Article Text

Abstract
Introduction Pulmonary hypertension is a major determinant of postnatal survival in infants with a congenital diaphragmatic hernia (CDH). The current care during the perinatal stabilisation period in these infants might contribute to the development of pulmonary hypertension after birth—in particular umbilical cord clamping before lung aeration. An ovine model of diaphragmatic hernia demonstrated that cord clamping after lung aeration, called physiological-based cord clamping (PBCC), avoided the initial high pressures in the lung vasculature while maintaining adequate blood flow, thereby avoiding vascular remodelling and aggravation of pulmonary hypertension. We aim to investigate if the implementation of PBCC in the perinatal stabilisation period of infants born with a CDH could reduce the incidence of pulmonary hypertension in the first 24 hours after birth.
Methods and analysis We will perform a multicentre, randomised controlled trial in infants with an isolated left-sided CDH, born at ≥35.0 weeks. Before birth, infants will be randomised to either PBCC or immediate cord clamping, stratified by treatment centre and severity of pulmonary hypoplasia on antenatal ultrasound. PBCC will be performed using a purpose-built resuscitation trolley. Cord clamping will be performed when the infant is considered respiratory stable, defined as a heart rate >100 bpm, preductal oxygen saturation >85%, while using a fraction of inspired oxygen of <0.5. The primary outcome is pulmonary hypertension diagnosed in the first 24 hours after birth, based on clinical and echocardiographic parameters. Secondary outcomes include neonatal as well as maternal outcomes.
Ethics and dissemination Central ethical approval was obtained from the Medical Ethical Committee of the Erasmus MC, Rotterdam, The Netherlands (METC 2019-0414). Local ethical approval will be obtained by submitting the protocol to the regulatory bodies and local institutional review boards.
Trial registration number NCT04373902.
- NEONATOLOGY
- PERINATOLOGY
- Respiratory physiology
- OBSTETRICS
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This is the first randomised controlled trial evaluating the effect of physiological-based cord clamping on the incidence of pulmonary hypertension in the first 24 hours after birth in infants with a congenital diaphragmatic hernia (CDH).
To detect a clinically relevant difference in mortality a significantly larger sample size would be required, but pulmonary hypertension is an adequate proxy as it is a major contributor to mortality in infants with a CDH.
Treatment allocation cannot be blinded in this trial; to account for this, objective echocardiographic parameters are used to objectify the primary outcome.
Real-time monitoring of physiological parameters will improve our understanding of the physiological changes occurring during the perinatal stabilisation period in infants with a CDH.
Although a multicentre trial has inherent disadvantages, collaboration is essential given that CDH is a rare disease; the use of a relatively early primary outcome may decrease the impact of centre-specific differences.
Introduction
A congenital diaphragmatic hernia (CDH) is a birth defect characterised by incomplete closure of the diaphragm. Abdominal organs herniate into the fetal thorax and interfere with lung development, thereby contributing to the development of pulmonary hypoplasia.1–8 Pulmonary hypoplasia translates in delayed lung aeration after birth, thereby requiring prompt resuscitation and respiratory support. In anticipation of this requirement, the umbilical cord is usually clamped immediately after birth so that the infant can be transferred to a resuscitation table. Despite extensive respiratory support, infants with a CDH face significant mortality (around 30% in most series) and long-term morbidity, with many survivors suffering from chronic respiratory problems and pulmonary hypertension.9–12 The aetiology of pulmonary hypertension in infants with a CDH is multifactorial. Abnormal structural development of the vasculature, altered vasoreactivity, and progressive vascular remodelling are considered important factors in developing and maintaining high perfusion pressures in the lungs.13–15 Postnatal left ventricular systolic dysfunction correlates with outcomes in infants with a CDH and also contributes to the development of pulmonary hypertension.16 17 Pulmonary hypertension can develop in the first hours after birth and can persist for weeks to even months. The presence of severe pulmonary hypertension at 1 month of life is associated with a 56% mortality rate prior to discharge.18 Current treatment options for pulmonary hypertension are limited and mainly consist of pulmonary vasodilator drugs with varying responses and the use of extracorporeal membrane oxygenation.19
Currently, immediate cord clamping is performed in almost all infants born with a CDH. Before cord clamping, oxygenated blood in the umbilical veins shunts to the left atrium via the ductus venosus and foramen ovale, thereby guaranteeing venous return to the left ventricle of the heart.20 21 Thus, clamping the cord separates the infant from both its oxygen source as well as the blood flow required to maintain left ventricular preload.20 21 In addition, left ventricular afterload increases when the low-resistance circulation of the placenta is removed.20 21 As a result, cardiac output decreases. In term neonates with normal lung development, lung aeration causes the pulmonary vascular resistance to decrease and the pulmonary blood flow to increase, allowing the lungs to take over from the placenta in providing gas exchange (oxygenation) and maintaining cardiac output.20 21
In contrast, most infants born with a CDH are faced with a complicated transition from the fetal to the neonatal phenotype. Due to the abnormally developed pulmonary vasculature and hypoplastic lungs, lung aeration is delayed and, thus, the pulmonary vascular resistance does not decrease sufficiently to accommodate the entire output of the right ventricle.21–23 Pulmonary vascular pressures then increase and potentially result in a reactive vasospasm triggering vascular remodelling, perpetuated by ongoing hypoxic pulmonary vasoconstriction.22 When lung aeration is established prior to clamping the cord, called physiological-based cord clamping (PBCC), the lungs will already have taken over the placental function before the cord is clamped, thereby avoiding the hypoxia and high pulmonary arterial pressures that can occur after immediate cord clamping (figure 1). Recently, in an ovine model of a diaphragmatic hernia, we have confirmed that PBCC resulted in significantly lower pulmonary arterial pressures while maintaining higher pulmonary blood flows up to 20 and 120 min after birth, respectively.22 PBCC, thus, has the potential to influence the functionality of the pulmonary vessels.
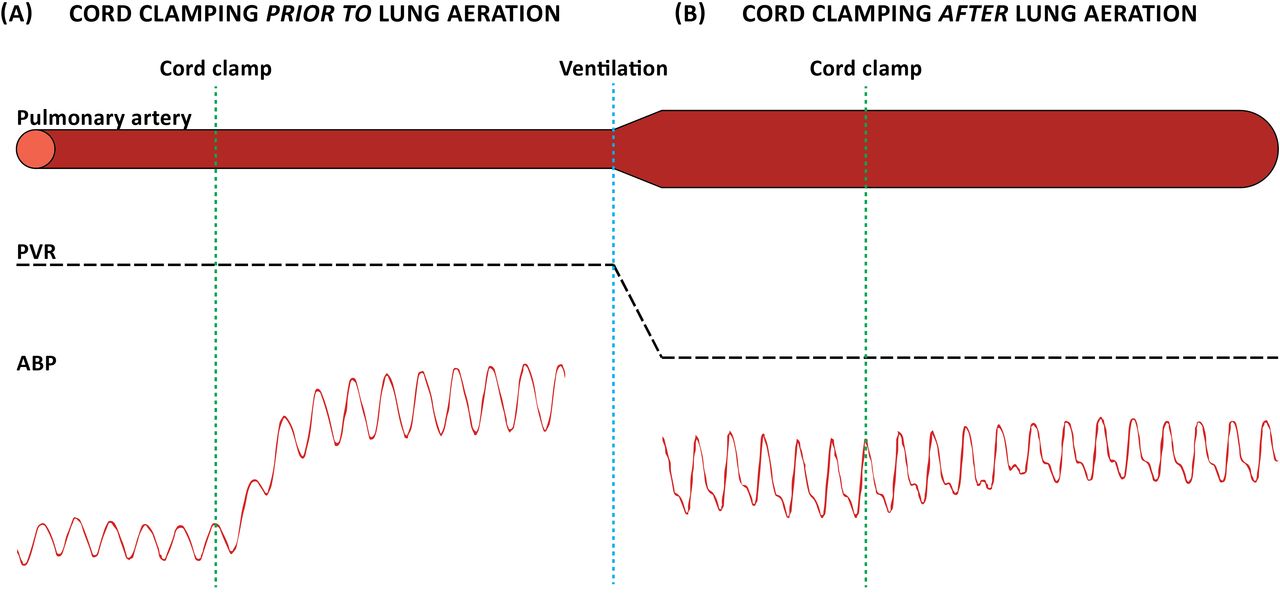
Fetal-to-neonatal transition in congenital diaphragmatic hernia. (A) Clamping the umbilical cord prior to lung aeration has been established and, thus, prior to the pulmonary vascular resistance (PVR) has decreased, increases the arterial blood pressure (ABP, afterload) and decreases the preload to the left ventricle. As a result, the cardiac output decreases. (B) Clamping the umbilical cord after lung aeration has been established and, thus, after the PVR has decreased, will result in a more stable transition. In that case, the left ventricular afterload and preload remain stable.
Two recent feasibility studies described the concept of initiating respiratory support prior to cord clamping in infants with a CDH.24 25 Both studies confirmed that this approach was feasible and had promising effects on the cardiovascular adaptation in the first hours after birth, although neither studies were powered to detect differences in outcomes.24 25 Hence, the logical next step is a randomised clinical trial to determine the true benefit of PBCC for infants with a CDH.26 We hypothesise that implementing a non-invasive intervention (such as PBCC) during the perinatal stabilisation period avoids initial high pulmonary perfusion pressures that initiate a vasoreactive response, thereby reducing the risk of pulmonary hypertension. The primary aim of this study is to investigate if the implementation of PBCC in the stabilisation period of infants born with a CDH reduces the incidence of pulmonary hypertension in the first 24 hours after birth, a clinically relevant outcome in these infants. The secondary aim of this study is to perform real-time monitoring of physiological parameters, which will improve our understanding of the physiological changes occurring during the perinatal stabilisation period in this population of infants.
Methods and analysis
Study design
The PBCC in CDH (PinC) trial is an international randomised controlled trial, that will be conducted in multiple academical centres in Europe and Australia. Infants will be randomised to either PBCC or immediate cord clamping (figure 2), whereas ongoing management will be according to a consensus-based postnatal management protocol.19

Trial flow chart. The flow chart depicts the steps from the screening of a subject until the evaluation of the primary outcome of the trial. CDH, congenital diaphragmatic hernia.
Patient and public involvement
Patients were not involved in the design of this study.
Patient population
We will include infants diagnosed with an isolated left-sided CDH on prenatal ultrasound with gestational age at delivery ≥35.0 weeks. Exclusion criteria are right-sided and bilateral CDH, antenatal diagnosed major associated structural or genetic abnormalities, high urgency caesarean section (intended interval to delivery <15 min), cases that have been treated during pregnancy with experimental drug therapy aiming to decrease the occurrence of pulmonary hypertension, twin pregnancies in which the infant diagnosed with a CDH is born first, multiple birth >2, and placental abnormalities (anterior placenta praevia, placental abruption).
Randomisation
Participants will be randomised using Castor electronic data capture (EDC), an EDC system that uses a computer-generated randomisation list and, thus, ensures concealment of allocation. Infants will be randomised 1:1 to either PBCC or the current standard approach of immediate cord clamping. Allocation will be stratified by predicted lung size (determined by observed/expected lung-to-head ratio and liver position, graded as mild/moderate/severe lung hypoplasia, measured between 20 and 26 weeks or at the initial visit) and by treatment centre, using variable random permutated block sizes (4–8).27
Study procedures
Providing adequate respiratory support immediately after birth while performing PBCC requires a resuscitation table near the mother. To facilitate this approach, several trolleys have been developed and we will preferably use the Concord Birth Trolley (Concord Neonatal B.V., Leiden, The Netherlands). This trolley was purpose-built for PBCC and has shown excellent feasibility in preterm infants.28 The trolley is fully equipped for stabilisation of infants with a CDH. In all infants, we will use a monitor that records vital parameters during stabilisation. Prior to the start of the study, all caregivers involved in delivery room care will be trained using the Concord.
In PBCC, the Concord will be placed next to the bed of the mother and all equipment will be checked before the second stage of labour has started (figure 3). The infant will be placed on the platform of the Concord immediately after birth, avoiding any traction or pressure on the cord and avoiding heat loss by radiation heating. The umbilical cord will not be clamped until the infant is considered respiratory stable, which is defined as the presence of a heart rate >100 bpm and preductal oxygen saturation >85%, while using a fraction of inspired oxygen of <0.5. Oxytocin administration will be postponed until after cord clamping if there are no obstetric concerns. To both guarantee an optimal placental-to-fetal transfusion as well as avoid excessive maternal blood loss, the minimum and maximum times of cord clamping are three and ten minutes after birth, respectively.29 At any time, the attending neonatologist and obstetrician can decide that PBCC should not be performed or be interrupted. In that case, the infant can be placed on the standard resuscitation table for (further) stabilisation. In this trial, physicians cannot be blinded to treatment allocation. However, we believe that the lack of blinding will not lead to deviations from the intended intervention, hence the influence on the primary outcome will be limited. In the immediate cord clamping group, the cord will be clamped immediately after birth. The infant will then be transferred to the standard neonatal resuscitation table. Thermomanagement during stabilisation is an important focus in both groups since hypothermia is a known trigger for pulmonary hypertension. Normal precautions will be taken to prevent heat loss, such as dry towels, caps, and a radiant warmer. After cord clamping, all infants will be managed according to the standardised neonatal management protocol for infants with a CDH, which is a consensus of current clinical guidelines by the CDH EURO consortium.19 A 2D echocardiography will be performed within the first 24 hours of life to evaluate the presence or absence of pulmonary hypertension.

{kind=link}
{kind=link}
{kind=link}
Position of the Concord birth trolley. The Concord birth trolley is positioned at the left side of the mother. The infant is then stabilised while the umbilical cord is still intact. The Concord birth trolley is fully equipped for stabilisation of infants that are born with a congenital diaphragmatic hernia.
This trial provides the unique possibility of collecting umbilical cord blood samples from a significant number of infants with a CDH that will have been randomised for two different stabilisation methods. We speculate that the physiological changes during the stabilisation period could trigger the release of biomarkers, such as free oxygen radicals, iron/hepcidin and metabolomics. Free oxygen radicals stimulate pulmonary vasoconstriction and could thus contribute to the occurrence and therapy-resistance of pulmonary hypertension.30 These biomolecules also induce lipid peroxidation modifying certain metabolic pathways, such as the endocannabinoid metabolism. Endocannabinoids are an interesting target for further analysis because of their involvement in supporting the fetal-to-neonatal transition.31 A second promising pathway is iron homeostasis, in particular the regulatory protein hepcidin. Iron-deficiency seems to alter smooth muscle cell activity, influence pulmonary vascular function, and, thus, contribute to the severity of pulmonary hypertension.32 Hepcidin treatment in rats with pulmonary hypertension resulted in a decrease in right ventricular systolic pressure and mean pulmonary arterial pressure, and with that in a decrease in pulmonary lesions induced by pulmonary hypertension.33 In this trial, samples will be collected and stored in a Biobank in the Erasmus MC. Cord blood will be analysed to detect relevant biomarkers in the prediction of postnatal outcomes. The above-mentioned biomarkers could eventually be used as early predictors of both short- and long-term outcomes, thereby allowing early interventions, individualised treatments, and specialised package of care.
Primary and secondary outcomes
The primary study outcome is pulmonary hypertension diagnosed in the first 24 hours after birth combining clinical and echocardiographic parameters (table 1). As the physician assessing the echocardiogram cannot be blinded to the intervention in all centres, we will collect the following echocardiographic parameters to guarantee objective evaluation of the presence or absence of the echocardiographic parameters: right ventricular systolic pressure, right ventricular size, pulmonary artery acceleration time (PAAT), right ventricular ejection time (RVET), PAAT:RVET ratio, intraventricular septum configuration, left ventricular end-systolic eccentricity index, tricuspid regurgitation, peak velocity of tricuspid regurgitation, tricuspid annular plane systolic excursion, transductal shunting direction, interatrial shunting direction, and right ventricular systolic to diastolic duration ratio.34
Primary outcome
Secondary outcomes that will be reported in the total population:
Maternal blood loss during delivery, estimated using the volume in the suction device and on the surgical swabs.
Time interval between birth and start respiratory support.
Apgar scores.
Umbilical cord pH.
Temperature at admission to the intensive care unit.
Respiratory support during resuscitation.
Mortality.
Secondary outcomes that will be reported in the total population and in the subgroup of survivors separately:
Presence of pulmonary hypertension requiring therapy on day 7, 14, 21, 28, and at discharge.
Treatment for pulmonary hypertension.
Use of inotropes and fluid therapy.
Presence of early-onset and late-onset sepsis.
Surgical characteristics.
Presence of hyperbilirubinaemia requiring therapy.
Presence of neurological complications.
Respiratory support during hospitalisation.
Presence and severity of bronchopulmonary dysplasia.
Number of days on the intensive care unit.
Postpartum haemorrhage is considered a safety parameter, because PBCC will result in later cord clamping times than are currently used for infants with a CDH.
Data collection
All outcome variables will be collected by local physicians and will be entered in a password protected online database (Castor EDC). Data access will be granted to the principal investigators of all participating centres. On request the collected data will be available.
Informed consent
Informed consent will be obtained before birth and the procedure will be explained to the parents by the investigators during a specific antenatal counselling session, followed by a time of reflection for the parents.
Data and safety monitoring
The data and safety monitoring board will conduct two interim statistical analyses on safety during the course of this study, after approximately 25% and 50% of the total required patients have completed their primary outcome. The only stopping condition will be concerns regarding safety outcomes. The safety analysis will include, but will not be restricted to, serious adverse events and the context-specific safety outcomes listed as secondary outcomes (bronchopulmonary dysplasia, sepsis, cerebral complications, need for extracorporeal membrane oxygenation). An annual safety report of all context-specific serious adverse events will be presented to the data and safety monitoring board and approving ethics committee. All other serious adverse events will be reported to the approving ethics committee in accordance with their guidelines.
Sample size estimates
The background incidence of pulmonary hypertension in infants with a CDH can be estimated based on historical cohorts. The largest registry available is the CDH Study Group registry consisting of data from 70 participating centres in 13 countries. A recent review of 3367 patients of this cohort (2007–2014) reports a 69.7% incidence of pulmonary hypertension in the first week after birth (median of 0 days (0–8)).35 As this is the first human clinical study evaluating PBCC with pulmonary hypertension as primary outcome, we cannot estimate the effect size. Thus, we suggest using a clinically relevant change in incidence of pulmonary hypertension to determine the sample size. We consider that a relative decrease by one-third in the incidence of pulmonary hypertension in the first 24 hours after birth is realistic and is significant enough to influence change in the neonatal management of infants with a CDH. Based on the background incidence of pulmonary hypertension, we calculated that at least 140 infants (70 in each group) are needed to detect a 1/3 reduction, with 80% power and 0.05 significance level. It will be difficult to estimate the number of cases that will have the umbilical cord clamped earlier than the times within the PBCC protocol. However, based on the results from two small human feasibility studies, it can be expected that we will have good overall adherence to the protocol.
Statistical analyses
The effect of PBCC on the primary outcome (pulmonary hypertension) will be analysed in the intention-to-treat population. The intention-to-treat population is defined as all patients that were randomised to a particular treatment arm, independent of protocol deviations. The effect will be analysed using multivariable logistic regression analysis with pulmonary hypertension as dependent variable and treatment allocation, severity of pulmonary hypoplasia, and treatment centre as independent variables. Per protocol analysis for the primary outcome will be employed as secondary analysis. The per protocol population is defined as all randomised patients who completed the protocol for the arm they were assigned to, had the primary endpoint measured, and had no major protocol violations.
The primary analysis will be a complete case analysis. By protocol, the independent variables in this multivariable analysis will be present in all cases. The dependent outcome could however be missing in the rare event that evaluation has not been performed in the first 24 hours after birth. We will perform a sensitivity analysis by imputing missing values in the primary outcome by using the ‘worst case’ observed in cases in which the primary outcome was assessed.
If more than 20% of values on a secondary outcome are missing, we will remove that variable from analyses. If no more than 20% of a secondary outcome are missing, we will use multiple imputation to deal with the missing data. Additionally, we will perform a sensitivity analysis by replacing missing values with the ‘worst case’ observed in patients with available data. For secondary outcomes we will calculate risk ratios or ORs with 95% CIs.
All data will be tested for normality using a Shapiro-Wilk test. Normally distributed data will be presented as mean±SD, not-normally distributed data as medians (IQRs). Statistical significance is set at p<0.05, using two-sided tests. Statistical analyses will be performed using the computing environment R (R Core Team (2020), Vienna, Austria).
Ethics and dissemination
Central ethical approval was obtained from the Medical Ethical Committee of the Erasmus MC, Rotterdam, The Netherlands (METC 2019-0414). Local ethical approval was obtained from the ethical committees of the University Hospital of Graz, Austria; the Radboudumc University Medical Centre, Nijmegen, the Netherlands; Monash Health, Clayton, Australia; University Hospitals Leuven, Belgium. The study is in the final stage of the review process by the ethical committees of the University of Bonn, Germany, and the University Medical Centre Mannheim, Germany. The study will be conducted according to the principles of the Declaration of Helsinki and international rules and regulations on personal data protection. The results of this study will be disseminated via peer-reviewed publications.
Trial status
Currently five university medical centres are enrolling patients. The first patient was included on 11 May 2020, and by 8 March 2022, 24 patients had been included. In 2022, two additional international centres will be added. Final inclusion is expected in 2023. The current article is based on protocol V.1.5 (15 March 2021).
Ethics statements
Patient consent for publication
References
Footnotes
Correction notice This article has been corrected since it first published. Author 'Marijn J Vermeulen' has been added in the author byilne.
Contributors PLJD, EJJH-O and MJV wrote the first draft of the study protocol. RK, MJV, ABtP, SBH, SCMC-dO, RMHW, KJC, NR, TS, WPdB, AD, BU, CTR, FK and IKMR participated in critical revision of the protocol. EJJH-O and PLJD drafted the manuscript. RK, MJV, ABtP, SBH, SCMC-dO, RMHW, KJC, NR, TS, WPdB, AD, BU, CTR, FK and IKMR reviewed and edited the manuscript. All authors approved the final manuscript as submitted and agreed to be accountable for all aspects of the work.
Funding This trial is supported by grants from Sophia Children’s Hospital Foundation (SSWO, grant S19-12 and CAM20-11).
Disclaimer This funding source did not have any further role in the writing of the protocol or the decision to submit it for publication.
Competing interests ABtP and SBH are members of the advisory committee of Concord Neonatal B.V. However, the authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.