Article Text

Abstract
Objective To document socioepidemiological theories used to explain the relationship between socioeconomic disadvantage and multimorbidity.
Design Scoping review.
Methods A search strategy was developed and then applied to multiple electronic databases including Medline, Embase, PsychInfo, Web of Science, Scielo, Applied Social Sciences, ERIC, Humanities Index and Sociological Abstracts. After the selection of studies, data were extracted using a data charting plan. The last search was performed on the 28 September 2021. Extracted data included: study design, country, population subgroups, measures of socioeconomic inequality, assessment of multimorbidity and conclusion on the association between socioeconomic variables and multimorbidity. Included studies were further assessed on their use of theory, type of theories used and context of application. Finally, we conducted a meta-narrative synthesis to summarise the results.
Results A total of 64 studies were included in the review. Of these, 33 papers included theories as explanations for the association between socioeconomic position and multimorbidity. Within this group, 16 explicitly stated those theories and five tested at least one theory. Behavioural theories (health behaviours) were the most frequently used, followed by materialist (access to health resources) and psychosocial (stress pathways) theories. Most studies used theories as post hoc explanations for their findings or for study rationale. Supportive evidence was found for the role of material, behavioural and life course theories in explaining the relationship between social inequalities and multimorbidity.
Conclusion Given the widely reported social inequalities in multimorbidity and its increasing public health burden, there is a critical gap in evidence on pathways from socioeconomic disadvantage to multimorbidity. Generating evidence of these pathways will guide the development of intervention and public policies to prevent multimorbidity among people living in social disadvantage. Material, behavioural and life course pathways can be targeted to reduce the negative effect of low socioeconomic position on multimorbidity.
- epidemiology
- public health
- social medicine
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This is the first scoping review exploring the use of theories to explain the association between socioeconomic position and multimorbidity.
Our review has identified critical gaps in the literature that must be addressed if interventions and public policies are to be designed to reduce socioeconomic inequalities in multimorbidity.
We applied a comprehensive search strategy to identify relevant articles and applied a peer-reviewed robust methodology to assess theories in studies on socioeconomic inequalities in multimorbidity.
Articles that were not in English were excluded from our review. This could have obstructed the inclusion of papers from countries where English is not the main language, therefore limiting the generalisability of our findings.
Introduction
Multimorbidity is a societal challenge and an increasingly recognised public health concern.1–3 It is described as the co-occurrence of two or more chronic conditions in an individual.4 Multimorbidity leads to reduced quality of life, high psychological distress, burden of polypharmacy and managing multiple treatment protocols, and an increased risk of premature death in people.5 There is an emerging threat of increased multimorbidity worldwide, primarily due to population ageing and the epidemiological transition from communicable to non-communicable diseases.6 The COVID-19 pandemic has put a spotlight on multimorbidity as people with existing chronic conditions have suffered a higher risk of its infection, as well as more severe consequences of SARS-CoV-2 infection.7 Furthermore, multiple studies have reported socioeconomic inequalities in multimorbidity within countries regardless of their level of economic development.8–12
A meta-analysis of 24 cross-sectional studies reported that low education compared with high education was associated with 64% higher odds of multimorbidity.13 Another systematic review with 41 studies from high-income countries reported that people with the lowest level of income had 4.4 times higher odds of multimorbidity than those with the highest level of income, while those in most deprived areas had 1.42 times higher odds of multimorbidity than those in the least deprived areas.14 A clear causal relationship between socioeconomic conditions and multimorbidity has also been argued based on empirical evidence;10 however, pathways through which socioeconomic disadvantage leads to multimorbidity are not well studied.4
Theories are used in epidemiology to understand the relationships between exposure to, for example, socioeconomic disadvantage and non-communicable diseases. This is mainly because, as opposed to conceptual frameworks, specific theoretical pathways can be tested using empirical data. Theories provide insight into the mechanisms through which an exposure (eg, socioeconomic position) leads to a health outcome,15 and as such, they are particularly helpful in informing intervention designs. Since the release of the Black Report in 1982,16 several categories of theories have been proposed to explain associations between social inequalities and health outcomes16 17 although in the context of single diseases or health measure. These include:
Behavioural: the behavioural explanation posits that people from different backgrounds behave differently and make health-related choices that are commonly based on their socioeconomic background. As people experience socioeconomic deprivation, they also encounter more barriers to adopting healthy lifestyles. For instance, individual health damaging and promoting behaviours are differentially distributed across the social scale, with more disadvantaged groups more likely to engage in health damaging behaviours such as smoking, and advantaged groups more likely to engage in health-promoting behaviours such as physical activity.18 As a result, poor health outcomes are commonly clustered at the lower end of the socioeconomic scale.17 Behavioural theory can be extended to apply to multimorbidity from a common risk factor approach, as a behavioural risk factor can cause multiple diseases (eg, smoking can cause cancer, asthma and cardiovascular diseases19 20).
Psychosocial: this theory postulates that the emotions that arise due to social inequality can directly affect biological health.17 This can be caused in two ways, either through the practice of health compromising behaviours or through biological changes due to the individual being in a sustained state of stress.17 Hence, the behavioural explanation can be a descendent of psychosocial processes under this explanation. The perceived lack of control and psychosocial stress may lead to adverse health behaviours and may activate neuroendocrine mechanisms, and in doing so, may affect multiple body systems and lead to multimorbidity.
Materialist: the material environment has a significant impact on the health of an individual. Exposure to health risk or health protective factors varies according to socioeconomic position due to differential access to material resources; differences are more evident in non-egalitarian societies. For instance, individuals living in socioeconomic disadvantage are less likely to be able to access information and resources necessary to maintain good health compared with their more advantaged counterparts.17 Socioeconomically deprived individuals are also more likely to be exposed to hazardous working environments.17 The materialist theory proposes these explanations as pathways between socioeconomic deprivation and health inequalities.17 Lack of material resources such as inadequate housing, for example, can lead to multimorbidity by causing depression as well as respiratory illnesses such as asthma.
Social support: this theory holds that positive social support mitigates the detrimental effect of socioeconomic deprivation in health.21 22 Accordingly, strong social networks and good social relationships are linked to good health, and conversely, poor social relations and weak social support networks are deleterious to health. Social support is considered to be a distal determinant of health that may influence health through multiple mechanisms, for example, by reducing stress and providing access to local resources, and in doing so, may prevent both mental and physical multimorbidity.
Social capital: while variously defined, social capital is broadly described as the functioning of social groups through a shared sense of identity, trust, cooperation, reciprocity and shared understandings, norms and values.23 Social capital emphasises that a more unequal distribution in income undermines trust and damages social relationships at a population level. This theory attempts to explain why egalitarian societies tend to be healthier than non-egalitarian societies.24 25 Similar to social support, high social capital is likely to boost health and prevent multimorbidity by reducing stressors and increasing access to shared resources.
In addition to the above-mentioned theories, a life course framework examines the effect of early life socioeconomic exposures on later health outcomes.26 Two models are proposed to explain the life course framework: the accumulation model and the critical periods model. The accumulation model emphasises the cumulative effect of exposure to socioeconomic disadvantage across different stages in life on subsequent increased risk of poor health outcomes.27 The critical periods model focuses on the effect of exposure to factors influencing health during critical periods of development.27 Finally, a neo-liberal framework for health inequalities emphasises the role of political arrangements in leading to socioeconomic inequalities and in turn health inequalities.28
We aim to review the socioepidemiological theories applied to explain the relationship between socioeconomic disadvantage and multimorbidity in the population. Where possible, we examined whether theories applied were tested using robust analytical methods such as mediation analysis.
Methods
We conducted a scoping review to examine epidemiological theories applied to explain the association between socioeconomic disadvantage and multimorbidity29 30 and to map the information available in the current literature. Because the primary purpose of this study was to identify and categorise the theories being used in the existing literature, a scoping review was preferred over a systematic review. We followed the steps of a scoping review as per previously defined guidelines.29 30
Stage I: identifying the research question
Our review question was: ‘How are the socio-epidemiologic theories applied to explain the relationship between socioeconomic disadvantage and multimorbidity?’.
Stage II: identifying relevant studies
We identified search terms and keywords relevant to socioeconomic disadvantage, theoretical pathways and multimorbidity from published systematic reviews13 31 and tailored them to answer our research question. First, a detailed search strategy was developed using keywords and hierarchically defined subject headings. Once the search terms were agreed on, they were adapted for multiple electronic databases including Medline, Embase, PsychInfo (Ovid platform), Web of Science, Scielo, Applied Social Sciences, ERIC, Humanities Index and Sociological Abstracts (see online supplemental appendix 1). The reference lists of all selected articles were screened to identify any additional studies. Search alerts were set up to notify the research team of articles published after 25 May 2018 when literature search was implemented. This search was updated on 11 December 2019 and then on 28 September 2021.
Supplemental material
Stage III: study selection
We applied a strict inclusion and exclusion criteria; these are displayed in table 1. We use the term socioeconomic position to reflect socioeconomic status of individuals or groups in the population. Socioeconomic status indicates the position in which an individual or a group is located within the social structure. It can be measured using educational attainment, income, occupation, wealth and area level measures (deprivation, socioeconomic scores). We use the term socioeconomic inequalities in health to indicate the differences in disease levels between people living with different socioeconomic positions. Socioeconomic disadvantage refers to those who have the low socioeconomic position. For inclusion in this review, socioeconomic position could be measured using the following indicators: occupation, income (household or individual), educational attainment, area level socioeconomic deprivation, wealth and social class.17 32
Study selection criteria
We excluded studies on ‘comorbidity’ as such studies are focused on an index condition (eg, diabetes).33 The terms multimorbidity and comorbidity are often used interchangeably as both describe the presence of multiple chronic conditions. However, comorbidity is a disease-centred term that describes the presence of additional conditions associated with an index disease.4 The focus of this review is multimorbidity only. Studies on institutionalised individuals, qualitative research and those written in a language other than English were excluded. A detailed list of inclusion and exclusion criteria can be found in table 1. Abstracts and full-text articles were reviewed for inclusion by LFA using the citation manager EndNote. A second reviewer (AS) cross-checked 10% of these articles.
Stage IV: charting the data
A data charting form was created that included study details (study design, country, population subgroups, measures of socioeconomic inequality, assessment of multimorbidity and conclusion on the association between socioeconomic variables and multimorbidity), use of theory, type of theories and context of application. Use of theory was categorised as inferred by us (reviewers/readers) or explicitly mentioned by the original study authors. It is important to distinguish between the two because the former relies on the reviewers/readers’ subjective judgement (which may not be accurate), while the latter accurately reflects the theoretical reasoning of the original authors. Data charting was performed by LFA and 10% of the studies were cross checked by AS.
Each study was examined for the type of theory (example: psychosocial or material), extent of use (whether used in a post hoc manner or integrated within an analysis) and their context of use (background, methods or discussion section of retrieved paper(s)). We recorded whether theories that were directly mentioned or inferred were consistent with any of the existing socioepidemiological theories. When directly mentioned, types of theories were recorded verbatim. This follows the approach previously applied in a published study examining the application of socioepidemiological theories in studies on the relationship between social inequality and oral health.31
Stage V: collating, summarising and reporting the results
We carried out a narrative synthesis to summarise the results from the retrieved data. Because the objective of this review is to offer a snapshot of the available evidence of theories explaining socioeconomic inequalities in multimorbidity and not on assessing the effect of socioeconomic disadvantage on multimorbidity development, we did not assess the quality of included papers in accordance with the guidelines for conducing scoping reviews.29
Patient and public involvement
No patients were directly involved in this study as this is a review of published studies.
Results
Our initial search led to the identification of 751 unique papers that underwent title and abstract screening. Sixty-nine papers were deemed eligible for full-text review. In addition, two studies were included for full-text review from other sources. Thirty-six studies proceeded to data charting stage after completion of full-text review. Online supplemental appendix 2 displays a list of studies with reasons for exclusion after full-text review. The updated search on 28 September 2021 led to a further screening of 461 titles and abstracts from the 573 newly identified records. After full-text screening of 44 studies, 27 new studies were included in the review. A total of 64 studies were included in this review. A flow chart of this process is shown in figure 1.

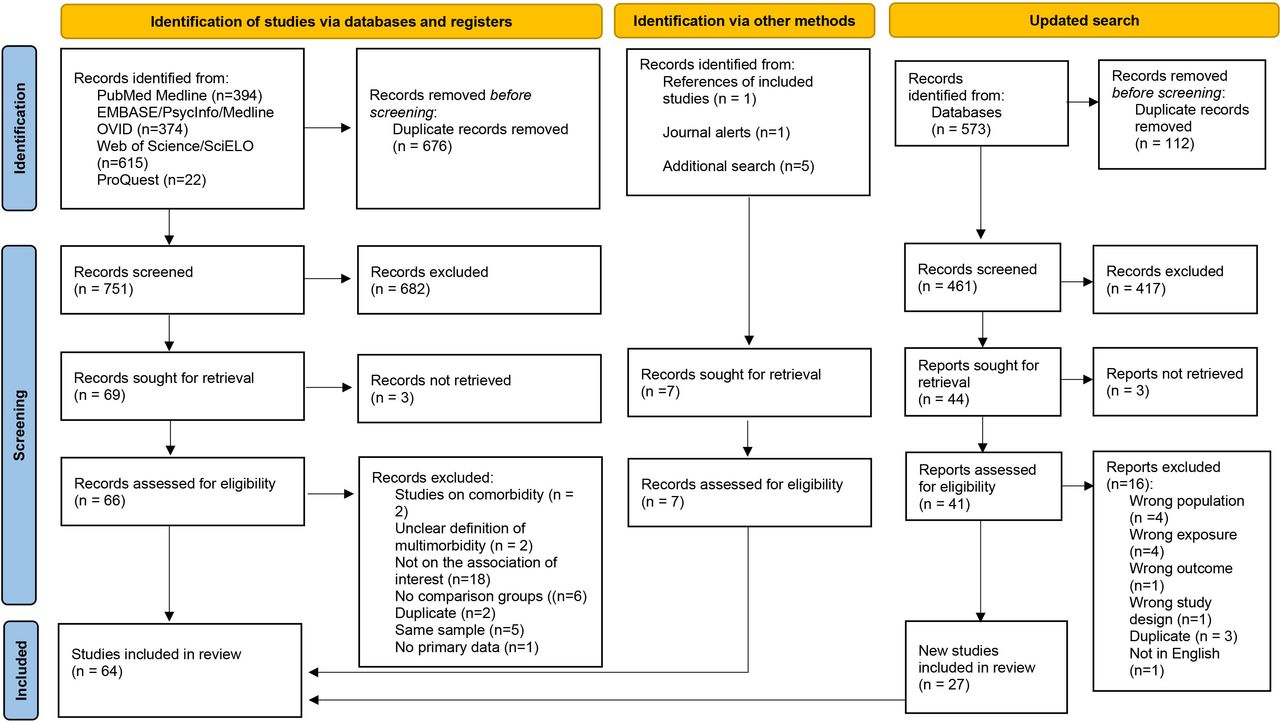{kind=link}
Flow chart of the study selection process.
Summary characteristics of included studies
Twenty studies were from low-income and middle-income countries12 34–52 and the remaining 45 studies were from high-income countries. The majority of articles were conducted among adults and only three study included children.53–55 More than half (n=38/64) were cross-sectional and 26/64 used longitudinal data9 10 42 54 56–76 (table 2).
Summary characteristics of included studies
Educational attainment was the preferred measure of socioeconomic position (n=38/64), and 38 studies used multiple measures of socioeconomic position as exposures. The majority of studies (n=51/64) simply documented the presence of multimorbidity, and approximately one-third (n=13/64) additionally examined different patterns of multimorbidity9 40 41 45 47 53 55 67–70 72 75 77 78 (table 2).
Types of theories
Overall, nearly half of studies (33/64) referred to at least one socioepidemiological theory. Therefore, 31 studies can be considered largely atheoretical, without any emphasis on pathways through which socioeconomic disadvantage leads to multimorbidity. In the 33 studies applying a theory, the following theories were referred to: behavioural,10 34 35 37 38 40–42 46 51–53 59 71 72 79–82 materialist38 41 42 45 46 48 50 52 71 72 74 79 82–85 and psychosocial.34 42 51 52 57 72 73 82 84–86 In addition, four studies applied a theoretical construct called ‘sense of coherence’, which indicates an individual’s coping capacity to deal with life and stressful events,87 and is an indicator of self-efficacy and psychosocial well-being (consistent with psychosocial explanations),73 and also encompasses social capital51 and social support,57 which are widely considered as psychosocial assets (table 3). Five studies used a life-course framework.10 55 63 64 74 Collectively, behavioural theory was the most referred to among studies.
Types of theories and context of application
Context of application of theories
Of the papers using theories, 15 explicitly stated those theories,10 35 38 41 57 63 64 72–74 80 82 84–86 and the other 21 studies were inferred to be consistent with a presumed theoretical pathway, based on definitions from existing literature.
Testing the explanatory potential of theories
Only five studies10 38 63 72 80 tested variables consistent with theoretical pathways as mediators between socioeconomic disadvantage and multimorbidity. Applying material theory, Chung et al38 examined perceptions of financial hardship, an indicator of economic deprivation, as a mediator between housing tenure and multimorbidity. They found a small mediation effect (1.41%), indicating that increased financial burden puts private housing residents at a higher risk of suffering multimorbidity when compared with public housing residents.38
Drawing on behavioural theory as well as a life course framework, Katikireddi et al10 quantified mediation by five behavioural risk factors (diet, smoking, physical activity, alcohol and body mass index (BMI)) acting on the association between two socioeconomic measures (area-based deprivation and household income) and multimorbidity over the life course. Their analyses showed that the combination of behavioural factors partially mediated (by 40.8%) the inverse association between area level deprivation and multimorbidity.
The life course framework was applied by Johnston et al63 in their examination of educational attainment during adulthood as a mediator of the association between father’s occupational social class at birth and multimorbidity. Their analyses showed a partial attenuation of the effect of childhood socioeconomic position on multimorbidity by educational attainment. Authors did not report the proportion of effect that was mediated by adult educational attainment.
Mondor et al80 also drew on behavioural theory in their study that quantified the mediation effect of lifestyle factors (physical activity, smoking and BMI) on the association between income inequalities and multimorbidity. Lifestyle factors only explained a small proportion of observed income-related inequalities in multimorbidity. Physical activity explained 10.9% of income inequalities, while smoking and BMI only accounted for 1.8% and 0.4%, respectively.
Finally, Singh et al72 examined social support as a mediator between financial hardship and multimorbidity among Australian adults and found that 30% of the total effect of financial hardship on multimorbidity was transmitted through social support.
Discussion
Summary of findings
Overall, we found limited use of theories to explain the relationship between socioeconomic position and multimorbidity. When used, theories were seldom explicitly mentioned or tested. Among all the potential explanations, behavioural theories were the most frequently used, followed by materialist and then psychosocial theories.
Only five studies tested the explanatory potential of theories and their mediation effect on the association between socioeconomic position and multimorbidity. Although we identified the use of seven different theories, materialist, behavioural, psychosocial and life course theories were the only ones tested. Existing evidence partially support these theories10 38 63 72 80; however, their use was mostly limited to post hoc explanations of findings in the overall literature.
Our findings are consistent with the two major evidence gaps highlighted in the report ‘Multimorbidity: a priority for global health research’.4 First, evidence of the relationship between socioeconomic disadvantage and multimorbidity is largely cross-sectional. This is a limitation of the existing evidence, as temporal ordering between exposure (social disadvantage) and outcome (multimorbidity), a key undisputed criterion of causality,88 is difficult to establish cross-sectionally. Second, there is a paucity of evidence regarding pathways (eg, behavioural, material and psychosocial) between the shared causal factor (exposure to socioeconomic disadvantage) and multiple conditions that co-occur in multimorbidity.4 The lack of evidence precludes policymakers from intervening on causal mechanisms that can prevent or mitigate observed socioeconomic inequalities in multimorbidity.89 Among those studies testing theories, there was a predominance of the application of the behavioural theory. However, the use of contemporary approaches to causal inference, using a counterfactual framework to maximise exchangeability between exposed and unexposed participants, was limited.72 89 Therefore, we cannot rule out bias arising from mediator-outcome confounding, time varying confounding or the presence exposure–outcome interaction. Approaches need to shift towards a more comprehensive examination of pathways to allow policymakers to select interventions with maximum capacity to reduce inequalities. It is also worth noting that given the variations in the relationship of interest according to individual (eg, age) and contextual characteristics (eg, country level of income development), future studies should examine the relevance of theories across different contexts and age groups.
Strengths and limitations
Our study has some strengths and limitations. To our knowledge, this is the first scoping review that explores the use of theories to explain the association between socioeconomic position and multimorbidity in the current literature. We identified numerous gaps in the literature that need to be addressed to improve our understanding of the socioeconomic inequalities in multimorbidity. Our search strategy drew on a wide range of electronic databases, and we used a robust methodology, already piloted and verified in previous work.31 A key limitation is that articles not in English were excluded in our review. Moreover, we did not use any tool to assess the quality of the included studies. This information is already provided by existing reviews.13 14 Lastly, we restricted this review to articles assessing only multimorbidity and excluded those looking at comorbidities. We acknowledge that some authors use both terms interchangeably, therefore papers using the term comorbidity to indicate the presence of multiple independent chronic conditions may be missing from this review.
Conclusion
Our understanding of the pathways between socioeconomic inequalities and multimorbidity is limited and mostly unexplained. Studies often focus on the patterns of distribution of multimorbidity across the population, rather than the mechanisms shaping these distributions. Robust evidence from longitudinal and interventional studies is needed to understand the pathways between socioeconomic disadvantage and multimorbidity. Generating such evidence will guide the development of interventions and public policies to prevent multimorbidity among people living in disadvantage.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
This study does not involve human participants.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors LFA contributed towards the development of search strategy, screening, data extraction and appraisal of included studies and manuscript preparation. AS contributed towards the design, development of search strategy, screening, data extraction and appraisal of included studies and manuscript preparation. EY contributed towards the development of search strategy, data extraction of included studies and manuscript preparation. TK and DC-S contributed towards the development of search strategy and manuscript preparation. SZ contributed towards manuscript preparation. LFA and AS are the guarantors.
Funding TK is also supported by an Australian Research Council Discovery Early Career Research Award (DE200100607).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.