Article Text

Abstract
Objectives The aim of this study was to assess the association of antenatal maternal dietary patterns (DPs) and other health aspects with infant temperament in a large multiethnic cohort, taking maternal personality and prenatal stress into account.
Design and methods Using data from 3968 children born in 2009/2010 and their mothers from the Growing Up in New Zealand cohort, infant temperament was assessed at 9 months using the Infant Behavior Questionnaire-Revised Very Short Form. Maternal antenatal diet and other health aspects were assessed antenatally. Maternal DPs (n=4) were derived using principal components analysis based on food intake reported on a 44-item food frequency questionnaire. Path analyses investigated factors associated with infant temperament, namely maternal personality, prenatal maternal stress, DPs and other health aspects, including potential inter-relations and mediating effects.
Results Women who scored higher in the fusion DP (standardised beta (β)=0.05; 95% CI 0.02 to 0.09) and healthy DP (β=0.05; 95% CI 0.02 to 0.09), who exercised more (β=0.04; 95% CI 0.01 to 0.07), and who drank less alcohol (β=−0.05; 95% CI −0.08 to –0.02) were more likely to have infants with an overall less difficult temperament. Sex-specific differences were found in the associations between maternal DP and infant temperament. Maternal personality and prenatal stress were significantly associated with all dimensions of infant temperament. The strongest predictors for a more difficult temperament were prenatal stress (β=0.12; 95% CI 0.08 to 0.15) and the personality dimensions neuroticism (β=0.10; 95% CI 0.07 to 0.14) and extraversion (β=−0.09; 95% CI −0.12 to –0.06).
Conclusions Associations of antenatal maternal diet and health aspects with infant temperament were statistically significant but small. While they should not be overinterpreted as being deterministic, the findings of this study support the link between maternal modifiable health-related behaviours and infant temperament outcomes.
- nutrition & dietetics
- epidemiology
- mental health
- gynaecology
- paediatrics
Data availability statement
Data are available upon reasonable request. Anyone who wants to use Growing Up in New Zealand data needs to first submit a Data Access Application. Further information on the possibilities can be found here: https://www.growingup.co.nz/access-growing-data.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This is the first study to look at the association between the whole of diet and infant temperament.
A major strength is the use of path analysis, which enables the exploration of the complex inter-relations between antenatal maternal diet, antenatal stress and maternal personality.
This analysis uses data from roughly 4000 children and their mothers from a large multiethnic population-representative cohort.
It is a limitation of this study that all information was mother-reported and could be not validated by observed information.
A further limitation, which comes as a result of the large number of variables in the analysis, is that more than one-third of the initial study population of about 6500 children could not be considered in the analysis.
Introduction
Temperament is defined as ‘constitutional differences in reactivity and regulation… influenced over time by heredity, maturation, and experience’ (Rothbart and Derryberry, p.37),1 and is typically conceptualised in the three broad dimensions: Negative Affectivity—tearful, easily frustrated, difficult to soothe; Surgency—happy, active, sensation-seeking; and Effortful Control—attentive, concentrated, easy to please.2 Temperament in infancy is of public health interest, because it is the foundation on which behaviour and personality develop, and thus has been shown to predict later problem behaviour, cognitive outcomes and mental and physical health.3–8
Current research is making advances in explaining differences in temperament, behaviour and mental health not only by examining genetic differences but also through a multitude of early life exposures. Based on the Developmental Origins of Health and Disease approach, which puts the first 1000 days between conception and the second birthday into focus, research has increasingly focused on common in utero exposures, such as stress, health behaviour and variations in maternal diet.9–11 There is now growing evidence that the offspring’s psychological, behavioural and cognitive development is associated with such variations in the in utero environment, especially with regards to maternal stress.11–16 Apart from its potential direct effect on the fetus’s brain, stress experience has also been shown to coincide with and to alter the mother’s behaviour with regards to dietary intake, physical activity or medication and drug intake,17 18 which may in turn have direct effects on the fetus’s development.11 12 19 20
A number of studies have associated particular diets or specific nutrient intakes or deficiencies with changes in temperament or behaviour in children,21–23 however, to date, no published study has looked at the associations between the whole of diet and temperament or behaviour in infancy.24 During the last few years, a small body of studies has evolved which investigated potential effects of certain aspects of maternal diet in conjunction with prenatal stress.11 15 In their literature review, Monk et al state, ‘These prenatal experiences exert their influence in the context of one another and yet, almost uniformly, are studied independently’. Since 2013, a small number of studies have shown that a bidirectional effect between stress and diet exists, and that there are possible interaction effects of prenatal stress and diet/nutrition on infant and child temperament and behaviour development.11 17 25–27 However, only two of the above studies looked at infant temperament, one at the association with antenatal chocolate intake26 and the other at the association with antenatal omega 3 to omega 6 fatty acid intake ratio,27 and none has investigated the influence of the whole of maternal diet during pregnancy on the offspring temperament.
In summary, while there is a body of studies on the associations between certain domains of prenatal stress, diet and other health aspects with infant and child temperament, the literature in this field is very patchy, excessively heterogeneous and conspicuously devoid of null results. Moreover, most of the studies have three major shortcomings in common: (1) failure to draw a complete picture of antenatal maternal diet and other health aspects: a large proportion of publications studied single micronutrients or macronutrients in isolation, thus neglecting the context of the whole of diet or other health aspects, such as exercise or smoking and alcohol consumption; (2) poor confounder adjustment: while the majority of studies adjusted for sociodemographic variables, such as maternal age and education, maternal personality was not considered as potential confounder, even though a substantial part of temperament is thought to be genetic;28 and (3) limited statistical analyses techniques to explore inter-related factors such as maternal personality, maternal stress, maternal diet, other health aspects and their effect on temperament.
The aim of our study was to assess the association between antenatal maternal dietary patterns and other health aspects with infant temperament in a large multiethnic cohort using path analyses, which enable the exploration of the complex inter-relations between antenatal maternal diet and other health aspects, antenatal stress and maternal personality.
Methods
Study population
This study was conducted within the contemporary New Zealand birth cohort study Growing Up in New Zealand (GUiNZ), which enrolled 6822 pregnant women and their 6853 children who survived to age 6 weeks.29 Written informed consent was obtained from all mothers in this study. The cohort of children is broadly generalisable to New Zealand birth statistics with respect to ethnicity, maternal age and socioeconomic status.29 This study used information from three data collection waves, completed antenatally and when the children were approximately 9 months and 2 years old. From the antenatal questionnaire, we used information on maternal stress, sociodemographics and health aspects, including diet (assessed with a food frequency questionnaire (FFQ)). Infant temperament was assessed at the 9-month interview and maternal personality was assessed at the 2-year interview. Baby’s sex and gestational age were collected perinatally and linked to GUiNZ data set from perinatal and maternity records.30
Infants were included in the analysis: if information on infant temperament was available from the 9-month interview; if mothers had provided information on stress, sociodemographics, diet and other health aspects antenatally; if mothers had provided information on maternal personality at the 2-year interview; and if perinatal information could be linked from the official records (n=6129 of the 6476 children who took part in the 9-month interview) (online supplemental figure 1). Children were excluded from analysis if factors were present, which would likely affect the validity of the infant temperament scale: inadequate English language skills of the mother (n=161); infant’s behaviour during the preceding week less than somewhat typical (scores 1–2) (n=703); born preterm (n=393); or older than 52 weeks old at the interview (n=107), as this is outside the target range of the infant temperament measure.31 Children whose mothers had not been able to respond to the antenatal questionnaire prior to giving birth were excluded to minimise recall bias for the FFQ (n=712). Finally, n=179 children had to be excluded from analysis because of missing values in at least one of the explanatory or adjustment variables other than body mass index (BMI) and gestational weight gain. Thus, the final number of children assessed was 3968, corresponding to 61.3% of the children who took part in the 9-month interview (online supplemental figure 1).
Supplemental material
Study variables
Antenatal maternal diet
Antenatal maternal diet was assessed by a semiquantitative 44-item FFQ during pregnancy, for which mothers recalled their food intake over the 4 weeks preceding the antenatal interview. The food list of the FFQ was developed based on the New Zealand Ministry of Health guidelines for healthy pregnant women,32 which recommends the adequate intake of four core food groups: fruits and vegetables, breads and cereals, milk and milk products and lean meat, meat alternatives and eggs. The frequency of the intake of individual foods was described by categories increasing from not at all or less than once a month to a number of times per month, week or day. Show cards were used to illustrate a standard portion size.33 34
A previous study identified four distinct dietary patterns (DPs) during pregnancy using principal components analysis and performing a varimax orthogonal rotation.34 High loadings for the food items were defined as being larger than 0.30 or smaller than −0.30. The DP junk was characterised by high positive loadings for confectionary, snacks, takeaways, hot chips, soft/energy drinks, cakes/biscuits, processed meats, battered fried fish/seafood and ice cream. The healthy DP had high positive loadings for vegetables, brown whole meal bread, cheese, non-citrus fruits, yoghurt, dried fruits, high fibre cereal and Vegemite/Marmite. The traditional DP had high positive loadings for whole/standard milk, white bread, margarine, jam/honey/marmalade, peanut butter/Nutella and a high negative loading for skim/trim milk. The fusion DP had high positive loadings for noodles/rice/pasta, seafood, chicken, green leafy vegetables, eggs, red meat, processed fish and citrus fruits (online supplemental table 1).34 Together, these four DPs explained 23.4% of the total dietary variance in this population and individually the junk, healthy, traditional and fusion DPs explained 7.7%, 5.6%, 5.4% and 4.8% of the dietary variance, respectively. For all following analyses, the women were ranked in quintiles of the score in each of the four respective DPs.34
Supplemental material
Other relevant health aspects
Folic acid supplementation during pregnancy was described in three categories: folic acid supplementation that started before pregnancy; folic acid supplementation that started in first trimester; and folic acid supplementation that started after the first trimester or never.
Women reported on their moderate and vigorous weekly physical activity before and during pregnancy by providing the number of days with exercise and the duration of an average exercise episode over the last 7 days. Using an abbreviated version of the International Physical Activity Questionnaire,35 we decided to focus on pre-pregnancy exercise because pre-pregnancy exercise levels are not affected by pregnancy health problems. The American College of Sports Medicine and the American Heart Association recommend 150 min of moderate or 60 min of vigorous physical activity for adults aged 18–65 years.36 In alignment with these recommendations, we calculated a weighted exercise score, towards which vigorous physical activity counted with a factor of 1, and moderate physical activity with a factor of 0.4.
Pre-pregnancy BMI was calculated based on self-reported pre-pregnancy weight and height and it was classified according to the WHO cut-offs.37 Monthly gestational weight gain (kg) was calculated as the difference between the current weight at the time of the antenatal interview and the reported pre-pregnancy weight. To take account of different gestational ages at the time of the interview, this difference was divided by the elapsed months of pregnancy up to the time of the interview.
Nausea experience was reported during the first trimester and after the first trimester on a 4-point scale, ranging from 0 – no nausea, over 1 – mild nausea and 2 – moderate nausea, to 3 – severe nausea, respectively. In this study, nausea was defined as the maximum severity of nausea experienced at any time during pregnancy. Finally, we also captured self-reported alcohol consumption and smoking during pregnancy. We created three categories: women who did not drink any alcohol before pregnancy; women who stopped drinking alcohol at the beginning of pregnancy; and women who drank alcohol during pregnancy. Self-reported smoking behaviour was categorised likewise.
Prenatal stress
Prenatal perceived stress was assessed during the antenatal interview by the 10-item Perceived Stress Scale,38 for which women have to report the frequency of different stress-related experiences and feelings during the preceding 4 weeks on a 5-point scale (1=Never, 2=Almost never, 3=Sometimes, 4=Fairly often, 5=Very often). The perceived stress score was retrieved by summing up over the 10 items.
Maternal personality
Maternal personality was assessed by the big five inventory (BFI) at the 2-year interview.39 40 The 44 items for the assessment of personality are a popular measure of personality due to the established factor structure, high reliability, good convergent validity with other longer Big Five measures of personality and acceptable self-peer agreement.39–41 While few studies have looked at the stability of the BFI 44 across adulthood, high stability has been reported with the BFI 44 over a 3-year period across middle adulthood.42 In addition, research using the Big Five personality traits more generally, has repeatedly shown that the rank order stability of the Big Five personality increases with age peaking at around the age of 60 and does not vary much by assessment method.42 43 The BFI 44 used in this study uses a 5-point Likert scale which asks how strongly a person agrees or disagrees with statements about themselves. Each item is associated with one of the five personality factors: extraversion—sociable, outgoing, energetic; agreeableness—forgiving, compliant, sympathetic; conscientiousness—organised, efficient, thorough; neuroticism—irritable, shy, moody; and openness—imaginative, curious, excitable.39 Scores for the five personality factors are derived by averaging over all items that load on the respective factors.
Infant temperament
The 37-item Infant Behavior Questionnaire-Revised Very Short Form (IBQ-R VSF) was used to assess infant temperament at the 9-month interview.31 In a previous analysis it was shown that a five-factor structure was a better statistical fit for the Growing Up in New Zealand Cohort than the original three-factor structure.44 The fit of the five-factor model was found to be acceptable in this cohort44 and the factors were found to be similarly precise across four ethnic groups (European, Maori, Pacific Peoples and Asians).45 In addition, within this cohort, the five factors have also been related to mother- and partner-reported infant closeness, parenting confidence and parenting satisfaction in the expected direction.44 The five-factor model consists of Negative Affectivity (NEG), Positive Affect and Surgency (PAS) and a slightly altered factor Orienting Capacity (OC), along with two new factors Affiliation/Regulation (AR) and Fear, which separated out from the broader factors of Orienting and Regulatory Capacity and NEG, respectively (see online supplemental table 2) for a brief description of these factors).
In completing the IBQ-R VSF, mothers or caregivers were asked to indicate how frequently their child engaged in specific behaviours during the past week on a scale from 1 to 7 (1=Never, 2=Very rarely, 3=Less than half the time, 4=About half the time, 5=More than half the time, 6=Almost always, 7=Always). The mothers could choose the option ‘not applicable’ if they had not seen the child in the situation. Temperament scores were calculated by averaging over all items that were found to load on the respective temperament factors. Because infant behaviour is very changeable over any given week (eg, due to illness or teething), and the reference period for the questionnaire was the behaviour over the last week, an additional question was asked: ‘In terms of your baby’s behaviour, how typical has the last week been for your baby?’, in which mothers were asked to respond on a scale from 1 (not at all typical) to 5 (very typical).44
Sociodemographic variables/adjustment set
We used six antenatal sociodemographic variables in our analyses: parity; maternal education; maternal age; self-prioritised ethnicity; deprivation at area level; and deprivation at household level. Parity is binary in these analyses and discriminates between first-born and subsequent children. Mothers’ education was assessed in five categories, namely: no secondary school qualification; secondary school qualification; diploma or trade certificate; bachelor’s degree; and higher degree. The maternal self-prioritised ethnic group was categorised into: European; Māori; Pacific Peoples; Asian; and Middle Eastern, Latin American, African and Other. We used two distinct variables to account for deprivation, one at the area level and one at the household level. Area deprivation was based on results from the 2006 National Census around nine socioeconomic indicators, which enabled assignment of a 10-point deprivation index to each geographical area, where 1 was assigned to the least deprived areas and 10 to the most deprived areas.46 Household deprivation was based on six questions from the 9-month interview, asking mothers if their financial situation during the preceding 12 months had affected their access to adequate food, clothing and/or heating. A mean score was calculated over the six variables, with higher values indicating more severe household deprivation.
Statistical analysis
We fitted path analysis models to assess the associations between the dimensions of maternal personality, stress, maternal diet/other health aspects and infant temperament. To determine the important paths, we first assessed pairwise associations between these dimensions. We used directed acyclic graphs (DAGs) to describe hypothesised associations between our exposures, outcome, and potential confounding variables.47 A graphical presentation of our proposed DAGs can be found in online supplemental figure 2. We made decisions about which confounders we needed to adjust for in the respective analyses based on the respective DAGs. All regression models and path analyses were adjusted for the six sociodemographic variables.
Supplemental material
Preparatory analysis
To determine the important paths for the path analysis, in the preparatory analyses we first assessed pairwise associations via multivariable linear regressions between the following dimensions: (A) maternal personality and prenatal perceived stress; (B) maternal personality/stress and DPs/other health aspects; (C) maternal personality/stress and infant temperament; and (D) DPs/other health aspects and infant temperament. Associations between maternal personality and prenatal perceived stress were examined by regressing stress on the five factors of maternal personality (online supplemental figure 2, Panel A). Associations between maternal personality/stress and DPs/other health aspects were assessed by regressing each of the eleven maternal health aspects (DPs and other health aspects) on the five factors of maternal personality and the one stress factor: a total of 11 distinct linear regression models, adjusting for the six major confounders from the adjustment set (online supplemental figure 2, Panel B). Continuous outcomes are a requirement for linear regression. To be able to use diet and other health aspect variables as outcomes, these variables were transformed from categorical to ordinal scale, which implies a clear order of values: DPs (in quintiles); folic acid supplementation; nausea; alcohol consumption; and smoking. To give an example, alcohol was used as a continuous variable, taking on the values 0–1–2 for women who: did not drink any alcohol before pregnancy (0); who stopped drinking alcohol at the beginning of pregnancy (1); and who drank alcohol during pregnancy (2). Under the assumption of missing at random, multiple imputation with 20 data sets was applied to be able to use information from women with missing values for BMI and/or gestational weight gain.48
The association between maternal personality/stress and infant temperament was assessed in five linear regression models, one for each factor of infant temperament (online supplemental figure 2, Panel C). For the associations between DPs/other health aspects and infant temperament, we used five linear regression models with the respective infant temperament factors as outcomes, and the four DPs and the other health aspects (exercise, folic acid, BMI, gestational weight gain, nausea, alcohol and smoking), as explanatory variables, which were divided into meaningful categories, as presented in the online supplemental table 3. All five models were adjusted for maternal personality, stress and the six adjustment variables (online supplemental figure 2, panel D). As a preparation for the main path analyses, we performed a test for trend across the categories of the explanatory variables. A test for trend was conducted by assigning a clear order to categories of the variables of interest and subsequently using them as continuous variables in the analyses.
Path analysis
Five path models were used to investigate potential inter-relations and mediating effects between maternal personality/stress, DPs/other health aspects and the respective factor of infant temperament (online supplemental figure 2), panel E). As all variables for DPs/other health aspects were used as explanatory and outcome variables simultaneously in path analyses, they were used on a continuous scale. All models included the personality/stress variables, and the DPs/other health aspects variables, which had shown to be associated (p≤0.05) in a test for trend with the respective infant temperament factor. All direct paths between these variables and the temperament outcome were fitted. Paths between maternal personality and stress were defined if p≤0.05 from the preparatory regression analysis. Likewise, paths between personality factors/stress and DPs/other health aspects were only specified if p≤0.05 for their association from preparatory regression analysis. All equations in the path analyses were adjusted for the six sociodemographic variables, and maximum likelihood was used to treat missing values. Comparative Fit Index (CFI); root mean square error of approximation (RMSEA); and standardised root mean square residual (SRMR) were used to assess model fit for path analyses.
To estimate the significance level of indirect effects in path analyses, we used bootstrapping with 200 bootstrap samples. In those path models that included maternal BMI, we worked with a reduced sample of 3595 infants without missing values in maternal BMI. To assess potential differences between girls and boys, we additionally fitted stratified models by child’s sex. Data management and regression analyses were carried out using Stata IC V.14 software, and IBM Amos software was used to calculate path analyses, including indirect effects.49 50
Patient and public involvement
Patients or the public were not involved in the design, or conduct, or reporting, or dissemination plans of our research.
Results
Our final analysis sample of 3968 infants was largely comparable to the complete study population in most aspects (online supplemental table 4). Despite several statistically significant differences between included and excluded participants, the magnitude of the differences in mean values were mostly small and a sufficient number of participants could be maintained in all categories. On average, women in the final sample came from less deprived households, had higher education, were older, were less likely to smoke, had experienced less stress during pregnancy and identified more with European/Pākehā ethnicity. Women had on average been 7.4 months pregnant (SD=0.9 months) at the antenatal interview. The average age of the infants during the 9 months interview was 8.9 months (SD=0.5 months).
Direct associations with infant temperament
Prenatal stress was significantly associated with higher NEG and lower AR and OC, independent of maternal personality (figure 1). All dimensions of maternal personality were significantly associated with infant temperament and all dimensions of infant temperament were significantly associated with at least one dimension of maternal personality (figure 1, online supplemental table 5). The strongest associations were between maternal openness and infant PAS, and maternal neuroticism and infant NEG.
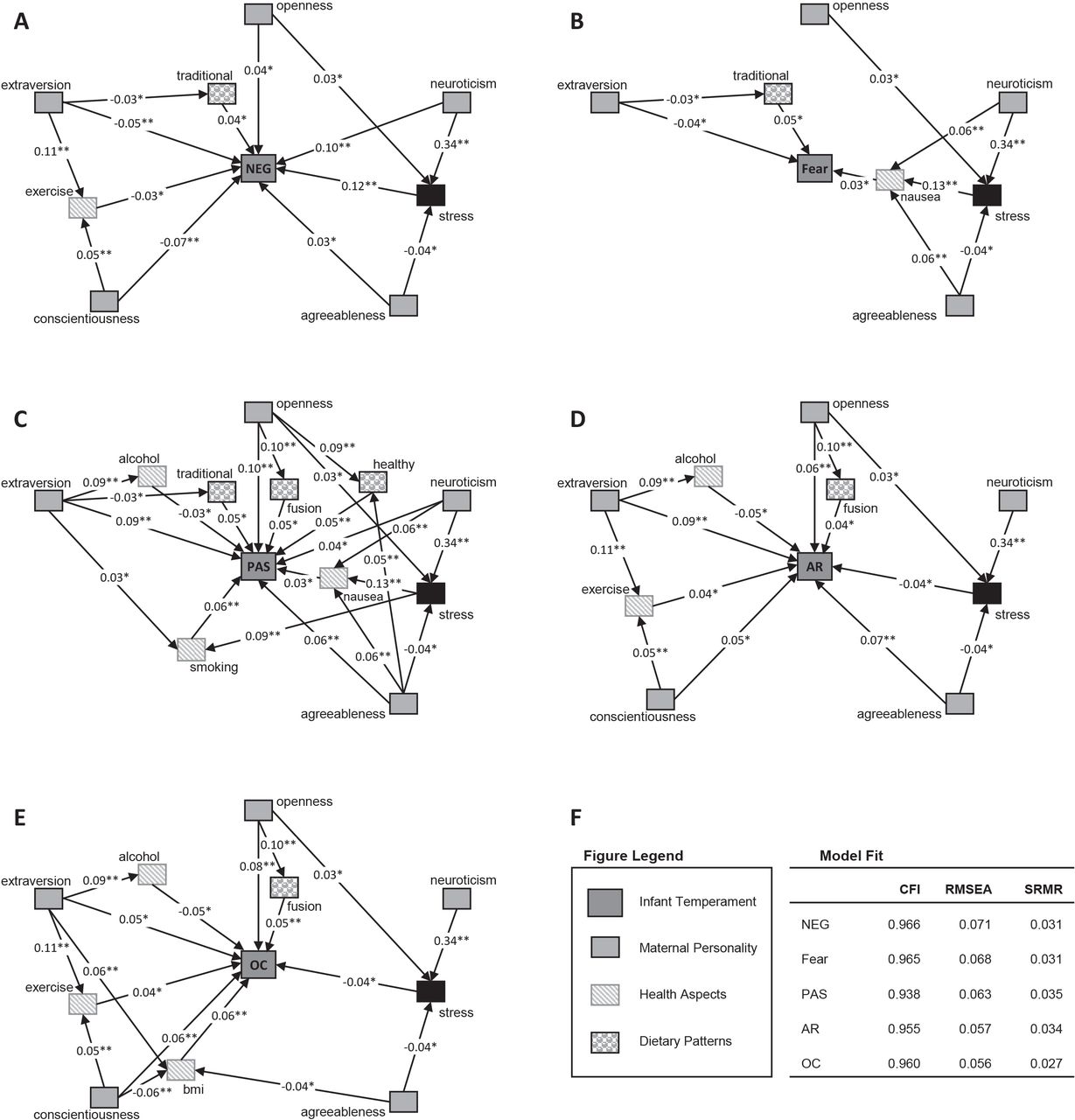
{kind=link}
Standardised estimates from final path analyses with each of the five infant temperament factors as major outcome, and maternal personality, stress, dietary patterns and other health aspects as explanatory variables, *p≤0.05, **p≤0.001, p>0.05 not shown. Analyses were adjusted for maternal age, maternal education, mothers’ ethnicity, area deprivation, household deprivation and parity. AR, Affiliation/Regulation; CFI, Comparative Fit Index; NEG, Negative Affectivity; OC, Orienting Capacity; PAS; Positive Affect Surgency; RMSEA, root mean square error of approximation; SRMR, standardised root mean square residual.
Maternal DPs and other health aspects were most strongly associated with the temperament dimensions PAS and OC, independent of maternal personality, prenatal stress and maternal sociodemographic factors. (figure 1C,E, online supplemental table 3). Higher adherence to the fusion pattern was significantly associated with higher scores in PAS, AR and OC. In addition, infant PAS was significantly higher in children whose mothers had higher adherence to the healthy DP. More exercise and, surprisingly, higher maternal pre-pregnancy BMI were significantly associated with higher infant OC. Higher alcohol consumption was significantly associated with lower scores in PAS, AR and OC. Conversely, continued smoking during pregnancy was associated with higher PAS after adjustment for maternal personality and stress. Results for the traditional DP were mixed: Children of women who scored higher in the traditional DP had higher scores in PAS, NEG and Fear. No statistically significant associations with infant temperament were found for the junk DP in the overall sample after adjustment for potential confounders. Model fit criteria indicated that all five path analysis models have good or acceptable fit (CFI ≥0.938, RMSEA ≤0.071 and SRMR ≤0.035) (figure 1F).
Indirect associations with infant temperament
Maternal personality and prenatal stress were associated with diet and other health aspects (online supplemental table 6), and maternal neuroticism was strongly associated with prenatal stress (figure 1A–E). In addition to its direct effect on infant NEG and PAS, maternal neuroticism showed significant indirect effects on infants’ NEG, Fear and AR (0.04, 0.01 and −0.01, respectively, p<0.05). The standardised total effect of maternal neuroticism on infant NEG was 0.14 (95% CI 0.11 to 0.18), consisting of the direct effect of 0.10 (95% CI 0.07 to 0.14) and the indirect effect of 0.04 (95% CI 0.03 to 0.05) via prenatal stress. Apart from the indirect effect of maternal neuroticism on infant NEG, several other indirect effects of maternal personality and prenatal stress on infant temperament were significant at the 5%-level but were very small (β ≈ 0.01).
Sex-specific differences
The results in girls and boys were largely comparable in most aspects (online supplemental figure 3), but some differences were apparent. The traditional DP of the mother was significantly associated with infant NEG, Fear and PAS in girls, but only showed minor associations in boys. The opposite was seen for the fusion DP of the mother, which was significantly associated with increased PAS, AR and OC in boys but not in girls, except for OC. The same was shown for alcohol consumption during pregnancy, which seemed to be negatively associated with boys’ temperament more strongly than with girls’ temperament. NEG in both girls and boys was associated with maternal neuroticism and prenatal stress. While the direct association between maternal neuroticism and NEG was stronger in girls, there was a stronger indirect association via stress in boys (β=0.05; 95% CI 0.03 to 0.07) than in girls (β=0.03; 95% CI 0.01 to 0.05). Maternal openness contributed more strongly to infant PAS and AR in girls, while maternal agreeableness was more strongly associated with infant PAS and AR in boys.
Supplemental material
Discussion
Our findings indicate that maternal diet and other health aspects during pregnancy were significantly associated with infant temperament, independent of and in conjunction with maternal personality and prenatal stress. However, overall effect sizes of diet and health aspects were rather small, mostly around 0.05, and should therefore not be over interpreted as being deterministic of infant temperament. The major pattern that evolved in our analysis was that a healthier diet (higher scores in the fusion and healthy DP and lower scores in the traditional DP) as well as a healthier behaviour (more prenatal exercise and less alcohol consumption in pregnancy) were associated with a so called ‘easier’ infant temperament (lower NEG and higher PAS, AR and OC), independent of maternal personality, prenatal stress, maternal age, parity, education, deprivation and ethnicity. Two of the maternal DPs (traditional and healthy) and maternal pre-pregnancy exercise showed stronger associations with infant temperament in girls, while the fusion DP and alcohol use were more strongly associated with infant temperament in boys.
The potential influence of maternal diet on the infants’ temperament may be explained by potential direct biological or epigenetic effects. Studies in animals and humans have shown associations between certain nutrient intakes or deficiencies and temperament/behaviour outcomes.12 13 22 25 27 An alternative and indirect explanation could be that healthier women or women with healthier diets and health behaviours may have physically healthier children,51 52 and that healthier children may be more likely to show a ‘sunnier’ temperament in infancy. The finding that a poorer overall health rating in children at the 9-month interview was significantly associated with a more ‘difficult’ temperament in our cohort (results not shown) to some extent supports this. The key for both explanations may be the offspring’s gut microbiome, which has only recently been associated with behavioural outcomes.53 54
Infants of mothers with higher scores in the fusion DP showed higher scores in OC, AR and PAS, and infants of mother with higher scores in the healthy DP scored higher in PAS. The fusion DP is characterised by high intakes of meat, seafood, eggs and green leafy vegetables, which are good sources of iron, folate, selenium and vitamin A. Thus, a higher score in the fusion DP could be protective of iron deficiency which has been shown to affect neural plasticity and brain function in animal studies.12 However, in this study we did not measure actual iron status, so we are unable to support this pathway. The healthy DP was characterised by high intakes of vegetables, wholegrain bread, cheese, non-citrus fruits, yoghurt, dried fruits and high fibre cereal, which are good sources of dietary fibre, selenium, vitamin C and provitamin A (carotenoids). Ours findings align partially with findings reported by a cohort study in the USA, which identified that higher maternal intake of selenium and vitamins A and C during pregnancy was associated with higher scores in toddlers’ Surgency, which is closely related to infant PAS.25
While the junk DP was strongly associated with prenatal stress in our sample, we found no independent association between the junk DP and infant temperament. Associations between unhealthy diet in pregnancy and negative behavioural outcomes have been demonstrated in other studies, although most of these studies have looked at outcomes in much older children, who may also have been exposed to unhealthy diets during childhood.21 23 24 55
In our study we identified significant associations between higher scores in the antenatal maternal traditional DP and higher infant NEG, Fear and PAS. The traditional DP is characterised by high intakes of whole/standard milk, white bread, margarine, jam/honey/marmalade, peanut butter/Nutella and low fibre/high sugar cereals. These food items are energy dense, with a high content of sugar, refined carbohydrates and saturated fat. Our finding is in agreement with an animal study that showed a higher activity level in piglets if the mother sows had received a diet high in fat and sugar.56
When examining the effect of micronutrient supplementation, such as folic acid, iron or multivitamin, we found no significant associations with infant temperament in the fully adjusted analyses. This is contrary to previous studies in humans and animals, which have shown associations between maternal use of iron and folic acid supplements and behaviour/cognitive outcomes.15 57 However, if we specify our regression models without adjustment, we also find negative association between earlier folic acid supplementation and infant NEG, Fear and PAS. Thus, any associations between maternal folic acid supplements use and infant temperament may in fact be explained by other maternal characteristics. While folic acid supplementation is recommended for all pregnant women in New Zealand, such a recommendation does not exist for iron supplementation,32 which is not generally recommended unless prescribed by a health professional.
We found two somewhat unexpected associations in our analyses, one of which is that infants whose mothers continued to smoke during pregnancy had higher scores in PAS. This is, however, supported by other findings from published studies in this area, one of which reported higher activity/intensity at 6 months and higher activity level at 5 years in the offspring of mothers who smoked during pregnancy.58 The second unexpected association was that pre-pregnancy BMI was positively associated with OC. Based on previous research, we did not expect to find this association because higher BMI had been associated with behaviour problems in later childhood and not convincingly been associated with any dimension of infant temperament.59–62 Thus, it is possible that maternal pre-pregnancy BMI per se does not negatively influence temperament or behaviour but that associations seen in later childhood actually depend on postnatal factors, such as child diet and nutrition. A bimodal association was observed between pre-pregnancy BMI and OC, where children of underweight and obese women had significantly higher scores in OC as compared with children of women with normal weight, while children of women who are overweight were not any different from women with normal BMI. It is however possible that a relationship between maternal obesity and parental attachment may impact on child temperament as previous research has demonstrated lower mother–child attachment in 19–58 month-old children of obese versus normal-weight mothers.63
Limitations
Our research question has a large scope in a very complex research area, and thus, undoubtedly, comes with several limitations. All variables that we used in our analysis were mother-reported, including infant temperament. While we did not have any laboratory assessments of infant temperament, other studies have demonstrated validity of the temperament measures using both laboratory studies and mother and partner reports.64 65 It could also be shown that the temperament factors related well to two measures of language and communication development in our cohort, and this information was also reported by mothers and their partners.44
In the present analysis, we treated maternal personality as a determinant of infant temperament, although it had actually been measured later, when the children were 2 years old. It is possible that the birth of a child may have slightly altered mothers’ personalities, but this should not have meaningfully influenced our estimates, as personality is assumed to be fairly stable during adult age, especially with regards to rank-order stability.66 67 In other words, while mothers may in general become less conscientious when a baby is born,67 this shift is likely to have influenced all mothers. Numerous factors are likely to contribute to the stability of personality over time including genetic factors, maturation, niche building (where people create, seek out and build environments associated with their traits) and the developing commitment to maintaining a sense of identity.43
We had to exclude 39% of children, whose mothers had initially provided information at the 9-month data collection wave, mainly due to the sensitivity of our measures of antenatal diet and infant temperament, which raises the question of generalisability of our findings. However, while the distribution of population characteristics was slightly altered after exclusion, thanks to the large study population, we still retained a large number of participants from all subgroups. We conducted a sensitivity analysis, which also included preterm infants and infants with non-typical behaviour (n=4777) and yielded comparable results. Thus, while the absolute distribution of characteristics in our sample may not be generalisable to the overall population, our measures of association are unlikely to be strongly biased by this selection.
A last limitation concerns the large number of associations tested and reported. As a result, a number of the presented associations may be spurious findings and should be interpreted with caution, especially the findings with larger p values and/or smaller effect estimates.
Conclusion
The present study offers an exceptionally broad view into the multiple interdependencies between maternal personality, prenatal stress, maternal diet, other health aspects and infant temperament. While maternal personality and prenatal stress are known predictors for the development of temperament, we provide evidence that healthy diet and behaviour have independent associations with a less ‘difficult’ infant temperament. Although these associations are not strong and should not be overvalued as being deterministic of infant temperament, their magnitude is in line with other temperament studies. Our findings support the existence of the developmental origins of temperament, and that prenatal stress, maternal diet and other health aspects play a part in them. Despite existing guidelines for a healthy nutrition in pregnancy, the food environment in New Zealand, just as the majority of the Western World, encourages intake of energy-dense and nutrient-poor foods, and makes healthy food choices difficult. We provide evidence, that improvements in the food environment may not only improve the physical health of the population, but could also have a positive although small impact on the development of temperament and mental health.
Data availability statement
Data are available upon reasonable request. Anyone who wants to use Growing Up in New Zealand data needs to first submit a Data Access Application. Further information on the possibilities can be found here: https://www.growingup.co.nz/access-growing-data.
Ethics statements
Patient consent for publication
Ethics approval
Ethical approval was granted by the Ministry of Health Northern Y Regional Ethics Committee (NTY/08/06/055). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The study has been designed and conducted by the Growing Up in New Zealand study team, led by the University of Auckland. The authors acknowledge the contributions of the original study investigators: Susan M.B. Morton, Polly E. Atatoa Carr, Cameron C. Grant, Arier C. Lee, Dinusha K. Bandara, Jatender Mohal, Jennifer M. Kinloch, Johanna M. Schmidt, Mary R. Hedges, Vivienne C. Ivory, Te Kani R. Kingi, Renee Liang, Lana M. Perese, Elizabeth Peterson, Jan E. Pryor, Elaine Reese, Elizabeth M. Robinson, Karen E. Waldie, Clare R. Wall. The views reported in this paper are those of the authors and do not necessarily represent the views of the Growing Up in New Zealand Investigators.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors The study idea, approach and methods were conceptualised by AS, ERP, CW, KEW and SM. SM was responsible for the design and the conduct of the Growing Up in New Zealand study. AS conducted the statistical analyses, prepared the tables and figures, and drafted the manuscript. TGC, CW, ERP and SD provided their expertise on the thematic areas and gave feedback throughout all stages of the analysis and the drafting of the manuscript. All authors reviewed the manuscript, provided input and approved the final version. AS is the guarantor of this study.
Funding AS was supported by a research fellowship of the German Research Foundation (DFG) (SCHO 1865/1-1).Growing Up in New Zealand has been funded by the New Zealand Ministries of Social Development, Health, Education, Justice and the former Pacific Island Affairs (now the Ministry of Pacific Peoples); the former Ministry of Science Innovation and the former Department of Labour (now both part of the Ministry of Business, Innovation and Employment); the former Ministry of Women’s Affairs (now the Ministry for Women); the Department of Corrections; the former Families Commission (later known as the Social Policy Evaluation and Research Unit and now disestablished); Te Puni Kokiri; New Zealand Police; Sport New Zealand; the Housing New Zealand Corporation; and the former Mental Health Commission, The University of Auckland and Auckland UniServices Limited. Other support for the study has been provided by the NZ Health Research Council, Statistics New Zealand, the Office of the Children’s Commissioner and the Office of Ethnic Affairs.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.