levels. Personnel at HLCs could though address and facilitate for those who might need more support with other means. Thus, investigating the future health characteristics of this study’s dropouts and if they will be in need of healthcare services would give more knowledge.
For this study, several strengths and limitations should be discussed. The cross-sectional design used to compare dropouts versus completers is limited in its ability to elucidate causal relationships. Nevertheless, the design yields information about associations and allowed us to compare the two groups.49
For the longitudinal design used, there was no control group for the follow-up measures, which limits the generalisability of findings. However, randomising participants against their expressed will to treatment, which solely involves behavioural change, may result in very low compliance of participants, which made an RCT design unfeasible in the given setting for HLC programmes in the Norwegian primary healthcare. A systematic bias could have occurred regarding motivation for the sample, and if the study had been two-armed, this could have been avoided. Nonetheless, single-arm studies are useful for assessing the effect of novel regimes (as this study intervention), for which it may not be feasible, or desirable, to use an RCT. Furthermore, unlike cohort studies, the differences observed from baseline to 12, 36 and 60 months are less likely to be the results of cultural of generational differences as the differences are observed within the group.49 For the study reliability, the same research nurse collected all information at the annual follow-up measures, and the same exercise physiologist performed the aerobic capacity (VO2-max), securing the internal validity of our study. Height, weight and WC were measured, not self-reported, which is considered to give more precise results.50
Participants for the VEND-RISK study were included with FINDRISC, a widely recommended prediction tool for T2D which makes the study relevant for the primary healthcare setting.38 The inclusion criterion for the FINDRISC as low as >12 was chosen because there were participants who wanted to attend who were <45 years of age, and intervening on younger individuals could be favourable for those in need of intervention, as >45 years is one of the scores on the scheme.51 The Norwegian national guideline for diabetes recommends individual assessments of patients <45 years with high BMI.52 Hence, this study included individuals at high risk also aged <45 years with a FINDRISC <12 who had other high-risk parameters, like a BMI ≥25 kg/m2, that is, they are entitled to treatment in the primary healthcare.38 These decisions were made to ensure relevance for clinical practice in the primary healthcare and to target the VEND-RISK study’s intention to prevent T2D, for individuals with overweight or obesity. The result of the participants in this study who were categorised as having possible T2D should be interpreted with caution as ‘possible diabetes’ is not the same as having diagnosed diabetes. The national guideline distinguishes between ‘possible diabetes’ and ‘diabetes’. The recommendation for diagnosing T2D is by using at least two of three measures, that is, HbA1c ≥48 mmol/mol (≥6.5%), and fasting plasma glucose ≥7.0 mmol/L and/or glucose ≥11.1 mmol/L 2 hours after a glucose stress test. Value above the diagnostic limit must be confirmed in a new sample before the diagnosis can be made.52
This study’s 60 months follow-up constitutes the longest follow-up on HLC programmes, that is, primary healthcare programmes in Norway to prevent T2D for people with overweight and/or obesity. The study could be affected by that the completers in the 60 months follow-up were highly motivated for lifestyle change, thus, our study intervention was only to offer participants to attend the existing HLC programme in the primary healthcare, to secure its validity and transferability for clinical practice. In addition, our results present the dropouts characteristics, suggesting there is a discrepancy for individuals with high risk for T2D and with overweight/obesity and needs support or preferences for interventions in the primary healthcare.
Data availability statement
Data are available on reasonable request. The data supporting the findings in this article can be found at the Centre for Obesity Research (ObeCe), St. Olavs Hospital, Trondheim, Norway and are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
The Regional Committee for Medical Research approved the VEND-RISK study (REK nr 2010/696). Participants in the VEND-RISK study received oral and written information to enable them to approve and sign an informed consent form.
References
Footnotes
Contributors ISF is the guarantor of the present study with full responsibility for the work and/or the conduct of the study, had access to the data, and controlled the decision to publish. BK planned and was responsible for the VEND-RISK study. ISF and BK designed the present study together with MTD and CK. CK analysed the data and interpreted the results, discussing with BK, MTD and ISF. ISF drafted the manuscript with comments from BK, MTD and CK. All authors read the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Disclaimer This work was supported by Centre for Obesity Research, St. Olavs Hospital, Trondheim, Norway.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.