Article Text

Abstract
Objectives Addressing the barriers to early breast and cervical cancer diagnosis in low and middle-income countries (LMICs) requires a sound understanding and accurate assessment of diagnostic timeliness. This review aimed to map the current evidence on the time to breast and cervical cancer diagnosis and associated factors in LMICs.
Design Scoping review.
Sources MEDLINE (via PubMed), Cochrane Library, Scopus and CINAHL.
Eligibility criteria Studies describing the time to diagnosis and associated factors in the context of breast and cervical cancer in LMICs published from 1 January 2010 to 20 May 2021.
Study selection and data synthesis Two reviewers independently screened all abstracts and full texts using predefined inclusion criteria. The review was reported in accordance with the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews. Evidence was narratively synthesised using predefined themes.
Results Twenty-six studies conducted across 24 LMICs were included in the review, most (24/26) of which focused on breast cancer. Studies varied considerably in their conceptualisation and assessment of diagnostic time, events, intervals and delays, with a minority of the studies reporting the use of validated methods and tools. Patient-related intervals and delays were more frequently evaluated and reported than provider-related and health system-related intervals and delays. Across studies, there were variations in the estimated lengths of the appraisal, help-seeking, patient and diagnostic intervals for both cancers and the factors associated with them.
Conclusions Despite the significant burden of breast and cervical cancer in LMICs, there is limited information on the timeliness of diagnosis of these cancers. Major limitations included variations in conceptualisation and assessment of diagnostic events and intervals. These underscore the need for the use of validated and standardised tools, to improve accuracy and translation of findings to better inform interventions for addressing diagnostic delays in LMICs.
- breast tumours
- public health
- quality in health care
- diagnostic radiology
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This scoping review was conducted in accordance with an enhanced evidence synthesis methodology and reported using standard reporting guidelines.
This review updates the evidence base relating to the nature of the time to diagnosis of breast and cervical cancer and associated factors in low and middle-income countries.
Literature searches were comprehensive, covering both peer-reviewed and relevant grey literature.
Due to the broad nature of the topic, it is possible that not all relevant evidence sources were identified by the search strategy, however comprehensive.
Introduction
Breast and cervical cancer constitute a growing public health burden globally.1 2 The incidence, morbidity and mortality burdens of both cancers are disproportionately high among women in low and middle-income countries (LMICs).2 3 Breast cancer is the most commonly occurring cancer and the leading cause of cancer deaths among women worldwide, with an age-standardised incidence rate (ASIR) of 31 per 1 00 000 women in LMICs.4 5 Cervical cancer is the fourth most common cancer among women, with an ASIR of 16 per 1 00 000 women.2 Cancer survival rates are low in LMICs, the major attributable factors of which include late-stage diagnosis and suboptimal access to quality healthcare.1 6
Timely diagnosis is critical for optimising patients’ navigation of the pathway from cancer symptom awareness to treatment, and improving survival.7–9 However, the majority of breast and cervical cancers are diagnosed at a late stage when treatment is often less effective and more expensive.10–12 In LMICs, barriers to timely cancer diagnosis include individual and disease-related factors as well as health system constraints.13–15 Individual-level factors may include demographic, behavioural and psychosocial factors, in addition to those associated with underlying sociocultural barriers to timely diagnosis, such as lay beliefs that cancers are contagious and that they are inevitably fatal.16 17 Disease-related factors include those related to the site, size, clinical manifestation and growth of tumours.15 Health system factors in LMICs include health policy, access, quality and service delivery barriers, such as inadequate diagnostic capacity, weak referral systems, supoptimal access to treatment and insufficient human resources.6 18 19 While there is substantial evidence on the association between these factors and cancer diagnostic delays, not much is known about the extent to which they influence time to diagnosis and diagnostic intervals, particularly in LMICs.
Various approaches and tools have been used for assessing time to diagnosis and diagnostic intervals, while their use in LMICs has grown over the years.17 19 20 However, the tools commonly used often ignore existing models of patient behaviour and are poorly or inadequately validated.15 21 22 To bolster better conceptual understanding of patient’s navigation, Walter, Scott and colleagues proposed a Model of Pathways to Treatment that describes the distinct phases of cancer patients’ pathways from symptom awareness to diagnosis and treatment.15 22 To aid the development of valid tools for measuring time to cancer diagnosis, the Aarhus checklist has been proposed for guiding the design and reporting of early cancer diagnosis studies.23
A good understanding of the timeliness of breast or cervical cancer diagnosis, the diagnostic intervals and associated factors is important to guide interventions for addressing the growing public health problem of diagnostic delays in LMICs.24–26 In 2017, the WHO published the WHO Guide to Cancer Early Diagnosis to provide a global standard for addressing barriers that may impede timely cancer diagnosis and treatment.27 28 Addressing these barriers requires an accurate assessment and understanding of the time to diagnosis, related intervals and the multidimensional factors associated with the timeliness of diagnosis.28
This review aims to provide an updated and comprehensive synthesis of the evidence on the time to diagnosis and its associated factors, in the context of symptomatic breast and cervical cancer diagnosis in LMICs. It contributes a systematically organised evidence summary for health policymakers, cancer programme managers, oncologists and other cancer care providers for guiding policy and practice decision-making. In addition, the findings will be useful for informing the design of interventions and strategies for addressing existing breast and cervical cancer diagnostic delays in resource-limited settings, while identifying gaps for future research efforts at measuring and appraising diagnostic timeliness.
Methods and analysis
Conceptual framework
This scoping review used the Model of Pathways to Treatment to map the identified evidence on the timeliness, time intervals and associated factors of breast and cervical cancer diagnosis.15 22 The framework specifies the essential events, processes and time intervals that may occur in the period prior to diagnosis and the start of medical treatment and identifies the factors that may influence each interval.
Study design
The design of this study was guided by Arksey and O'Malley’s scoping review methodology,29 as enhanced by Levac and colleagues.30 The enhanced framework involves six stages for undertaking a scoping review: (1) identifying the research question, (2) identifying the relevant studies (defining the inclusion and exclusion criteria), (3) searching and selecting the evidence, (4) charting the evidence, (5) collating, summarising and reporting the evidence and (6) consultation with relevant stakeholders. The review was reported in accordance with the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews.31 Full details of the study design have been published elsewhere.32
Data sources
The literature search was guided by the review objectives and the population, concept and content (PCC) criteria. The search strategy was developed with guidance from a health sciences subject librarian and applied in accordance with the Peer Review of Electronic Search Strategies guidelines.33 The search strategy was pretested prior to the actual search. Search terms and free-text words were combined using the Boolean operators ‘AND’ and ‘OR’. Search terms included the use of controlled descriptors (such as MeSH terms, CINAHL and headings) and their synonyms. In order to restrict search to LMICs, a location filter containing all countries currently classified as part of LMICs and synonymous geographical, regional and economic categorisations were incorporated. The search strategy, as applied to the various literature databases, is outlined in the online supplemental appendix. More details of the search strategy are described in the review protocol published elsewhere.32
Supplemental material
A comprehensive literature search was conducted on the following electronic databases: MEDLINE (via PubMed), Cochrane Library (including the Cochrane Central Register of Controlled Trials (CENTRAL) and the Database of Abstracts of Reviews of Effects (DARE)), Scopus, CINAHL and the International Clinical Trials Registry Platform (ICTRP). Additionally, relevant grey literature sources were searched for potentially eligible articles, including the publication database of the WHO’s International Agency for Research on Cancer (IARC), the Cancer Atlas of the Union for International Cancer Control (UICC) and the Global Cancer Project Map. A hand-search of reference lists of included studies was conducted. For recency, only articles published from 1 January 2010 to the last date of search (20 May 2021) were considered eligible. No language restrictions were applied. Non-English potentially eligible articles would have been translated using a Web-based translation tool.34
Eligibility criteria
Inclusion criteria were defined using the PCC framework, proposed by Peters and colleagues.35 Eligible population included women with breast or cervical cancer and healthcare providers (HCP) in LMIC contexts. The definition of LMICs was based on the World Bank’s current classification using per capita gross national income.36 The concepts of interest were time to diagnosis and diagnostic intervals of breast and/or cervical cancers. To be considered eligible for inclusion, studies need to have measured time to diagnosis in the context of breast and/or cervical cancer diagnosis in LMICs, using specific methods, tools or strategies; and/or assessed diagnostic intervals of breast and/or cervical cancers; whether or not they evaluated the factors associated with diagnostic time or time intervals. Multinational literature involving LMIC and non-LMIC countries and meeting inclusion criteria were eligible for inclusion, except where country-specific information could not be abstracted. Similarly, articles involving multiple cancer types were eligible for inclusion, except relevant cancer type-specific information could not be abstracted.
Articles focused solely or mainly on theoretical and conceptual understanding of timeliness of breast or cervical cancer diagnosis were excluded, as were those assessing cancer patient pathways that are not related to diagnostic time and intervals. Studies focused primarily on screening of asymptomatic individuals were also excluded. Study design eligibility included randomised trials, non-randomised trials and observational studies, with or without controls. Only primary studies were included, while systematic, scoping reviews and other forms of aggregated evidence were excluded.
Study selection
The review process consisted of two levels of screening. For the first level of screening, two reviewers (CAN and PK) independently screened the titles and abstracts of all retrieved records from the search output. Articles considered relevant by either or both of the reviewers were included in the full-text assessment. Following the removal of duplicates, full texts of remaining studies were retrieved. In the second step, the two reviewers (CAN and EFE) independently assessed the full-texts to determine whether they met the inclusion/exclusion criteria. Disagreements in eligibility assessment were resolved through consensus between.
Data extraction
Two reviewers (CAN and EFE) independently abstracted data from all included studies using a standardised data abstraction tool, adapted from the framework proposed by Carlos and colleagues.37 The tool includes four domains: (1) study identification details (article title, journal title, authors, country of the study, language, publication year, host institution of the study), (2) methodological characteristics (study design, study objective or research question or hypothesis, sample characteristics (eg, sample size, sex, age, ethnicity, groups and controls, follow-up duration, validation of measures, statistical analyses), (3) main findings and (4) conclusions. Study eligibility was reverified at the start of/during data extraction. Any discrepancies in the abstracted data between the two reviewers were resolved by discussion. CAN combined the two spreadsheets of abstracted data for analysis. JM and FMW reviewed analysed data for accuracy and consistency with protocol.
Data analysis
Findings were narratively summarised and reported based on themes that emerged from the charted evidence. Where applicable, quantitative evidence was aggregated using summary statistics. Time to diagnosis and diagnostic intervals were described based on the Model of Pathways to Treatment.15 22 The Model also allowed for the assessment of patient; HCP and health system and disease-related factors that could influence diagnostic timeliness.
Patient and public involvement
Patients or the public were not involved in this research.
Results
Search results
A total of 10 591 records were identified from literature database searches. After the removal of duplicates, there were 9347 unique records. These were screened by their titles and abstracts, following which 9174 clearly ineligible publications were excluded. The full texts of the remaining 173 potentially eligible studies were reviewed against predefined inclusion and exclusion criteria; 26 of which were included in the review, while 147 were excluded for various reasons. Figure 1 presents the PRISMA flowchart of the study selection process and reasons for exclusion.
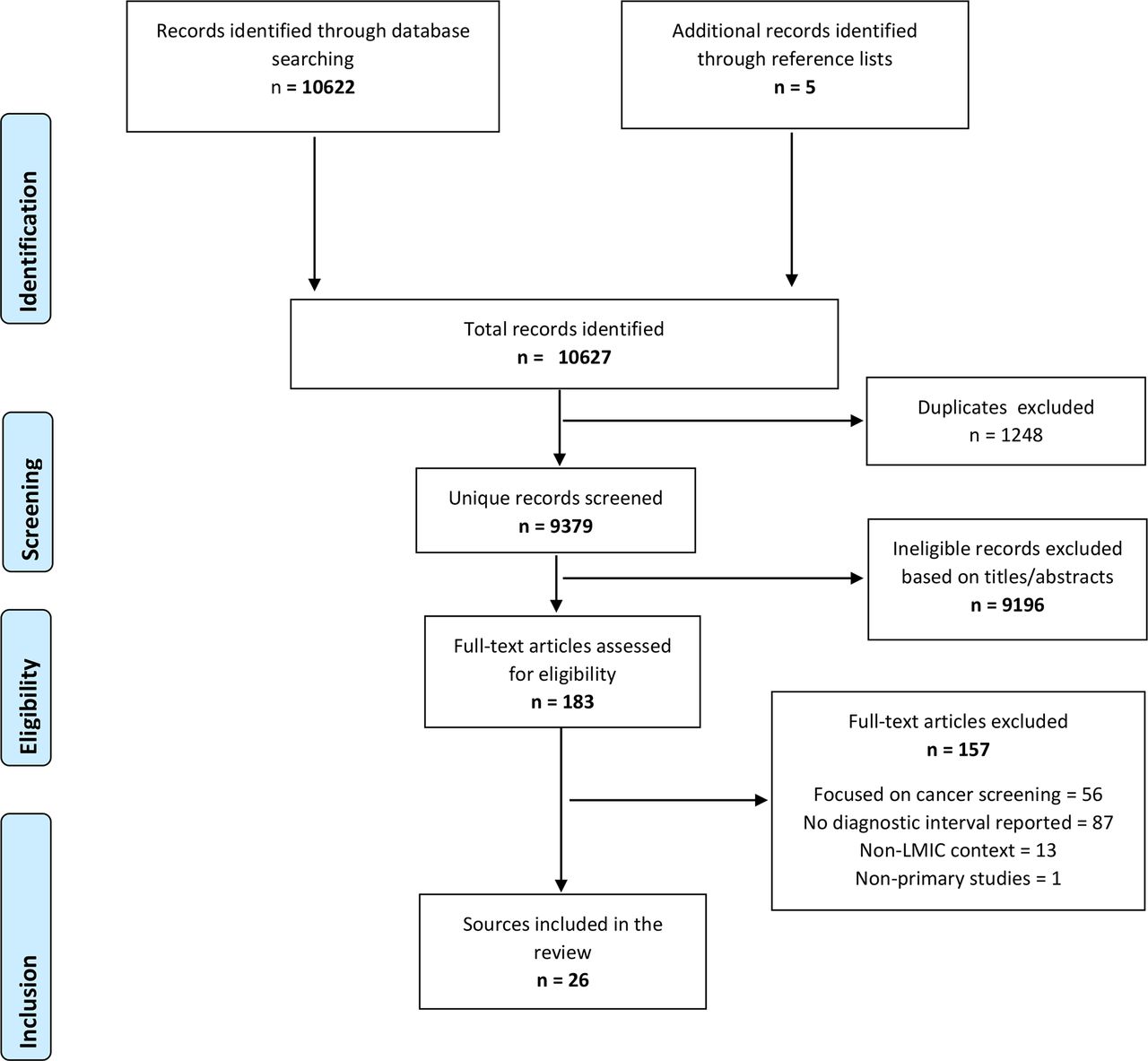
PRISMA flowchart of the study selection process. LMICs, low and middle-income countries; PRISMA, Preferred Reporting Items for Systematic reviews and Meta-Analyses.
Characteristics of included studies
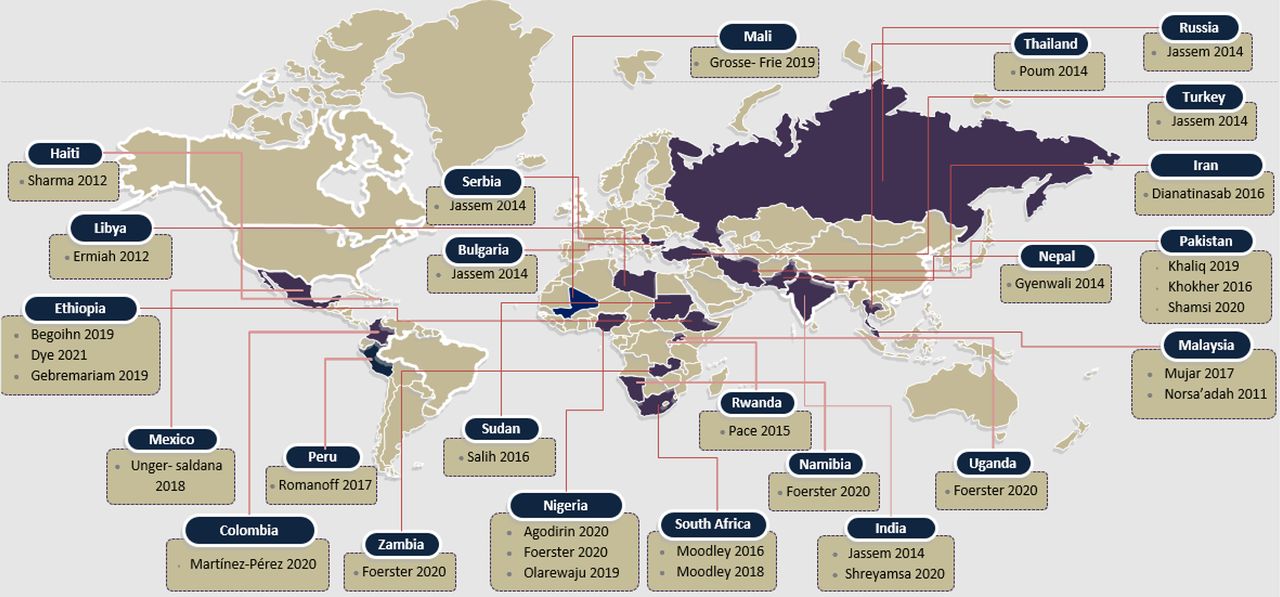
Online supplemental table 1 describes the characteristics of included studies. Most (24/26) of the studies were focused on breast cancer, with only two focusing on cervical cancer. The studies were published between 2011 and 2020, conducted across 24 LMICs across the regions of Africa, Europe, Latin America, Middle-East Asia and South-East Asia. The following countries (number of studies) were represented: Bulgaria (1), Colombia (1), Ethiopia (3), Haiti (1), India (2), Iran (1), Libya (1), Malaysia (2), Mali (1), Mexico (1), Namibia (1), Nepal (1), Nigeria (3), Peru (1), Pakistan (3), Russia (1), Rwanda (1), Serbia (1), South Africa (2), Sudan (1), Thailand (1), Turkey (1), Uganda (1) and Zambia (1). Figure 2 illustrates the geographical distribution of included studies.
Supplemental material
{kind=link}
{kind=link}
Geographical distribution of included studies.
Nearly, all (24/26) of the studies included were quantitative in design, including cross-sectional (21), cohort-type longitudinal (2) and case–control (1) studies. One study had a mixed-methods cross-sectional design, while another was a qualitative study. Most (24/26) of studies primarily focused on breast cancer, whereas the remaining two focused on cervical cancer. Participants were mostly adult women with newly diagnosed breast or cervical cancer. All of the studies were conducted within healthcare settings, of which 18 were urban, 3 were rural and 5 were both rural and urban.
Methods of diagnosis
In the majority (20/26) of the studies, diagnosis was defined based on pathological or histological confirmation.7 18 19 38–54 The rest of the studies relied on clinical assessment as a diagnostic modality.55–60
Methods/tools used for assessing diagnostic timeliness and intervals
Online supplemental table 1 describes the various methods and tools used for assessing diagnostic timeliness and intervals across studies. In most (23/26) of the studies, diagnostic events, timeliness and intervals were assessed using questionnaires or interviews that relied on participants’ recall,7 18 19 38–56 59 seven of which combined patients’ reports obtained from questionnaires or interviews with diagnostic information derived from facility-based medical records.40 43 50 52–54 59 Three studies assessed diagnostic events and intervals using medical records.38 57 60
To define diagnostic time and intervals, 14 studies relied on authors’ definition18 38–41 44 45 49 52–54 57 59 while four adopted definitions from previous studies.47 50 51 56 Four studies adopted the Model of Pathways to Treatment,7 19 43 55 three studies adopted the Aarhus Statement,42 46 55 while two studies adopted the Anderson Model.48 58
The studies varied considerably in the use of common terminologies relating to diagnostic events and intervals. Only two studies defined the appraisal interval (time between discovery of symptoms and perceiving reasons to seek help) and help-seeking interval (time between symptom recognition and first HCP consultation) as separate intervals as defined by the Model of Pathways to Treatment.7 55 Most other studies combined both appraisal and help-seeking intervals as a single interval (time between symptom recognition and first HCP visit/consultation). Varying terminologies were used across studies to refer to this single interval, including help-seeking interval,43 55 patient (-related) interval (also patient delay or patient time),7 18 42 44–47 49–54 58 59 time to action,56 precontact time,41 consultation time40 48 and presentation interval.60 Table 1 describes how diagnostic timeliness and intervals were defined across studies.
Diagnostic timeliness and intervals as assessed by included studies
Diagnostic interval was defined in various ways across studies: the time commencing from the point of symptom detection to diagnosis,40 48 57 time from first clinical consultation to diagnosis7 18 19 41 42 44 47 49 50 52 54 and time from first presentation at a diagnostic centre to diagnosis.46 Notably, the diagnostic interval was also referred to as primary care interval (time between first HCP visit and first specialist visit).44 46 55 Less than half (10/26) of the studies defined total diagnostic interval (time from symptom detection to diagnosis).19 38–41 44 47 48 50 55
Similarly, the thresholds for defining intervals as delayed also varied across studies. Notably, a patient interval was considered as delayed if longer than 2 months in one study,44 whereas two other studies considered it as delayed if longer than 3 months.49 53 Likewise, a diagnostic interval was considered as delayed if longer than 7 days44 but considered as delayed if longer than 1 month53 and longer than 2 months49 in other studies.
Breast cancer intervals
Appraisal and help-seeking intervals as separate intervals
Only one study assessed appraisal interval (between the detection of breast symptoms to first disclosure, eg, to partners, family and friends) and help-seeking interval (between symptom detection and first HCP visit) as separate intervals.55 The study found a median appraisal interval of 6 days (approximately 1 week) and a median help-seeking interval of 6 weeks among women (N=420) with breast cancer in Nigeria.
Patient interval (combination of appraisal and help-seeking intervals)
In most (22/24) of the studies focusing on breast cancer, appraisal and help-seeking intervals were assessed together as a single ‘patient interval’ or ‘time to action’ (between the detection of breast symptoms and first HCP visit). The interval ranged from 10 days among breast cancer patients in Mexico (N=886)52 to 2 weeks in Thailand (N=180)18; 3 weeks in Colombia (N=242)47 and South Africa (N=201)7; 4 weeks in Ethiopia (N=441)42; 8 weeks in Malaysia (N=328)48; 10 weeks in Malaysia (N=340)54; 16 weeks in India (N=435)53 and Libya (N=200)40; 19 weeks in Mali (N=124)43; 20 weeks in Rwanda (N=144)50; 23 weeks in South Africa (N=20)19; 28 weeks in Peru (N=113)51; 48 weeks in Sudan (N=63)58; 63 weeks in Pakistan (N=449)59 and 81 weeks in Ethiopia (N=55).56 One multicountry study (N=1429) assessed patient intervals for Namibia (1 week in non-black women and 5 weeks in Black women), Nigeria (15 weeks), Uganda (14 weeks) and Zambia (4 weeks).41 Another multi-country study (N=6588) reported patient intervals for Bulgaria (19 weeks), India (24 weeks), Russia (19 weeks), Serbia (18 weeks) and Turkey (19 weeks).45
Diagnostic interval
The majority (16/24) of the studies focusing on breast cancer measured diagnostic intervals (between the first HCP visit and diagnosis of breast cancer). The interval ranged from 3 weeks in Mali (N=124)43 and Thailand (N=180)18; to 4 weeks in South Africa (N=201)7 and Malaysia (N=340)54; 8 weeks in Colombia (N=242)47; 10 weeks in Ethiopia (N=441)42; 13 weeks in another South African study (N=20)19; 15 weeks in Nigeria (N=420)55; 18 weeks in Mexico (N=886)52; 20 weeks in Rwanda (N=144)50 and 22 weeks in Malaysia (N=328).48 One multicountry study (N=1429) assessed diagnostic intervals for Namibia (3 weeks in non-black women and 8 weeks in Black women), Nigeria (1 week), Uganda (19 weeks) and Zambia (10 weeks).41
Diagnostic endpoints varied across studies, with pathology (histology) being the most commonly used method, while a minority defined diagnosis based on clinical and/or radiological assessment.
Total diagnostic interval (combination of appraisal, help-seeking and diagnostic intervals)
A minority (7/24) breast cancer studies assessed total diagnostic interval (between the awareness of symptoms and diagnosis). This interval ranged from 15 weeks in Colombia (N=242)47; to 21 weeks in Iran (N=505)39; 30 weeks in Libya (N=200)40; 34 weeks in Nigeria (N=420)55; 36 weeks in South Africa (N=20)19; 60 weeks in Rwanda (N=144).50 One multicountry study (N=1429) reported total diagnostic intervals for Namibia (10 weeks in non-black women and 26 weeks in Black women), Nigeria (22 weeks), Uganda (45 weeks) and Zambia (33 weeks).41 Table 2 summarises the intervals.
Diagnostic intervals and factors associated with diagnostic timeliness
Cervical cancer intervals
Appraisal and help-seeking intervals as separate intervals
Neither of the two cervical studies assessed appraisal interval (between the detection of cervical symptoms to first disclosure, for example, to partners, family and friends) and help-seeking interval (between symptom detection and first HCP visit) as separate intervals.
Patient interval (combination of appraisal and help-seeking intervals)
One of the two cervical cancer studies assessed appraisal and help-seeking intervals together as a single ‘patient interval’ (between the detection of cervical symptoms and first HCP visit). It found a patient interval of 10 weeks among women (N=110) with cervical cancer in Nepal.44
Diagnostic interval
One cervical cancer study evaluated diagnostic intervals (between the first HCP visit and diagnosis). It found an interval of 8 weeks among women with cervical cancer in Nepal (N=110).44
Total diagnostic interval (combination of appraisal, help-seeking and diagnostic intervals)
Both cervical cancer studies assessed total diagnostic interval (between the awareness of symptoms and diagnosis). The interval was 22 weeks in a cohort of women in Nepal (N=110)44 and 30 weeks in Ethiopia (N=1575).38
Factors associated with diagnostic timeliness
Appraisal and health-seeking intervals
Online supplemental table 2 summarises the factors associated with diagnostic timeliness and interval lengths across studies. Women who reported the presence of a family history of breast cancer,59 women who reported the fear of breast cancer45 and those that initially visited private clinics/tertiary hospitals43 tended to have shorter help-seeking intervals. Also, being employed,45 receiving supports from family/friends,45 living in big cities,45 receiving correct advice,55 presence of a large tumor55 and worsening of, or development of new symptoms56 were associated with shorter health-seeking interval. Longer help-seeking intervals were associated with not practising self-breast examination,40 51 older age,40 42 50 not receiving a cervical examination at first consultation,44 living in rural areas or farther away from cities,38 52 having ≥5 children,42 low health literacy level,7 40 42 58–60 use of traditional/complementary medicine,42 50 54 59 lower socioeconomic status42 52 58 59 and living in denial.7 52 Higher family income,18 fear of high treatment cost,60 self-medication,18 non-disclosure52 and seeking medical advice from family or friends18 were also associated with longer help-seeking intervals.
Diagnostic interval
Shorter diagnostic delay was associated with higher educational level,39 urban residence,39 ability to conduct self-breast examination39 and self-detection of lump.39 On the other hand, longer diagnostic interval was associated with wrong attribution of symptoms,41 48 low heath literacy,19 41 44 53 symptom denial,7 presence of comobidities,7 unemployment,18 46 lower socioeconomic status,41 52 53 older age,18 44 46 47 49 being unmarried,41 49 lay beliefs,41 residing far from a health facility41 44 53 and longer travel time.18 Other factors associated with longer diagnostic interval were lack of cervical examination at first consultation,44 seeking care from multiple health practitioners and complementary/alternative care before diagnosis,18 46 48 50 54 health-seeking in government subsidised facilities,47 referral delays,53 false-negative diagnosis48 53 and poor treatment behaviour.48 Notably, patients who initially visited private clinics/tertiary hospitals tended to have shorter help-seeking intervals but longer diagnostic delays.43
Discussion
Addressing the barriers to early diagnosis of breast and cervical cancer requires a sound understanding of diagnostic timeliness, intervals and delays and the factors associated with them. This review offers up-to-date evidence with which to bolster that understanding. Overall, it demonstrates that patient-related and health-system-related delays are common in LMICs. However, it is difficult to infer and compare findings across studies owing to variations in how diagnostic time, events, intervals and delays were conceptualised and assessed. While the amount of evidence identified points to the substantial and growing attention paid to early breast and cervical cancer in LMICs over the past decade, this review has also identified gaps both in terms of quantity and methodological diversity of the available literature.
The current evidence shows a dearth of studies evaluating the timeliness of cervical cancer diagnosis, with only two of such studies identified in this review (constituting <10% of studies found). This is despite the substantial burden of cervical cancer and late-stage diagnosis in LMICs.1–5 Consistent with finding from previous reviews of cancer diagnostic delays,10 61 a major methodological issue identified by this review is the marked variability in the conceptualisation and operationalisation of the time to diagnosis and corresponding intervals. In spite of the availability of validated tools and methods for evaluating cancer diagnostic timeliness, a minority of the studies reported the use of such tools in the context of breast and cervical cancer—including the Anderson model,48 58 the Model of Pathways to Treatment7 19 43 55 and the Aarhus Statement.42 46
The studies varied considerably in the use of common terminologies relating to diagnostic events and intervals. There were also variations in the thresholds used for defining delays. For instance, a patient interval was considered as delayed if longer than 2 months in one study,44 whereas two other studies considered it as delayed if longer than 3 months.49 53 Similarly, different time points were used to define intervals. For instance, the end point for diagnosis was operationalised as the date of diagnosis based on clinical or imaging evaluation in some studies, while it was the date of pathological diagnosis in others. It is, therefore, important to standardise methods of assessing and reporting of diagnostic end points, one approach of which are the European Network of Cancer Registries guidelines.62 The wide discrepancy between the estimated patient-related intervals of 4 weeks and 81 weeks among women with breast cancer in Ethiopia, as reported by two different studies,42 56 starkly reflects such within-country variations. These further complicate the interpretation and comparison of findings across studies.
Patient-related intervals and delays were more frequently evaluated and reported than provider-related and health system-related ones. This is consistent with the findings of a previous review on cancer diagnostic delays in LMICs.10 The trend may be a reflection of the patient-sided way in which diagnostic delays are currently perceived in LMICs and underscores the need for more balanced and system-wide approaches to assessing and understanding the barriers to early diagnosis of breast and cervical cancer diagnostic. It also has important implications for policy and practice. For instance, focusing on patient-centred strategies such as improving awareness, without addressing provider-related and health system-related factors, may yield limited results.
It is noteworthy that most of the studies that assessed and reported patient-related intervals did not evaluate the appraisal interval as a distinct form of patient-related interval, but rather assessed the appraisal and help-seeking intervals as a single interval. Only two studies made such distinction.7 55 This highlights the need for more attention to be paid to this interval among women with breast and cervical cancer symptoms as a distinct and important aspect of their journey from symptom awareness to treatment. To develop evidence-based policies and holistic interventions for addressing diagnostic delays and barriers to early cancer diagnosis in LMICs, it is imperative to understand the time and events that characterise patients’ journey from the perception of bodily changes to discerning the need and urgency to seek help, as these will ultimately influence time to diagnosis and treatment.
Our review also identified a multiplicity of patient and health system-related factors associated with diagnostic timeliness and delay across specific diagnostic intervals. While the factors influencing one interval (such as the help-seeking interval) might be distinct (at least empirically) from those affecting other intervals (such as the diagnostic or provider interval), this may not be so in practice as the length of each interval is likely to be the result of a complex interplay between patient and health system drivers. For instance, women may delay help-seeking not only due to patient‐related factors (such as having a low level of cancer awareness) but also due to health-system factors such as the non-availability of a health facility or HCPs.
Likewise, women with symptoms of cancer presenting at health facilities may delay definitive diagnosis following referral, due to fear of the consequences of being diagnosed with cancer (such as mastectomy, stigma and death). Hence, it is essential that these interrelationships are taken into consideration when conceptualising, evaluating and interpreting diagnostic intervals and the factors associated with them. We again emphasise the importance of standardising the assessment and reporting of cancer diagnostic intervals, to improve the translation of research findings and to better inform interventions for addressing the growing public health challenge of delayed breast and cervical cancer in resource-limited settings.
Limitations
While our review adds significantly to the existing body of literature on cancer diagnostic timeliness in LMIC contexts, it is not without limitations. First, as has been acknowledged earlier, the heterogeneous nature of the studies and the use of non-standardised methods limit the interpretation and comparability of findings. Besides, the small sample size and non-representativeness of participants of some of the studies limited both internal and external validity of the studies, making it difficult to interpret findings in the context of their reference geographic populations.
The cross-sectional retrospective nature of many of the studies and the reliance on patients’ recall to estimate events such as the time they first discovered their symptoms come with the risk of recall bias. These also come with the potential of social desirability bias that can lead to underestimation of patient and diagnostic delays. Another important limitation of this review is that, as in most scoping reviews, a formal quality appraisal of included literature was not conducted. As such, the strength of the evidence cannot be ascertained. Finally, while our literature search was comprehensive, it is possible that the review did not include all relevant literatures available, as some may not have been accessible at the time search.
Conclusions
Despite the significant burden of breast and cervical cancer in LMICs, there is limited evidence on the timeliness of diagnosis of both cancers. Available evidence demonstrates between-country and within-country variations in how diagnostic timeliness and intervals of breast and cervical cancer are conceptualised and measured in LMICs. Such variations underscore the need for the increased use of validated and standardised tools for assessing diagnostic timeliness in more reproducible and comparable ways to more accurately inform interventions for addressing the growing public health problem of diagnostic delays in LMICs.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
This study does not involve human participants.
Acknowledgments
The authors wish to thank Namhla Madini of the Faculty of Health Sciences Library, University of Cape Town, for the support and guidance in developing the literature search strategy.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @ChuxNesta_Nnaji
Contributors JM conceived the study, provided conceptual guidance for the design of the protocol and is the guarantor of the review. CAN wrote the first draft of the manuscript. PK, FMW and JM supported the refinement of the study protocol. CAN and PK performed literature search and study selection. CAN and EE conducted full text review, data extraction and analysis. JM and FMW provided critical insights and guided the coherence of the manuscript. All authors have contributed to, and approved, the final version of the manuscript.
Funding This research was jointly supported by the Cancer Association of South Africa (CANSA), the University of Cape Town and, the SA Medical Research Council with funds received from the SA National Department of Health, GlaxoSmithKline Africa Non-Communicable Disease Open Lab (via a supporting grant Project Number: 023) and the UK Medical Research Council (via the Newton Fund). Authors retained control of the final content of the publication. FW is the Director of the multi-institutional CanTest Collaborative, which is funded by Cancer Research UK (C8640/A23385).
Map disclaimer The depiction of boundaries on the map(s) in this article does not imply the expression of any opinion whatsoever on the part of BMJ (or any member of its group) concerning the legal status of any country, territory, jurisdiction or area or of its authorities. The map(s) are provided without any warranty of any kind, either express or implied.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.