Article Text

Abstract
Introduction Family members who care for elderly people experience high levels of chronic stress because of the intensive assistance they provide permanently to those who are losing their autonomy. Often considered a burden, this stress causes serious consequences to their health and worsens their quality of life (QoL). Reducing caregivers’ chronic stress via self-hypnosis protocols may be an effective treatment. The objective is to evaluate the feasibility and acceptance of self-hypnosis protocols taught by hypnotherapy-trained nurses to reduce the chronic stress of in-family caregivers.
Methods and analysis This study is a prospective, monocentric, non-blinded, parallel, pilot, randomised waitlist-controlled trial that will be conducted at the University Hospital of Reunion Island. Sixty participants will be randomly allocated to one of two groups: a self-hypnosis group (intervention) or a waitlist control group. After an 8-week training programme, intervention participants will practice self-hypnosis for ten minutes/day over 8 weeks and subsequently be followed up for 16 weeks thereafter. The primary outcome is to assess the feasibility of a 16-week self-hypnosis protocol for in-family caregivers. Secondary outcomes include the evaluation of the effects of practising self-hypnosis among in-family caregivers of elderly people concerning their stress levels, sleep disorders, levels of fatigue, and QoL at 2, 4 and 8 months on an exploratory basis.
Ethics and dissemination Ethics approval was obtained from the Institutional Ethics Committee CPP Ile de France VI—Groupe Hospitalier Pitié Salpêtrière on 14 April 2021 (ID RCB: 2021-A00009-32). All participants will receive information about the trial in verbal and written forms. They will give an oral consent which is notified in a dedicated research file prior before enrolment. Results will be published in peer-reviewed journals as well as presented and disseminated at conferences.
Trial registration number NCT04909970.
- EDUCATION & TRAINING (see Medical Education & Training)
- COMPLEMENTARY MEDICINE
- PUBLIC HEALTH
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
This study is the first to assess the practicability and acceptance of self-hypnosis use for in-family caregivers who feel chronic stress due to caring for dependent elderly people at home.
Objective tools to assess sleep quality, burden, fatigue and quality of life for family caregivers will be used in this study.
The sample size of the study pilot will be small to examine the effects of self-hypnosis for the treatment of stress.
All participants will be trained in self-hypnosis, however, at various times which may cause a bias.
The results of this feasibility study will provide data for fully powered effectiveness definitive randomised controlled trial.
Introduction
Population ageing is a worldwide phenomenon.1 Many countries are experiencing a boom in both the size and proportion of older individuals. In 2019, there were 703 million elderly individuals (65 years).1
Even though ageing is not considered an ailment in itself, it is associated with the decline in physiological and functional capacities of an individual which might impair the ability to cope with normal day-to-day living situations.2 It is also related to an increased prevalence of chronic illness and functional impairment resulting in a greater proportion of homebound individuals.3 4 A significant portion of elderly people, therefore, needs the help of another person to perform daily activities. Caregivers often provide (on a permanent or non-permanent basis) tasks such as bathing and dressing as well as several other instrumental activities of daily living such as shopping, preparing meals, communication and psychological support. They may also provide medical or nursing tasks.5 Moreover, 80% of adults requiring long-term care currently live in private accommodation and unpaid family caregivers provide 90% of their care.6
In-family caregivers, usually including the spouses, parents, children and/or other relatives such as friends, neighbours or others who have a significant personal relationship with the care recipients, play an essential role in supporting the well-being of older people.7 It requires time and effort, has financial costs and includes a change in an individual’s responsibilities which may alter family relationships.8 Therefore, caregiving for dependent elderly people at home is often considered an immense and tangible burden9 as evidenced by 84.6% of in-family caregivers,10 and is a significant source of chronic stress that can drastically affect a caregiver’s life where stress levels can increase as they age.11 This type of care is stressful since it requires intense, sometimes instantaneous daily actions performed for someone else who may have difficulty managing their physical, behavioural and cognitive needs over long periods. In other words, it creates a strain on the daily lives of caregivers. In many situations, providing care to a person with severe limitations is a full-time responsibility that can monopolise caregivers 24 hours a day.5 This assistance work has all the characteristics of a chronic stress producer, especially since caregivers often do not take time for themselves or seek out dedicated support structures.
In psychology, chronic stress is defined as a constant feeling of strain and pressure. Although small amounts of stress may be desirable, beneficial and even healthy, excessive amounts of stress can be physically harmful.12 The prevalence of stress among in-family caregivers is profound and varies according to the type of care being provided and the severity of the disease.13–15 Chronic stress experienced by caregivers leads to a deterioration in their quality of life (QoL) as well as their physical and mental health.16 Adverse consequences of stress have been reported in the literature17 with depression, pain and disturbances being the most common negative effects.17 An increased risk of coronary heart disease and ischaemic stroke in caregivers after their spouses were diagnosed with cancer was validated in a Swedish cohort study in 2012.18 An increased risk of mortality risk was also suggested.19 Lastly, chronic stress leads to the accelerated ageing of cognitive abilities.11 It is therefore necessary for healthcare professionals to consider the psychological health of caregivers.
Nursing interventions could reduce caregiver stress and help them to maintain an acceptable level of health.20 Moreover, complementary therapies are practiced by a growing number of nurses because of their effects on improving both physical and psychological health.21–23 Hypnosis is one complementary medicine that is effective in reducing chronic stress.24 25 Proposed by the American Psychological Association’s Division 30 (Society of Psychological Hypnosis), the definition of hypnosis is as ‘one person (the subject) is guided by another (the hypnotherapist) to respond to suggestions for changes in subjective experience, alterations in perception, sensation, emotion, thought or behaviour’.26 This state of consciousness known as the dissociative state is a natural phenomenon that occurs in moments of distraction, reverie or intense absorption in an activity and it is experienced by every person several times a day.27 Induction is an essential part of a session and consists of helping a subject focus on themselves and detach from the external environment to better feel sensations, emotions and memories. As such, it is the process that leads to unconscious content through a trance.28 A hypnotherapeutic group programme designed for a wide range of healthy people with high levels of perceived stress indicated positive effects.29
In stress management, the goal of hypnosis is to educate and train subjects to perform self-hypnosis to improve stress. Self-hypnosis can be defined as self-induction into the hypnotic process produced by self-generated suggestions without a hypnotherapist. The advantage of self-hypnosis is that it can be used independently and at a low cost.27
Hypnosis/self-hypnosis has been shown to provide clinical benefits with few adverse effects. It has shown to be efficacious in reducing stress and anxiety.30 A systematic review, consisting of 22 RCTs examining the effect of self-hypnosis as a clinical treatment published in 2019 (including 3 RCTs specifically on stress management), demonstrated the superior effectiveness of self-hypnosis compared with neurofeedback, relaxation or psychotherapy sessions in reducing stress.30 Self-hypnosis is likely to be most effective when taught as a stand-alone skills, involving at least three training sessions.30 Moreover, a 2018 systematic literature review of medical students identified different stress management interventions and tested its effectiveness. Students practising self-hypnosis gave significantly lower stress scores during the examination period than those in the control group.31 Regular training is considered necessary to master the technique and to be able to put oneself in a hypnotic state in the absence of a therapist. Practiced in a group setting, it is very useful for its reinforcing effects. This is particularly true when the different participants have common goals.32 Learning the basics of self-hypnosis is accessible to everyone.27 The appropriation of this technique and the subsequent acquisition of a new psychosocial skill for the caregiver will help to develop better self-esteem as well as enhance their involvement in the role of caregiver, therefore, empowering them daily.
In France, the use of self-hypnosis by caregivers is not yet available, nor are there any studies on its effects in terms of stress reduction. If it proves effective, self-hypnosis could be considered as a support treatment to reduce the stress of caregivers for the elderly. Professionals will be able to offer this therapy in a standardised and supervised manner to any caregiver either in or out of a hospital environment. This innovative tool will help broaden the range of care services available to family and friends who care for the elderly. Moreover, the contribution of new tools for senior care will be a factor in favour of improving the quality of healthcare.
Objectives
The objective of this study is to describe the protocol for a randomised waitlist-controlled trial (RWCT), pilot trial, designed with the primary outcome of assessing the feasibility of a 16-week self-hypnosis protocol for in-family caregivers (recruitment and adherence) to conduct a fully powered effectiveness definitive randomised controlled trial. The secondary outcomes are to compare the effects of self-hypnosis among in-family caregivers of elderly people on their stress levels, associated burdens, sleep quality, fatigue and QoL after 4 months.
Methods and analysis
Trial design
A prospective, monocentric, non-blinded, parallel, pilot, RWCT will take place at the University Hospital of Reunion Island (France) from May 2022 to August 2023. Sixty participants will be randomly allocated to one of two groups: a self-hypnosis group (intervention) or a waitlist control group. A non-treatment control was chosen instead of an active control because it would be very difficult to find a true placebo for hypnosis and as a pilot study the feasibility objective is a priority. The acronym POSSAID is in reference to the French title of the study ‘…d’autohyPnOse sur le StresS chronique des AIDants.’
Participant recruitment
The recruitment will take place in the Geriatric unit (short stay, day hospital and/or cognitive behavioural unit) and in the Medicine Department of the University Hospital Center of Reunion Island, where elderly people are received continuously. Study flyers will be posted in these units to advertise the clinical trial.
The nursing staff will inform in-family caregivers about participation in the study when they visit their loved ones. In the event of a positive response from them, the professionals will then fill out a study recruitment form on which the caregivers’ contact details will be noted. This form will be sent by secure email to the principal investigator (PI) every week. The PI will then contact the caregivers and arrange a visit either at home or at the university hospital during the hospitalisation of the patients that the caregivers take care of. The purpose of this first meeting will be to assess caregiver stress levels using the Chamoux scale, to collect consent after full information about the study, and to validate the caregiver’s inclusion. Recruitment will be carried out over 6 months. All caregivers will be compensated for their participation. Participant progress through the study is shown in figure 1.

Study flow chart.
Eligibility criteria
The target population will be in-family caregivers who cared for elderly people. Inclusion criteria will be as follows: (1) ≥aged 18 and (2) who are non-professional caregivers looking after a relative over 60 years of age in a situation of dependence (Iso-Resource Group <5),33 or are followed in the Geriatrics department or other medical department. Included participants will be those providing daily assistance in at least one of the three spheres of activity to an elderly person and who have a stress level assessment of more than 3 on the Visual Analogue Scale. They must have provided care to an elderly person for more than 2 years and have resided on Reunion Island for the duration of the study. Lastly, they must be able to read and write, be affiliated with or benefit from a social healthcare plan and give expressed oral consent.
Caregivers will be excluded if they: (1) suffer from serious chronic illness, (2) have a counter indication to hypnosis such as cognitive and/or psychiatric disorders or alcohol dependence, (3) use specific treatment(s) that prevent them from carrying out the procedure in a consistent manner or (4) have already practiced or currently practice hypnosis or another type of meditation.
Intervention group: self-hypnosis group
The intervention group will be in-family caregivers practising self-hypnosis. The self-hypnosis programme is going to be based on expert recommendations, data in literature and our experience/training. Figure 2 explains the self-hypnosis programme which will include two periods.

Self-hypnosis programme.
The first will consist of learning self-hypnosis. Caregivers will benefit from three individual sessions of 1 hour per session and two group meetings of 4 hours carried out over 8 weeks.
From week 1 (S1) to week 7 (S7), each participant will have three individual sessions with the nurse hypnotherapist. Hypnosis theory and practice will be developed during these first weeks. In week 5 (S5) and week 8 (S8), two group meetings will be held during which a group hypnosis session will be conducted. Weeks 2, 4 and 7 (S2, S4 and S7) will be free time slots for individual sessions for carers who were unable to attend the sessions scheduled in the study.
The individual hypnosis session will consist of five steps/phases (table 1). At the end of a third individual session, each participant in the intervention group will receive a self-hypnosis booklet with a CD (Reference: Petit cahier d'exercises d’hypnose avec 1 CD audio - David Ogez - Éditions Jouvence - 2017- ISBN 978-2-88905-774-0).
Phases of the individual hypnosis session in the first period of the programme (online supplemental file 1)
Supplemental material
A group meeting will be held for 10 caregivers at a time. For the study, three groups will be formed. The session will last 4 hours and will be marked by two key moments: (1) 1 hour of hypnosis practice followed by 3 hours of debriefing about experiences and feelings, benefits and (2) the ability to practice self-hypnosis of each caregiver. The emulation created by the motivation of the group will reinforce the new hypnosis skills of each participant.
The second period will consist of the autonomous regular practice of the techniques. Caregivers will have to carry out daily, autonomous, self-hypnosis sessions lasting 10 min over 8 weeks. All sessions will be conducted by a certified competent nurse and will take place at hospital in a dedicated and fully equipped room.
Waitlist control group
Participants who are allocated to the waiting-list control group may be offered hypnosis/self-hypnosis sessions at the end of the trial after they have completed their 16-week assessments. Treatment will subsequently be given as per the intervention group. Participants in the study will not be required to start another hypnosis programme or other alternative care practice programme during the research period.
Treatment as usual
All participants will continue the standard stress management practices such as anxiolytics, relaxation techniques, individual psychotherapy and any other treatment that is deemed necessary by the doctor.
Study duration
The treatment duration will be 16 weeks. The duration of each patient’s involvement in the study will be a minimum of 16 weeks with assessments at baseline, at the end of 8 weeks of treatment and 16 weeks. In the intervention group only, participants will continue hypnosis at home for another 16 weeks and an evaluation will be performed at 32 weeks to assess possible long-term effects.
Primary outcome measures
Primary feasibility outcomes: (1) recruitment: enrolment of 60 participants within 6 months before beginning the hypnosis intervention, (2) Intervention adherence: at least 80% of intervention-allocated participants completing at least two of the three individual sessions and one group session and at least 80% of planned interventions (daily self-hypnosis session) to be carried out over 2 months of daily practice.
Secondary outcome measures
The secondary outcomes will be as follows: (1) comparison of the variation between T0 and T2, in each of the two groups of caregivers of the average score of stress (Perceived Stress Scale-10, PSS 10), burden (Zarit), sleep quality (PSQI (Index de Qualité de Sommeil de Pittsburg)), fatigue level (Pichot) and QoL (Short Form 12, SF-12), (2) comparison in each of the two groups of the use of care, by collecting the consumption of care on the logbook and (3) measurement of changes in stress, burden, sleep, fatigue level and QoL over time (T0, T1, T2 and T3) only in the intervention arm.
Perceived stress will be assessed by the PSS-10 which is the most widely used psychological instrument for measuring perceived stress in terms of ‘perceived overwhelm’ and ‘perceived ability to cope’. It is a 10-item questionnaire developed for use in the general population because of its ease of reading and completion.34
The associated burden of caregivers will be measured using the 22-item Zarit scale presents a list of statements characterising the baseline state of people who care for someone else daily.35 This scale will be used as a self-questionnaire in our study.
For sleep quality, the Pittsburg Sleep Quality Index is a questionnaire consisting of 19 self-reported questions and assesses sleep disturbance over the past few months. It measures seven sleep components which cover subjective sleep quality, habitual sleep efficiency, sleep latency, sleep disturbance, sleep duration, sleep medication uses and daytime dysfunction.36
In-family caregiver fatigue will be assessed using the Pichot Fatigue Scale, which is a self-administered questionnaire used in general practice to assess the general level of fatigue.37
The QoL of caregivers will be assessed using the SF-12 scale. The SF-12 explores emotional, physical and social health. The SF-12 is a self-administered questionnaire and includes 12 items divided into 8 categories: physical activity, life and relationships with others, physical pain, perceived health, vitality, limitations due to mental state, limitations due to physical state and/or mental health.38
Data will be collected on the use of anxiolytics and antidepressant treatments, the number of doctor visits and the number of days in the hospital and/or respite care. Medication used by intervention group participants will be detailed by the caregivers during the research.
All participants will complete self-reported questionnaires at different times, under the same conditions. At T0, they will fill in the questionnaires at the university hospital before randomisation. However, at T1 and T2, for both groups, the questionnaires will be completed by the caregivers at home in week 9 and week 17, respectively. Caregivers will have to return the questionnaires and logbook by mail to the investigating team.
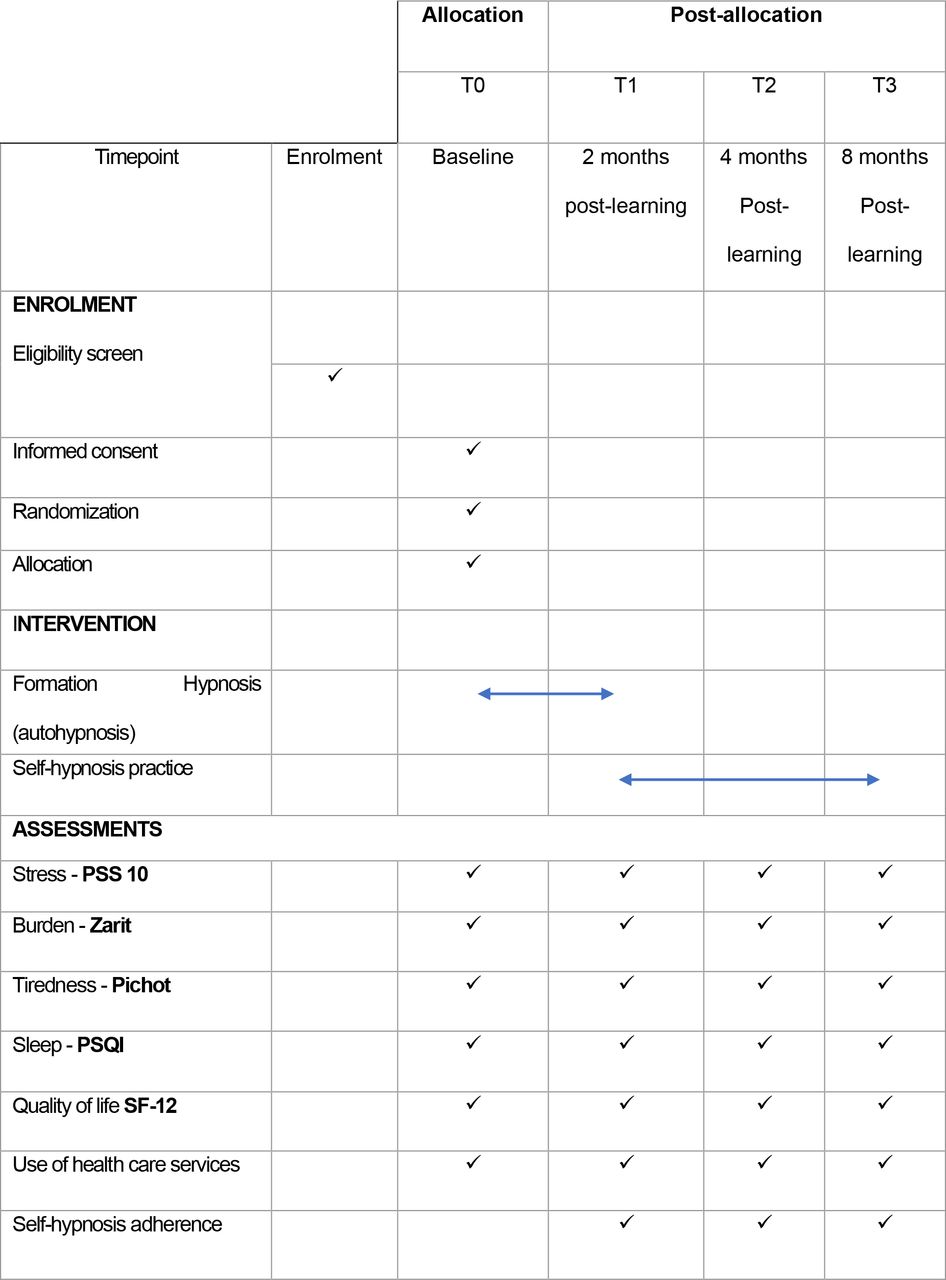
Study drop-out rates are to be defined as the number of participants who fail to complete the T2 and T3 post-treatment assessments. Figure 3 provides the schedule of this assessment and enrolment criteria for the study. Since we would need to recruit a sufficient number of participants before the intervention group begins, there will be a delay between the recruitment and beginning hypnosis or waiting list control for participants who are to be recruited early.
{kind=link}
{kind=link}
{kind=link}
Schedule of enrolment, interventions and assessments of the study.
Randomisation intervention
Eligible patients will be randomised on the day of inclusion by the main investigator and by using the Ennov Clinical software system. Randomisation will be balanced in both groups with a 1:1 allocation ratio without stratification. The randomisation list will be established by a statistician from the methodological support department before the start of the research. The method used will be a randomised block approach using the SAS Proc Plan system. We will build blocks of variable sizes and the investigator will perform the randomisation step directly via the electronic case report form (eCRF) using the CS Random module of the Ennov Clinical eCRF system on the day of inclusion.
Blinding intervention
Full blinding is not possible for this study because of the treatment (hypnosis). Caregivers, the project team and the researcher group will not be blinded concerning to which group the participant is randomised into. However, the statisticians will be blinded to treatment assignment until the primary analyses are completed.
Data collection
Data will be collected using an eCRF system. The database will be created by a data manager at the Methodology and Data Center using EnnovClinical software. All information required by the protocol will be recorded in the eCRF and explanations will be given for any missing data. Data will be collected as it is obtained and subsequently legibly transcribed into the eCRF.
Reasons for premature exit from the study will be as follows: (1) premature discontinuation of treatment, (2) participant unavailable for follow-up, (3) withdrawal of consent, (4) abandonment of the research project and (5) major protocol deviation (absence from individual and group training sessions).
Caregivers who discontinue research treatment, are unavailable for follow-up, or who drop-out of the study will all be included in the intention-to-treat (ITT) analysis. Database access will be protected by a username and password and will include various data access security levels according to the role assigned. Research team members will perform the data entry.
Data analysis
The sample size of 60 caregivers (30 per group) will be determined following the calculation recommendations for a pilot study (2005)39 and will be considered to be large enough to gauge whether or not the study will be feasible for a full-scale clinical trial intervention. This sample will allow us to estimate an adherence rate of 0.8 with confidence limits±0.1 around the point estimate. The primary analysis of this pilot trial will focus on the outcomes assessing feasibility by descriptive analysis. Objectives are key and will be focused on recruitment, intervention adherence and dropout rates. The recruitment rate will be calculated as the number of participants enrolled in the trial divided by the number of eligible patients to whom participation in the study is proposed. Intervention adherence will be measured dichotomously as to the proportion satisfying the noted adherence definition and the proportion of daily self-hypnosis sessions practiced over the 2 months. The drop-out rate is the proportion of participants who fail to complete the post-treatment assessment (T3). Although no statistical test for an efficacy objective is planned for a potentially undersized pilot study, we have considered it for the study in the future. No formal intervention effectiveness tests are planned due to the intentionally underpowered pilot nature of the study.39 40 The variation in scores (for stress, associated burdens, sleep disorders, levels of fatigue and QoL scales) between T0 and T2 will be compared between the two groups using an analysis of variance-covariance, adjusted on the group and the value of the score at T0. The comparison of the number of healthcare consumptions (including consultations and hospitalisations) will be compared between the two groups using a Student or Mann-Whitney U test depending on the conditions of application.
Changes in stress, burden, sleep, fatigue level and QoL in the intervention group will be estimated using a linear mixed model to account for intraindividual variability. All hypotheses will be tested two sided at the 5% alpha threshold. Analyses will be performed on an ITT basis and a sensitivity analysis on a per-protocol basis will also be performed. Patients who stopped research treatment, died, were lost to follow-up or dropped out of the study will all be included in the ITT analysis. Analyses will be performed using SAS V.9.4 software (SAS Institute).
Data monitoring
A clinical research associate mandated by the sponsor will check the participant files four times: (1) after inclusion, (2) 8 weeks post-inclusion, (3) 16 weeks postinclusion and (4) at the end of the research. Following the risk-based monitoring plan during these visits (participant, logistics, impact and resources), the following elements will be reviewed: a collection of informed consent, compliance with the research protocol and the procedures defined therein, the quality of data collected in the CRF namely accuracy, missing data and quality of the data collected in the observation book such as accuracy, missing data and the consistency of data with source documents. All visits will be documented in a written monitoring report.
Patient and public involvement
The research question on the effect of self-hypnosis on managing caregivers’ stress will be a first in the hospital. Participants were not involved in developing the study.
Ethics and dissemination
This study protocol was reviewed and approved by CPP Ile de France VI—Groupe Hospitalier Pitié Salpêtrière on 14 April 2021 (ID RCB: 2021-A00009-32). The study was registered on ClinicalTrials.gov on 9 June 2021 (NCT04909970). Results will be published in peer-reviewed journals as well as presented and disseminated at scientific conferences.
Ethics statements
Patient consent for publication
Acknowledgments
The authors would like to thank the Reunion Island University Hospital for their funding of the study and AcaciaTools for their proofreading services. The authors would also like to thank the nursing teams of the Geriatric and General Medicine departments, more specifically Dr. Nolwen Kervella, Dr. Christophe Donikian, Thierry Hoarau, David Ferrere, Laurie Kichenapanaidou and Anne-Françoise Casimir for their contributions, as well as Marie Coudy, the hypnotherapy nurse.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors DR and LB developed the research project concept and design. DR obtained funding and will manage the research project in the various departments of the University Hospital of Reunion Island. DR and LB wrote the manuscript.All authors read and approved the final manuscript.
Funding The study will be funded by the Reunion Island University Hospital. This research received no specific grant from any funding agency for commercial and not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.