Article Text

Abstract
Background Maternal and newborn mortality are still high in low-income and middle-income countries despite global efforts to improve the quality of care by prioritising evidence-based practices and increasing the number of births attended by skilled personnel. During childbirth, women are hesitant to use the health facility services. Concerns about safety and risks during pregnancy, childbirth and postpartum period are deeply rooted in local health practices and beliefs.
Objective The aim of this study was to explore the perceptions of local health knowledge and derived practices among nurse-midwives in urban eastern Tanzania.
Methods An exploratory qualitative study design was carried out in a district hospital in eastern Tanzania. Twenty-one nurse-midwives participated in two focus group discussions. The data were analysed using qualitative content analysis.
Results Based on existing scientific data, local knowledge and derived practices were categorised as potentially beneficial, neither beneficial nor harmful and potentially harmful. Our study identified a wide range of local knowledge and derived practices used by women. These include to refrain from shouting or crying to prevent exhaustion during labour, drinks and foods restrictions during labour and after birth, and use of local herbs to stimulate labour. In addition, midwives reinforced the importance of integrating local knowledge and practices with potential benefits with evidence-based practices. Encouraging and listening to women would offer an opportunity to reduce harmful practices.
Conclusions While non-harmful and beneficial practices for ensuring safety during pregnancy, childbirth and postpartum period should be accepted and supported as a part of our cultural richness, harmful practices should be discouraged. This can be achieved through antenatal health education and afterbirth health messages on hospital discharge to promote positive childbirth health outcomes.
- QUALITATIVE RESEARCH
- PUBLIC HEALTH
- Maternal medicine
Data availability statement
Data are available on reasonable request. The datasets generated and/or analysed during the current study are not publicly available and are limited due to confidentiality but are available from the corresponding author on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
A qualitative study through focus group discussions enhanced the richness and credibility of findings.
Selection bias may have limited the findings, since the study recruited participants from those involved in the larger scope mobile educational App study.
A limited sample, only two focus group discussions were conducted at a single health facility.
Nurse-midwives expressed opinions about the beliefs and practices of pregnant and postpartum women without a supporting information collected directly from them.
Introduction
Despite efforts to reduce maternal and newborn mortality, their rates in Tanzania are among the highest in the world, with 524 deaths/100 000 and 21 deaths/1000 live births, respectively.1 Postpartum haemorrhage, eclampsia and puerperal sepsis, as well as birth asphyxia, are the leading causes of these deaths.2 In Tanzania, 63% of deliveries take place in a health facility, and 64% of these are assisted by a skilled birth attendant.3 Several factors negatively influence the decision of a woman to give birth in a healthcare facility: geographical distance, perception of care quality, fear of stigma or discrimination and lack of privacy within healthcare facilities.4 Women might be hesitant to use the health facility during childbirth owing to the negative attitude of the healthcare provider towards them.5 6 Additionally, the cultural background of a woman can influence her needs and expectations during pregnancy and childbirth and prevent her from receiving antenatal, delivery and postnatal care at the health facility.7
Childbirth is a biosocial event distinguished by its universality and the uniqueness of each social and cultural context in which it occurs.8 Currently, it is crucial for healthcare professionals to ensure the survival of the mother and newborn. Concerns regarding pregnancy-related, childbirth-related and postpartum-related safety and risks are firmly rooted in local health practices and beliefs.9 Traditional practices and beliefs on maternal and newborn care vary from community to community, depending on their distinct culture and traditions. Several studies describe the traditional beliefs and practices surrounding childbirth.10–12 Some traditional practices are advantageous for mother and child, while others are not. Women continue resorting to them, considering them beneficial for their well-being, because their mothers and other senior women close to them have used these practices and guaranteed for their health benefits.13
Local knowledge is defined as a type of knowledge formed through people’s practice and experience in their daily interactions with the natural and social environments.14 This includes not only traditional practices, but also modern scientific knowledge, which is in accordance with the beliefs of people based on their everyday life. Globally, women continue to use local knowledge and derived practices during pregnancy, childbirth and postpartum periods.8 12 15 In Asia, confinement of postpartum women is more frequent owing to the perception they are weak and susceptible to illness.11 In India, it is believed that if a pregnant woman craves sweet foods, the baby will be a girl; if she craves salty foods, the baby will be a boy.16 In sub-Saharan African countries, local knowledge and derived practices include food restrictions, abdominal massage with hot water, delaying initiation of breast feeding, avoiding colostrum, confinement to protect pregnancy from evil forces and use of local herbs,7 17 18 while religious beliefs include prayer and revelations, nullification of negative dreams by praying, imposition of hands and anointment.19
Local knowledge includes practices that sometimes contradict the medical view on risk and safety during childbirth, myths and beliefs that are neither beneficial nor harmful, and practices that are psychologically and physiologically beneficial for both mothers and babies. However, the extent of their potential benefits is not clearly understood as scientific reports on the subject are scarce. This resonates with Shigeta’s statement that pointed out two different approaches can be used to obtain knowledge in developmental studies and applied anthropology: one based on the significance of the practical aspect of something and the other seeking universality in its cognitive aspect. They are not antithetical, but rather complementary.20
As part of enriching our culture and values, the healthcare system should include local practices that could be beneficial for the patient while counteracting those that could be harmful. Rather than viewing local practices of women during pregnancy, childbirth and postpartum period in terms of a dualistic point of view (tradition vs modernity), this paper examines how midwives perceive these local practices, paying particular attention exactly to the points that cannot be captured by a dualistic view. This might help rethink the sociocultural practices of patients in terms of the generation and organisation of unknown knowledge about childbirth.
The global effort of improving the quality of care is based on prioritising evidence-based practices and increasing the number of births attended by skilled personnel to ensure the survival and well-being of maternal and newborns.21 However, this may not be sufficient because quality of care is subjective, therefore, healthcare system must consider the needs and expectations of service recipients.22 In the fields of environment or education, policy-making is based on local knowledge.23 24 In health sciences, in healthcare in general and in maternal and child healthcare in particular, local knowledge is not yet integrated into policy and healthcare standards. However, there is an ongoing dialogue regarding turning local knowledge and experiences into innovative tools for improving quality of care during labour and childbirth.25 26 UNESCO promotes local and indigenous knowledge for Sustainable Development Goals (SDGs), and explaines that SDG number three (good health and well-being) should respect local culture and practices to gain social acceptability.27
This study investigated how the local knowledge and cultural practices are used for promoting safety and health during pregnancy and childbirth, as well as how health professionals may integrate these habits in their current practice to make women more willing to resort to them. We described local knowledge based on the perspective of local healthcare specialists. The research team attempted to develop this area of science, named ‘medical local knowledge’.28 A better understanding of the local context may facilitate the modification of health education messages for women and communities, thus increasing their efficacy in reducing the risk of perinatal deaths.
Methods
Study design and context
This exploratory qualitative study employed focus group discussions (FGDs) to gain insight into the phenomenon of local knowledge and derived practices used by women during pregnancy and childbirth among nurse-midwives in Tanzania. The study was conducted at Mnazi Mmoja Hospital located at the centre of Dar es Salaam city. It has one of the oldest clinics in Dar es Salaam that provides antenatal care (ANC) to a big population and is easily accessible by public transit from all areas of the city. Dar es Salaam has the highest percentage (35%) of women receiving ANC.3 Nurse-midwives working at this facility have a great potential to meet women with different backgrounds and culture. Thus, the facility is ideal for studying what nurse-midwives have learnt on local knowledge and derived practices during childbirth.
Study participants and recruitment
This study is part of a more extensive study that aimed to assess the feasibility of using a mobile App-based antenatal education programme among pregnant women and their families in Tanzania and its potential efficacy in teaching them danger signs and preparing them for birth from 2020 to 2021. The development of the App was led by the fourth author using the WHO guideline recommendations on antenatal and intrapartum care. The App was named ‘Goocus’ and was accessed in form of a smartphone App that contained educational content in a form of videos, pictures and narratives. The more extensive study involved nurse-midwives to download and study materials provided by the App. The interview on local knowledge was included so that the App would not contain only imported but also local knowledge beneficial for pregnant women. To this end, participants were purposively recruited as they possessed local knowledge related to pregnancy and childbirth based on the following criteria (1) being involved in the mobile educational App study, (2) working at the antenatal clinic or labour ward and (3) providing counselling and health education to women during pregnancy, labour or after delivery. The matron (in-charge of nurses and midwives) was contacted to identify participants and to help organising the FGDs. The identified participants were contacted by the researchers either in person or by phone to establish rapport and to set a day and time for an appointment to participate in one of the FGDs. We conducted 2 FGDs, 1 with 11 and the other with 10 participants, thus including a total of 21 participants.
Patient and public involvement
None.
Data collection
The data were collected in July 2021. The FGD guide was developed in English (see table 1) by the fourth author and then translated into Kiswahili by the first author. The latter version was used for conducting the FGDs. The first and second author who are fluent in both English and Kiswahili acted as facilitators of the discussions, took notes, audiorecorded the discussions and checked transcription and translation from Kiswahili to English and vice versa. The transcripts and notes were only shared to the research team for data analysis. Written informed consent was obtained from each participant for taking part in the FGD and for audiorecording. FGDs procedures were explained, and participants were informed that their participation is voluntarily and they may choose to stop the discussion at any time.
Focus group discussion guide
The FGDs took place at the health facility for the convenience of study participants, in a conference room suggested by them and the hospital matron. One FGD per day was conducted to provide the time needed for debriefing and preparing for the following FGD. The lead moderator asked questions while the comoderator took notes and audiorecorded the discussion. The items were constructed based on literature data17–19 and the prior experience of researchers on what concerns pregnancy-related and childbirth-related sociocultural beliefs. Based on FGD results, we investigated the local knowledge and derived practices used by women during pregnancy, labour and childbirth among nurse-midwives and how they should use local knowledge when providing health services. Participants were encouraged to share their opinions on the local knowledge no matter if they perceived it to be useful or harmful. The FGDs lasted between 60 and 65 min.
Data analysis
All FGD transcripts were transcribed verbatim. Before an analysis, the Kiswahili transcripts were translated into English. Second author cross-checked the accuracy and completeness of translations against the original data. Qualitative content analysis approach as described by Graneheim and Lundman was used to guide the analysis.29 The first author developed the initial coding scheme based on our objective and the conceptual understanding of the local knowledge and derived practices in Tanzania. The coding template was checked by the fourth author. Before beginning the coding process, two researchers (first and fourth authors) read and reread the transcripts to familiarise themselves with the data. The text were divided into meaning units and then were condensed while keeping their original meaning intact. Codes were extracted from the condensed meaningful units. We coded the meaningful units of text to specific codes representing that unit manually. To ensure reliability, two researchers independently coded each transcript and then met to discuss and agree on the codes. The new codes were assigned as a separate codes or expansion of the codes available in the initial codebook. Then, similar codes were grouped together, and subcategories were created through abstraction. Categories reflecting the apparent content of the text were formed by comparing, checking and rechecking similarities and differences across the subcategories. The third author reviewed the initial results, then all authors discussed and agreed on the final subcategories and categories. Categories were supported with suitable quotes from the transcripts.
Trustworthiness
To enhance the credibility and dependability of this study, we triangulated study participants (diversity in experience, education level and working unit) and researchers (midwives and an anthropologist). To confirm that the findings reflect the perspectives of the participants rather than the researcher’s understanding of the phenomenon under study, categories, were inductively generated and presented alongside concise quotes. The transferability of the study findings is enhanced through the description of the study design, context, data collection and analysis process.
Results
Background information
Twenty-one midwives participated in FDGs. Their average age was 43.3 (range from 27 to 59, SD 9.9). The average years of work experience was 15.1 (range from 5 to 33, SD 8.6). Most midwives (61.9%) completed secondary school, seven (33.3%) completed a university and one (4.8%) completed a primary school. Most midwives had an education qualification of a certificate (42.9%), diploma (42.9%) or degree (14.3%). Out of 21, 20 defined their occupation as nurse-midwife (95.2%) and 1 (4.8%) as midwife. All of them worked in the antenatal clinic and provide counselling to patients 2–5 days a week.
From the analysis of FGDs, we identified four categories that characterised the local knowledge used by women to promote positive outcomes during pregnancy, labour and after birth. As this information would be used for the further development of the App, we screened its accuracy and safety. Subsequently, based on scientific data, the local knowledge information was categorised as either potentially beneficial, neither beneficial nor harmful, or potentially harmful. The midwives’ perceptions on the use of local knowledge are illustrated in figure 1.
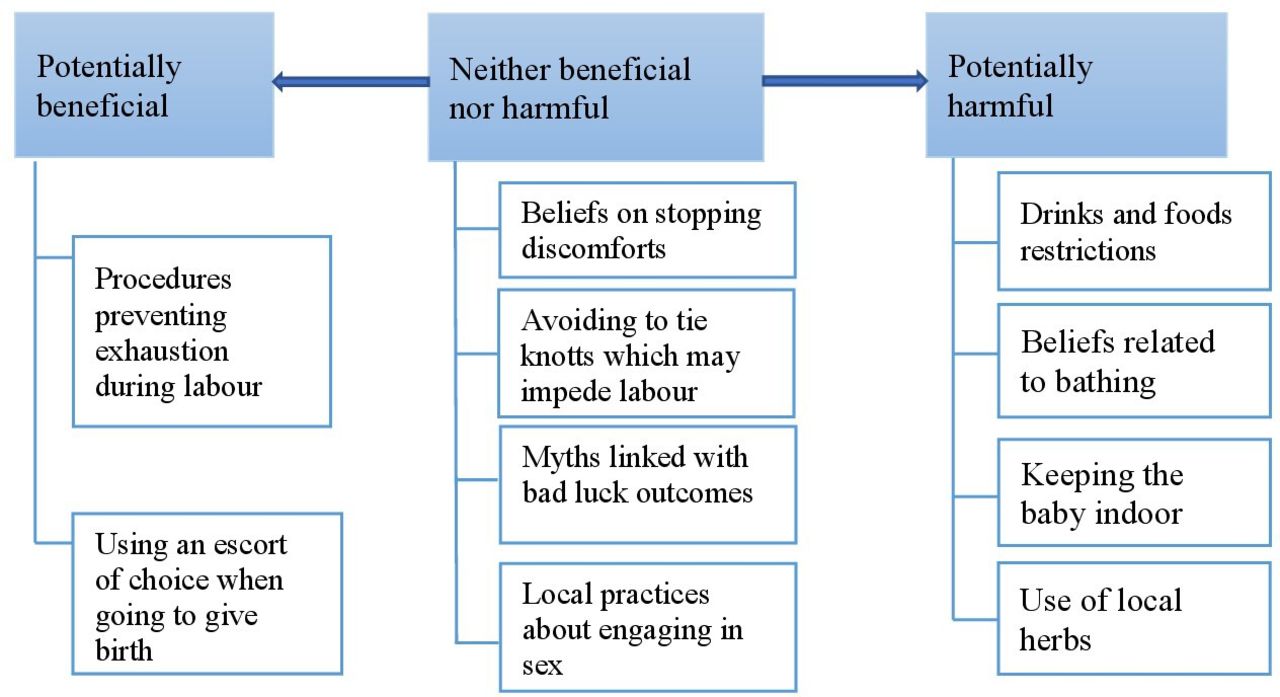
{kind=link}
The perceptions of midwives on the use of local knowledge.
Potentially beneficial local knowledge and derived practices and beliefs
Participants reported that women use local knowledge to refrain from shouting or crying during labour so as not to spend energy needed during the pushing stage. The community frequently prepares women for parturition, the primary focus being to ensure that they can endure prolonged labour. Participants stated that women feel that if they scream or cry of pain, they will be unable to push the baby during the second stage of labour owing to exhaustion.
"…locally, pregnant women are frequently adviced not to cry because the baby will become tired and not cry, and not to shout for a long time or otherwise she will become weak … when she reaches the second stage, she may be restless and unable to push the baby out or, after birth the baby may have a low score" (FGD1, Participant 2)
Another local practice in preparation for childbirth is having an escort of choice when going to give birth and a preferred assistant after birth. Participants reported that women prefer having their mothers to accompany them to the hospital and stay with them after delivery for assistance with childcare and breast feeding. Conversely, some women, particularly those giving birth for the first time, tend to travel to their parents for the same purpose: getting support from a preferred individual.
"When a woman is pregnant for the first time, she prefers to have her mother or grandmother present as her due date approaches or … may also choose to move to her parents. Women believe that they will receive more assistance and support regarding childbirth related issues from other fellow women than from their partners" (FGD2, Participant 3)
Neither beneficial nor harmful local knowledge and derived procedures and beliefs
Myths and beliefs on how to stop discomforts during pregnancy also exist. Participants stated that locally women smell their own fingernails or armpits to stop morning sickness during pregnancy. In addition, licking ashes is claimed to prevent heartburn.
"I learnt this from my mother, who also learned it from her grandmother that a pregnant woman with nausea must smell her five fingernails … if she smells her fingernails or her armpit the nausea goes away … this is the mostly used […method…] to alleviate the nausea" (FGD1, Participant 2)
"… for example, when a pregnant woman experiences heartburn, she is instructed to eat ashes; when she licks ashes, the discomfort subsides" (FGD2, Participant2)
Further, participants stated that most people believe that a pregnant woman wearing a cloth around her neck will lead to the baby having a cord wrapped around his neck. They also said that at the onset of labour, women are forbidden from zipping their bags or tying knots on their clothing, as this might prevent the start or continuation of labour. Conversely, leaving the zipper open or avoiding tying knots on clothing allows the cervix of the woman to open and the labour to progress unimpeded.
"My mother once taught me that a pregnant woman who is about to give birth or who is close to term should not close her bag containing delivery materials or tie knots in her clothing …. she should leave the bag open and refrain from tying knots to facilitate a rapid dilatation during labour" (FGD1, Participant 8)
Participants described the events believed to be linked with bad luck especially on the outcome of the baby. Thus, pregnant women are told not to shake hands with strangers or stand at the door as this brings bad luck on the outcome of the pregnancy. Also, a woman should never cry during labour as this determines bad luck, causing her baby not to cry immediately after birth.
"Some people also believe that a woman who is about to give birth must be forbidden from standing at the door … and should not wear a cloth that comes around the neck because the baby will have a cord wrapped around its neck" (FGD1, Participant7)
Participants reported engaging in sex in late stages of pregnancy is a local practice in preparation for labour. Women believe that engaging in sex is essential in ensuring smooth delivery and is highly recommended. Furthermore, sex restrictions might make one’s partner engage in extra marital affairs.
"Having sexual intercourse especially in the final days of the pregnancy, stretches the path for the baby so that the woman does not experience any complication…. it also prevents men from engaging in extramarital affairs to satisfy their sexual needs and from passing sexually transmitted diseases to the mother and the unborn baby" (FGD1, Participant 6)
Additionally, participants reported that women practice sexual restriction after childbirth to protect the health of the infant. This is because having sex while breast feeding a baby who has not yet learnt to walk is said to be harmful and to delay the child to walk. Participants said other women move to their parents during late stage of pregnancy or immediately after giving birth to avoid resuming sexual activity. Sexual restrictions may extend to a period of up to 6 months for women who gave birth through caesarean section (C-s).
"I also wanted to say another thing: that during breastfeeding, women feel that having sexual contact with their partners after harms their infant by inducing diarrhea and delay walking … many believe this and after giving birth, they avoid having sex until the child walks" (FGD2, Participant 5)
Potentially harmful local knowledge and derived procedures and beliefs
Participants indicated women believe drinking and eating during labour should be restricted, as they slow contractions. Midwives said some women do not drink during labour because their relatives have convinced them that drinking cold water will stop the pain and delay childbirth. The bowel movement shortly preceding pushing is believed to show that a woman consumed food during labour and is considered a shameful event. These views are described below.
“Some women who come to labour wards do not eat. They have been mistakenly told that eating makes them defecate, which is unfortunate and a shame. So, women strive not to eat at all, despite being told by midwives that defecating is normal…” (FGD2, Participant 7)
Another participant added that the food restriction is highly practiced among mothers who underwent C-s who feel they should not eat even when permitted by a physician to avoid wound related problems.
"Who give birth by C/S, are more anxious … at home after being discharged, they drink only porridge or mtori (stew of banana) for several days or months … they believe that food is stored where the incision lays" (FGD2, Participant 2)
Specific beliefs related to bathing exist, such as giving postpartum mothers a hot bath/shower or a hot water sponge bath to aid a fast recovery after delivery-associated pain. Participants considered this a harmful practice that needs to be changed even though many tribes have adopted it.
"I wa thinking about the hot water bath practice during the first postpartum week, however, is less practiced and phasing out… now a hot water body sponging is mostly practiced and believed to make a woman feel better and relax her so that when she goes to sleep, it will be long and restful" (FGD2, Participant 10)
On the other hand, taking bath during labour is thought to stop the contractions as explained by one of the participants.
"Another concern of pregnant women which come to labour ward is they feel that taking a shower makes their labour pain subside. So, you may find a woman stays for even 2 days without bathing" (FGD2, Participant10)
Women keep their babies indoor for about 40 days or even more, despite recommendations babies benefit from light. Other beliefs include that tying the umbilical cord with the rope around the neck will prevent the baby’s navel from falling on his or her genitalia, thus preventing infertility in the adulthood.
"There is a practice of tying the navel with a rope around the baby’s neck. One woman once told me “if I let it fall on my son’s penis, it would not function later, he would become infertile” …. this has been a tenacious belief for a long time" (FGD1, Participant 11)
Additionaly, participants stated that some women believe that taking local herbs throughout pregnancy and during labour promotes a healthy pregnancy and gentle delivery. They reported women chew an okra stem to enable a quick opening of the cervix and a shorter and painless labour. However, participants declared that evidence associates the use of local herbs with abnormal labour, excessive pain and even uterine rupture.
"Women use roots that we believe are local herbs … there are times when a mother enters labour ward and we do not know if she has taken something until she explains that her mother gave her a medication that expedite her labour pain … she has precipitous labour, sometimes women end up with uterine rupture and a series of other looming complications" (FGD1, Participant11)
The points of view of midwives on the use of local knowledge
Participants stated that women have strong ties to the local knowledge because related beliefs, based on personal childbirth experiences, were instilled to them by their grandmothers, mothers-in-law, senior women in the community, or other close and trustworthy individuals. Additionally, the reliance of women on traditional beliefs to maintain their safety throughout pregnancy, childbirth and motherhood, is also a consequence of limited access to accurate scientific information.
"Let me add just a little bit there, a woman receives information from a close adult person, and because she is younger, she must listen … there is a saying an adult is a medicine, having seen many more than we have… thus, she must believe what is told by older people" (FGD1, Participant 9)
Participants acknowledged that they must listen and understand why women value local practices. They said listening can be the key to impede the use of harmful traditional beliefs and practices. Another participant stated that healthcare providers must learn not to disregard the ideas of women for them to cooperate and speak up.
"You listen to it and then support her if it has not effects but if it is a bad practice, you do not command her to stop; rather you must listen and look for an appropriate way to rectify it. Because if you immediately dismiss her idea, she will not cooperate, and you will be unable to stop the behavior" (FGD1, Participant 4)
Midwives admitted that some of the beliefs and practices of women can be encouraged owing to their potential benefits. They added that women avoid exposing newborns to people to prevent evil spirits from attacking the infant. When considering tuberculosis as an example, participants thought avoiding exposure could be beneficial because it minimises the risk for infection. Additionally, avoiding sexual intercourse early after childbirth, for up to 42 days, is considered a beneficial practice and encouraged since it would lower the risk of infection in women.
"Some people may visit … you may give them your baby; someone may have tuberculosis, and as soon as the woman offers her child to them, they may begin kissing the baby … I also encourage them not to give a newborn baby to every guest who pays a visit" (FGD1, Participant11)
"… not letting people see a newborn before 40 days is practised in most tribes because they are afraid that people with bad eyes would harm the baby… others apply black ink to infant’s face to conceal their true appearance … mmmh things like that … to protect them from evil mmmh" (FGD2, participant8)
Participants also agreed that it is the time to discourage potentially harmful local knowledge and derived practices. They explained that by enhancing health education and counselling in our reproductive and child health (RCH) clinics, employing talks between peer health providers, and using social media, women may have access to proper information to counteract the myths and beliefs that put them at risk for several health complications. They stated that they cannot force women to not believe in local knowledge, but they can listen to them, build trust, and encourage them to follow advice and instructions given by health professionals.
"We should strive to discourage those that lead to poor outcomes, but how can we do it? … by changing gradually their traditions, customs and beliefs by providing regular health education at RCH and playing educational CDs in the waiting areas" (FGD1, Participant4)
Moreover, participants reported to rely on evidence-based knowledge when providing RCH services. They reported to encourage sexual resumption as outlined in the postnatal care guidelines, after 42 days following the birth. Additionally, nurse-midwives reported encouraging women to bring their partners to the health facility to promote male participation and increase access to accurate information regarding childbirth and parenting.
"… from my perspective, it is good that we utilize scientific knowledge. Although traditional beliefs may be useful in some ways, I still think we should rely on scientific knowledge" (FGD1, Participant 10)
"… we are making a concerted effort to inform mothers to come with their partners to the antenatal clinic, however, this does not happen frequently and hence makes a majority of men miss out on correct information regarding childbirth" (FGD1, Participant 3)
Discussion
This study highlights the descriptions of midwives of several local practices which women resort to, to ensure the safety of mother and baby during pregnancy, childbirth and postpartum period. The point of view of midwives provides both cultural sensitivity and scientific judgement. Despite being rooted in traditional habits, certain practices are scientifically sound. Some women prevented fatigue by refraining from shouting or crying owing to labour pain, as they believe that excessive shouting or crying during the first stage of labour would consume a lot of energy and interfere with their ability to push during the second stage of labour, resulting in birth asphyxia. They adhered to pain tolerance as one non-pharmacological approach, owing to both information on delivery received from family, as well as to their own apprehension on the importance of not depleting their energy in this manner but conserving it. According to studies, the ability to cope with labour pain reduces anxiety and fatigue,30 and helps conserving energy.31
Participants in our study reported that grandmothers, mothers and mothers-in-law care for women during pregnancy, childbirth and postpartum period, especially for those having their first child.9 32 Their responsibilities include escorting women to the health facility for ANC and delivery, as well as providing postpartum infant care support. The evidence shows that women greatly value and benefit from having a person of their choice nearby to provide emotional, psychological, practical support and advice during pregnancy, childbirth and post partum.33
Nurse-midwives perceived that women adhere to potentially harmful practices by not drinking or eating during labour, because drinking during labour is thought to stop contractions, while eating will contribute to defecation during the second stage of labour. The recommendation to avoid solid food during labour is made only to prevent the possibility of aspiration in case anaesthesia is used. However, mothers in uncomplicated labour are permitted to drink small amounts of liquids.34 35 In line with results from other studies, our findings indicate, after childbirth, women are encouraged to eat hot foods, large quantities of food, protein-rich foods and drink special fluids believed to significantly increase breast milk production.10–12 Additionally, we found that after C-s, women refrain from eating solid and semisolid foods owing to the belief that eating will cause wound-related complications. In Africa, the typical surgical wound is healed on the third postoperative day to a sufficient extent that a woman is discharged and eating is permitted at any time after surgery when the woman feels hungry.36 The health talk messages emphasise the prevention of potential infections during bathing, dressing and physical activities, as well as the maintenance of nutritious diet with a variety of food groups for safe recovery, the restoration of normal bowel function and the support of breast feeding.
Not only in Tanzania, but also in other countries, newborns are believed to be vulnerable to the ‘evil eye’ of jealous individuals; consequently, newborns and their mothers are placed in confinement for approximately 40 days.18 37 This has been associated with women not receiving postnatal care during the first 6 weeks after birth.18 This practice must be counteracted because it predisposes newborn to death. The statistics indicate that a high number of neonatal deaths occur in the first week of life and most of the associated fatal morbidities require prompt attention.38 In our study, participants provided opinions that local herbs are also widely used aiming to induce and shorten labour, as well as to facilitate a smooth delivery. A population-based study conducted in Tanzania shows that women used local herbs in their late pregnancy for stomach pain and for the health of the child, a practice which has been associated with childbirth-related complications.39 Other studies have also reported women to ingest or use local herbs as an enema in preparation for labour and birth with a belief that herbs will shorten and ease labour.18 40 41 The literature shows conflicting information regarding the use of local herbs during pregnancy. Some studies showed that the use of traditional herbs was associated with highly adverse obstetric outcomes, such as uterine rupture and fetal distress.39 42 43 In contrast, other studies reported no difference or found a higher prevalence of maternal complications in women who did not use local herbs than in those who did.44 45 These findings open the opportunity for discussions and investigations on how traditional remedies may be incorporated into modern medicine.
Participants also perceived that there were several non-beneficial but non-harmful local derived actions practiced by women to reduce discomfort and ensure their safety during pregnancy, labour and the postpartum period. Pregnant women adhere to practices such as avoiding tying knots in their clothing, because a knot would make delivery difficult and painful. Pregnant women are believed to be susceptible for being bewitched, which may result in negative outcomes such as losing pregnancy or death of the mother or baby. Additionally, pregnant women avoid standing at the door and shaking hands with non-family members because this would expose them to evil forces. This particular practice is harmless; however, the fear of bewitchment during pregnancy may contribute to some women delaying their first ANC bookings because they avoid people with the so called ‘bad or evil eye’.46 47 Healthcare providers must counteract this practice by discussing about the advantages of early ANC booking during health education so that pregnant women would not miss out the crucial preventive interventions provided in the first trimester.
Nurse-midwives showed a willingness to use available scientific evidence in the provision of midwifery care with the support of regular on-the-job training.48 49 Furthermore, they thought that integrating local knowledge and derived practices with potential benefits into the healthcare system, would contribute to meeting the needs and expectations of women. Incorporating practices that women and their families value would provide intercultural healthcare that acknowledges diversity and respects local knowledge. This has been shown to improve service quality and attract consumers.50 Despite the growing global acceptance of integration,51 the gap between healthcare systems and local health knowledge and derived practices persist in many countries.52 Nevertheless, some countries have successfully achieved such integration. Latin America is regarded as a good example where intercultural healthcare is widely accepted and traditional health beliefs and practices have been integrated into the healthcare practices.51
While the focus of the healthcare system is on counteracting harmful local knowledge and derived practices, our study revealed that listening to women may be an effective strategy for identifying and tackling harmful local practices that pose risks to the health of women and their newborns. This finding is in line with the results of a cluster randomised controlled trial by Sarmiento et al, in which a context-specific intercultural dialogue was conducted to listen ‘reflexively’ and identify culturally coherent maternal health responses from indigenous women.53 The study focused on understanding traditional midwifery and the existing cultural conflicts that prevent indigenous women to access healthcare services. The authors showed that listening provides women with the opportunity to share their views on local knowledge and derived practices, enabling healthcare providers to identify harmful practices and find collaborative ways to mitigate them.
Conclusion
This paper applied the concept of local knowledge to issues in the medical field. Local knowledge and derived practices regarding safe childbirth represent a practice that has been passed down from generation to generation, has become prevalent and is widely used even after the introduction of modern medicine. It is based not on the merits of the practice itself, but on the fact that the population surrounding the future mother encourages the practice. Our study provides opinions among nurse-midwives regarding local knowledge and derived practices used by women to reduce discomfort and ensure the safety of themselves and their babies during pregnancy and childbirth. Moreover, our findings indicate nurse-midwives thought that harmless local knowledge and derived practices and those having potential benefits are acceptable and may be integrated in provision of care to enhance satisfaction and to respect context specific-culture and values. We recommend that health education should be provided in health facilities during antenatal contacts/visits to prevent potential health complications among pregnant women and their infants. The implication of this research is that these practices were reported by healthcare providers, indicating they are aware they should focus not only on providing information but also on listening to the beliefs of their patients/clients. In this area of local knowledge research, knowledge and practices of local people (the local knowledge itself) are respected, however, its safety of local knowledge needs to be evaluated thoroughly.
Data availability statement
Data are available on reasonable request. The datasets generated and/or analysed during the current study are not publicly available and are limited due to confidentiality but are available from the corresponding author on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
Ethical clearance and permission to conduct this study were obtained from (1) Kyoto University Graduate School and Faculty of Medicine, Ethics Committee (C1446), (2) National Institute for Medical Research, Tanzania (NIMR/HQ/R.8/Vol.IX/1604) and (3) Tanzania Commission for Science and Technology (No. 2013-273-NA-2013-101). The study was conducted based on the principles of ethics such as harmlessness, lack of constraint, anonymity and protection of privacy and personal information. After obtaining information regarding the aim and design of the study, each participant provided written informed consent to participate in the FGD and to be recorded with an audio recorder. They were made aware that taking part in the study was voluntarily and they were free to decline or withdraw at any time. The participants were referred to using numbers to ensure anonymity during data collection.
Acknowledgments
Authors would like to thank all participants for giving up their time to participate in this study. We would like to thank Editage for English language editing.
References
Footnotes
Twitter @DMwakawanga
Contributors DLM participated in data collection, analysis and drafting the manuscript. YS participated in conceiving the study, its design, data analysis, writing and reviewing the manuscript. YS was the overall coordinator and guarantor of the study. MK participated in analysis, writing and reviewing the manuscript. BM participated in data collection, translation and reviewing the manuscript. All authors read and approved the final manuscript.
Funding This study was supported by KAKENHI Grant-in-Aid for Scientific Research (C) (20K10935).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.