Article Text

Abstract
Objectives Serum chloride has a unique homeostatic role in modulating neurohormonal pathways. Some studies have reported that hypochloremia has potential prognostic value in cardiovascular diseases; thus, we aimed to investigate the association of baseline serum chloride with clinical outcomes in elderly patients with non-ischaemic dilated cardiomyopathy (NIDCM).
Design Retrospective study.
Setting and participant A total of 1088 patients (age ≥60 years) diagnosed with NIDCM were enrolled from January 2010 to December 2019.
Results Logistic regression analyses showed that serum chloride was significantly associated with in-hospital death. Receiver operating characteristic (ROC) curve analyses showed that serum chloride had excellent prognostic ability for in-hospital and long-term death (area under the curve (AUC)=0.690 and AUC=0.710, respectively). Kaplan-Meier survival analysis showed that the patients with hypochloremia had worse prognoses than those without hypochloremia (log-rank χ2=56.69, p<0.001). After adjusting for age, serum calcium, serum sodium, left ventricular ejection fraction, lg NT-proBNP and use of diuretics, serum chloride remained an independent predictor of long-term death (HR 0.934, 95% CI 0.913 to 0.954, p<0.001).
Conclusions Serum chloride concentration was a prognostic indicator in elderly patients with NIDCM, and hypochloremia was significantly associated with both in-hospital and long-term poor outcomes.
- cardiomyopathy
- heart failure
- adult cardiology
Data availability statement
Data are available upon reasonable request. The datasets generated during and/or analysed during the current study are not publicly available due to privacy or ethical restrictions but are available from the corresponding author on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
This study enrolled a relatively large cohort with non-ischaemic dilated cardiomyopathy (NIDCM).
This is the first study to report the relationship between serum chloride and prognosis in elderly patients with NIDCM.
It is unknown whether hypochloremia was corrected during hospitalisation.
Large prospective randomised clinical trials are required to evaluate the negative effect of hypochloremia in cardiovascular disease.
Introduction
Non-ischaemic dilated cardiomyopathy (NIDCM) is defined as left ventricle (LV) enlargement and global systolic function impairment (left ventricular ejection fraction (LVEF) <45%) in the absence of coronary artery disease or increased loading conditions,1 and NIDCM is one of the most common causes of heart failure (HF) and the most common indicator for heart transplantation, with an estimated prevalence of 40 per 100 000 individuals and an annual incidence of 7 per 100 000 individuals.2 3 Currently, no effective treatments can prevent the progression of NIDCM to HF,4 and patients often suffer from refractory HF and even sudden cardiac death (SCD) and could to benefit from cardiac transplantation.5 6 This condition places a heavy financial burden on global healthcare systems. Patients with NIDCM have an increased risk of life-threatening arrhythmia and HF, and the stratification of their risk is a real challenge for clinicians.7
Previous research has shown that a few variables, such as reduced LVEF and elevated levels of brain natriuretic peptide,8 have been associated with poor outcomes of patients (age <60 years) with dilated cardiomyopathy (DCM). Although there have been many studies on DCM,1–3 9 to the best of our knowledge, there have been no previous studies on risk factors for elderly patients. Recently, several studies showed that serum chloride has unique homeostatic roles in modulating neurohormonal pathways, regulating tubular diuretic-sensitive channels and influencing renal salt handling,10 11 and hypochloremia was found to have a potential prognostic role in HF.12–14 Thus, in this study, we assessed the association of serum chloride with clinical outcomes in elderly patients with NIDCM.
Methods
Study population
According to the scientific statement established by the American Heart Association, NIDCM is defined as ventricular dilatation and systolic dysfunction excluding vascular diseases such as coronary heart disease and myocardial infarction.8 For this study, we retrospectively investigated 1088 patients (age ≥60 years) admitted for NIDCM to Guangdong Provincial People’s Hospital (Guangzhou, China) from January 2010 to December 2019.
Patient and public involvement
No patient was involved.
Data source
Baseline characteristics, medical history and laboratory results were collected from the electronic medical database. Clinical information was collected from an electronic case report form by one researcher and randomly confirmed by another researcher. Basal serum chloride samples were collected the morning after admission. Serum chloride was measured by the bromocresol green method using a Beckman Coulter AU5821 or AU5831 (Beckman Coulter, California, USA). The LVEF was determined using Simpson’s biplane method. Linear internal measurements of the LV and its walls were performed in the parasternal view.
Definition and endpoints
Serum chloride of <96 mmol/L on admission was defined as hypochloremia.10 The patients were followed up through telephone calls or via a review of their outpatient clinic records in 2021. The endpoints of this study were in-hospital death and all-cause death during follow-up.
Statistical analysis
Continuous variables are presented as the mean±SD and were compared by one-way analysis of variance. Categorical variables are expressed as numbers, n (proportions, %) and were compared through Pearson’s χ2 tests. Missing values were excluded from the analysis. Kaplan-Meier survival curves were drawn to compare the cumulative event rates among the groups and were compared by the log-rank test. Receiver operating characteristic (ROC) curves were drawn to assess the prognostic value of serum chloride. Logistic regression analyses were used to evaluate the association of serum chloride with in-hospital mortality. Multivariate Cox proportional hazard regression models were built to adjust for possible confounders at baseline and evaluate the association of serum chloride with long-term mortality. All analyses were performed using SPSS software V.26.0, and p values were two-sided with a significance level of 0.05.
Results
A total of 1088 patients (711 men and 377 women) were included in this study, and 167 patients were older than 75 years old. A total of 506 patients died, and 30 were lost during a median follow-up of 67±1.8 months. All patients were divided into two groups according to the serum chloride concentrations on admission: hypochloremia (<96 mmol/L) and nonhypochloremia (≥96 mmol/L).
First, detailed baseline characteristics for this cohort showed that sex composition and smoking history were similar between the two groups. The patients with hypochloremia were older than those without (69.57±7.07 years vs 68.24±6.22 years, p=0.042). Second, the mean LVEF was less than 35% in both groups and lower in the hypochloremic group, in which the patients had higher values of serum creatinine on admission (table 1). Third, the prevalence of in-hospital death (12.9% vs 3.2%, p<0.001) and long-term death (65.3% vs 40.0%, p<0.001) was significantly higher in the hypochloremic patients.
Baseline demographics and clinical characteristics
Univariate logistic regression analysis showed that admission serum chloride concentrations were independently and inversely associated with in-hospital mortality (OR 0.887, 95% CI 0.845 to 0.930, p<0.001). After adjusting for age, serum calcium, serum sodium, LVEF, lg NT-proBNP and use of diuretics, serum chloride levels remained significantly related to in-hospital death (OR 0.943, 95% CI 0.892 to 0.998, p=0.042).
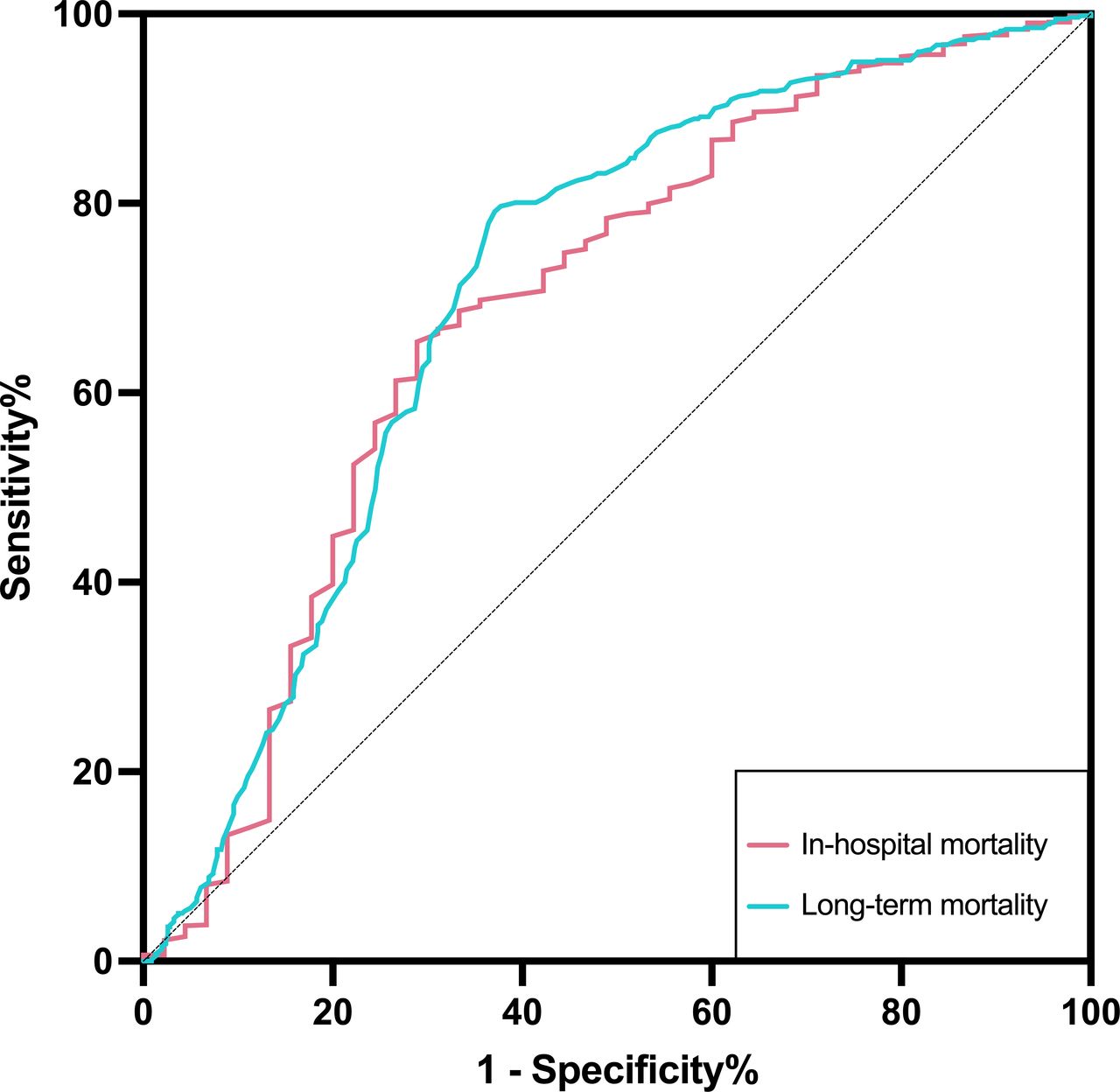
ROC curve analyses showed that serum chloride had excellent predictive ability for in-hospital and long-term death (area under the curve (AUC)=0.690, p<0.001, and AUC=0.710, p<0.001, respectively) (figure 1). A total of 461 all-cause deaths (303 men and 158 women) were recorded during the follow-up period. Kaplan-Meier survival estimates showed that the patients with hypochloremia had a lower cumulative survival rate (log-rank χ2=56.69, p<0.001) (figure 2).

Receiver operating characteristic curves of serum chloride concentrations in predicting in-hospital and long-term mortality.

{kind=link}
{kind=link}
Kaplan-Meier survival curves.
The multivariate Cox proportional hazard analysis showed that serum chloride remained a significant predictor for long-term mortality after adjusting for age, serum calcium, serum sodium, LVEF, lg NT-proBNP and use of diuretics (HR 0.934, 95% CI 0.913 to 0.954, p<0.001). Meanwhile, hypochloremia was a risk factor for all-cause death in elderly patients with NIDCM (HR 1.584, 95% CI 1.181 to 2.124, p=0.002) (table 2).
Multivariate Cox proportional hazard regression models for long-term mortality
Discussion
NIDCM has a high incidence in populations and often leads to HF and heart transplantation,2 3 accompanied by poor prognosis and high 3-year treated mortality.9 Older age was independently associated with impaired survival,15 so it is important to identify high-risk older patients early to improve their survival rate by choosing the appropriate treatment. However, there are limited studies in elderly patients with NIDCM. Studies in recent years have reported that hypochloremia is frequently present in different HF populations and that it is associated with a poor diuretic response and a higher risk of death,16–18 which suggests that chloride concentrations may be related to the prognosis of NIDCM.
To explore the relationship mentioned previously, we selected a relatively large Chinese cohort to study the prognostic role of serum chloride in elderly patients with NIDCM. The results showed that serum chloride concentrations on admission had a potential ability to predict in-hospital and long-term death, and hypochloremia was associated with lower survival, which indirectly reflected the pathological role of serum chloride in the progression of DCM, illuminating its prognostic role.
NIDCM is a heterogeneous heart muscle disease involving changes in the structure and composition of cardiomyocytes that lead to myocardial remodelling and severe impaired cardiac function.19 20 Plasma levels of NT-proBNP and LVEF have been proven to be powerful prognostic biomarkers of cardiac disease21 22; after adjusting for them, serum chloride remained independently associated with clinical outcome in this study. In addition, patients with DCM often receive diuretic treatment, especially in those with volume overload, which may promote the depletion of chloride and sodium.23 Serum calcium is recognised as an important electrolyte for maintaining cardiac function. Our study showed that serum chloride concentrations were still independently associated with in-hospital and long-term death after multivariable adjustment for potential confounders, including serum sodium and calcium levels and the use of diuretics, while serum sodium levels were no longer related to prognosis. These findings suggest that chloride provided stronger prognostic power than sodium, which is consistent with previous studies reporting that serum chloride but not serum sodium was a strong predictor of mortality in patients with HF.14 16 24 When considering electrolyte disturbances in cardiovascular disease, people have often tended to focus on hyponatremia, and the effect of serum chloride is largely ignored. This real-world observational study verified that chloride plays a key role in the progression of cardiovascular disease in a relatively large cohort of NIDCM, making up for the deficiency of randomised controlled trials.
These results could be explained by the regulatory role of chlorine in neurohormone activation.25 Patients with NIDCM are frequently admitted because of HF symptoms, including chronic HF and acute decompensated HF, whereas those enrolled in this study presented with a mean LVEF lower than 35%, which suggests a higher risk of SCD.26 27 When the cardiac ejection fraction decreases, compensatory homeostatic responses to the decrease in cardiac output are activated, such as the activation of the sympathetic nervous system and the renin–angiotensin–aldosterone system (RAAS); however, chronic activation of these neurohormonal systems will exert deleterious effects on the heart.28 It was reported that hypochloremia is related to higher renin secretion and then improves RAAS activity, resulting in worsening HF.29 30 Meanwhile, the stimulation of angiotensin II and aldosterone will also promote the excretion of chloride, which is involved in the development of hypochloremia.31 This means that the relationship between hypochloremia and RAAS activity is complex and closely related to HF pathophysiology.
In chronic HF, hypochloremia mayt be dilutional in nature and may result from an increased release of arginine vasopressin that promotes free-water reabsorption in the renal collecting ducts, and increased angiotensin II activation can stimulate aldosterone secretion, resulting in fluid retention.25 On the other hand, hypochloremia could also be depletional because of diuretic-induced salt wasting, especially when chloride is lower relative to sodium.14 25 Loop diuretics primarily inhibit the sodium–potassium–chloride cotransporter (NKCC) to reduce sodium and chloride reabsorption, which may lead to excessive chloride wasting.14 32 The asymmetrical reduction of sodium and chlorine in plasma compartments may be due to chloride being excreted in the urine while bicarbonate is being retained to maintain electroneutrality.33 In addition, NKCC has a role in maintaining myocardial volume and pH levels34; if acid–base imbalance occurs, myocardial contractility will be impaired.35
The use of loop and thiazide diuretics can effectively reduce the plasma volume by depleting serum chloride; however, these diuretics may induce hypochloremia that could lead to diuretic resistance.29 Previous studies indicated that acetazolamide, sodium glucose cotransporter 2 inhibitors and vasopressin receptor antagonists have the potential ability to increase serum chloride concentration while decreasing plasma volume, but further randomised controlled trials are required to verify the efficiency of these therapies.10 When hypochloremia is observed in patients with DCM, clinicians should choose diuretics carefully. Hypertonic saline and lysine chloride (an orally administered organic chloride salt) may directly enhance serum chloride levels, but their pharmacological impact is not clear,36 whereas correction of electrolyte imbalance can improve hemodynamics, myocardial contractility and prognosis of patients.
The present study highlights that the analysis of serum chloride concentrations remains favourable to refine outcomes of patients and provides new insights into the clinical strategies of DCM, such as the correction of chloride disturbance. Meanwhile, it provides the information needed to further study the mechanism of hypochloremia and emphasises the requirement to consider it when predicting the mortality of patients with DCM.
This is a retrospective study, and some limitations need to be clarified. In our study, serum chloride concentrations were measured at specific time points, but the influence of time-related changes cannot be ignored. The impact of changes in chloride levels on the prognosis is difficult to estimate. These patients are often admitted to the hospital due to worsening HF. It is difficult to know from the medical records whether hypochloremia was corrected during hospitalisation. Future studies should evaluate whether the strict monitoring and correction of hypochloremia have a beneficial effect on prognosis.
Conclusions
Serum chloride concentration was a prognostic indicator in elderly patients with NIDCM, and hypochloremia was significantly associated with both in-hospital and long-term poor outcomes, which may be related to haemodynamic abnormalities and activation of the neurohormonal system. The present study showed that analysis of serum chloride concentrations remains favourable in determining the outcomes of patients, but large prospective randomised clinical trials are still required to evaluate the negative effects of hypochloremia and the clinical benefits of serum chlorine-enhancing therapies in patients with DCM.
Data availability statement
Data are available upon reasonable request. The datasets generated during and/or analysed during the current study are not publicly available due to privacy or ethical restrictions but are available from the corresponding author on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the ethics committee of Guangdong Provincial People’s Hospital with a waiver of written informed consent due to the retrospective design of the study (approval number KY2020-475-01). Oral informed consent was obtained from the patients or their relatives by telephone and recorded by trained nurses during the follow-up period.
References
Footnotes
XL and XZ are joint first authors.
Correction notice The article has been corrected since it was published online. The authors wants to inform that Xinyi Li and Xiaonan Zhang are the joint first authors.
Contributors LJ contributed to the conception or design of the study and acted as the guarantor. XL, XZ, YL, FS and SS contributed to the acquisition, analysis or interpretation of data. XL and XZ drafted the manuscript. LJ and NT critically revised the manuscript. All the authors gave final approval and agreed to be accountable for all aspects of work ensuring integrity and accuracy.
Funding This study was supported by National Natural Science Foundation (grant number 82170339and 82270241), Science and Technology Planning Project of Guangzhou (grant number 202102080055) and Medical Science and Technology Research Fund Project of Guangdong (grant number C2020005). The work was not funded by any industry sponsors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, conduct, reporting or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.